
The Role of Robotic Visceral Surgery in Patients with Adhesions: A Systematic Review and Meta-Analysis


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Study Selection
2.2. Data Extraction and Quality Assessment of Included Studies
2.3. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment of Studies and Performance
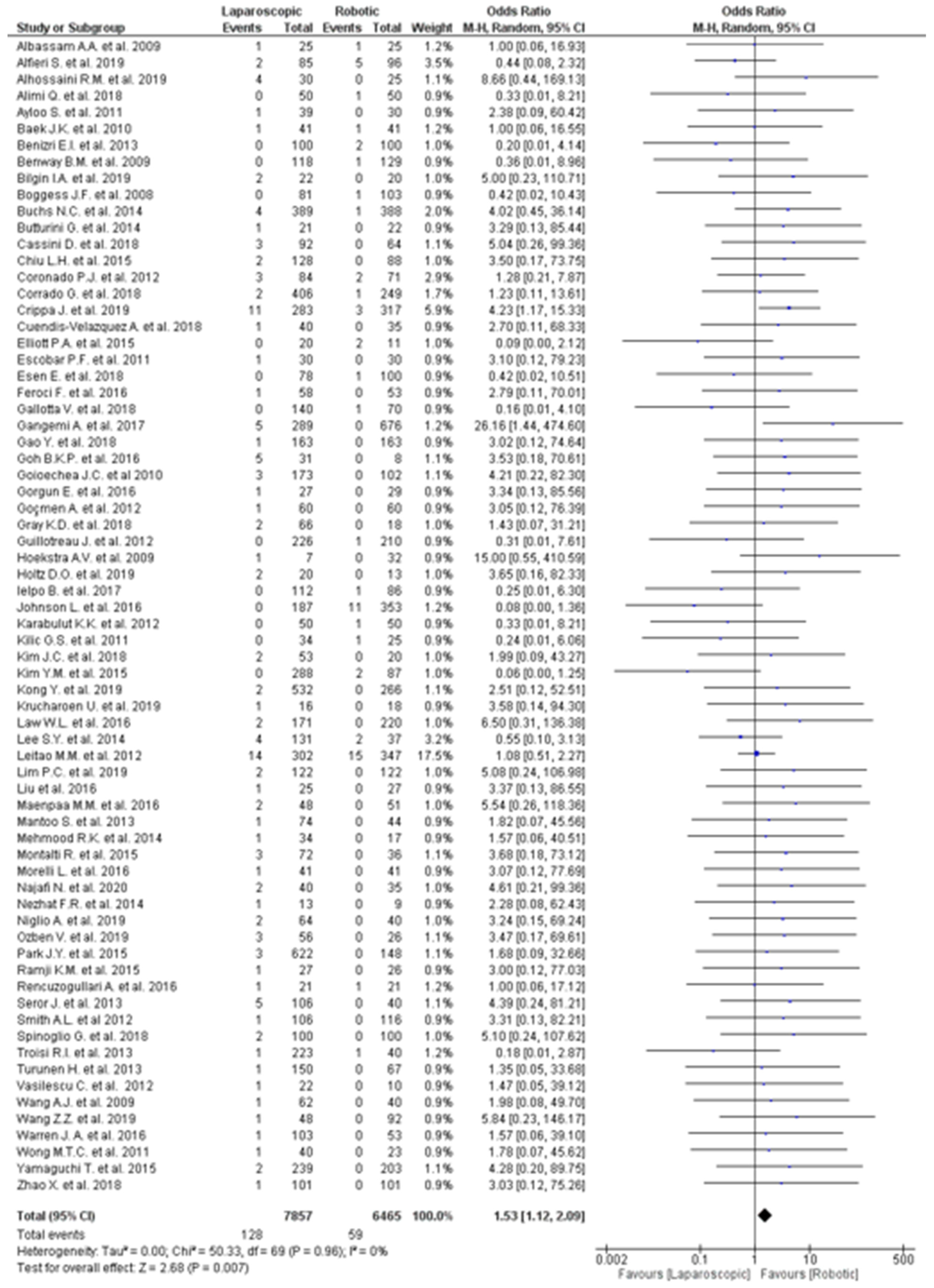
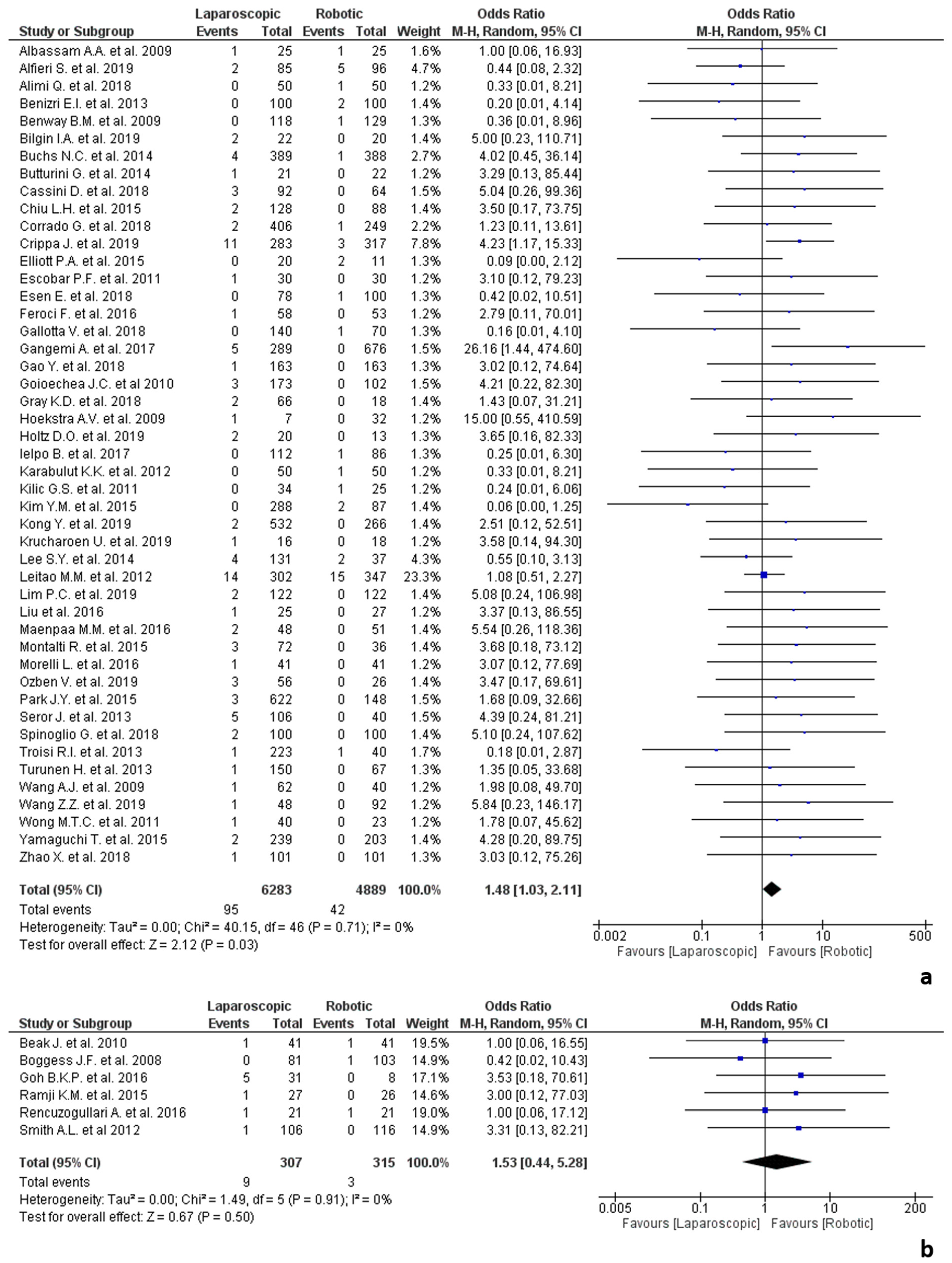
3.4. Conversion to Open Surgery Due to Adhesions
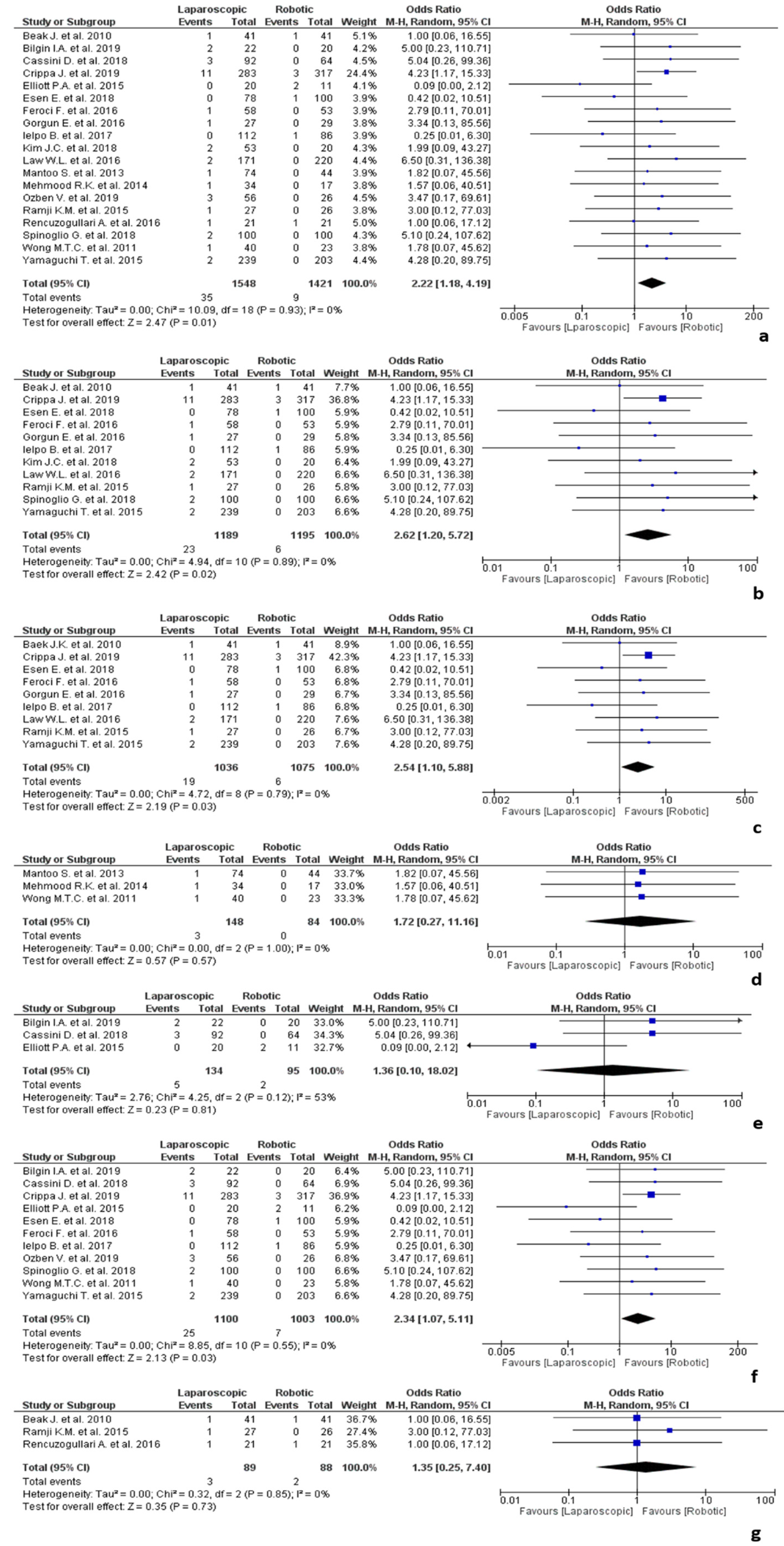
3.5. Subgroup Analysis
3.5.1. Colorectal Surgery
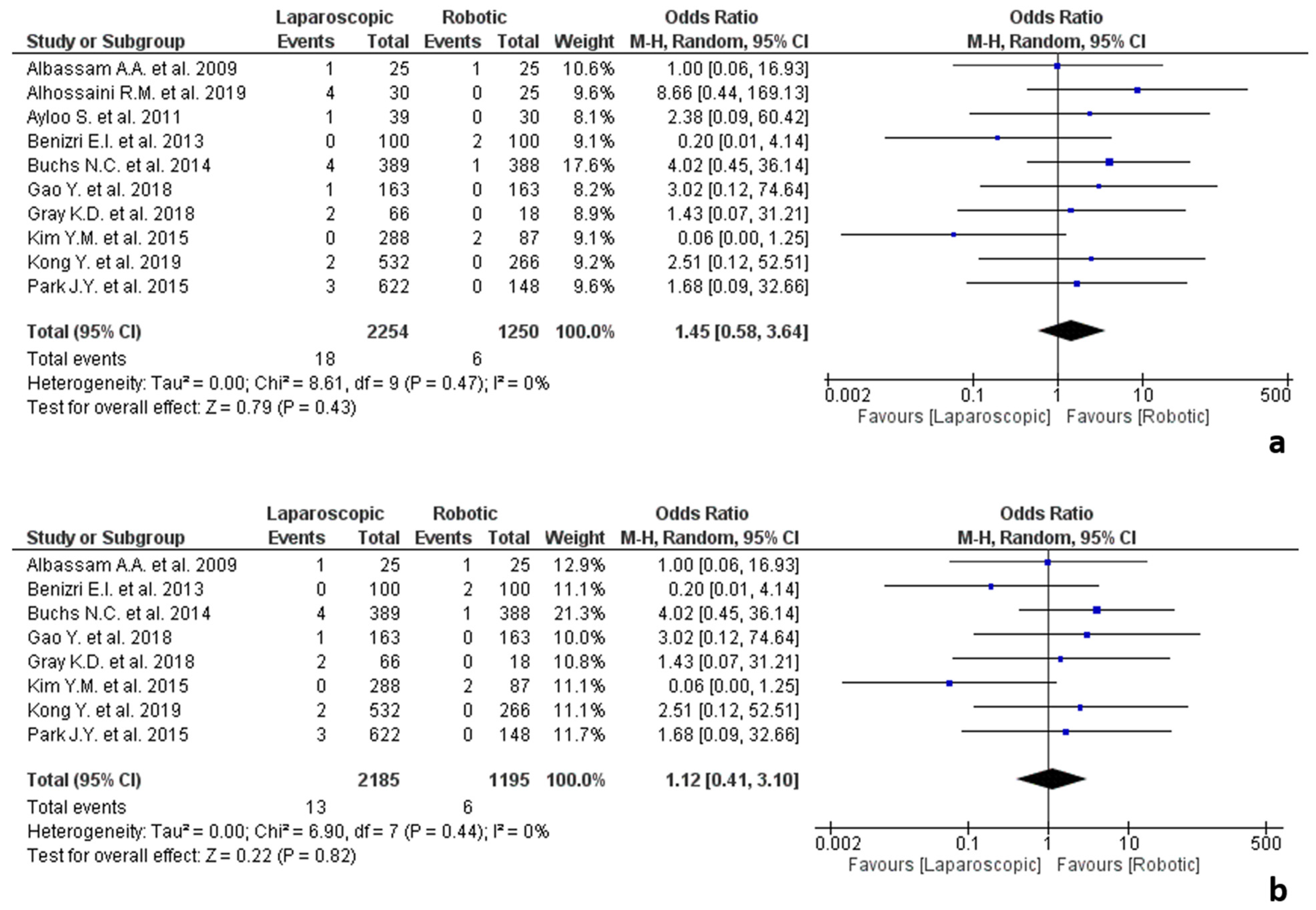
3.5.2. Oesophagogastric Surgery
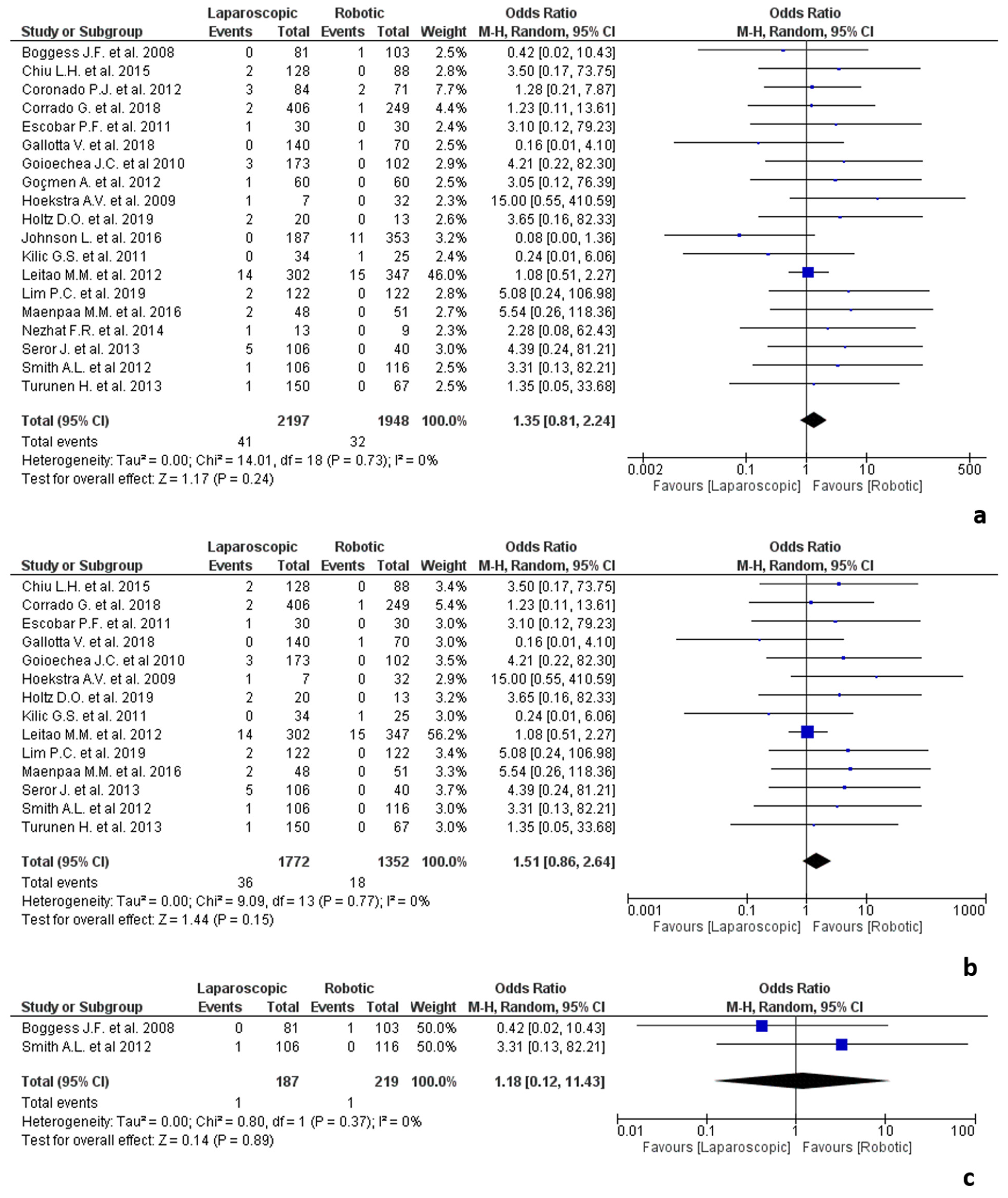
3.5.3. Gynaecologic Surgery
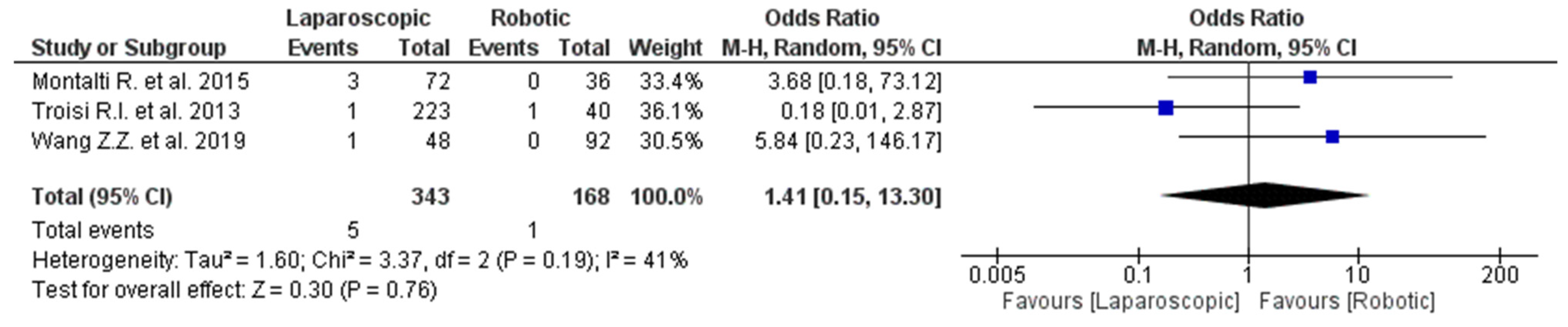
3.5.4. Hepatobiliary Surgery
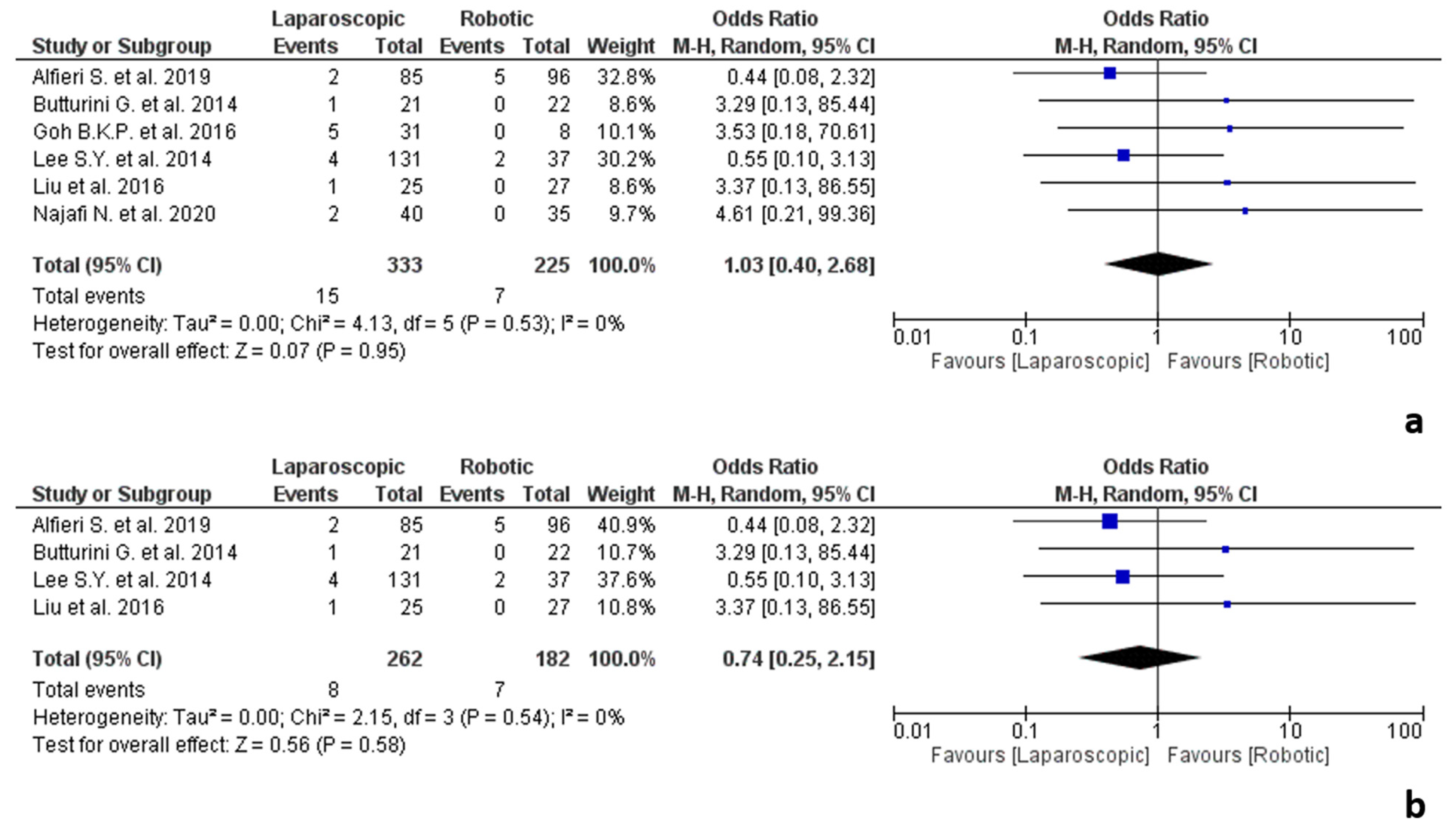
3.5.5. Pancreatic Surgery
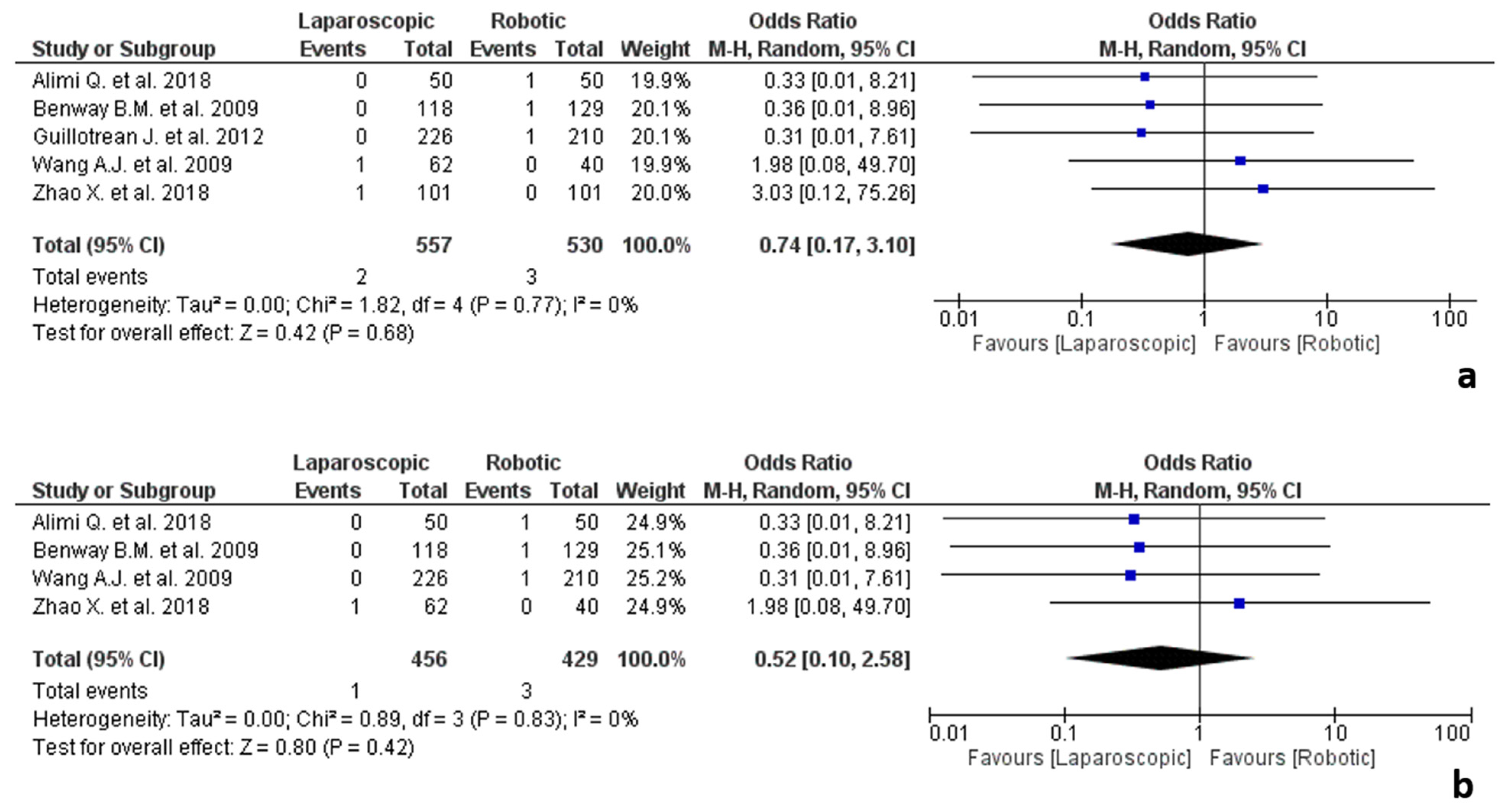
3.5.6. Urologic Surgery
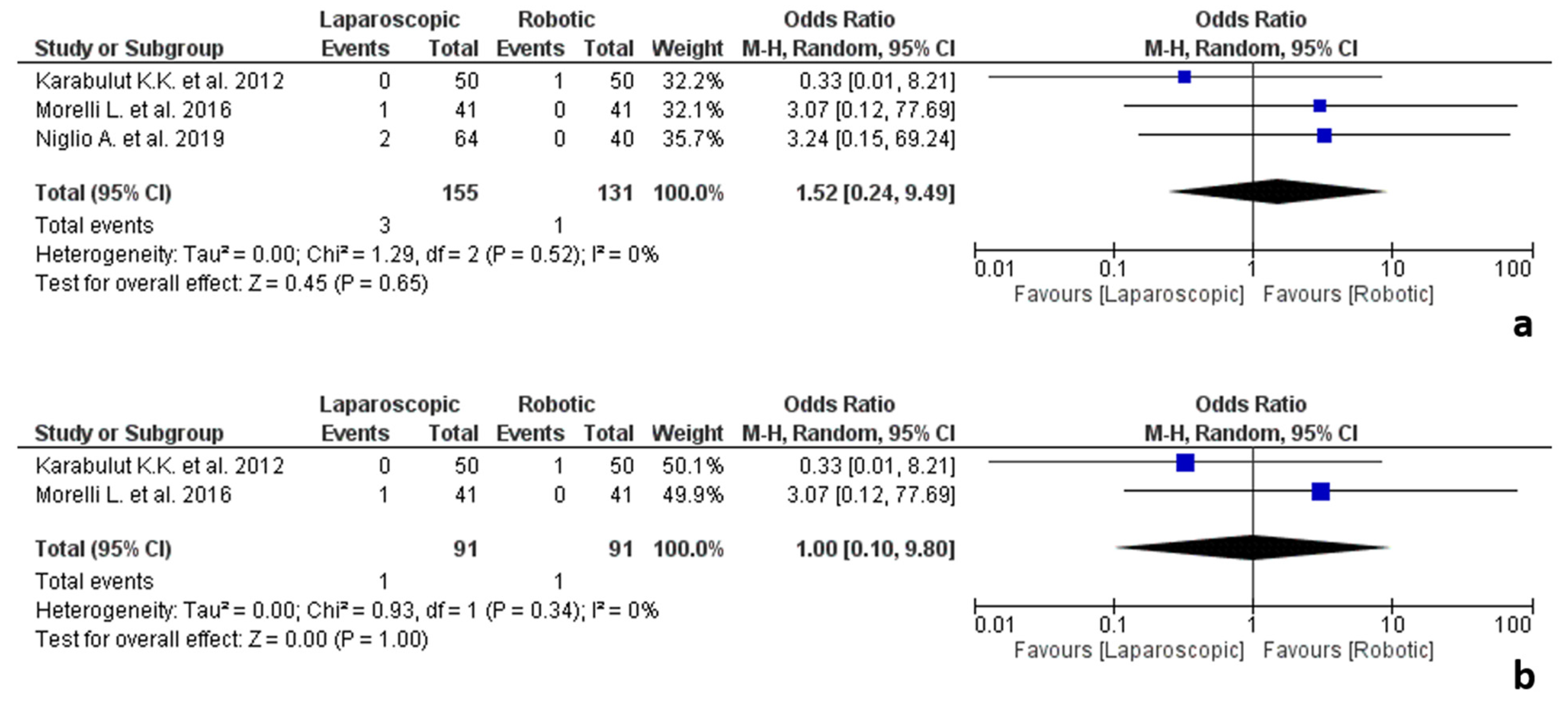
3.5.7. Endocrine Surgery
3.5.8. Other Surgical Fields
3.6. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Milone, M.; Manigrasso, M.; Vertaldi, S.; Velotti, N.; Aprea, G.; Maione, F.; Gennarelli, N.; De Simone, G.; De Conno, B.; Pesce, M.; et al. Robotic versus laparoscopic approach to treat symptomatic achalasia: Systematic review with meta-analysis. Dis. Esophagus 2019, 32, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Pan, Y.; Zhang, B.; Maher, H.; Wang, X.F.; Cai, X.J. Robotic versus laparoscopic Gastrectomy for gastric cancer: A systematic review and updated meta-analysis. BMC Surg. 2017, 17, 93. [Google Scholar] [CrossRef] [PubMed]
- Gavriilidis, P.; Wheeler, J.; Spinelli, A.; de’Angelis, N.; Simopoulos, C.; Di Saverio, S. Robotic vs laparoscopic total mesorectal excision for rectal cancers: Has a paradigm change occurred? A systematic review by updated meta-analysis. Colorectal Dis. 2020, 22, 1506–1517. [Google Scholar] [CrossRef] [PubMed]
- Solaini, L.; Bazzocchi, F.; Cavaliere, D.; Avanzolini, A.; Cucchetti, A.; Ercolani, G. Robotic versus laparoscopic right colectomy: An updated systematic review and meta-analysis. Surg. Endosc. 2017, 32, 1104–1110. [Google Scholar] [CrossRef]
- Milone, M.; Manigrasso, M.; Velotti, N.; Torino, S.; Vozza, A.; Sarnelli, G.; Aprea, G.; Maione, F.; Gennarelli, N.; Musella, M.; et al. Completeness of total mesorectum excision of laparoscopic versus robotic surgery: A review with a meta-analysis. Int. J. Colorectal Dis. 2019, 34, 983–991. [Google Scholar] [CrossRef]
- Ng, A.T.; Tam, P.C. Current status of robot-assisted surgery. Hong Kong Med. J. 2014, 20, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Ceccarelli, G.; Andolfi, E.; Biancafarina, A.; Rocca, A.; Amato, M.; Milone, M.; Scricciolo, M.; Frezza, B.; Miranda, E.; De Prizio, M.; et al. Robot-assisted surgery in elderly and very elderly population: Our experience in oncologic and general surgery with literature review. Aging Clin. Exp. Res. 2017, 29 (Suppl. 1), 55–63. [Google Scholar] [CrossRef] [Green Version]
- Park, D.A.; Lee, D.H.; Kim, S.W.; Lee, S.H. Comparative safety and effectiveness of robot-assisted laparoscopic hysterectomy versus conventional laparoscopy and laparotomy for endometrial cancer: A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2016, 42, 1303–1314. [Google Scholar] [CrossRef]
- Huang, Y.J.; Kang, Y.N.; Huang, Y.M.; Wu, A.T.; Wang, W.; Wei, P.L. Effects of laparoscopic vs robotic-assisted mesorectal excision for rectal cancer: An update systematic review and meta-analysis of randomized controlled trials. Asian J. Surg. 2019, 42, 657–666. [Google Scholar] [CrossRef]
- Nota, C.L.; Rinkes, I.H.B.; Molenaar, I.Q.; van Santvoort, H.C.; Fong, Y.; Hagendoorn, J. Robot-assisted laparoscopic liver resection: A systematic review and pooled analysis of minor and major hepatectomies. HPB 2016, 18, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Albright, B.B.; Witte, T.; Tofte, A.N.; Chou, J.; Black, J.D.; Desai, V.B.; Erekson, E.A. Robotic versus laparoscopic hysterectomy for benign disease: A systematic review and meta-analysis of randomized trials. J. Minim. Invasive Gynecol. 2016, 23, 18–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ind, T.; Laios, A.; Hacking, M.; Nobbenhuis, M. A comparison of operative outcomes between standard and robotic laparoscopic surgery for endometrial cancer: A systematic review and meta-analysis. Int. J. Med Robot. Comput. Assist. Surg. 2017, 13, e1851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goh, B.K.; Chan, C.Y.; Soh, H.L.; Lee, S.Y.; Cheow, P.C.; Chow, P.K.; Ooi, L.L.; Chung, A.Y. A comparison between robotic-assisted laparoscopic distal pancreatectomy versus laparoscopic distal pancreatectomy. Int. J. Med. Robot. 2017, 13, e1733. [Google Scholar] [CrossRef] [PubMed]
- Qu, L.; Zhiming, Z.; Xianglong, T.; Yuanxing, G.; Yong, X.; Rong, L.; Yee, L.W. Short- and mid-term outcomes of robotic versus laparoscopic distal pancreatosplenectomy for pancreatic ductal adenocarcinoma: A retrospective propensity score-matched study. Int. J. Surg. 2018, 55, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Jayne, D.; Pigazzi, A.; Marshall, H.; Croft, J.; Corrigan, N.; Copeland, J.; Quirke, P.; West, N.; Rautio, T.; Thomassen, N.; et al. Effect of robotic-assisted vs conventional laparoscopic surgery on risk of conversion to open laparotomy among patients undergoing resection for rectal cancer: The ROLARR randomized clinical trial. JAMA 2017, 318, 1569–1580. [Google Scholar] [CrossRef]
- Bhama, A.R.; Wafa, A.M.; Ferraro, J.; Collins, S.; Mullard, A.J.; Vandewarker, J.F.; Krapohl, G.; Byrn, J.C.; Cleary, R.K. Comparison of risk factors for unplanned conversion from laparoscopic and robotic to open colorectal surgery using the Michigan surgical quality collaborative (MSQC) database. J. Gastrointest. Surg. 2016, 20, 1223–1230. [Google Scholar] [CrossRef]
