4.1. Observational Study
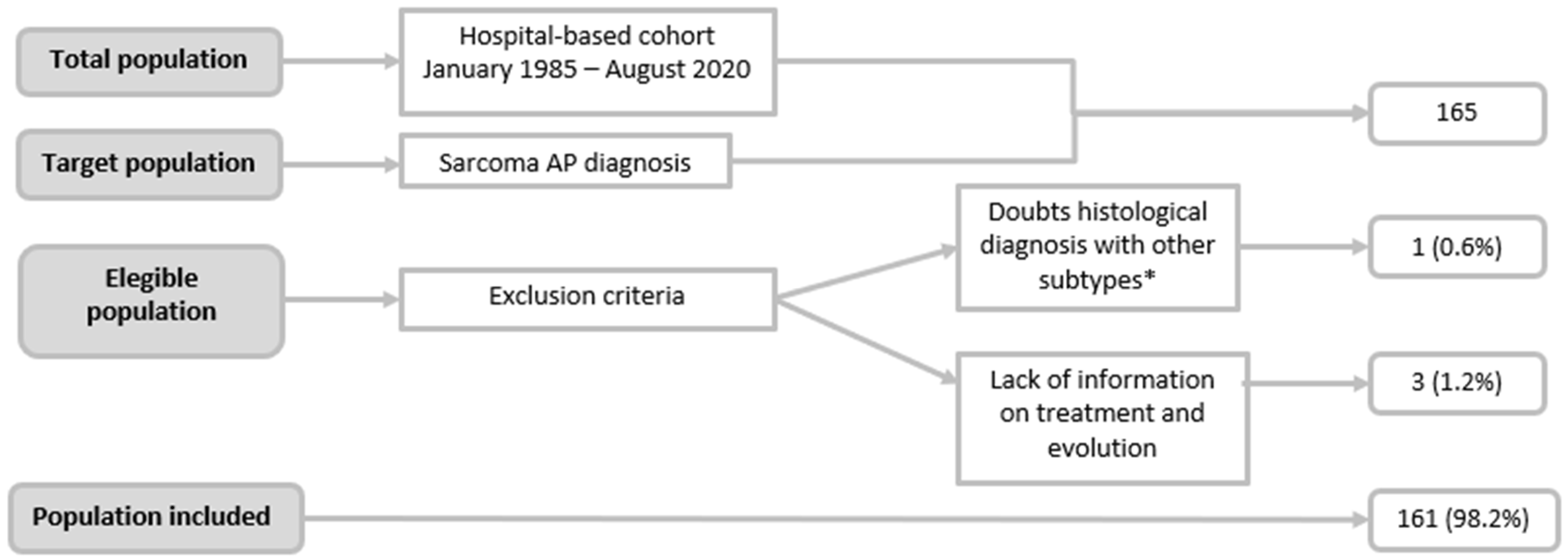
This study provided a general description of 35 years of experience at our centre, during which 161 patients diagnosed with uterine sarcoma were treated, for an incidence of 4–5 cases per year. This description focused on differentiating cases by histological subtype, with the most frequent being carcinosarcoma (45.3%). Statistically significant differences were found between some of the variables analysed, including postmenopausal status, advanced FIGO stage at diagnosis, and the existence of postsurgical residual tumours, which were each associated with poorer survival. The median OS was 176 months, and the DFS was 61.8 months. The analysis of survival by histological subgroup was not statistically significant, failing to identify differences that may have been clinically relevant.
Taking into account the number of patients in our series and in comparison with the various published studies, those that contributed a greater number of cases in less time were multicentre studies. Abeler et al. (2009) [
5] included 419 patients with sarcomas, followed by Wais M. et al. [
10] with 302 patients, the latter excluding CSs from their analysis. Regarding studies from a single centre, such as ours, Burghaus et al. [
8] and Park et al. [
19] performed their analyses on 143 and 127 patients with sarcomas, respectively. Although all authors agreed on the low incidence per year of this type of tumour, described between 0.5 and 2.1 per 100,000 women [
1,
2,
3,
4,
5,
6,
8], the large number of patients included in our study was the result of 35 years during which no significant differences were observed.
