
Depression, Insomnia and Post-Traumatic Stress Disorder in COVID-19 Survivors: Role of Gender and Impact on Quality of Life

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Questionnaire and Psychometric Scales
- (1)
- Sociodemographic and clinical factors: gender, age, body mass index (BMI), smoking, comorbidities, disease severity, hospitalization in COVID-19 clinic or ICU, and days of hospitalization (total and ICU).Disease severity was assessed according to the National Institute of Health criteria [15] as follows:
- Mild Illness: Individuals who have any of the various signs and symptoms of COVID-19 (e.g., fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste and smell) but who do not have shortness of breath, dyspnea, or abnormal chest imaging.
- Moderate Illness: Individuals who show evidence of lower respiratory disease during clinical assessment or imaging and who have an oxygen saturation (SpO2) ≥ 94% on room air at sea level.
- Severe Illness: Individuals who have SpO2 < 94% on room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) < 300 mm Hg, a respiratory rate > 30 breaths/min, or lung infiltrates > 50%.
- Critical Illness: Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction.
- (2)
- The Hospital Anxiety and Depression Scale (HADS) is a 14-item self-administered screening tool for the presence of depression and anxiety [16]. Respondents are asked to reflect on their mood in the past week. On the scale, 7 items assess depression and 7 items assess anxiety. Scores for items in each subscale of the HADS are summed to produce an anxiety score (HADS-A) or a Depression score (HADS-D) or can be added to produce a total score (HADS-T). Total scores range between 0 and 21 for each scale and are graded for severity from normal (0–7), mild (8–10), moderate (11–14) to severe (15–21). The scale has been validated in Greek, demonstrating good psychometric properties, i.e., high internal consistency (Cronbach’s alpha coefficient was 0.884) and stability (test–retest correlation coefficient 0.944) while factor analysis confirmed a two-factor structure [16].
- Impact of Event Scale-Revised (IES-R) is a validated 22-item self-report that measures subjective psychological distress in response to traumatic events [17,18]. It has 3 subscales (Intrusion, Avoidance and Hyperarousal), which are closely associated with post-traumatic stress disorder (PTSD) symptoms. Total scores range between 0 and 88 and are graded for severity from normal (0–23), mild (24–32), moderate (33–36) to severe psychological distress (>37). A cut-off score of 24 is commonly used to define PTSD of a clinical concern. The Greek version used has shown good psychometric features; the Cronbach’s alphas for the intrusion, avoidance, and hyperarousal scales were 0.72, 0.77, and 0.85, respectively; overall test–retest reliability was also satisfactory [17].
- The AIS is a questionnaire developed to evaluate insomnia problems [19]. Each item is rated from 0 (no problem at all), 1 (mild problem), and 2 (marked problem), to 3 (very serious problem). The first 5 items assess difficulty with sleep induction, awakenings during the night, early morning awakening, total sleep time, and overall sleep quality. The last three items assess the next-day consequences of insomnia, such as problems with sense of wellbeing, functioning, and daytime sleepiness. A cut-off score of >6 is used to establish the diagnosis of insomnia. The Greek version was used; the scale has shown very good psychometric characteristics (with Cronbach’s α around 0.90 and test–retest reliability correlation coefficient at almost 0.90) [19].
- Numerical fear rating scale (NFRS) was used to measure the level of fear in the study, which has been reported to have good reliability and validity [20]. It is a segmented numeric version of the visual analog scale (VAS) in which a respondent selects a whole number (0–10 integers) that best reflects the intensity of their fear. Higher scores indicate greater fear as follows: 0 for no fear, 1–3 for mild fear, 4–6 for moderate fear, 7–9 for severe fear, 10 for extreme fear.
- Quality of Life (EQ-5D-5L) essentially consists of 2 parts: the EQ-5D descriptive system and the EQ visual analogue scale (EQ-5D-5L VAS) [21,22], which we report on here. The descriptive system consists of 5 dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. The EQ-5D-5L VAS records the patient’s self-rated health on a vertical visual analogue scale from the best to worst health and can be used as a patient-reported quantitative measure of health outcome. The scale has been validated in Greek, showing good performance in terms of low ceiling effects, high absolute and relative informativity, and convergent and known-group validity efficiency [21].
