
Factors Predisposing the Response to Lumacaftor/Ivacaftor in People with Cystic Fibrosis

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
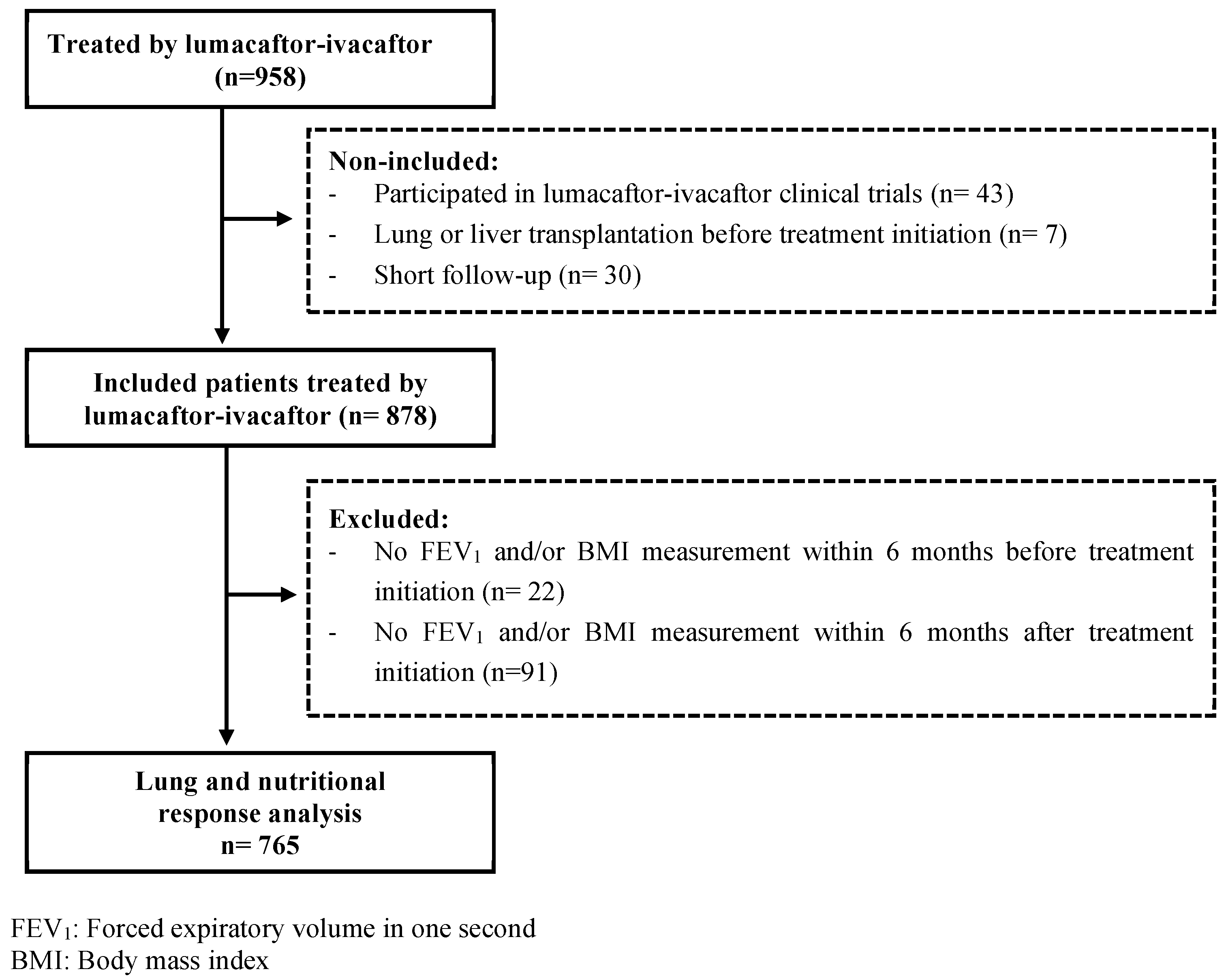
2.1. Study Design and Patients
2.2. Lung and Nutritional Response to Combined Lumacaftor/Ivacaftor Therapy
2.3. Modifiers of Response to Combined Lumacaftor/Ivacaftor Therapy
2.4. Statistical Analysis
3. Results
3.1. Study Population
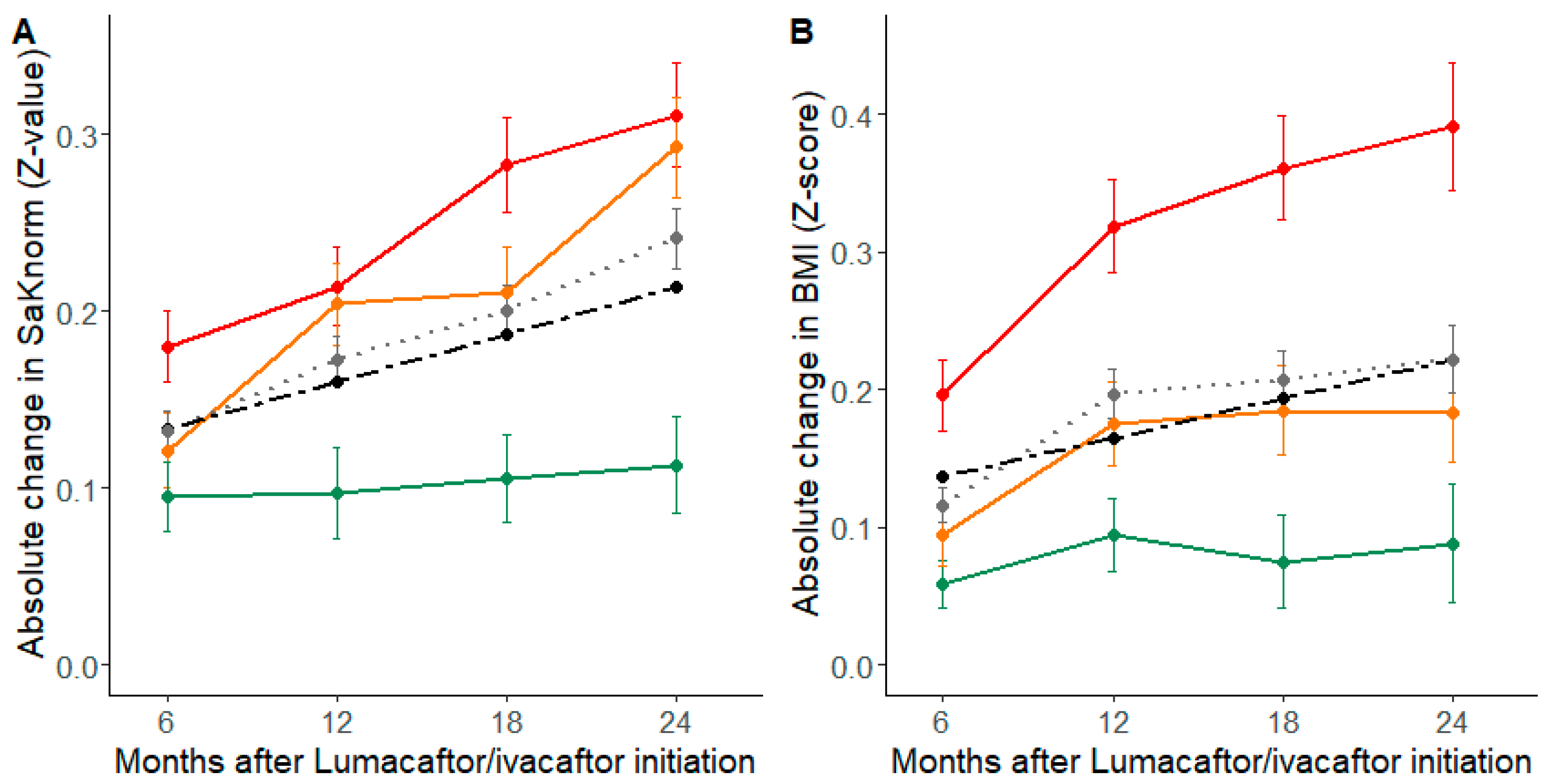
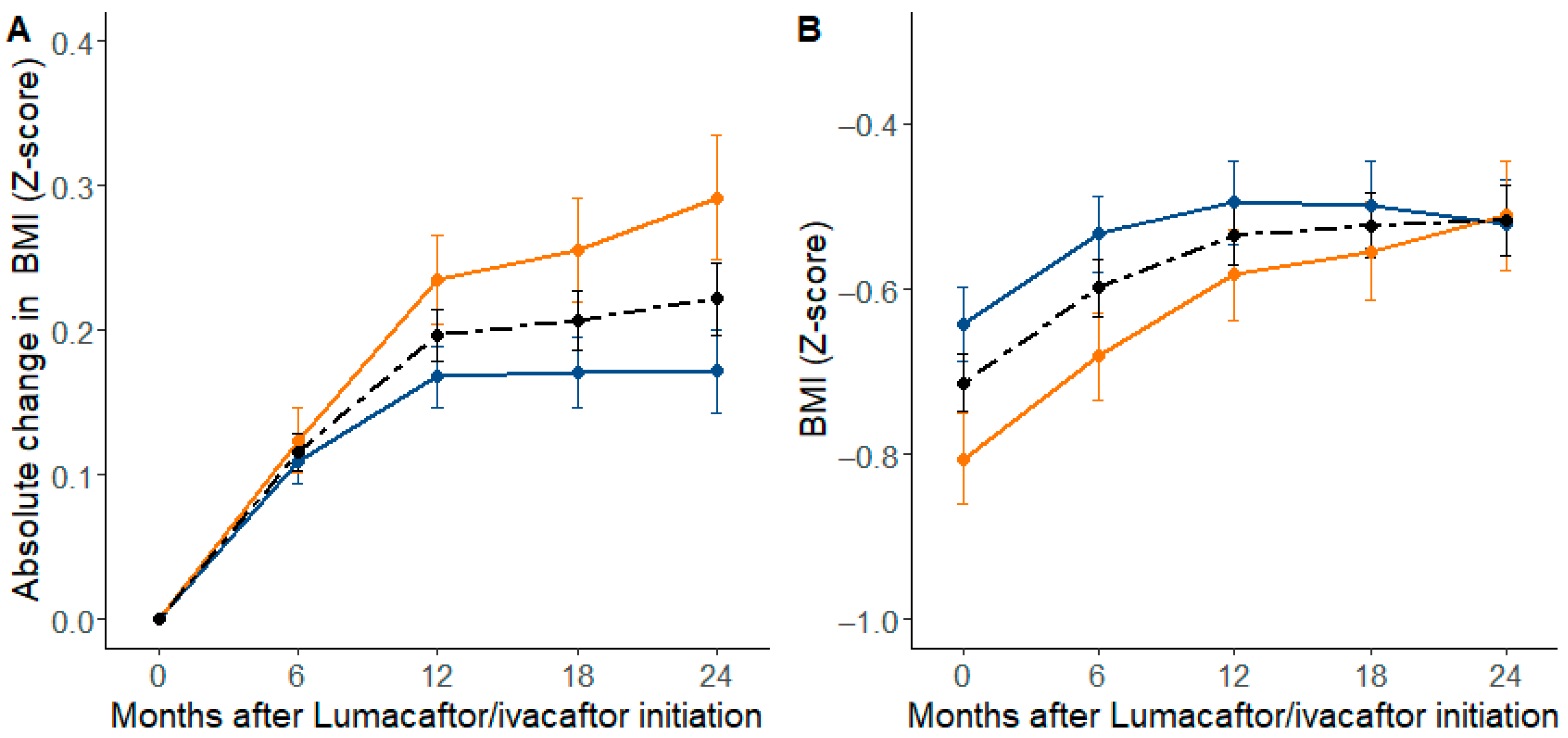
3.2. Overall Changes in Lung Function and Nutritional Status with LUMA-IVA
3.3. Genetic Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bell, S.C.; Mall, M.A.; Gutierrez, H.; Macek, M.; Madge, S.; Davies, J.C.; Burgel, P.-R.; Tullis, E.; Castaños, C.; Castellani, C.; et al. The future of cystic fibrosis care: A global perspective. Lancet Respir. Med. 2020, 8, 65–124, Corrigendum in 2019, 7, e40. [Google Scholar] [CrossRef] [Green Version]
- Wainwright, C.E.; Elborn, J.S.; Ramsey, B.W.; Marigowda, G.; Huang, X.; Cipolli, M.; Colombo, C.; Davies, J.C.; De Boeck, K.; Flume, P.A.; et al. Lumacaftor–Ivacaftor in Patients with Cystic Fibrosis Homozygous for Phe508del CFTR. N. Engl. J. Med. 2015, 373, 220–231. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.M.; Barry, P.J. Lumacaftor/ivacaftor for patients homozygous for Phe508del-CFTR: Should we curb our enthusiasm? Thorax 2015, 70, 615–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elborn, J.S.; Ramsey, B.; Wainwright, C.; Boyle, M. Response to: ‘Lumacaftor/ivacaftor for patients homozygous for Phe508del-CFTR: Should we curb our enthusiasm? Thorax 2015, 71, 185–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jennings, M.T.; Dezube, R.; Paranjape, S.; West, N.E.; Hong, G.; Braun, A.; Grant, J.; Merlo, C.A.; Lechtzin, N. An Observational Study of Outcomes and Tolerances in Patients with Cystic Fibrosis Initiated on Lumacaftor/Ivacaftor. Ann. Am. Thorac. Soc. 2017, 14, 1662–1666. [Google Scholar] [CrossRef] [PubMed]
- Konstan, M.W.; McKone, E.F.; Moss, R.B.; Marigowda, G.; Tian, S.; Waltz, D.; Huang, X.; Lubarsky, B.; Rubin, J.; Millar, S.J.; et al. Assessment of safety and efficacy of long-term treatment with combination lumacaftor and ivacaftor therapy in patients with cystic fibrosis homozygous for the F508del-CFTR mutation (PROGRESS): A phase 3, extension study. Lancet Respir. Med. 2016, 5, 107–118. [Google Scholar] [CrossRef]