Because of this long study period, CS was not excluded from our series, although in 2009, the FIGO proposed exclusion from the sarcoma group. In our study, CSs represented 45.3% of cases, followed by LMSs, which constituted 31.7%. Taking into account other published studies that included CSs, despite the change in FIGO staging, the results herein are similar to those of Eiriz et al., 44% [
11], and other studies [
12], lower than that reported by Sait et al., 58% [
9], and higher than that reported by Gao Y. et al., 23% [
3]. We do not know the substantial basis for these differences, but they may be due to differences in the mean age of the patients treated by each centre.
Excluding CS from the classification, LMS was the most frequent subtype of uterine sarcoma, constituting 57.9% of cases. These data agree with the results reported by other authors, i.e., between 40–60% of uterine sarcomas [
1,
2,
4,
5,
6,
8,
16,
17,
18,
19,
22].
Again, taking into account the entire series and focusing on clinical variables, particularly age, herein, the mean age at diagnosis was 59.5 years, very similar to other studies [
4,
5,
8,
9,
10,
11]. Among the subgroups, there were significant differences, highlighting 4 years earlier in the ESS group and 3 years later in the CS and other sarcoma groups (
p < 0.001). For the majority of the authors, both ESS and LMS present early [
8,
12], which in turn is related to the premenopausal status being significantly more frequent in the LMS group (
p < 0.001). These differences in mean age were related to the frequency of associated comorbidities, being statistically more frequent in the CS group (72.6%) (
p = 0.01). The most frequently associated medical pathology was arterial hypertension, in 33.5% of patients.
No significant differences were found among the subgroups for the history of previous pelvic RT, in agreement with that published by Benito et al. and Koivisto-Korander et al. [
12,
13], nor were differences found in the history of tamoxifen use.
Regarding the clinical presentation, we found significant differences among the subgroups, highlighting bleeding in the CS group (84.9%) and incidental finding in surgical specimens in the LMS group (45%), similar to those reported by Van Den Haak et al. [
22] and higher than those described by Wang et al., 25% [
23]. Specifically, for LMSs, a presurgical diagnosis of leiomyoma is suspected, and subsequently, the histopathological analysis reveals tumour cell growth. In addition, this subtype occurs in two out of three patients in early stages, generally as a mass confined to the uterus that can be confused with a leiomyoma.
Regarding stage at diagnosis, the differences found among the subgroups trended towards statistical significance (
p = 0.05). A total of 62.3% were diagnosed at early stages; similar data have been reported in the literature, ranging from 56.4 to 69% [
3,
4,
8,
11,
12,
13,
18]. In contrast, other studies, such as those by Sait et al. [
9] and Kokawa et al. [
21] reported higher rates of diagnosis at advanced stages (III–IV), constituting 51.6% and 52.8%, respectively. As has been described, two out of every three LMSs are diagnosed at stage I, while two out of every three of the other sarcoma subgroup are diagnosed at more advanced stages. Although more than half of patients with ESSs are diagnosed at the initial stages, in agreement with Kokawa et al. [
21], we do not know why it is that up to 29% of patients are diagnosed at stage IV. This is probably because 77% of the ESSs in our sample were high grade.
Regarding the treatment variables as a function of the groups, we did not find significant differences for most of the data analysed. Surgery is the most widespread treatment for this type of tumour, and in our series, it was the first-line treatment for 93.2% of patients, with an average time from diagnosis to surgery of less than 1 month. The literature reports very similar surgical treatment rates ranging from 87.6% to 98% [
3,
11,
12,
13].
