
Improved Music Perception after Music Therapy following Cochlear Implantation in the Elderly Population




Abstract
:1. Introduction
2. Material and Methods
2.1. Study Cohort
2.2. Pre- and Post-Design (before and after 10 MT Sessions)
- (a)
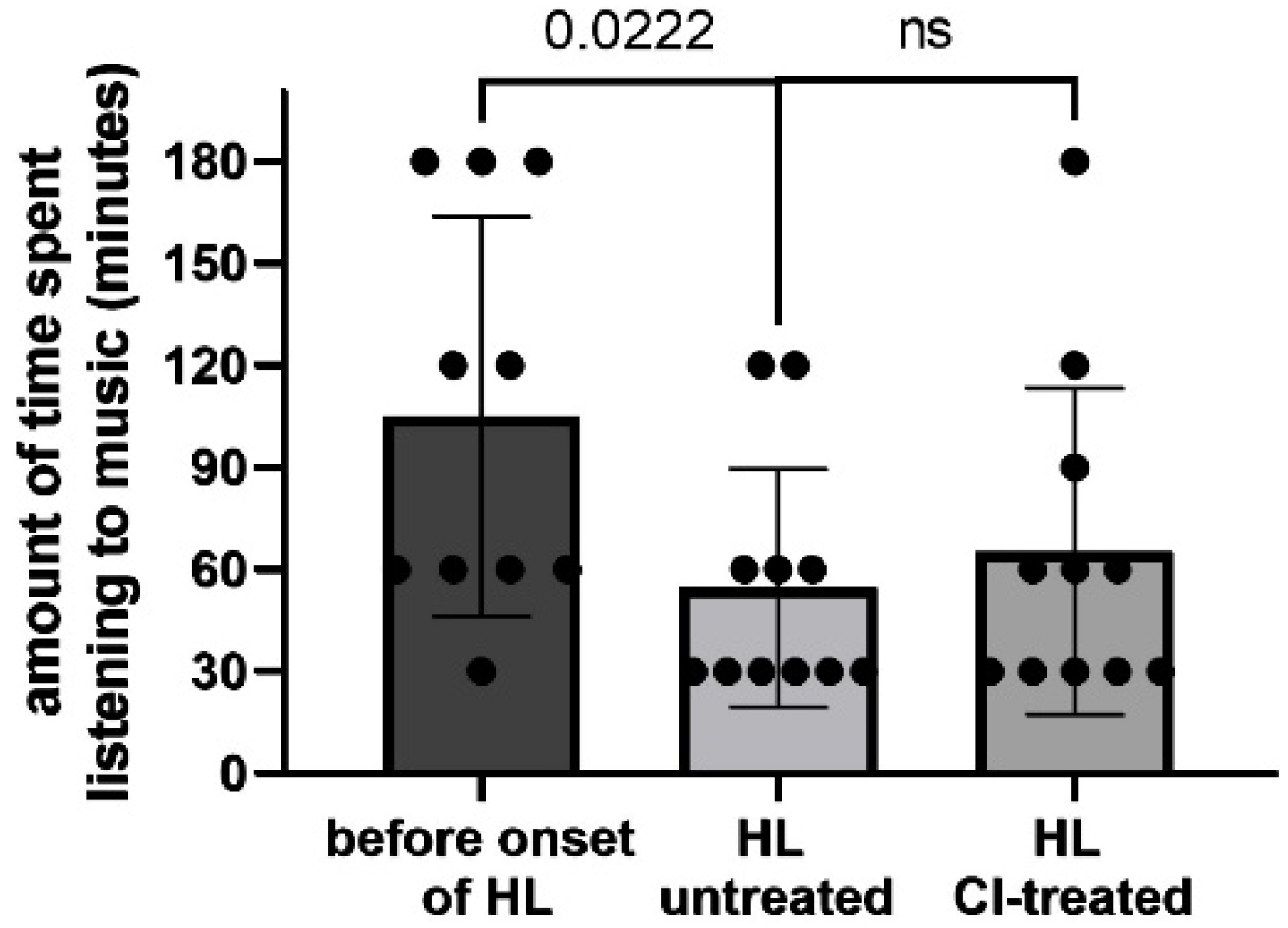
- MUMU Questionnaire: developed by S.J. Brockmeier, (MED-EL) is a tool to scientifically collect actual data about music listening habits of CI users with post-lingual deafness [13]. For the NH-cohort a short version of the questionnaire (23 out of 46) was adapted to exclude hearing device-specific questions.