- Burgel, P.R.; Munck, A.; Durieu, I.; Chiron, R.; Mely, L.; Prevotat, A.; Murris-Espin, M.; Porzio, M.; Abely, M.; Reix, P.; et al. Real-Life Safety and Effectiveness of Lumacaftor-Ivacaftor in Patients with Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2020, 201, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Cousar, J.L.; Jain, M.; Barto, T.L.; Haddad, T.; Atkinson, J.; Tian, S.; Tang, R.; Marigowda, G.; Waltz, D.; Pilewski, J.; et al. Lumacaftor/ivacaftor in patients with cystic fibrosis and advanced lung disease homozygous for F508del-CFTR. J. Cyst. Fibros. 2018, 17, 228–235. [Google Scholar] [CrossRef] [Green Version]
- Burgel, P.-R.; Durieu, I.; Chiron, R.; Mely, L.; Prevotat, A.; Murris-Espin, M.; Porzio, M.; Abely, M.; Reix, P.; Marguet, C.; et al. Clinical response to lumacaftor-ivacaftor in patients with cystic fibrosis according to baseline lung function. J. Cyst. Fibros. 2020, 20, 220–227. [Google Scholar] [CrossRef]
- Aalbers, B.; Groot, K.D.W.-D.; Arets, H.; Hofland, R.; de Kiviet, A.; Ven, M.V.O.-V.D.; Kruijswijk, M.; Schotman, S.; Michel, S.; van der Ent, C.; et al. Clinical effect of lumacaftor/ivacaftor in F508del homozygous CF patients with FEV1 ≥ 90% predicted at baseline. J. Cyst. Fibros. 2020, 19, 654–658. [Google Scholar] [CrossRef]