Regarding the surgical approach, 74.6% were laparotomies, and the differences among groups was significant (
p = 0.08), with a higher percentage (85.1%) in the ESS group. Regarding the less-frequent laparoscopy route (13.3%), this approach was used the most in the CS group (18.8%). The published rates in the literature are higher than those for our sample; Koivisto-Korander et al. [
13] reported 83% laparotomy, and Gao et al. [
3] reported 98.7% laparotomy. These laparotomy rates may be secondary to a higher stage at diagnosis, a larger tumour size, and the greater use of laparotomy in previous decades. Although it is not the object of our study, a greater tendency to use laparoscopy was observed.
Taking into account the various surgical techniques closely related to the performance of lymphadenectomy, there were statistically significant differences among the groups. Lymphadenectomy is used less frequently for LMS (
p < 0.01); in this histological subtype, lymphadenectomy is only indicated if pathological lymphadenopathy is observed by imaging tests or during surgery. Specifically, in the surgical techniques used for treatment, the least used was debulking (<10%), highlighting hysterectomy associated with bilateral adnexectomy in 90% of cases. A similar rate was reported by Benito et al., 93.6% [
12], and a slightly higher rate was reported by Koivisto-Korander et al., 97% [
13]; however, Burghaus et al. [
8] reported a lower rate of bilateral adnexectomy, ranging from 65% to 74%. These variations in adnexectomy rates highlight the existing controversy regarding the possibility of preserving the ovaries [
2]. Some studies report that performing bilateral adnexectomy improves the prognosis of patients with LMS and decreases the recurrence of ESS; however, other studies have not observed significant differences in OS or DFS [
19]. Ovarian preservation can be considered in premenopausal women with CSs and ESSs in early stages [
8]. In our study, the ovaries were preserved in only 10% of patients, with no differences among subgroups.
As described, in our series, significant differences were found in the lymphadenectomy rate (38%), a rate slightly higher than the 32.5% reported by Koivisto-Korander et al. [
13]. The highest lymphadenectomy rates were ESSn in the CS subgroup (61.4%), followed by the ESS subgroup (25.9%). These high lymphadenectomy rates for CS have been reported previously: Burghaus et al. [
8] reported a rate of 67%, and Gao et al. [
3] reported a rate of 88.9%. This is mainly due to the higher rate of lymph node involvement that this tumour subtype presents (approximately 22%) [
3,
12,
24]; lymphadenectomy has been part of the necessary surgical staging for this type of tumour since 2009, when it was classified as a high-grade endometrial carcinoma.
In our series, the rate of complete tumour resection was 84.6%. Other studies reported complete resection rates after surgery ranging from 72% to 87.7% [
8,
15,
19]. This variable is closely related to the stage at diagnosis and the prognosis of patients with this type of tumour, with higher rates of incomplete resection in locally advanced disease and lower survival for patients in whom R0 surgery is not achieved.
A total of 53.4% of the patients received adjuvant treatment, with statistically significant differences among the subgroups, highlighting a greater use of adjuvant treatment for the management of patients with CS (75.3% of cases), followed by those with ESS (38.7%). The rate of adjuvant treatment use was lower than the 58.4% reported by Benito et al. [
12] and 78% reported by Koivisto-Korander [
13]. These differences may be primarily due to the stage at diagnosis, the persistence of postsurgical residual tumours, and the number of CSs included in the sample.
In independent analyses of the use of adjuvant RT and chemotherapy (CT) in our series, the percentages were 40.4% and 22.4%, respectively. In the literature, adjuvant RT and CT rates range from 14% to 51% and 9% to 69%, respectively [
1,
9,
12,
13]. The variability reflects the fact that there is little evidence to support the use of adjuvant RT and/or CT in any type of uterine sarcoma except in CS.