2.3. Statistical Analysis
3. Results
3.1. Demographic and Participant Characteristics
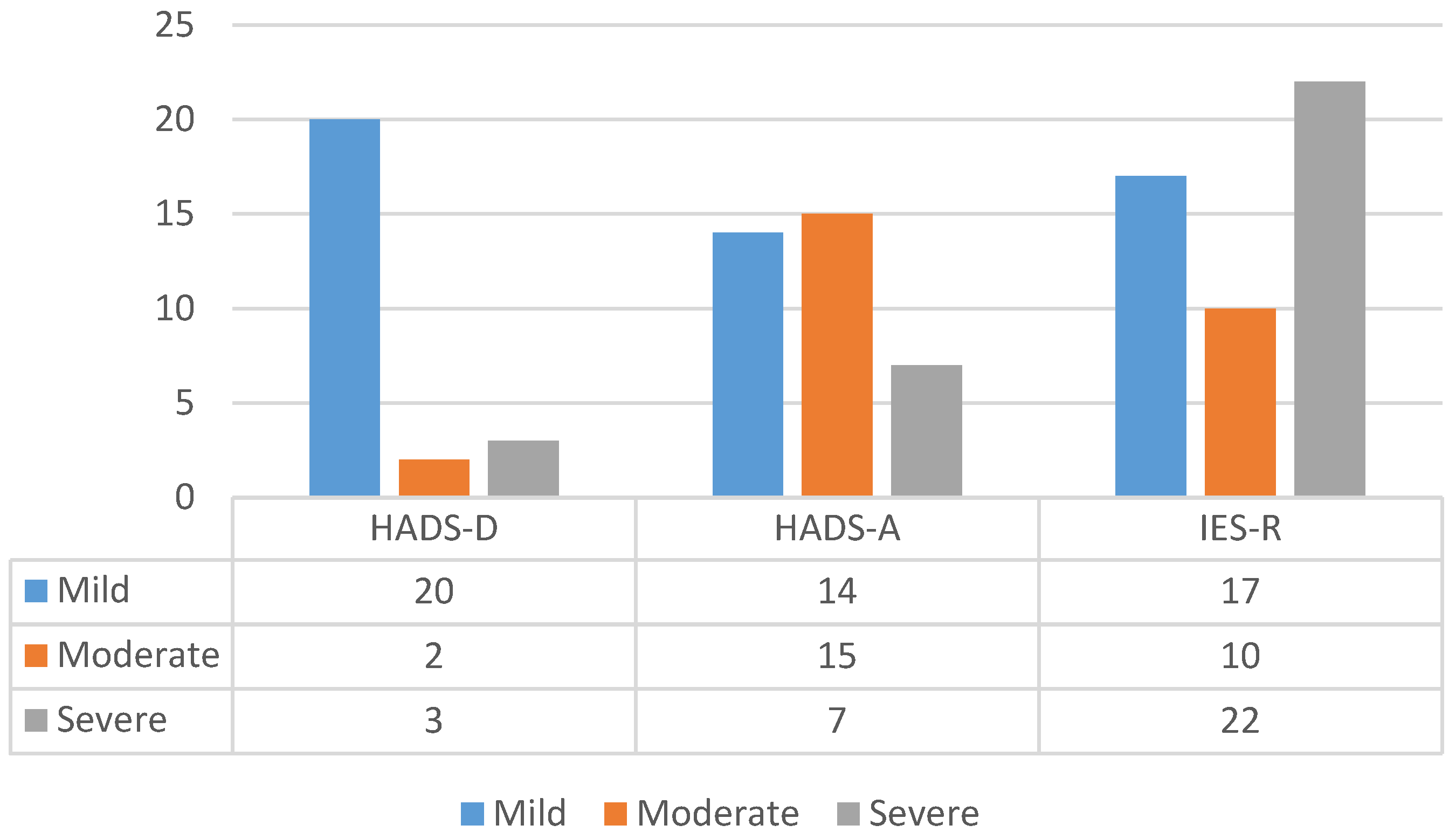
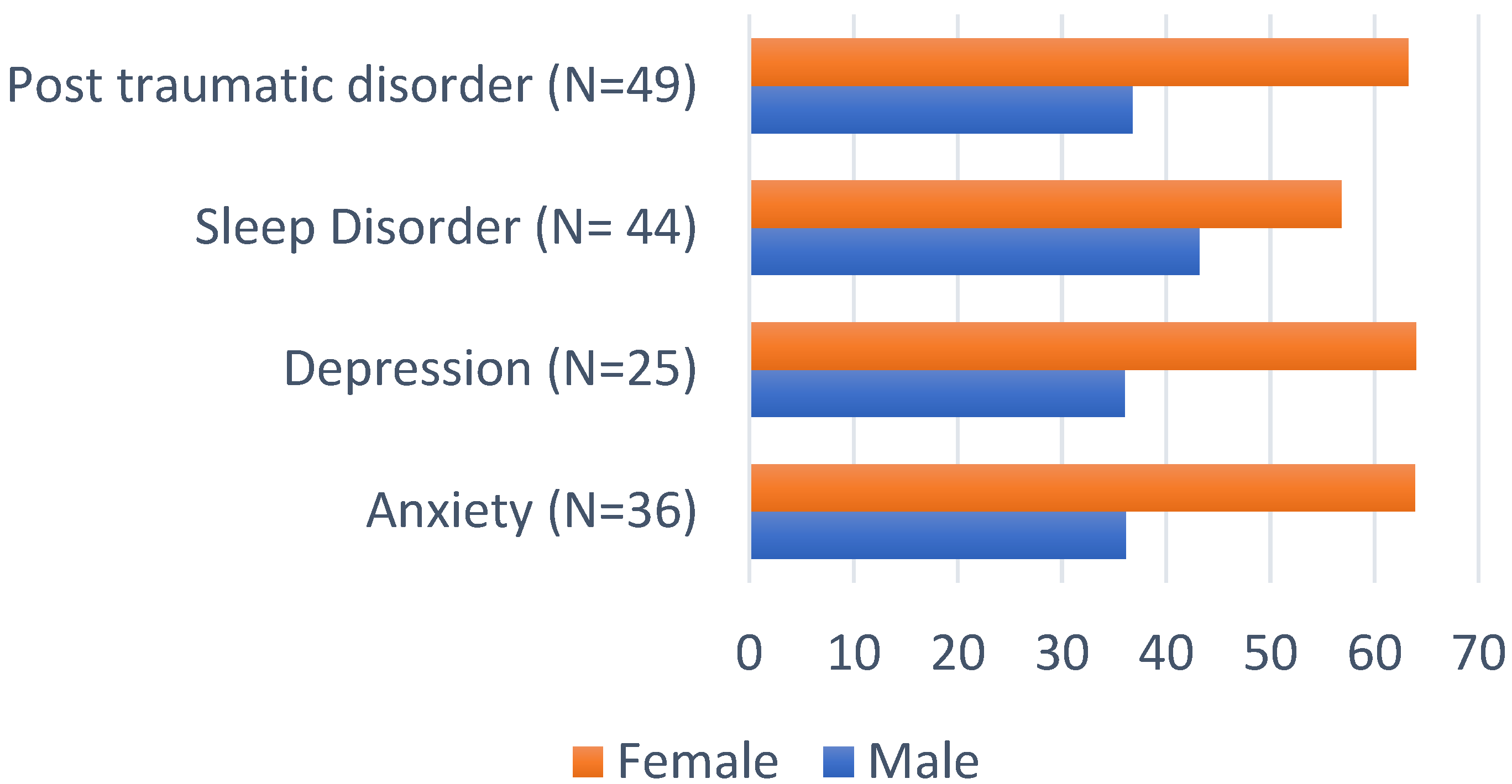
3.2. Psychometric Scales Outcomes
4. Discussion
4.1. Depression and Anxiety
4.2. Traumatic Stress and PTSD
4.3. Insomnia
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 397–506. [Google Scholar] [CrossRef] [Green Version]
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The epidemiology, diagnosis and treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105955. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Khan, S.; Siddique, R.; Li, H.; Shereen, M.A.; Bashir, N.; Xue, M. Impact of coronavirus outbreak on psychological health. J. Glob. Health 2020, 10, 010331. [Google Scholar] [CrossRef]
- Kim, H.C.; Yoo, S.Y.; Lee, B.H.; Lee, S.H.; Shin, H.S. Psychiatric Findings in Suspected and Confirmed Middle East Respiratory Syndrome Patients Quarantined in Hospital: A Retrospective Chart Analysis. Psychiatry Investig. 2018, 15, 355–360. [Google Scholar] [CrossRef]