- Elborn, J.S.; Ramsey, B.W.; Boyle, M.P.; Konstan, M.W.; Huang, X.; Marigowda, G.; Waltz, D.; Wainwright, C. Efficacy and safety of lumacaftor/ivacaftor combination therapy in patients with cystic fibrosis homozygous for Phe508del CFTR by pulmonary function subgroup: A pooled analysis. Lancet Respir. Med. 2016, 4, 617–626. [Google Scholar] [CrossRef] [Green Version]
- Corvol, H.; Mésinèle, J.; Douksieh, I.-H.; Strug, L.J.; Boëlle, P.-Y.; Guillot, L. SLC26A9 Gene Is Associated With Lung Function Response to Ivacaftor in Patients With Cystic Fibrosis. Front. Pharmacol. 2018, 9, 828. [Google Scholar] [CrossRef] [PubMed]
- Strug, L.J.; Gonska, T.; He, G.; Keenan, K.; Ip, W.; Boëlle, P.-Y.; Lin, F.; Panjwani, N.; Gong, J.; Li, W.; et al. Cystic fibrosis gene modifierSLC26A9modulates airway response to CFTR-directed therapeutics. Hum. Mol. Genet. 2016, 25, 4590–4600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eastman, A.C.; Pace, R.G.; Dang, H.; Aksit, M.A.; Vecchio-Pagán, B.; Lam, A.-T.N.; O’Neal, W.K.; Blackman, S.M.; Knowles, M.R.; Cutting, G.R. SLC26A9 SNP rs7512462 is not associated with lung disease severity or lung function response to ivacaftor in cystic fibrosis patients with G551D-CFTR. J. Cyst. Fibros. 2021, 20, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.V.