In turn, we found significant differences among the subgroups in the use of adjuvant RT, which was highest in the CS group (60.3%), followed by the ESS group (29%). In contrast, we did not find differences among subgroups in the use of adjuvant chemotherapy, but there was a greater tendency to use adjuvant chemotherapy in the CS group (31.5%), followed by the LMS group (17.6%). The rates of adjuvant RT for CS in our series were higher than those reported in the literature (48–51%) [
8,
13,
15], and those of adjuvant CT were similar to the 35% rate observed by Burghaus et al. [
8], approximately half of that reported by Durnali et al. [
15] and much higher than the rate of 0% reported by Benito et al. [
12]. These differences reflect the notorious controversy over the benefit of this type of treatment in recent decades.
In our study, we had a recurrence rate of 45.3%, with no statistically significant differences among the different subtypes. These tumours have a high recurrence rate; some studies report a recurrence rate of 50–70% [
4,
12,
18]; others, such as those by Benito et al. [
12] and Sait et al. [
9], observed recurrence rates lower than 35% and 22%, respectively. This is also reflected in a DFS rate of less than 50%. The DFS rates reported in the literature range from 30% to 36% [
19]. In our study, the DFS rates were slightly higher than 49.7% at 5 years and 43.6% at 10 years, with a mean follow-up period of 69.4 months.
The prognosis of patients with these tumours is poor, with an overall 5-year survival rate of 54.2%, slightly better results than those reported by other studies, in which 5-year survival rates range from 27% to 51% [
4,
11,
12,
13,
14]. Survival from these tumours is fundamentally conditioned by their high recurrence rate (especially in the form of disseminated disease; in our study, 89.1% of cases), the stage at diagnosis, and the postsurgical residual tumour.
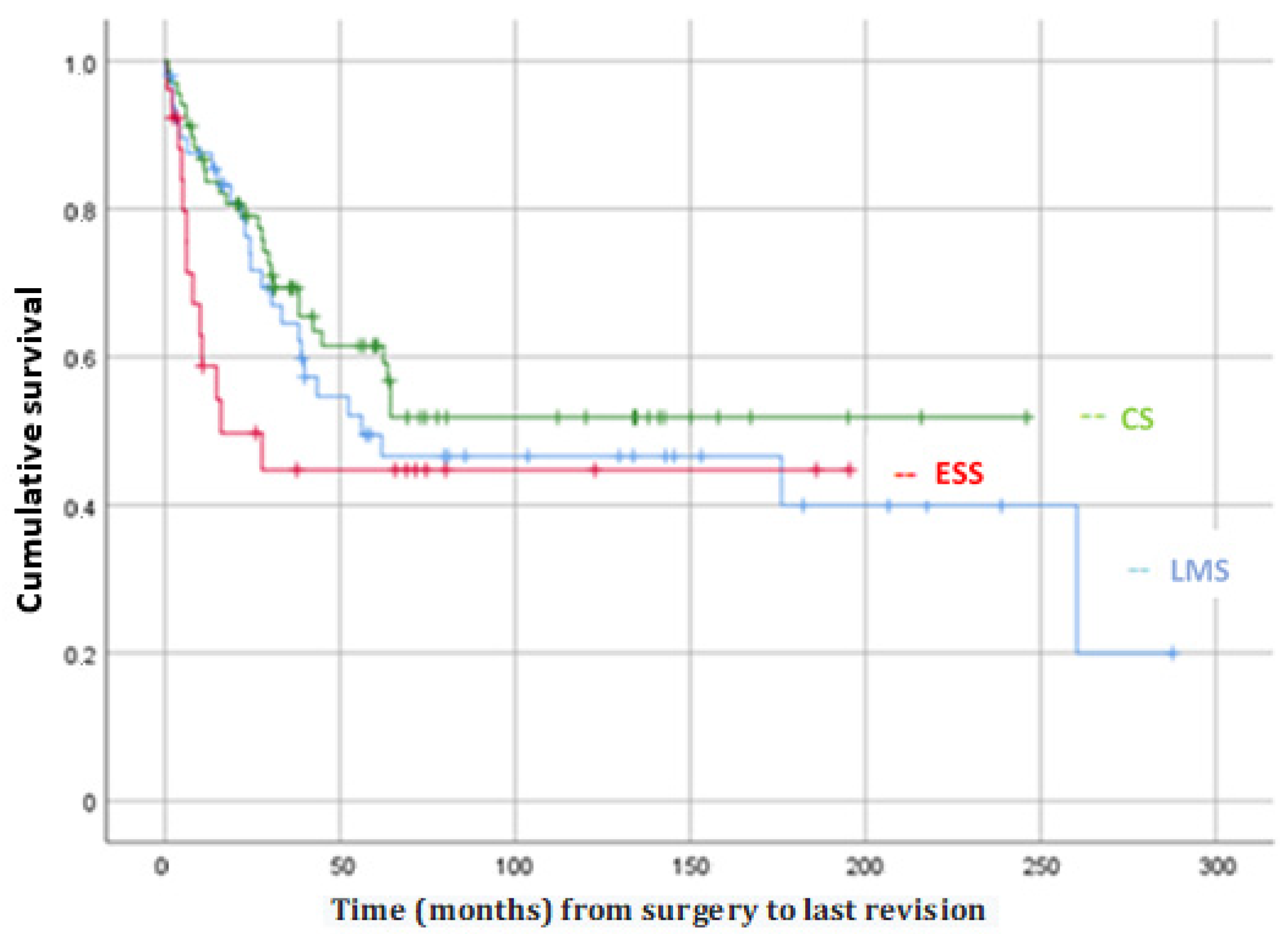
The survival analysis indicated that postmenopausal status, higher FIGO stage (III–IV), and the presence of residual tumours after surgery were significantly associated with a poorer mean survival, in agreement with other studies [
2,
8,
11,
18,
19,
25]. However, no statistically significant differences were observed with respect to OS or with respect to DFS among the different histological subtypes. Finally, although the literature shows that patients with the ESS subtype have the best prognosis [