- Jones, N.; Fleming, N.D.; Nick, A.M.; Munsell, M.F.; Rallapalli, V.; Westin, S.N.; Meyer, L.A.; Schmeler, K.M.; Ramirez, P.T.; Soliman, P.T. Conversion from robotic surgery to laparotomy: A case-control study evaluating risk factors for conversion. Gynecol. Oncol. 2014, 134, 238–242. [Google Scholar] [CrossRef] [Green Version]
- Unger, C.A.; Lachiewicz, M.P.; Ridgeway, B. Risk factors for robotic gynecologic procedures requiring conversion to other surgical procedures. Int. J. Gynaecol. Obstet. 2016, 135, 299–303. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Francis, N.K.; Curtis, N.J.; Crilly, L.; Noble, E.; Dyke, T.; Hipkiss, R.; Dalton, R.; Allison, A.; Salib, E.; Ockrim, J. Does the number of operating specialists influence the conversion rate and outcomes after laparoscopic colorectal cancer surgery? Surg. Endosc. 2018, 32, 3652–3658. [Google Scholar] [CrossRef] [PubMed]
- Foster, J.D.; Mackenzie, H.; Nelson, H.; Hanna, G.B.; Francis, N.K. Methods of quality assurance in multicenter trials in laparoscopic colorectal surgery: A systematic review. Ann. Surg. 2014, 260, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P.; Ottawa Hospital Research Institute. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.html (accessed on 1 December 2021).
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albassam, A.A.; Mallick, M.S.; Gado, A.; Shoukry, M. Nissen fundoplication, robotic-assisted versus laparoscopic procedure: A comparative study in children. Eur. J. Pediatr. Surg. 2009, 19, 316–319. [Google Scholar] [CrossRef]
- Alfieri, S.; Butturini, G.; Boggi, U.; Pietrabissa, A.; Morelli, L.; Vistoli, F.; Damoli, I.; Peri, A.; Fiorillo, C.; The Italian Robotic pNET Group; et al. Short-term and long-term outcomes after robot-assisted versus laparoscopic distal pancreatectomy for pancreatic neuroendocrine tumors (pNETs): A multicenter comparative study. Langenbeck’s Arch. Surg. 2019, 404, 459–468. [Google Scholar] [CrossRef]
- Alhossaini, R.M.; Altamran, A.A.; Cho, M.; Roh, C.; Seo, W.J.; Choi, S.; Son, T.; Kim, H.-I.; Hyung, W.J. Lower rate of conversion using robotic-assisted surgery compared to laparoscopy in completion total gastrectomy for remnant gastric cancer. Surg. Endosc. 2020, 34, 847–852. [Google Scholar] [CrossRef]
- Alimi, Q.; Peyronnet, B.; Sebe, P.; Cote, J.-F.; Kammerer-Jacquet, S.-F.; Khene, Z.-E.; Pradere, B.; Mathieu, R.; Verhoest, G.; Guillonneau, B.; et al. Comparison of short-term functional, oncological, and perioperative outcomes between laparoscopic and robotic partial nephrectomy beyond the learning curve. J. Laparoendosc. Adv. Surg. Tech. 2018, 28, 1047–1052. [Google Scholar] [CrossRef]
- Ayloo, S.; Buchs, N.C.; Addeo, P.; Bianco, F.M.; Giulianotti, P.C. Robot-assisted sleeve gastrectomy for super-morbidly obese patients. J. Laparoendosc. Adv. Surg. Tech. 2011, 21, 295–299. [Google Scholar] [CrossRef] [Green Version]
- Baek, J.H.; Pastor, C.; Pigazzi, A. Robotic and laparoscopic total mesorectal excision for rectal cancer: A case-matched study. Surg. Endosc. 2011, 25, 521–525. [Google Scholar] [CrossRef]
- Benizri, E.I.; Renaud, M.; Reibel, N.; Germain, A.; Ziegler, O.; Zarnegar, R.; Ayav, A.; Bresler, L.; Brunaud, L. Perioperative outcomes after totally robotic gastric bypass: A prospective nonrandomized controlled study. Am. J. Surg. 2013, 206, 145–151. [Google Scholar] [CrossRef]
- Benway, B.M.; Bhayani, S.B.; Rogers, C.G.; Dulabon, L.M.; Patel, M.N.; Lipkin, M.; Wang, A.J.; Stifelman, M.D. Robot assisted partial nephrectomy versus laparoscopic partial nephrectomy for renal tumors: A multi-institutional analysis of perioperative outcomes. J. Urol. 2009, 182, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Bilgin, I.A.; Bas, M.; Benlice, C.; Esen, E.; Ozben, V.; Aytac, E.; Baca, B.; Hamzaoglu, I.; Karahasanoglu, T. Totally laparoscopic and totally robotic surgery in patients with left-sided colonic diverticulitis. Int. J. Med. Robot. 2020, 16, e2068. [Google Scholar] [CrossRef] [PubMed]
- Boggess, J.F.; Gehrig, P.A.; Cantrell, L.; Shafer, A.; Ridgway, M.; Skinner, E.N.; Fowler, W.C. A comparative study of 3 surgical methods for hysterectomy with staging for endometrial cancer: Robotic assistance, laparoscopy, laparotomy. Am. J. Obstet. Gynecol. 2008, 199, 360.e1–360.e9. [Google Scholar] [CrossRef] [PubMed]
- Buchs, N.C.; Morel, P.; Azagury, D.; Jung, M.K.; Chassot, G.; Huber, O.; Hagen, M.E.; Pugin, F.L. Laparoscopic versus robotic Roux-en-Y gastric bypass: Lessons and long-term follow-up learned from a large prospective monocentric study. Obes. Surg. 2014, 24, 2031–2039. [Google Scholar] [CrossRef] [PubMed]
- Butturini, G.; Damoli, I.; Crepaz, L.; Malleo, G.; Marchegiani, G.; Daskalaki, D.; Esposito, A.; Cingarlini, S.; Salvia, R.; Bassi, C. A prospective non-randomised single-center study comparing laparoscopic and robotic distal pancreatectomy. Surg. Endosc. 2015, 29, 3163–3170. [Google Scholar] [CrossRef] [PubMed]
- Cassini, D.; Depalma, N.; Grieco, M.; Cirocchi, R.; Manoochehri, F.; Baldazzi, G. Robotic pelvic dissection as surgical treatment of complicated diverticulitis in elective settings: A comparative study with fully laparoscopic procedure. Surg. Endosc. 2019, 33, 2583–2590. [Google Scholar] [CrossRef] [PubMed]
- Chiu, L.H.; Chen, C.H.; Tu, P.C.; Chang, C.W.; Yen, Y.K.; Liu, W.M. Comparison of robotic surgery and laparoscopy to perform total hysterectomy with pelvic adhesions or large uterus. J. Minim. Access Surg. 2015, 11, 87–93. [Google Scholar]
- Coronado, P.J.; Herraiz, M.A.; Magrina, J.F.; Fasero, M.; Vidart, J.A. Comparison of perioperative outcomes and cost of robotic-assisted laparoscopy, laparoscopy and laparotomy for endometrial cancer. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 165, 289–294. [Google Scholar] [CrossRef]