-N.; Ribeiro, J.D.; Bertuzzo, C.S.; Marson, F.A.L. Association of clinical severity of cystic fibrosis with variants in the SLC gene family (SLC6A14, SLC26A9, SLC11A1 and SLC9A3). Gene 2017, 629, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Rommens, J.M.; Corvol, H.; Li, W.; Li, X.; Chiang, T.A.; Lin, F.; Dorfman, R.; Busson, P.-F.; Parekh, R.V.; et al. Multiple apical plasma membrane constituents are associated with susceptibility to meconium ileus in individuals with cystic fibrosis. Nat. Genet. 2012, 44, 562–569. [Google Scholar] [CrossRef]
- Corvol, H.; Blackman, S.M.; Boëlle, P.-Y.; Gallins, P.J.; Pace, R.G.; Stonebraker, J.R.; Accurso, F.J.; Clement, A.; Collaco, J.M.; Dang, H.; et al. Genome-wide association meta-analysis identifies five modifier loci of lung disease severity in cystic fibrosis. Nat. Commun. 2015, 6, 8382. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Soave, D.; Miller, M.R.; Keenan, K.; Lin, F.; Gong, J.; Chiang, T.; Stephenson, A.L.; Durie, P.; Rommens, J.; et al. Unraveling the complex genetic model for cystic fibrosis: Pleiotropic effects of modifier genes on early cystic fibrosis-related morbidities. Qual. Life Res. 2014, 133, 151–161. [Google Scholar] [CrossRef]
- Dehillotte, C.; Lemonnier, L. Registre Français de la Mucoviscidose—Bilan des Données 2018, Vaincre la Mucoviscidose. 2020. Available online: https://www.vaincrelamuco.org/registredelamuco (accessed on 1 June 2021).