19,
23,
26], we found a lower OS and a lower DFS in the ESS group, without reaching significance. These differences are probably due to the fact that in our sample 77% of ESS were high-grade.
In this study, we highlighted the differences and similarities of CS and the whole group of other subtypes of uterine sarcomas. CSs appeared more frequently in advanced ages, and consequently, in patients with more associated comorbidities. Unlike the rest of the histological subtypes, a higher percentage of CS cases presented in the form of vaginal bleeding (84.9%, followed by other less frequent subtypes of uterine sarcomas 66.6%) as well as other endometrial carcinomas. Furthermore, CSs tended to have a higher rate of lymph node involvement compared with other subtypes of uterine sarcomas, which may suggest a different biological behavior and would support its reclassification as a high-grade endometrial cancer subtype.
This higher rate of lymph node involvement together with the fact that lymphadenectomy is part of the surgical staging of endometrial carcinoma justify the higher rate of lymphadenectomy in this type of tumours. This is also in line with the higher rates of use of adjuvant treatment (both chemotherapy and radiotherapy) in this tumour type.
However, despite the reclassification of CS as a subtype of endometrial cancer and the systematisation of treatment, CSs still have a poor prognosis and in this study no differences were observed regarding survival between the different histological subtypes.
Among the limitations of the study are those subject to the descriptive nature of the study itself, as well as the long period of patient recruitment, during which new proposals for diagnosis, histological classification, staging, and treatments have been introduced. Another limitation is that the small sample size of low-grade ESS did not allow us to separate them from high-grade ESS, which can make the interpretation of the results difficult. On the other hand, among the strengths, we have already highlighted the high number of patients, from a single centre, resulting from the long recruitment period, allowing us to have a broader view of the entire series and to be able to compare the clinical, histopathological, diagnostic, and therapeutic characteristics of these tumours specifically.