- (b)
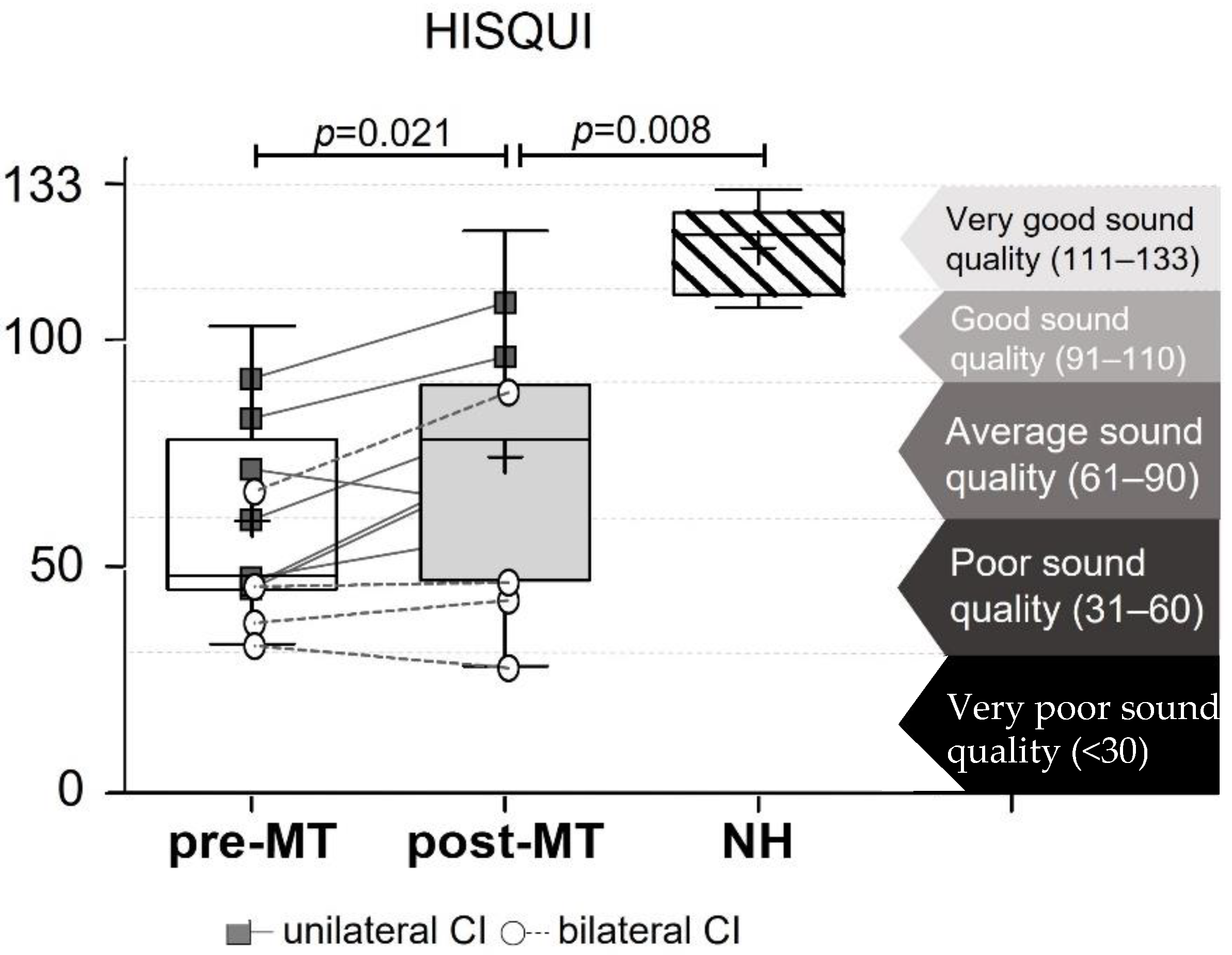
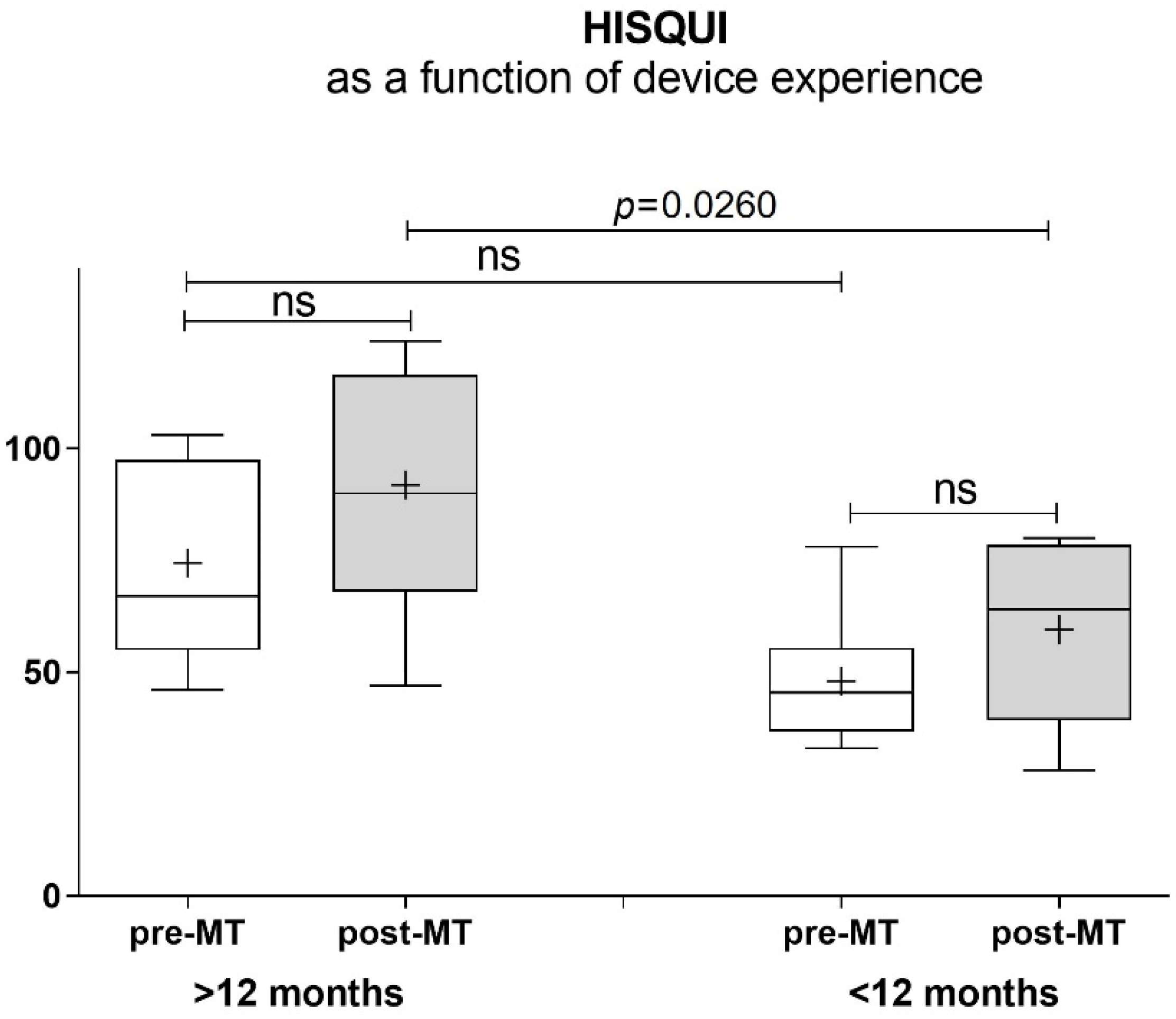
- HISQUI Questionnaire: was established for adults concerning subjective sound quality detection after CI surgery (MED-EL) [14]. The HISQUI measures the sound quality in everyday life situations. The total HISQUI score is obtained by adding the numerical values of all 29 evaluated questions. The score achieved overall indications of how good or poorly you find the sound quality in your personal everyday listening situations with the hearing implant. The result is interpreted by a score of the total achieved numbers: Very poor sound quality < 60, poor sound quality 60–90, moderate sound quality 90–120, good sound quality 120–150 and very good sound quality 150–203.
- (c)
- VAS: The VAS serves as evaluation of the effects of MT on self-confidence, social-participation, actual well-being, frustration, motivation, quality of life, confidence, acceptance on a scale from 0 to 10 [15].