- HAS. Conférence de Consensus—Prise en Charge du Patient Atteint de Mucoviscidose. 2002. Available online: https://www.has-sante.fr/upload/docs/application/pdf/Mucovisc_pneumo_infectio_long.pdf (accessed on 1 June 2021).
- HAS. Mucoviscidose: Protocole National de Diagnostic et de Soins Pour une Maladie Rare. Guide—Affection de Longue Durée. 2017. Available online: https://www.has-sante.fr/jcms/c_2792719/fr/mucoviscidose (accessed on 1 June 2021).
- Castellani, C.; Duff, A.J.; Bell, S.C.; Heijerman, H.G.; Munck, A.; Ratjen, F.; Sermet-Gaudelus, I.; Southern, K.W.; Barben, J.; Flume, P.A.; et al. ECFS best practice guidelines: The 2018 revision. J. Cyst. Fibros. 2018, 17, 153–178. [Google Scholar] [CrossRef] [Green Version]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Kulich, M.; Rosenfeld, M.; Campbell, J.; Kronmal, R.; Gibson, R.L.; Goss, C.H.; Ramsey, B. Disease-specific Reference Equations for Lung Function in Patients with Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2005, 172, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.; Commander, C.; Collaco, J.M.; Strug, L.J.; Li, W.; Wright, F.A.; Webel, A.D.; Pace, R.G.; Stonebraker, J.R.; Naughton, K.; et al. A novel lung disease phenotype adjusted for mortality attrition for cystic fibrosis Genetic modifier studies. Pediatr. Pulmonol. 2011, 46, 857–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Robins, J.M.; Rotnitzky, A.; Zhao, L.P. Analysis of Semiparametric Regression Models for Repeated Outcomes in the Presence of Missing Data. J. Am. Stat. Assoc. 1995, 90, 106–121. [Google Scholar] [CrossRef]
- Preisser, J.S.; Lohman, K.K.; Rathouz, P.J. Performance of weighted estimating equations for longitudinal binary data with drop-outs missing at random. Stat. Med. 2002, 21, 3035–3054. [Google Scholar] [CrossRef] [Green Version]
- Boëlle, P.; Debray, D.; Guillot, L.; Clement, A.; Corvol, H.; on behalf of the French CF Modifier Gene Study Investigators. Cystic Fibrosis Liver Disease: Outcomes and Risk Factors in a Large Cohort of French Patients. Hepatology 2018, 69, 1648–1656. [Google Scholar] [CrossRef] [Green Version]
- Kmit, A.; Marson, F.; Pereira, S.V.-N.; Vinagre, A.M.; Leite, G.S.; Servidoni, M.F.; Ribeiro, J.D.; Ribeiro, A.F.; Bertuzzo, C.S.; Amaral, M.D. Extent of rescue of F508del-CFTR function by VX-809 and VX-770 in human nasal epithelial cells correlates with SNP rs7512462 in SLC26A9 gene in F508del/F508del Cystic Fibrosis patients. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2019, 1865, 1323–1331. [Google Scholar] [CrossRef]
- Durand, E.; Boutin, P.; Meyre, D.; Charles, M.A.; Clement, K.; Dina, C.; Froguel, P. Polymorphisms in the Amino Acid Transporter Solute Carrier Family 6 (Neurotransmitter Transporter) Member 14 Gene Contribute to Polygenic Obesity in French Caucasians. Diabetes 2004, 53, 2483–2486. [Google Scholar] [CrossRef] [Green Version]