- Corrado, G.; Vizza, E.; Cela, V.; Mereu, L.; Bogliolo, S.; Legge, F.; Ciccarone, F.; Mancini, E.; Gallotta, V.; Baiocco, E.; et al. Laparoscopic versus robotic hysterectomy in obese and extremely obese patients with endometrial cancer: A multi-institutional analysis. Eur. J. Surg. Oncol. 2018, 44, 1935–1941. [Google Scholar] [CrossRef]
- Crippa, J.; Grass, F.; Achilli, P.; Mathis, K.L.; Kelley, S.R.; Merchea, A.; Colibaseanu, D.T.; Larson, D.W. Risk factors for conversion in laparoscopic and robotic rectal cancer surgery. Br. J. Surg. 2020, 107, 560–566. [Google Scholar] [CrossRef]
- Cuendis-Velázquez, A.; Trejo-Ávila, M.; Bada-Yllán, O.; Cárdenas-Lailson, E.; Morales-Chávez, C.; Fernández-Álvarez, L.; Romero-Loera, S.; Rojano-Rodríguez, M.; Valenzuela-Salazar, C.; Moreno-Portillo, M. A new era of bile duct repair: Robotic-assisted versus laparoscopic hepaticojejunostomy. J. Gastrointest. Surg. 2019, 23, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.A.; McLemore, E.C.; Abbass, M.A.; Abbas, M.A. Robotic versus laparoscopic resection for sigmoid diverticulitis with fistula. J. Robot. Surg. 2015, 9, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Escobar, P.F.; Frumovitz, M.; Soliman, P.T.; Frasure, H.E.; Fader, A.N.; Schmeler, K.M.; Ramirez, P.T. Comparison of single-port laparoscopy, standard laparoscopy, and robotic surgery in patients with endometrial cancer. Ann. Surg. Oncol. 2012, 19, 1583–1588. [Google Scholar] [CrossRef] [PubMed]
- Esen, E.; Aytac, E.; Ağcaoğlu, O.; Zenger, S.; Balik, E.; Baca, B.; Hamzaoğlu, I.; Karahasanoğlu, T.; Buğra, D. Totally robotic versus totally laparoscopic surgery for rectal cancer. Surg. Laparosc. Endosc. Percutaneous Tech. 2018, 28, 245–249. [Google Scholar] [CrossRef]
- Feroci, F.; Vannucchi, A.; Bianchi, P.P.; Cantafio, S.; Garzi, A.; Formisano, G.; Scatizzi, M. Total mesorectal excision for mid and low rectal cancer: Laparoscopic vs robotic surgery. World J. Gastroenterol. 2016, 22, 3602–3610. [Google Scholar] [CrossRef]
- Gallotta, V.; Conte, C.; Federico, A.; Vizzielli, G.; Alletti, S.G.; Tortorella, L.; Anchora, L.P.; Cosentino, F.; Chiantera, V.; Fagotti, A.; et al. Robotic versus laparoscopic radical hysterectomy in early cervical cancer: A case matched control study. Eur. J. Surg. Oncol. 2018, 44, 754–759. [Google Scholar] [CrossRef]
- Gangemi, A.; Danilkowicz, R.; Elli, F.E.; Bianco, F.; Masrur, M.; Giulianotti, P.C. Could ICG-aided robotic cholecystectomy reduce the rate of open conversion reported with laparoscopic approach? A head to head comparison of the largest single institution studies. J. Robot. Surg. 2017, 11, 77–82. [Google Scholar] [CrossRef]
- Gao, Y.; Xi, H.; Qiao, Z.; Li, J.; Zhang, K.; Xie, T.; Shen, W.; Cui, J.; Wei, B.; Chen, L. Comparison of robotic- and laparoscopic-assisted gastrectomy in advanced gastric cancer: Updated short- and long-term results. Surg. Endosc. 2019, 33, 528–534. [Google Scholar] [CrossRef]
- Göçmen, A.; Şanlıkan, F.; Uçar, M.G. Robot-assisted hysterectomy vs total laparoscopic hysterectomy: A comparison of short-term surgical outcomes. Int. J. Med. Robot. 2012, 8, 453–457. [Google Scholar] [CrossRef]
- Cardenas-Goicoechea, J.; Adams, S.; Bhat, S.B.; Randall, T.C. Surgical outcomes of robotic-assisted surgical staging for endometrial cancer are equivalent to traditional laparoscopic staging at a minimally invasive surgical center. Gynecol. Oncol. 2010, 117, 224–228. [Google Scholar] [CrossRef]
- Gorgun, E.; Ozben, V.; Costedio, M.; Stocchi, L.; Kalady, M.; Remzi, F. Robotic versus conventional laparoscopic rectal cancer surgery in obese patients. Colorectal Dis. 2016, 18, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.D.; Moore, M.D.; Elmously, A.; Bellorin, O.; Zarnegar, R.; Dakin, G.; Pomp, A.; Afaneh, C. Perioperative outcomes of laparoscopic and robotic revisional bariatric surgery in a complex patient population. Obes. Surg. 2018, 28, 1852–1859. [Google Scholar] [CrossRef] [PubMed]
- Guillotreau, J.; Haber, G.-P.; Autorino, R.; Miocinovic, R.; Hillyer, S.; Hernandez, A.; Laydner, H.; Yakoubi, R.; Isac, W.; Long, J.-A.; et al. Robotic partial nephrectomy versus laparoscopic cryoablation for the small renal mass. Eur. Urol. 2012, 61, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, A.V.; Jairam-Thodla, A.; Rademaker, A.; Singh, D.K.; Buttin, B.M.; Lurain, J.R.; Schink, J.C.; Lowe, M.P. The impact of robotics on practice management of endometrial cancer: Transitioning from traditional surgery. Int. J. Med. Robot. 2009, 5, 392–397. [Google Scholar] [CrossRef]
- Holtz, D.O.; Miroshnichenko, G.; Finnegan, M.O.; Chernick, M.; Dunton, C.J. Endometrial cancer surgery costs: Robot vs laparoscopy. J. Minim. Invasive Gynecol. 2010, 17, 500–503. [Google Scholar] [CrossRef]
- Ielpo, B.; Duran, H.; Diaz, E.; Fabra, I.; Caruso, R.; Malavé, L.; Ferri, V.; Nuñez, J.; Ruiz-Ocaña, A.; Jorge, E.; et al. Robotic versus laparoscopic surgery for rectal cancer: A comparative study of clinical outcomes and costs. Int. J. Colorectal Dis. 2017, 32, 1423–1429. [Google Scholar] [CrossRef]
- Johnson, L.; Bunn, W.D.; Nguyen, L.; Rice, J.; Raj, M.; Cunningham, M.J. Clinical comparison of robotic, laparoscopic, and open hysterectomy procedures for endometrial cancer patients. J. Robot. Surg. 2017, 11, 291–297. [Google Scholar] [CrossRef]
- Karabulut, K.; Agcaoglu, O.; Aliyev, S.; Siperstein, A.; Berber, E. Comparison of intraoperative time use and perioperative outcomes for robotic versus laparoscopic adrenalectomy. Surgery 2012, 151, 537–542. [Google Scholar] [CrossRef]
- Kilic, G.S.; Moore, G.; Elbatanony, A.; Radecki, C.; Phelps, J.Y.; Borahay, M.A. Comparison of perioperative outcomes of total laparoscopic and robotically assisted hysterectomy for benign pathology during introduction of a robotic program. Obstet. Gynecol. Int. 2011, 2011, 683703. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.C.; Lee, J.L.; Yoon, Y.S.; Kim, C.W.; Park, I.J.; Lim, S.B. Robotic left colectomy with complete mesocolectomy for splenic flexure and descending colon cancer, compared with a laparoscopic procedure. Int. J. Med. Robot. 2018, 14, e1918. [Google Scholar] [CrossRef]