4.2. Systematic Review
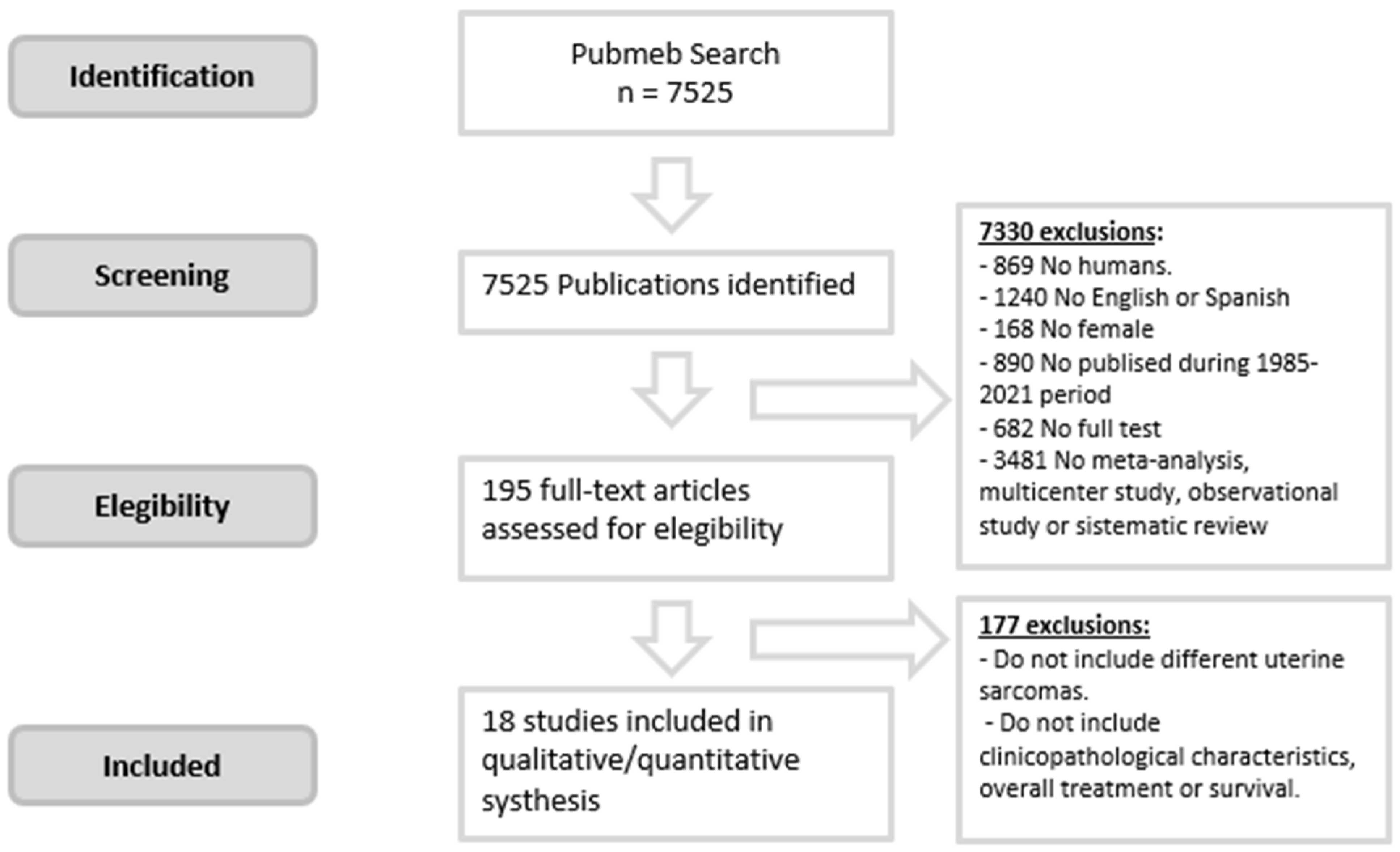
To our knowledge, this is the first systematic review on the subject. The review grouped a total of 2211 patients with a diagnosis of uterine sarcoma from 19 articles (including ours) published in 16 countries from 2002 to 2021, all with retrospective analyses. There is a growing interest in the topic because more than 68% of the studies have been published in the last decade. We also found a significant increase in articles that excluded CS from 2009 onward in their analysis. Regarding the recruitment period, only one article reported recruiting for less than 10 years, and 31.6% recruited for 20 years or more. Regarding participation in the studies, 73.7% were carried out in single centres.