- (d)
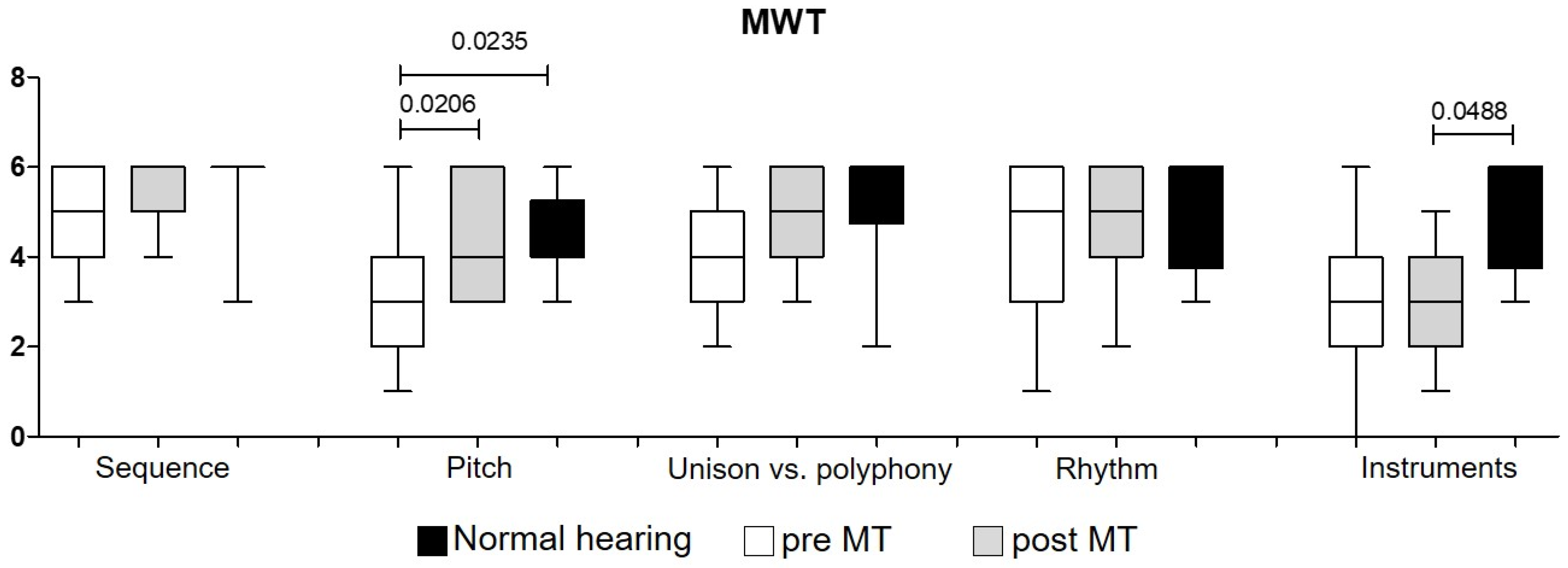
- MWT: The music perception test is an objective method, to test different parameters in music skills containing the following musical aspects: detection of sound sequences (descending, rising or constant), pitch discrimination, differentiation of one or two notes (unison vs. polyphony), rhythm, discrimination and recognition of different instruments. The MWT is divided into two parts: the first part (melody, pitch, rhythm, unison or polyphony) is tested by playing live on the harp by the music therapist. The harp was used because, within therapeutic sessions, it turned out that this instrument produced “enjoyable” sound and offered enough pitch range. The second part, the instrument recognition, was investigated by playing solo versions of professional artists using two loudspeakers.
- (e)
- Interviews: after completion of the 10 MT sessions, interviews were conducted by the music therapist and recorded with a Zoom H1 Handy Recorder. All interviews were transcribed and evaluated per qualitative criteria using Strauss and Corbin’s Grounded Theory model [16].