- Kim, Y.-W.; Reim, D.; Park, J.Y.; Eom, B.W.; Kook, M.-C.; Ryu, K.W.; Yoon, H.M. Role of robot-assisted distal gastrectomy compared to laparoscopy-assisted distal gastrectomy in suprapancreatic nodal dissection for gastric cancer. Surg. Endosc. 2016, 30, 1547–1552. [Google Scholar] [CrossRef]
- Kong, Y.; Cao, S.; Liu, X.; Li, Z.; Wang, L.; Lu, C.; Shen, S.; Zhu, H.; Zhou, Y. Short-term clinical outcomes after laparoscopic and robotic gastrectomy for gastric cancer: A propensity score matching analysis. J. Gastrointest. Surg. 2020, 24, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Khrucharoen, U.; Juo, Y.Y.; Chen, Y.; Jimenez, J.C.; Dutson, E.P. Short- and intermediate-term clinical outcome comparison between laparoscopic and robotic-assisted median arcuate ligament release. J. Robot. Surg. 2020, 14, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Law, W.L.; Foo, D.C.C. Comparison of short-term and oncologic outcomes of robotic and laparoscopic resection for mid- and distal rectal cancer. Surg. Endosc. 2017, 31, 2798–2807. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Allen, P.J.; Sadot, E.; D’Angelica, M.I.; DeMatteo, R.P.; Fong, Y.; Jarnagin, W.R.; Kingham, T.P. Distal pancreatectomy: A single institution’s experience in open, laparoscopic, and robotic approaches. J. Am. Coll. Surg. 2015, 220, 18–27. [Google Scholar] [CrossRef]
- Leitao, M.M., Jr.; Briscoe, G.; Santos, K.; Winder, A.; Jewell, E.L.; Hoskins, W.J.; Chi, D.S.; Abu-Rustum, N.R.; Sonoda, Y.; Brown, C.L.; et al. Introduction of a computer-based surgical platform in the surgical care of patients with newly diagnosed uterine cancer: Outcomes and impact on approach. Gynecol. Oncol. 2012, 125, 394–399. [Google Scholar] [CrossRef]
- Lim, P.C.; Kang, E.; Park, D.H. A comparative detail analysis of the learning curve and surgical outcome for robotic hysterectomy with lymphadenectomy versus laparoscopic hysterectomy with lymphadenectomy in treatment of endometrial cancer: A case-matched controlled study of the first one hundred twenty two patients. Gynecol. Oncol. 2011, 120, 413–418. [Google Scholar]
- Liu, R.; Zhang, T.; Zhao, Z.M.; Tan, X.L.; Zhao, G.D.; Zhang, X.; Xu, Y. The surgical outcomes of robot-assisted laparoscopic pancreaticoduodenectomy versus laparoscopic pancreaticoduodenectomy for periampullary neoplasms: A comparative study of a single center. Surg. Endosc. 2017, 31, 2380–2386. [Google Scholar] [CrossRef]
- Mäenpää, M.M.; Nieminen, K.; Tomás, E.I.; Laurila, M.; Luukkaala, T.H.; Mäenpää, J.U. Robotic-assisted vs traditional laparoscopic surgery for endometrial cancer: A randomized controlled trial. Am. J. Obstet. Gynecol. 2016, 215, 588.e1–588.e7. [Google Scholar] [CrossRef] [Green Version]
- Mantoo, S.; Podevin, J.; Regenet, N.; Rigaud, J.; Lehur, P.A.; Meurette, G. Is robotic-assisted ventral mesh rectopexy superior to laparoscopic ventral mesh rectopexy in the management of obstructed defaecation? Colorectal Dis. 2013, 15, e469–e475. [Google Scholar] [CrossRef]
- Mehmood, R.K.; Parker, J.; Bhuvimanian, L.; Qasem, E.; Mohammed, A.A.; Zeeshan, M.; Grugel, K.; Carter, P.; Ahmed, S. Short-term outcome of laparoscopic versus robotic ventral mesh rectopexy for full-thickness rectal prolapse. Is robotic superior? Int. J. Colorectal Dis. 2014, 29, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Montalti, R.; Scuderi, V.; Patriti, A.; Vivarelli, M.; Troisi, R.I. Robotic versus laparoscopic resections of posterosuperior segments of the liver: A propensity score-matched comparison. Surg. Endosc. 2016, 30, 1004–1013. [Google Scholar] [CrossRef] [PubMed]
- Morelli, L.; Tartaglia, D.; Bronzoni, J.; Palmeri, M.; Guadagni, S.; Gennai, A.; Bianchini, M.; Bastiani, L.; Moglia, A.; Fommei, E.; et al. Robotic assisted versus pure laparoscopic surgery of the adrenal glands: A case-control study comparing surgical techniques. Langenbeck’s Arch. Surg. 2016, 401, 999–1006. [Google Scholar] [CrossRef] [PubMed]
- Najafi, N.; Mintziras, I.; Wiese, D.; Albers, M.B.; Maurer, E.; Bartsch, D.K. A retrospective comparison of robotic versus laparoscopic distal resection and enucleation for potentially benign pancreatic neoplasms. Surg. Today 2020, 50, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Nezhat, F.R.; Finger, T.N.; Vetere, P.; Radjabi, A.R.; Vega, M.; Averbuch, L.; Khalil, S.; Altinbas, S.K.; Lax, D. Comparison of perioperative outcomes and complication rates between conventional versus robotic-assisted laparoscopy in the evaluation and management of early, advanced, and recurrent stage ovarian, fallopian tube, and primary peritoneal cancer. Int. J. Gynecol. Cancer 2014, 24, 600–607. [Google Scholar] [CrossRef]
- Niglio, A.; Grasso, M.; Costigliola, L.; Zenone, P.; De Palma, M. Laparoscopic and robot-assisted transperitoneal lateral adrenalectomy: A large clinical series from a single center. Updates Surg. 2020, 72, 193–198. [Google Scholar] [CrossRef]
- Ozben, V.; De Muijnck, C.; Karabork, M.; Ozoran, E.; Zenger, S.; Bilgin, I.A.; Aytac, E.; Baca, B.; Balik, E.; Hamzaoglu, I.; et al. The da Vinci Xi system for robotic total/subtotal colectomy vs. conventional laparoscopy: Short-term outcomes. Tech. Coloproctol. 2019, 23, 861–868. [Google Scholar] [CrossRef]
- Park, J.Y.; Ryu, K.W.; Reim, D.; Eom, B.W.; Yoon, H.M.; Rho, J.Y.; Choi, I.J.; Kim, Y.-W. Robot-assisted gastrectomy for early gastric cancer: Is it beneficial in viscerally obese patients compared to laparoscopic gastrectomy? World J. Surg. 2015, 39, 1789–1797. [Google Scholar] [CrossRef]