- Kaputu-Kalala-Malu, C.; Musalu, E.M.; Walker, T.; Ntumba-Tshitenge, O.; Ahuka-Mundeke, S. PTSD, depression and anxiety in Ebola virus disease survivors in Beni town, Democratic Republic of the Congo. BMC Psychiatry 2021, 21, 342. [Google Scholar] [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, C.Y.; Chang, O.; Huang, E.; Zuo, Q.K. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: A meta-analysis. Ann. NY Acad. Sci. 2021, 1486, 90–111. [Google Scholar] [CrossRef] [PubMed]
- Hatch, R.; Young, D.; Barber, V.; Griffiths, J.; Harrison, D.A.; Watkinson, P. Anxiety, Depression and Post Traumatic Stress Disorder after critical illness: A UK-wide prospective cohort study. Crit. Care 2018, 22, 310. [Google Scholar] [CrossRef] [Green Version]
- Mazza, M.G.; De Lorenzo, R.; Conte, C.; Poletti, S.; Vai, B.; Bollettini, I.; Melloni, E.; Furlan, R.; Ciceri, F.; Rovere-Querini, P.; et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav. Immun. 2020, 89, 594–600. [Google Scholar] [CrossRef]
- Matalon, N.; Dorman-Ilan, S.; Hasson-Ohayon, I.; Hertz-Palmor, N.; Shani, S.; Basel, D.; Gross, R.; Chen, W.; Abramovich, A.; Afek, A.; et al. Trajectories of post-traumatic stress symptoms, anxiety, and depression in hospitalized COVID-19 patients: A one-month follow—up. J. Psychosom Res. 2021, 143, 110399. [Google Scholar] [CrossRef]
- Taquet, M.; Geddes, J.R.; Husain, M.; Luciano, S.; Harrison, P.J. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: A retrospective cohort study using electronic health records. Lancet Psychiatry 2021, 8, 416–427. [Google Scholar] [CrossRef]
- Stefanou, M.I.; Palaiodimou, L.; Bakola, E.; Smyrnis, N.; Papadopoulou, M.; Paraskevas, G.P.; Rizos, E.; Boutati, E.; Grigoriadis, N.; Krogias, C.; et al. Neurological manifestations of long-COVID syndrome: A narrative review. Ther. Adv. Chronic Dis. 2022, 13, 20406223221076890. [Google Scholar] [CrossRef] [PubMed]
- Badenoch, J.B.; Rengasamy, E.R.; Watson, C.; Jansen, K.; Chakraborty, S.; Sundaram, R.D.; Hafeez, D.; Burchilll, E.; Saini, A.; Thomas, L.; et al. Persistent neuropsychiatric symptoms after COVID-19: A systematic review and meta-analysis. Brain Comms. 2021, 4, fcab297. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 13 December 2021).