3. Data Analysis
4. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lima, J.P.; Iervolino, S.M.S.; Schochat, E. Musical and Temporal Auditory Skills in Cochlear Implant Users after Music Therapy. Codas 2018, 30, e20180006. [Google Scholar] [PubMed] [Green Version]
- Driscoll, V.D.; Oleson, J.; Jiang, D.; Gfeller, K. Effects of Training on Recognition of Musical Instruments Presented through Cochlear Implant Simulations. J. Am. Acad. Audiol. 2009, 20, 71–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvin, J.J., III; Fu, Q.J.; Nogaki, G. Melodic Contour Identification by Cochlear Implant Listeners. Ear Hear. 2007, 28, 302–319. [Google Scholar] [CrossRef] [Green Version]
- Fuller, C.D.; Galvin, J.J., III; Maat, B.; Baskent, D.; Free, R.H. Comparison of Two Music Training Approaches on Music and Speech Perception in Cochlear Implant Users. Trends Hear. 2018, 22, 765379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Nardo, W.; Schinaia, L.; Anzivino, R.; de Corso, E.; Ciacciarelli, A.; Paludetti, G. Musical Training Software for Children with Cochlear Implants. Acta Otorhinolaryngol. Ital. 2015, 35, 249–257. [Google Scholar] [PubMed]
- Hutter, E.; Argstatter, H.; Grapp, M.; Plinkert, P.K. Music Therapy as Specific and Complementary Training for Adults after Cochlear Implantation: A Pilot Study. Cochlear Implant. Int. 2015, 16 (Suppl. 3), S13–S21. [Google Scholar] [CrossRef]
- Gfeller, K.; Driscoll, V.; Kenworthy, M.; van Voorst, T. Music Therapy for Preschool Cochlear Implant Recipients. Music Ther. Perspect. 2011, 29, 39–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosaner, J.; Kilinc, A.; Deniz, M. Developing a Music Programme for Preschool Children with Cochlear Implants. Cochlear Implant. Int. 2012, 13, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Abdi, S.; Khalessi, M.H.; Khorsandi, M.; Gholami, B. Introducing Music as a Means of Habilitation for Children with Cochlear Implants. Int. J. Pediatr. Otorhinolaryngol. 2001, 59, 105–113. [Google Scholar] [CrossRef]
- Torppa, R.; Huotilainen, M. Why and How Music Can Be Used to Rehabilitate and Develop Speech and Language Skills in Hearing-Impaired Children. Hear. Res. 2019, 380, 108–122. [Google Scholar] [CrossRef]
- Huber, M.; Roesch, S.; Pletzer, B.; Lukaschyk, J.; Lesinski-Schiedat, A.; Illg, A. Cognition in Older Adults with Severe to Profound Sensorineural Hearing Loss Compared to Peers with Normal Hearing for Age. Int. J. Audiol. 2020, 59, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Sarant, J.; Harris, D.; Busby, P.; Maruff, P.; Schembri, A.; Lemke, U.; Launer, S. The Effect of Hearing Aid Use on Cognition in Older Adults: Can We Delay Decline or Even Improve Cognitive Function? J. Clin. Med. 2020, 9, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brockmeier, S.J.; Peterreins, M.; Lorens, A.; Vermeire, K.; Helbig, S.; Anderson, I.; Skarzynski, H.; van de Heyning, P.; Gstoettner, W.; Kiefer, J. Music Perception in Electric Acoustic Stimulation Users as Assessed by the Mu.S.I.C. Test. Adv. Otorhinolaryngol. 2010, 67, 70–80. [Google Scholar]