- Ramji, K.M.; Cleghorn, M.C.; Josse, J.M.; MacNeill, A.; O’brien, C.; Urbach, D.; Quereshy, F.A. Comparison of clinical and economic outcomes between robotic, laparoscopic, and open rectal cancer surgery: Early experience at a tertiary care center. Surg. Endosc. 2016, 30, 1337–1343. [Google Scholar] [CrossRef]
- Rencuzogullari, A.; Gorgun, E.; Costedio, M.; Aytac, E.; Kessler, H.; Abbas, M.A.; Remzi, F.H. Case-matched comparison of robotic versus laparoscopic proctectomy for inflammatory bowel disease. Surg. Laparosc. Endosc. Percutaneous Tech. 2016, 26, e37–e40. [Google Scholar] [CrossRef]
- Seror, J.; Bats, A.S.; Huchon, C.; Bensaïd, C.; Douay-Hauser, N.; Lécuru, F. Laparoscopy vs robotics in surgical management of endometrial cancer: Comparison of intraoperative and postoperative complications. J. Minim. Invasive Gynecol. 2014, 21, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.L.; Krivak, T.C.; Scott, E.M.; Rauh-Hain, J.A.; Sukumvanich, P.; Olawaiye, A.B.; Richard, S.D. Dual-console robotic surgery compared to laparoscopic surgery with respect to surgical outcomes in a gynecologic oncology fellowship program. Gynecol. Oncol. 2012, 126, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Spinoglio, G.; Bianchi, P.P.; Marano, A.; Priora, F.; Lenti, L.M.; Ravazzoni, F.; Petz, W.; Borin, S.; Ribero, D.; Formisano, G.; et al. Robotic versus laparoscopic right colectomy with complete mesocolic excision for the treatment of colon cancer: Perioperative outcomes and 5-year survival in a consecutive series of 202 patients. Ann. Surg. Oncol. 2018, 25, 3580–3586. [Google Scholar] [CrossRef]
- Troisi, R.I.; Patriti, A.; Montalti, R.; Casciola, L. Robot assistance in liver surgery: A real advantage over a fully laparoscopic approach? Results of a comparative bi-institutional analysis. Int. J. Med. Robot. 2013, 9, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Turunen, H.; Pakarinen, P.; Sjöberg, J.; Loukovaara, M. Laparoscopic vs robotic-assisted surgery for endometrial carcinoma in a centre with long laparoscopic experience. J. Obstet. Gynaecol. 2013, 33, 720–724. [Google Scholar] [CrossRef]
- Vasilescu, C.; Stanciulea, O.; Tudor, S. Laparoscopic versus robotic subtotal splenectomy in hereditary spherocytosis. Potential advantages and limits of an expensive approach. Surg. Endosc. 2012, 26, 2802–2809. [Google Scholar] [CrossRef]
- Wang, A.J.; Bhayani, S.B. Robotic partial nephrectomy versus laparoscopic partial nephrectomy for renal cell carcinoma: Single-surgeon analysis of >100 consecutive procedures. Urology 2009, 73, 306–310. [Google Scholar] [CrossRef]
- Wang, Z.Z.; Tang, W.B.; Hu, M.G.; Zhao, Z.M.; Zhao, G.D.; Li, C.G.; Tan, X.L.; Zhang, X.; Lau, W.Y.; Liu, R. Robotic vs laparoscopic hemihepatectomy: A comparative study from a single center. J. Surg. Oncol. 2019, 120, 646–653. [Google Scholar] [CrossRef]
- Warren, J.A.; Cobb, W.S.; Ewing, J.A.; Carbonell, A.M. Standard laparoscopic versus robotic retromuscular ventral hernia repair. Surg. Endosc. 2017, 31, 324–332. [Google Scholar] [CrossRef]
- Wong, M.T.; Meurette, G.; Rigaud, J.; Regenet, N.; Lehur, P.A. Robotic versus laparoscopic rectopexy for complex rectocele: A prospective comparison of short-term outcomes. Dis. Colon. Rectum. 2011, 54, 342–346. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Kinugasa, Y.; Shiomi, A.; Tomioka, H.; Kagawa, H.; Yamakawa, Y. Robotic-assisted vs. conventional laparoscopic surgery for rectal cancer: Short-term outcomes at a single center. Surg. Today 2016, 46, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Lu, Q.; Campi, R.; Ji, C.; Guo, S.; Liu, G.; Zhang, S.; Li, X.; Gan, W.; Minervini, A.; et al. Endoscopic robot-assisted simple enucleation versus laparoscopic simple enucleation with single-layer renorrhaphy in localized renal tumors: A propensity score-matched analysis from a high-volume centre. Urology 2018, 121, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, J.O.; Adhikari, N.K.; Beyene, J. Inclusion of zero total event trials in meta-analyses maintains analytic consistency and incorporates all available data. BMC Med. Res. Methodol. 2007, 7, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furukawa, T.A.; Barbui, C.; Cipriani, A.; Brambilla, P.; Watanabe, N. Imputing missing standard deviations in meta-analyses can provide accurate results. J. Clin. Epidemiol. 2006, 59, 7–10. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Thompson, S.G.; Sharp, S.J. Explaining heterogeneity in meta-analysis: A comparison of methods. Stat. Med. 1999, 18, 2693–2708. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Milone, M.; Manigrasso, M.; Burati, M.; Elmore, U.; Gennarelli, N.; Giglio, M.C.; Maione, F.; Musella, M.; Conte, V.L.; Milone, F.; et al. Intracorporeal versus extracorporeal anastomosis after laparoscopic gastrectomy for gastric cancer. A systematic review with meta-analysis. J. Visc. Surg. 2019, 156, 305–318. [Google Scholar] [CrossRef]
- Milone, M.; Vignali, A.; Milone, F.; Pignata, G.; Elmore, U.; Musella, M.; De Placido, G.; Mollo, A.; Fernandez, L.M.S.; Coretti, G.; et al. Colorectal resection in deep pelvic endometriosis: Surgical technique and post-operative complications. World J. Gastroenterol. 2015, 21, 13345–13351. [Google Scholar] [CrossRef]
- Milone, M.; Manigrasso, M.; Burati, M.; Velotti, N.; Milone, F.; De Palma, G.D. Surgical resection for rectal cancer. Is laparoscopic surgery as successful as open approach? A systematic review with meta-analysis. PLoS ONE 2018, 13, e0204887. [Google Scholar]
- Milone, M.; Elmore, U.; Vignali, A.; Gennarelli, N.; Manigrasso, M.; Burati, M.; Milone, F.; De Palma, G.D.; DelRio, P.; Rosati, R. Recovery after intracorporeal anastomosis in laparoscopic right hemicolectomy: A systematic review and meta-analysis. Langenbeck’s Arch. Surg. 2018, 403, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Inomata, M.; Kakisako, K.; Shiraishi, N.; Adachi, Y.; Kitano, S. Surgical technique influences bowel function after low anterior resection and sigmoid colectomy. Hepatogastroenterology 2003, 50, 1381–1384. [Google Scholar] [PubMed]