- Suviolahti, E.; Oksanen, L.J.; Öhman, M.; Cantor, R.M.; Ridderstråle, M.; Tuomi, T.; Kaprio, J.; Rissanen, A.; Mustajoki, P.; Jousilahti, P.; et al. The SLC6A14 gene shows evidence of association with obesity. J. Clin. Investig. 2003, 112, 1762–1772. [Google Scholar] [CrossRef]
- Miranda, R.C.; Vetter, S.B.; Genro, J.P.; Campagnolo, P.D.; Mattevi, V.S.; Vitolo, M.R.; Almeida, S. SLC6A14 and 5-HTR2C polymorphisms are associated with food intake and nutritional status in children. Clin. Biochem. 2015, 48, 1277–1282. [Google Scholar] [CrossRef]
- Sivaprakasam, S.; Sikder, M.O.; Ramalingam, L.; Kaur, G.; Dufour, J.M.; Moustaid-Moussa, N.; Wachtel, M.S.; Ganapathy, V. SLC6A14 deficiency is linked to obesity, fatty liver, and metabolic syndrome but only under conditions of a high-fat diet. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2021, 1867, 166087. [Google Scholar] [CrossRef] [PubMed]
- Debray, D.; Kelly, D.; Houwen, R.; Strandvik, B.; Colombo, C. Best practice guidance for the diagnosis and management of cystic fibrosis-associated liver disease. J. Cyst. Fibros. 2011, 10 (Suppl. 2), S29–S36. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patients Analysed n = 765 | Patients Excluded n = 113 | p-Value | |
|---|---|---|---|
| Male, % (n) | 56.21% (430) | 46.02% (52) | 0.042 |
| Caucasian origin, % (n) | 97.51% (745) | 97.35% (110) | 0.915 |
| Age at treatment initiation (years), mean ± SD | 22.2 ± 9.0 | 25.2 ± 9.4 | <0.001 |
| Age at treatment initiation (years), % (n) | |||
| ≤20 | 50.07% (383) | 31.86% (36) | 0.001 |
| 20–30 | 28.37% (217) | 38.05% (43) | |
| >30 | 21.57% (165) | 30.09% (34) | |
| Presence of meconium ileus % (n) | 16.57% (118) | 25.47% (27) | 0.025 |
| Presence of CFRD *, % (n) | 25.93% (195) | 31.13% (33) | 0.256 |
| Presence of CFLD *, % (n) | 36.04% (275) | 45.54% (51) | 0.052 |
| Presence of Pa-CC *, % (n) | 38.56% (295) | 44.25% (50) | 0.248 |
| Lung disease severity ‡ (SaKnorm Z-value), mean ± SD | 0.447 ± 0.702 | 0.457 ± 0.710 | 0.942 |
| Nutritional severity † (BMI Z-score), mean ± SD | −0.677 ± 0.932 | −0.807 ± 1.060 | 0.072 |
| Change in SaKnorm(Z-Value) ‡ ± SD | p-Value | Change in BMI(Z-Score) † ± SD | p-Value | |
|---|---|---|---|---|
| Female | −0.015 ± 0.023 | 0.5203 | 0.069 ± 0.034 | 0.0415 |
| Age at initiation (Years) | ||||
| ≤20 | Reference | Reference | Reference | Reference |
| 20–30 | 0.011 ± 0.026 | 0.6748 | 0.006 ± 0.037 | 0.8705 |
| >30 | −0.068 ± 0.023 | 0.0029 | −0.048 ± 0.038 | 0.2047 |
| Presence of meconium ileus | −0.019 ± 0.031 | 0.5401 | 0.010 ± 0.048 | 0.8407 |
| Presence of CFRD * | −0.003 ± 0.023 | 0.9066 | −0.011 ± 0.039 | 0.7698 |
| Presence of CFLD * | −0.004 ± 0.024 | 0.8839 | 0.003 ± 0.036 | 0.9414 |