- Amann, E.; Anderson, I. Development and Validation of a Questionnaire for Hearing Implant Users to Self-Assess Their Auditory Abilities in Everyday Communication Situations: The Hearing Implant Sound Quality Index (Hisqui19). Acta Otolaryngol. 2014, 134, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Hutter, E.; Grapp, M.; Argstatter, H. Music Therapy in Adults with Cochlear Implants: Effects on Music Perception and Subjective Sound Quality. HNO 2016, 64, 880–890. [Google Scholar] [CrossRef] [PubMed]
- Charmaz, K. Teaching Theory Construction with Initial Grounded Theory Tools: A Reflection on Lessons and Learning. Qual. Health Res. 2015, 25, 1610–1622. [Google Scholar] [CrossRef] [PubMed]
- Gfeller, K.E.; Olszewski, C.; Turner, C.; Gantz, B.; Oleson, J. Music Perception with Cochlear Implants and Residual Hearing. Audiol. Neurootol. 2006, 11 (Suppl. 1), 12–15. [Google Scholar] [CrossRef] [PubMed]
- Laske, R.D.; Veraguth, D.; Dillier, N.; Binkert, A.; Holzmann, D.; Huber, A.M. Subjective and Objective Results after Bilateral Cochlear Implantation in Adults. Otol. Neurotol. 2009, 30, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Peterson, N.; Bergeson, T.R. Contribution of Hearing Aids to Music Perception by Cochlear Implant Users. Cochlear Implant. Int. 2015, 16 (Suppl. 3), S71–S78. [Google Scholar] [CrossRef] [PubMed]
- Shukor, N.F.A.; Lee, J.; Seo, Y.J.; Han, W. Efficacy of Music Training in Hearing Aid and Cochlear Implant Users: A Systematic Review and Meta-Analysis. Clin. Exp. Otorhinolaryngol. 2021, 14, 15–28. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Session | Functional Level | Therapeutic Objective |
|---|---|---|
| 8,9,10 | Speech comprehension with music in the background | Ability to focus on a communication partner in a noisy environment |
| 1,2 | Rhythmical exercises as supportive tool to understand words with different syllables | Syllable supported rhythms to improve speech perception/comprehension |
| 5,6 | Familiar songs and well-known melodies with changed lyrics | Improving concentration ability |
| 1,3 | Discrimination of Sounds and Noises | Raise awareness in hearing experiences in everyday life |
| 1 | Writing down hearing experiences in a “Hearing-Diary” | Discovery and sensible perception of every-day-life listening environment |
| 2,3 | Finding and formulating hearing strategies | Implementation of individual hearing strategies in everyday life |
| 4 | Melody recognition of nursery rhymes/ familiar songs with/wo lyrics | Training in lyrics comprehension |
| 8,9 | Nursery rhymes with close test | Speech understanding using easy songs |
| 7 | Listening and talking about classical compositions in different versions | Learning skills to explore differences in instruments, tempi, dynamics etc. in cover versions |
| 4 | Recognition of unison vs. polyphony | Training in discrimination and hearing awareness |
| 4,5 | Musical exercises with digital media | Additional digital musical training to give more exercise opportunities |
| 2,3 | Audio exercises: discrimination of voices (male/female), instruments etc. | Learning to discriminate voices and timbres |
| 1-10 | Differentiation of tone length and sequence | Exploring different sound and melody offers (raising, descending, constant) |