- Papanikolaou, I.G. Robotic surgery for colorectal cancer: Systematic review of the literature. Surg. Laparosc. Endosc. Percutaneous Tech. 2014, 24, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.J.; Wong, M.J.; Choi, G.H.; Wu, Y.M.; Lai, P.B.; Goh, B.K.P. Systematic review and meta-analysis of robotic versus open hepatectomy. ANZ J. Surg. 2019, 89, 165–170. [Google Scholar] [CrossRef]
- Advincula, A.P.; Song, A. The role of robotic surgery in gynecology. Curr. Opin. Obstet. Gynecol. 2007, 19, 331–336. [Google Scholar] [CrossRef]
- Boylu, U.; Oommen, M.; Raynor, M.; Lee, B.R.; Thomas, R. Robot-assisted laparoscopic radical prostatectomy in patients with previous abdominal surgery: A novel laparoscopic adhesiolysis technique. J. Endourol. 2010, 24, 229–232. [Google Scholar] [CrossRef]
- Petros, F.G.; Patel, M.N.; Kheterpal, E.; Siddiqui, S.; Ross, J.; Bhandari, A.; Diaz, M.; Menon, M.; Rogers, C.G. Robotic partial nephrectomy in the setting of prior abdominal surgery. BJU Int. 2011, 108, 413–419. [Google Scholar] [CrossRef]
- Gkegkes, I.D.; Mamais, I.A.; Iavazzo, C. Robotics in general surgery: A systematic cost assessment. J. Minim. Access Surg. 2017, 13, 243–255. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Selection | Comparability | Outcome | Total | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of Exposed Cohort | Selection of the Non-Exposed Cohort | Ascertainment of Exposure | Outcome Not Present at the Start of the Study | Assessment of Outcome | Length of Follow-Up | Adequacy of Follow-Up | |||
| Albassam A.A. et al., 2009 [25] | * | * | * | * | * | * | * | ******* | |
| Alfieri S. et al., 2019 [26] | * | * | * | * | ** | * | * | * | ********* |
| Alhossaini R.M. et al., 2019 [27] | * | * | * | * | * | * | * | * | ******** |
| Alimi Q. et al., 2018 [28] | * | * | * | * | * | * | * | ******* | |
| Ayloo S. et al., 2011 [29] | * | * | * | * | * | * | * | ******* | |
| Beak J. et al., 2010 [30] | * | * | * | * | ** | * | * | * | ********* |
| Benizri E.I. et al., 2013 [31] | * | * | * | * | * | * | * | ******* | |
| Benway B.M. et al., 2009 [32] | * | * | * | * | * | * | * | ******* | |
| Bilgin I.A. et al., 2019 [33] | * | * | * | ** | * | * | * | ******** | |
| Boggess J.F. et al., 2008 [34] | * | * | * | * | * | * | * | ******* | |
| Buchs N.C. et al., 2014 [35] | * | * | * | ** | * | * | * | ******** | |
| Butturini G. et al., 2014 [36] | * | * | * | * | ** | * | * | * | ********* |
| Cassini D. et al., 2018 [37] | * | * | * | * | ** | * | * | * | ********* |
| Chiu L.H. et al., 2015 [38] | * | * | * | * | * | * | * | * | ******** |
| Coronado P.J. et al., 2012 [39] | * | * | * | ** | * | * | * | ******** | |
| Corrado G. et al., 2018 [40] | * | * | * | * | * | * | * | ******* | |
| Crippa J. et al., 2019 [41] | * | * | * | ** | * | * | * | ******** | |
| Cuendis-Velazquez A. et al., 2018 [42] | * | * | * | * | * | * | * | * | ******** |
| Elliott P.A. et al., 2015 [43] | * | * | * | * | ** | * | * | * | ********* |
| Escobar F. et al., 2011 [44] | * | * | * | * | * | * | * | ******* | |
| Esen E. et al., 2018 [45] | * | * | * | * | ** | * | * | * | ********* |
| Feroci F. et al., 2016 [46] | * | * | * | ** | * | * | * | ******** | |
| Gallotta V. et al., 2018 [47] | * | * | * | * | * | * | * | * | ******** |
| Gangemi A. et al., 2017 [48] | * | * | * | ** | * | * | * | ******** | |
| Gao Y. et al., 2018 [49] | * | * | * | * | ** | * | * | * | ********* |
| Goçmen A. et al., 2012 [50] | * | * | * | * | * | * | * | * | ******** |
| Goh B.K.P. et al., 2016 [13] | * | * | * | * | ** | * | * | * | ********* |
| Golcoechea J.C. et al., 2010 [51] | * | * | * | * | * | * | * | * | ******** |
| Gorgun E. et al., 2016 [52] | * | * | * | * | ** | * | * | * | ********* |
| Gray K.D. et al., 2018 [53] | * | * | * | * | ** | * | * | * | ********* |
| Guillotrean et al., 2012 [54] | * | * | * | ** | * | * | * | ******** | |
| Hoekstra A.V. et al., 2009 [55] | * | * | * | ** | * | * | * | ******** | |
| Holz D.O. et al., 2010 [56] | * | * | * | * | * | * | * | ******* | |
| Ielpo B. et al., 2014 [57] | * | * | * | ** | * | * | * | ******** | |
| Johnson L. et al., 2016 [58] | * | * | * | * | ** | * | * | * | ********* |
| Karabulut K.K. et al., 2012 [59] | * | * | * | * | * | * | * | * | ******** |
| Kilic G. et al., 2011 [60] | * | * | * | * | * | * | * | * | ******** |
| Kim J.C. et al., 2018 [61] | * | * | * | * | ** | * | * | * | ********* |
| Kim Y.W. et al., 2015 [62] | * | * | * | * | * | * | * | * | ******** |
| Kong Y. et al., 2019 [63] | * | * | * | * | ** | * | * | * | ********* |
| Krucharoen U. et al., 2019 [64] | * | * | * | ** | * | * | * | ******** | |
| Law W.L. et al., 2016 [65] | * | * | * | * | ** | * | * | * | ********* |
| Lee S.Y. et al., 2014 [66] | * | * | * | ** | * | * | * | ******** | |
| Leitao M.M. et al., 2012 [67] | * | * | * | * | * | * | * | ******* | |
| Lim P.C. et al., 2010 [68] | * | * | * | * | * | * | * | ******* | |
| Liu et al., 2016 [69] | * | * | * | * | * | * | * | ******* | |
| Maenpaa M.M. et al., 2016 [70] | * | * | * | * | * | * | * | * | ******** |
| Mantoo S. et al., 2013 [71] | * | * | * | ** | * | * | * | ******** | |
| Mehmood R.K. et al., 2014 [72] | * | * | * | * | * | * | * | * | ******** |
| Montalti R. et al., 2014 [73] | * | * | * | ** | * | * | * | ******** | |
| Morelli L. et al., 2016 [74] | * | * | * | * | * | * | * | ******* | |
| Najafi N. et al., 2020 [75] | * | * | * | * | ** | * | * | * | ********* |
| Nezhat F.R. et al., 2014 [76] | * | * | * | * | * | * | * | * | ******** |
| Niglio A. et al., 2019 [77] | * | * | * | ** | * | * | * | ******** | |
| Ozben V. et al., 2019 [78] | * | * | * | * | ** | * | * | * | ********* |