The average incidence per article/year was 6–7 cases, highlighting the rarity of this type of tumour. The highest incidence rate per year was observed in multicentre studies, highlighting those by Abeler et al. [
5] and Wais et al. [
10], with annual incidence rates of 13–14 and 21–22 cases, respectively. These higher incidence rates are explained by the multicentre design of the studies.
Based on subtype, we grouped 1106 patients with LMSs, 459 with ESSs, and 416 with CSs. LMS is the most common subtype of uterine sarcoma, representing 45.7% of cases. However, when interpreting these last data, it should be taken into account that 5 of the 19 articles in this systematic review excluded CSs from their analysis and another two did not indicate them as exclusion criteria, but no CSs were part of their sample. The study with the highest % of LMSs was published by Kyriazoglou et al. [
4] in 2018, with 83.6% of cases LMS, followed by Wais et al. [
10], with 73.2% (both excluded CSs from their study). Among those studies with the highest percentage of LMSs that did not exclude CSs are those by Durnali A et al. [
15], with 58%, and Eiriz et al. [
11], with 40.3%.
The average age at diagnosis of this type of tumour is 55.8 years, consistent with the observation that this tumour type appears most frequently in individuals between 50 and 70 years of age. Uterine bleeding was the most frequent clinical presentation in 57.3% of patients. The highest percentages of bleeding were reported in the study by Burghaus et al. [
8] (81–92%) and in that by Benito et al. [
12] (78.6%), neither of which excluded CSs from their analysis. The lowest rates of bleeding were reported in the study by Sait et al. [
9] and Gao et al. [
3], i.e., 45% and 26.6%, respectively.
It is more common for these tumors to be in the initial stages at diagnosis; 36.3% of the cases presented in advanced stages (III–IV) at diagnosis (ranging between 22.4–53% in the different studies) and reported for the majority of the articles. Based on this systematic review, the recurrence rate was high and close to 42% of the cases, taken in consideration the information from 11 of 19 articles. The study with the highest recurrence rate, 63.4%, was that of Durnali et al. [
15], followed by Barquez-Muñoz et al. [
18]. Thangappah RBP. [
16] presented a recurrence rate much lower than the mean (18.2%); these data should be interpreted with caution since the study had a small sample size (
n = 30) and there was a total of eight losses to follow-up.
Regarding the OS rate, most studies (13 from 19 articles) collect it at 5 years or less. The average OS rate at 5 years was 41.4%. The highest OS rate was reported by Barquet-Muñoz et al. [
18] in a study conducted in Mexico and published in 2018 (61.9%). The 5-year OS rate for our patients was slightly higher than the average (54.2%) but less than Barquet-Muñoz et al. [
18]. The lowest OS rate was reported by Kokawa et al. [
21] (17.5%) in a study conducted in Japan, which may probably be associated with the fact that a high percentage of the tumors in their sample are diagnosed in advanced stages (51.6%). In general, it could be interesting to study the impact of race on the prognosis of this type of tumor; in our study, it could not be carried out because almost all the patients in our sample were Caucasian (96.8%).
The average DFS rate at 5 years was 36.9%, with the lowest survival rate found in the study by Sait et al. [
9] (14%), which could probably be again associated with the fact that a high percentage of the tumors in their sample were diagnosed in advanced stages (53%).
Regarding the limitations of this systematic review, it is of note that most conclusions extracted are based on published data and some heterogeneous criteria including the possibility to exclude/included CS and the absent of data from some variable like DFS rate at 5 or more years.


 ,
, 




{kind=link}
{kind=link}
{kind=link}