| 6,7 | Singing or whistling songs | Learning to differentiate sounds |
| Subject ID | Age (Years) | Gender | Uni/ Bilateral | PTA4 CI | PTA4 Contralat. | AP Type | CI Experience (Months) | HA Contra-Lateral | Time Deafness (Years) |
|---|---|---|---|---|---|---|---|---|---|
| MTCI 01 | 82 | F | uni/right | 105 | 98.75 | Opus 2 | 42 | le | 14 |
| MTCI 02 | 69 | M | uni/left | 115 | 87.5 | Sonnet | 15 | ri | 1.5 |
| MTCI 03 | 76 | M | bilateral | 120 | 120 | Opus 2 (le) Sonnet (ri) | 144 (le); 21 (ri) | - | 14 |
| MTCI 04 | 76 | M | uni/right | 91.25 | 93.75 | Sonnet | 8 | le | 70 |
| MTCI 05 | 71 | F | uni/right | 86.25 | 33.75 | Sonnet | 24 | le | 3 |
| MTCI 06 | 66 | M | uni/left | 83.75 | 36.25 | Sonnet | 6 | ri | 5 |
| MTCI 07 | 78 | M | uni/right | 76.25 | 71.25 | Sonnet | 7 | le | 15 |
| MTCI 08 | 71 | F | uni/right | 85 | 58.75 | Kanso | 6 | le | 20 |
| MTCI 09 | 79 | F | bilateral | 68.75 (CI re) | 83.75 (li) | Opus 2 (le) Sonnet (ri) | 66 (le); 6 (ri) | - | 15–20 |
| MTCI 10 | 68 | F | bilateral | 113.75 (CI re) | 110 (li) | Sonnet (le). Opus 2 (ri) | 12 (le); 46 (ri) | - | > 20 |
| MTCI 11 | 65 | M | bilateral | 98.75 (CI re) | 71.25 (li) | Sonnet (le). Opus 2 (ri) | 7 (le); 65 (ri) | - | - |
| MEAN/SD CI | 72.8 ± 5.7 | 5F/6M | 4 Bilat. | 41.1 ± 43.6/23.7 ± 19.8 | 18.3 ± 19.5 | ||||
| MTNH 01 | 65 | F | - | - | - | - | - | ||
| MTNH 02 | 66 | M | - | - | - | - | - | ||
| MTNH 03 | 69 | F | - | - | - | - | - | ||
| MTNH 04 | 78 | F | - | - | - | - | - | ||
| MTNH 05 | 75 | F | - | - | - | - | - | ||
| MTNH 06 | 79 | M | - | - | - | - | - | ||
| MTNH 07 | 76 | F | - | - | - | - | - | ||
| MTNH 08 | 72 | F | - | - | - | - | - | ||
| MTNH 09 | 71 | F | - | - | - | - | - | ||
| MTNH 10 | 67 | F | - | - | - | - | - | ||
| MEAN/SD NH | 71.8 ± 4.9 | 7F/2M | - | - | - | - | - | ||
| #Subjects | HISQUI | VAS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Frustration | Motivation | Self-Confidence | Participation | Wellbeing | QoL | Acceptance | Auditory Perception | |||
| Pre/Post | NH | Pre/Post | Pre/Post | Pre/Post | Pre/Post | Pre/Post | Pre/Post | Pre/Post | Pre/Post | |
| 01 | 92/109 | 123 | 5/0 | 10/10 | 5/10 | 7/10 | 6/10 | 7/10 | 10/10 | 8/10 |
| 02 | 64/90 | 116 | 5/3 | 8/10 | 8/10 | 2/6 | 10/5 | 10/10 | 8/10 | 8/10 |
| 03 | 67/89 | 128 | 5/5 | 10/7 | 7/6 | 2/7 | 6/5 | 6/4 | 7/6 | 7/5 |
| 04 | 45/78 | 133 | 5/5 | 7/6 | 10/6 | 1/3 | 5/6 | 5/8 | 8/5 | 4/5 |
| 05 | 103/124 | 116 | 6/0 | 10/9 | 8/10 | 9/10 | 8/9 | 8/10 | 8/8 | 7/10 |
| 06 | 46/80 | 124 | 8/3 | 10/10 | 4/8 | 4/8 | 4/7 | 4/9 | 4/9 | 3/8 |
| 07 | 78/68 | 110 | 6/5 | 8/8 | 5/3 | 4/3 | 8/7 | 8/7 | 7/6 | 6/6 |
| 08 | 48/60 | 107 | 8/2 | 10/8 | 7/7 | 6/7 | 5/8 | 6/8 | 9/10 | 4/6 |
| 09 | 38/43 | 124 | 5/6 | 10/10 | 10/10 | 2/5 | 7/7 | 9/8 | 7/5 | 6/5 |
| 10 | 33/28 | 133 | 10/3 | 10/10 | 6/8 | 6/6 | 9/5 | 10/9 | 10/10 | 10/9 |
| 11 | 46/47 | - | 10/7 | 6/5 | 8/5 | 2/2 | 10/10 | 5/7 | 3/4 | 2/4 |
| MEAN | 60.0/74.2 | 121.4 | 5.7/3.6 | 9.0/8.45 | 7.1/7.6 | 4.1/6.1 | 7.1/7.2 | 7.1/8.2 | 7.4/7.6 | 5.9/7.1 |
| SD | 21.8/27.5 | 8.5 | 2.42/2.2 | 1.4/1.7 | 1.9/2.3 | 2.5/2.6 | 2.0/1.8 | 2.0/1.7 | 2.1/2.3 | 2.3/2.3 |
| Min | 33/28 | 107 | 0/0 | 6/5 | 4/3 | 1/2 | 4/5 | 4/4 | 3/4 | 2/4 |