| Park J.Y. et al., 2015 [79] | * | * | * | * | * | * | * | ******* | |
| Ramji K.M. et al., 2015 [80] | * | * | * | * | * | * | * | * | ******** |
| Rencuzogullari A. et al., 2016 [81] | * | * | * | ** | * | * | * | ******** | |
| Seror J. et al., 2016 [82] | * | * | * | * | ** | * | * | * | ********* |
| Smith A.L. 2012 [83] | * | * | * | * | * | * | * | * | ******** |
| Spinoglio G. et al., 2018 [84] | * | * | * | * | ** | * | * | * | ********* |
| Troisi R.I. et al., 2013 [85] | * | * | * | * | * | * | * | ******* | |
| Turunen H. et al., 2013 [86] | * | * | * | ** | * | * | * | ******** | |
| Vasilescu C. et al., 2012 [87] | * | * | * | * | * | * | * | ******* | |
| Wang A.J. et al., 2009 [88] | * | * | * | ** | * | * | * | ******** | |
| Wang Z.Z. et al., 2019 [89] | * | * | * | * | ** | * | * | * | ********* |
| Warren J.A. et al., 2016 [90] | * | * | * | * | ** | * | * | * | ********* |
| Wong M.T.C. et al., 2011 [91] | * | * | * | * | * | * | * | ******* | |
| Yamaguchi T. et al., 2015 [92] | * | * | * | * | ** | * | * | * | ********* |
| Zhao X. et al., 2018 [93] | * | * | * | * | * | * | * | ******* | |
| Study | Design | Patients | Surgical Field | Pathology | Procedure | Expertise | |
|---|---|---|---|---|---|---|---|
| Lap | Rob | ||||||
| Albassam A.A., 2009 [25] | Retrospective | 25 | 25 | Oesophago-gastric | GERD | Nissen fundoplication | Expert |
| Alfieri S. et al., 2019 [26] | Retrospective | 85 | 96 | Pancreatic | pNETs | Distal pancreatectomy | Expert |
| Alhossaini R.M. et al., 2019 [27] | Retrospective | 30 | 25 | Oesophago-gastric | Remnant gastric cancer | Completion total gastrectomy | NR |
| Alimi Q. et al., 2018 [28] | Prospective | 50 | 50 | Urologic | Renal tumour | Partial nephrectomy | Expert |
| Ayloo S. et al., 2011 [29] | Prospective | 39 | 30 | Oesophago-gastric | Morbid obesity | Sleeve gastrectomy | NR |
| Beak J. et al., 2010 [30] | Prospective | 41 | 41 | Colorectal | Rectal cancer | Rectal resection with TME | Early |
| Benizri E.I. et al., 2013 [31] | Prospective | 100 | 100 | Oesophago-gastric | Morbid obesity | Roux-en-Y gastric bypass | Expert |
| Benway B.M. [32] | Retrospective | 118 | 129 | Urologic | Renal tumour | Partial nephrectomy | Expert |
| Bilgin I.A. et al., 2019 [33] | Retrospective | 22 | 20 | Colorectal | Diverticular disease | Sigmoidectomy | Expert |
| Boggess J.F. et al., 2008 [34] | Prospective | 81 | 103 | Gynaecologic | Endometrial cancer | Hysterectomy | Early |
| Buchs N.C. et al., 2014 [35] | Prospective | 389 | 388 | Oesophago-gastric | Morbid obesity | Roux-en-Y gastric bypass | Expert |
| Butturini G. et al., 2014 [36] | Prospective | 21 | 22 | Pancreatic | Pancreatic tumours | Distal pancreatectomy | Expert |
| Cassini D. et al., 2018 [37] | Retrospective | 92 | 64 | Colorectal | Diverticular disease | Sigmoidectomy | Expert |
| Chiu L.H. et al., 2015 [38] | Prospective | 128 | 88 | Gynaecologic | Benign pathology or carcinoma IS | Hysterectomy | NR |
| Coronado P.J. et al., 2012 [39] | Retrospective | 84 | 71 | Gynaecologic | Endometrial cancer | Hysterectomy with bilateral salpingo-oophorectomy | NR |
| Corrado G. et al., 2018 [40] | Retrospective | 406 | 249 | Gynaecologic | Low-grade endometrial carcinoma | Hysterectomy | Expert |
| Crippa J. et al., 2019 [41] | Retrospective | 283 | 317 | Colorectal | Rectal cancer | LAR or APR with TME | Expert |
| Cuendis-Velazquez A. et al., 2018 [42] | Retrospective | 40 | 35 | Hepatobiliary | Bile duct injury | Hepaticojejunostomy | NR |
| Elliott P.A. et al., 2015 [43] | Retrospective | 20 | 11 | Colorectal | Diverticulitis | Sigmoidectomy | Expert |
| Escobar P.F. et al., 2011 [44] | Retrospective | 30 | 30 | Gynaecologic | Endometrial cancer | Hysterectomy | Expert |
| Esen E. et al., 2018 [45] | Retrospective | 78 | 100 | Colorectal | Rectal cancer | Rectal resection with TME | Expert |
| Feroci F. et al., 2016 [46] | Retrospective | 58 | 53 | Colorectal | Rectal cancer | Rectal resection with TME | Expert |
| Gallotta V. et al., 2018 [47] | Retrospective | 140 | 70 | Gynaecologic | Early cervical cancer | Hysterectomy | Expert |
| Gangemi A. et al., 2017 [48] | Retrospective | 289 | 676 | Hepatobiliary | Cholelithiasis/cholecystitis | Cholecystectomy | Expert |
| Gao Y. et al., 2018 [49] | Retrospective | 163 | 163 | Oesophago-gastric | Gastric cancer | Partial and total gastrectomy | Expert |
| Goh B.K.P. et al., 2016 [13] | Retrospective | 31 | 8 | Pancreatic | Pancreatic tumours | Distal pancreatectomy | Early |
| Goioechea J.C. et al., 2010 [51] | Retrospective | 173 | 102 | Gynaecologic | Endometrial cancer | Hysterectomy | Expert |
| Gorgun E. et al., 2016 [52] | Retrospective | 27 | 29 | Colorectal | Rectal cancer in obese patients | LAR and APR | NR |
| Goçmen A. et al., 2012 [50] | Prospective | 60 | 60 | Gynaecologic | Benign gynaecologic disease | Hysterectomy | NR |
| Gray K.D. et al., 2018 [53] | Retrospective | 66 | 18 | Oesophago-gastric | Revision of bariatric surgery | AGB, VSG, RYGB, VBG | Expert |
| Guillotrean J. et al., 2012 [54] | Prospective | 226 | 210 | Urologic | Small renal mass | Partial nephrectomy | NR |
| Hoekstra A.V. et al., 2009 [55] | Prospective | 7 | 32 | Gynaecologic | Endometrial cancer | Hysterectomy with bilateral salpingo-oophorectomy | Expert |
| Holtz D.O. et al., 2019 [56] | Retrospective | 20 | 13 | Gynaecologic | Endometrial cancer | Hysterectomy with bilateral salpingo-oophorectomy | Expert |
| Ielpo B. et al., 2017 [57] | Retrospective | 112 | 86 | Colorectal | Rectal cancer | Rectal resection | Expert |
| Johnson L. et al., 2016 [58] | Retrospective | 187 | 353 | Gynaecologic | Endometrial cancer | Hysterectomy | NR |
| Karabulut K.K. et al., 2012 [59] | Prospective | 50 | 50 | Endocrine | Pheochromocytoma | Adrenalectomy | Expert |