| Presence of Pa-CC * | 0.018 ± 0.023 | 0.4380 | −0.022 ± 0.034 | 0.5116 |
| Baseline | ||||
| 3rd tercile | Reference | Reference | Reference | Reference |
| 2nd tercile | 0.105 ± 0.027 | 0.0001 | 0.080 ± 0.036 | 0.0273 |
| 1st tercile | 0.145 ± 0.028 | <0.0001 | 0.237 ± 0.040 | <0.0001 |
| Position £ | Alleles * | MAF EUR | MAF Cohort | HWE ** | Change in SaKnorm Z-Value ‡ ± SD | p-Value | Change in BMI Z-Score † ± SD | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| SLC26A9 | |||||||||
| rs1874361 | 1:205939058 | A/C | 0.48 | 0.46 | 0.419 | −0.006 ± 0.017 | 0.7338 | 0.009 ± 0.022 | 0.6919 |
| rs4077468 | 1:205945629 | A/G | 0.41 | 0.41 | 0.406 | −0.011 ± 0.016 | 0.4976 | −0.019 ± 0.023 | 0.4178 |
| rs4077469 | 1:205945757 | C/T | 0.41 | 0.41 | 0.496 | −0.013 ± 0.016 | 0.4177 | −0.023 ± 0.023 | 0.3350 |
| rs7419153 | 1:205948181 | G/A | 0.38 | 0.41 | 0.033 | 0.011 ± 0.017 | 0.4894 | 0.015 ± 0.024 | 0.5456 |
| rs7512462 | 1:205930467 | T/C | 0.41 | 0.41 | 0.451 | −0.006 ± 0.017 | 0.7102 | −0.023 ± 0.023 | 0.3166 |
| rs12047830 | 1:205947571 | G/A | 0.49 | 0.47 | 0.501 | −0.011 ± 0.017 | 0.5290 | −0.017 ± 0.024 | 0.4936 |
| SLC9A3 | |||||||||
| rs57221529 | 5:586509509 | A/G | 0.21 | 0.20 | 0.735 | 0.029 ± 0.019 | 0.1256 | 0.022 ± 0.029 | 0.4564 |
| SLC6A14 | |||||||||
| rs3788766 | X:116435671435671 | G/A | 0.36 | 0.37 | 0.388 | 0.000 ± 0.014 | 0.9719 | 0.008 ± 0.019 | 0.6797 |
| rs12839137 | X:116434382 | G/A | 0.22 | 0.21 | 0.862 | 0.000 ± 0.017 | 0.9852 | 0.045 ± 0.020 | 0.0276 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mésinèle, J.; Ruffin, M.; Guillot, L.; Boëlle, P.-Y.; Corvol, H.; on behalf of the French CF Modifier Gene Study Investigators. Factors Predisposing the Response to Lumacaftor/Ivacaftor in People with Cystic Fibrosis. J. Pers. Med. 2022, 12, 252. https://doi.org/10.3390/jpm12020252
Mésinèle J, Ruffin M, Guillot L, Boëlle P-Y, Corvol H, on behalf of the French CF Modifier Gene Study Investigators. Factors Predisposing the Response to Lumacaftor/Ivacaftor in People with Cystic Fibrosis. Journal of Personalized Medicine. 2022; 12(2):252. https://doi.org/10.3390/jpm12020252
Chicago/Turabian StyleMésinèle, Julie, Manon Ruffin, Loïc Guillot, Pierre-Yves Boëlle, Harriet Corvol, and on behalf of the French CF Modifier Gene Study Investigators. 2022. "Factors Predisposing the Response to Lumacaftor/Ivacaftor in People with Cystic Fibrosis" Journal of Personalized Medicine 12, no. 2: 252. https://doi.org/10.3390/jpm12020252
APA StyleMésinèle, J., Ruffin, M., Guillot, L., Boëlle, P. -Y., Corvol, H., & on behalf of the French CF Modifier Gene Study Investigators. (2022). Factors Predisposing the Response to Lumacaftor/Ivacaftor in People with Cystic Fibrosis. Journal of Personalized Medicine, 12(2), 252. https://doi.org/10.3390/jpm12020252