| Max | 103/124 | 133 | 10/7 | 10/10 | 10/10 | 9/10 | 10/10 | 10 | 10/10 | 10/10 |
| #ID | MUMU | MWT | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Music Perception | Pitch Differentiation Ability | Instrument | Current Listening to Music (min.) | Sequence | Pitch | Unison/ Polyphony | Rhythm | Instruments | ||||||||||
| Pre/ Post | NH | Pre/ Post | NH | Pre/ Post | NH | Pre/ Post | NH | Pre/ Post | NH | Pre/ Post | NH | Pre/ Post | NH | Pre/ Post | NH | Pre/ Post | NH | |
| 01 | 8/10 | 8 | yes/yes | yes | no | yes | 60/120 | 60 | 4/4 | 6 | 4/6 | 5 | 4/5 | 6 | 2/5 | 6 | 3/3 | 6 |
| 02 | 5/10 | 10 | yes/yes | yes | yes | yes | 30/60 | 120 | 6/6 | 6 | 3/4 | 6 | 5/5 | 6 | 3/5 | 6 | 4/4 | 6 |
| 03 | 5/6 | 9 | yes/yes | yes | yes | no | 60/60 | 60 | 5/5 | 3 | 4/4 | 3 | 6/6 | 5 | 6/5 | 4 | 3/4 | 3 |
| 04 | 5/5 | 10 | yes/yes | yes | no | no | 30/30 | 30 | 3/5 | 6 | 1/3 | 5 | 2/3 | 4 | 4/5 | 6 | 0/2 | 4 |
| 05 | 6/8 | 7 | yes/yes | yes | no | no | 120/90 | 60 | 6/6 | 6 | 6/6 | 5 | 6/6 | 5 | 6/6 | 3 | 6/5 | 3 |
| 06 | 10/8 | 5 | yes/yes | yes | no | no | 30/60 | 120 | 5/6 | 6 | 2/6 | 4 | 5/6 | 5 | 6/6 | 5 | 3/5 | 5 |
| 07 | 7/4 | 10 | yes/yes | yes | no | no | 60/30 | 180 | 5/6 | 6 | 3/3 | 6 | 4/4 | 6 | 1/4 | 4 | 2/2 | 6 |
| 08 | 5/7 | 10 | yes/yes | yes | no | no | 30/30 | 180 | 6/5 | 6 | 4/4 | 5 | 2/5 | 5 | 6/6 | 4 | 4/3 | 6 |
| 09 | 1/1 | 10 | N/A/yes | yes | no | no | 30/30 | 60 | 5/6 | 6 | 2/3 | 4 | 3/6 | 2 | 5/3 | 3 | 2/3 | 4 |
| 10 | 8/8 | 10 | yes/yes | yes | no | no | 120/180 | 180 | 4/6 | 6 | 2/4 | 4 | 4/4 | 5 | 5/2 | 6 | 1/1 | 4 |
| 11 | 21 | - | yes/yes | - | no | - | 30/30 | - | 4/6 | - | 4/5 | - | 5/5 | - | 6/6 | 4/4 | - | |
| M | 5.6/6.2 | 8.9 | 54.5/65.5 | 105 | 4.8/5.5 | 5.7 | 3.2/4.4 | 4.7 | 4.2/5.0 | 4.9 | 4.5/4.7 | 4.7 | 2.9/3.3 | 4.7 | ||||
| SD | 2.5/3.0 | 1.6 | 33.4/45.8 | 55.7 | 0.9/0.7 | 0.9 | 1.4/1.2 | 0.9 | 1.4/1.0 | 1.2 | 1.8/1.3 | 1.2 | 1.6/1.3 | 1.2 | ||||
| Min | 1/1 | 5 | 30/30 | 30 | 3/4 | 3 | 1/3 | 3 | 2/3 | 2 | 2/2 | 3 | 0/1 | 3 | ||||
| Max | 10/10 | 10 | 120/180 | 180 | 6/6 | 6 | 6/6 | 6 | 6/6 | 6 | 6/6 | 6 | 6/6 | 6 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magele, A.; Wirthner, B.; Schoerg, P.; Ploder, M.; Sprinzl, G.M. Improved Music Perception after Music Therapy following Cochlear Implantation in the Elderly Population. J. Pers. Med. 2022, 12, 443. https://doi.org/10.3390/jpm12030443
Magele A, Wirthner B, Schoerg P, Ploder M, Sprinzl GM. Improved Music Perception after Music Therapy following Cochlear Implantation in the Elderly Population. Journal of Personalized Medicine. 2022; 12(3):443. https://doi.org/10.3390/jpm12030443
Chicago/Turabian StyleMagele, Astrid, Bianca Wirthner, Philipp Schoerg, Marlene Ploder, and Georg Mathias Sprinzl. 2022. "Improved Music Perception after Music Therapy following Cochlear Implantation in the Elderly Population" Journal of Personalized Medicine 12, no. 3: 443. https://doi.org/10.3390/jpm12030443
APA StyleMagele, A., Wirthner, B., Schoerg, P., Ploder, M., & Sprinzl, G. M. (2022). Improved Music Perception after Music Therapy following Cochlear Implantation in the Elderly Population. Journal of Personalized Medicine, 12(3), 443. https://doi.org/10.3390/jpm12030443