| Kilic G.S. et al., 2011 [60] | Prospective | 34 | 25 | Gynaecologic | Benign gynaecologic disease | Hysterectomy | Expert |
| Kim J.C. et al., 2018 [61] | Prospective | 53 | 20 | Colorectal | Colon cancer | Left colectomy | NR |
| Kim Y.W. et al., 2015 [62] | Prospective | 288 | 87 | Oesophago-gastric | Gastric cancer | Distal gastrectomy | Expert |
| Kong Y. et al., 2019 [63] | Retrospective | 532 | 266 | Oesophago-gastric | Gastric cancer | Partial and total gastrectomy | Expert |
| Krucharoen U. et al., 2019 [64] | Retrospective | 16 | 18 | Vascular | Median arcuate ligament syndrome | MAL release | Expert |
| Law W.L. et al., 2016 [65] | Prospective | 171 | 220 | Colorectal | Rectal cancer | Hartmann procedure, LAR and APR | NR |
| Lee S.Y. et al., 2014 [66] | Retrospective | 131 | 37 | Pancreatic | Pancreatic tumours | Distal pancreatectomy | Expert |
| Leitao M.M. et al., 2012 [67] | Retrospective | 302 | 347 | Gynaecologic | Uterine cancer | Hysterectomy | Expert |
| Lim P.C. et al., 2019 [68] | Retrospective | 122 | 122 | Gynaecologic | Endometrial cancer | Hysterectomy | Expert |
| Liu et al., 2016 [69] | Retrospective | 25 | 27 | Pancreatic | Periampullary neoplasms | PD | Expert |
| Maenpaa M.M. et al., 2016 [70] | Rct | 48 | 51 | Gynaecologic | Low-grade endometrial carcinoma | Hysterectomy | Expert |
| Mantoo S. et al., 2013 [71] | Retrospective | 74 | 44 | Colorectal | Obstructed defecation | Ventral mesh rectopexy | NR |
| Mehmood R.K. et al., 2014 [72] | Prospective | 34 | 17 | Colorectal | Rectal prolapse | Ventral mesh rectopexy | NR |
| Montalti R. et al., 2015 [73] | Retrospective | 72 | 36 | Hepatobiliary | Liver diseases | Posterosuperior segments resection | Expert |
| Morelli L. et al., 2016 [74] | Retrospective | 41 | 41 | Endocrine | Benign or malignant adrenal tumour | Adrenalectomy | Expert |
| Najafi N. et al., 2020 [75] | Retrospective | 40 | 35 | Pancreatic | Benign and borderline tumours | Distal pancreatic resection and enucleation | NR |
| Nezhat F.R. et al., 2014 [76] | Retrospective | 13 | 9 | Gynaecologic | Early ovarian cancer | Salpingo-oophorectomy | NR |
| Niglio A. et al., 2019 [77] | Retrospective | 64 | 40 | Endocrine | Adrenal cancer | Adrenalectomy | NR |
| Ozben V. et al., 2019 [78] | Retrospective | 56 | 26 | Colorectal | Benign or malignant pathology | Subtotal or total colectomy | Expert |
| Park J.Y. et al., 2015 [79] | Retrospective | 622 | 148 | Oesophago-gastric | Early gastric cancer | Partial and total gastrectomy | Expert |
| Ramji K.M. et al., 2015 [80] | Retrospective | 27 | 26 | Colorectal | Rectal cancer | Rectal resection | Early |
| Rencuzogullari A. et al., 2016 [81] | Retrospective | 21 | 21 | Colorectal | IBD | Proctectomy | Early |
| Seror J et al., 2013 [82] | Retrospective | 106 | 40 | Gynaecologic | Endometrial cancer | Hysterectomy with bilateral salpingo-oophorectomy | Expert |
| Smith A.L. et al., 2012 [83] | Retrospective | 106 | 116 | Gynaecologic | Endometrial cancer | Hysterectomy | Early |
| Spinoglio G. et al., 2018 [84] | Retrospective | 100 | 100 | Colorectal | Right colon cancer | Right colectomy with CME | Expert |
| Troisi R.I. et al., 2013 [85] | Retrospective | 223 | 40 | Hepatobiliary | Liver diseases | Liver resection | Expert |
| Turunen H. et al., 2013 [86] | Retrospective | 150 | 67 | Gynaecologic | Endometrial cancer | Hysterectomy | Expert |
| Vasilescu C. et al., 2012 [87] | Retrospective | 22 | 10 | Splenic | Hereditary spherocytosis | Splenectomy | NR |
| Wang A.J. et al., 2009 [88] | Retrospective | 62 | 40 | Urologic | Renal cell carcinoma | Partial nephrectomy | Expert |
| Wang Z.Z. et al., 2019 [89] | Retrospective | 48 | 92 | Hepatobiliary | Benign or malignant hepatic lesions | Hemiepatectomy | Expert |
| Warren J.A. et al., 2016 [90] | Retrospective | 103 | 53 | Abdominal wall | Ventral hernia | Ventral hernia repair | NR |
| Wong M.T.C. et al., 2011 [91] | Prospective | 40 | 23 | Colorectal | Complex rectocele | Ventral mesh rectopexy | Expert |
| Yamaguchi T. et al., 2015 [92] | Retrospective | 239 | 203 | Colorectal | Rectal cancer | Rectal resection | Expert |
| Zhao X. et al., 2018 [93] | Retrospective | 101 | 101 | Urologic | Renal tumour | Simple enucleation with single layer renorrhaphy | Expert |
| Covariates | p Value |
|---|---|
| Mean age | 0.67 |
| Female gender | 0.5 |
| BMI | 0.99 |
| ASA Score I | 0.44 |
| ASA Score II | 0.92 |
| Tumour stage II | 0.36 |
| Tumour stage IV | 0.22 |
| Previous abdominal surgery | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milone, M.; Manigrasso, M.; Anoldo, P.; D’Amore, A.; Elmore, U.; Giglio, M.C.; Rompianesi, G.; Vertaldi, S.; Troisi, R.I.; Francis, N.K.; et al. The Role of Robotic Visceral Surgery in Patients with Adhesions: A Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 307. https://doi.org/10.3390/jpm12020307
Milone M, Manigrasso M, Anoldo P, D’Amore A, Elmore U, Giglio MC, Rompianesi G, Vertaldi S, Troisi RI, Francis NK, et al. The Role of Robotic Visceral Surgery in Patients with Adhesions: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(2):307. https://doi.org/10.3390/jpm12020307
Chicago/Turabian StyleMilone, Marco, Michele Manigrasso, Pietro Anoldo, Anna D’Amore, Ugo Elmore, Mariano Cesare Giglio, Gianluca Rompianesi, Sara Vertaldi, Roberto Ivan Troisi, Nader K. Francis, and et al. 2022. "The Role of Robotic Visceral Surgery in Patients with Adhesions: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 2: 307. https://doi.org/10.3390/jpm12020307
APA StyleMilone, M., Manigrasso, M., Anoldo, P., D’Amore, A., Elmore, U., Giglio, M. C., Rompianesi, G., Vertaldi, S., Troisi, R. I., Francis, N. K., & De Palma, G. D. (2022). The Role of Robotic Visceral Surgery in Patients with Adhesions: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 12(2), 307. https://doi.org/10.3390/jpm12020307