- Michopoulos, I.; Douzenis, A.; Kalkavoura, C.; Christodoulou, C.; Michalopoulou, P.; Kalemi, G.; Fineti, K.; Patapis, P.; Protopapas, K.; Lykouras, L. Hospital Anxiety and Depression Scale (HADS): Validation in a Greek general hospital sample. Ann. Gen. Psychiatry 2008, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale-Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef]
- Mystakidou, K.; Tsilika, E.; Parpa, E.; Galanos, A.; Vlahos, L. Psychometric properties of the Impact of Event Scale in Greek cancer patients. J. Pain Symptom Manag. 2007, 33, 454–461. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 27, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kontodimopoulos, N.; Pappa, E.; Niakas, D.; Yfantopoulos, J.; Dimitrakaki, C.; Tountas, Y. Validity of the EuroQoL (EQ-5D) instrument in a Greek general population. Value Health 2008, 11, 1162–1169. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Athanasiou, N.; Sakkas, N.; Patrinos, S.; Sakka, E.; Barmparessou, Z.; Tsikrika, S.; Adraktas, A.; Pataka, A.; Migdalis, I.; et al. From Recession to Depression? Prevalence and Correlates of Depression, Anxiety, Traumatic Stress and Burnout in Healthcare Workers during the COVID-19 Pandemic in Greece: A Multi-Center, Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 2390. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Author Reply-Letter to the editor “The challenges of quantifying the psychological burden of COVID-19 on healthcare workers”. Brain Behav. Immun. 2021, 92, 209–210. [Google Scholar] [CrossRef]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef] [PubMed]
- Mak, I.W.; Chu, C.M.; Pan, P.C.; Yiu, M.G.; Ho, S.C.; Chan, V.L. Risk factors for chronic post-traumatic stress disorder (PTSD) in SARS survivors. Gen. Hosp. Psychiatry 2010, 32, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Dorri, M.; Mozafari Bazargany, M.H.; Khodaparast, Z.; Bahrami, S.; Seifi Alan, M.; Rahimi, F.; Kamipoor, Z.; Niksima, M.M.; Dehghan, H.; Rastad, H. Psychological problems and reduced health-related quality of life in the COVID-19 survivors. J. Affect. Disord. Rep. 2021, 6, 100248. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Gong, Y.M.; Liu, L.; Sun, Y.K.; Tian, S.S.; Wang, Y.J.; Zhong, Y.; Zhang, A.Y.; Su, S.Z.; Liu, X.X.; et al. Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: A meta-analysis and systematic review. Mol. Psychiatry 2021, 26, 4982–4998. [Google Scholar] [CrossRef] [PubMed]
- Pataka, A.; Kotoulas, S.; Sakka, E.; Katsaounou, P.; Pappa, S. Sleep Dysfunction in COVID-19 Patients: Prevalence: Risk Factors, Mechanisms, and Management. J. Pers. Med. 2021, 11, 1203. [Google Scholar] [CrossRef]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Newt. Open 2021, 4, e2128568. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Tarsitani, L.; Vassalini, P.; Koukopoulos, A.; Borrazzo, C.; Alessi, F.; Di Nicolantonio, C.; Serra, R.; Alessandri, F.; Ceccarelli, G.; Mastroianni, C.M.; et al. Post-traumatic Stress Disorder Among COVID-19 Survivors at 3-Month Follow-up After Hospital Discharge. J. Gen. Intern. Med. 2021, 36, 1702–1707. [Google Scholar] [CrossRef] [PubMed]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow—up: Results from a prospective UK cohort. Thorax 2021, 76, 399–401. [Google Scholar] [CrossRef] [PubMed]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age | N | Mean ± SD |
|---|---|---|
| Male/Female | 143 | 57.10 ± 13 |
| Gender | N | % |
| Male | 91 | 63.64 |
| Female | 52 | 36.36 |
| Severity Of COVID-19 | ||
| Mild | 4 | 2.80 |
| Moderate | 50 | 34.97 |
| Severe | 69 | 48.25 |
| Critical | 20 | 13.99 |
| Comorbidities | 108 (with a total of 161 comorbidities) | 75.52 |
| Diabetes mellitus | 12 | 8.39 |
| Hypertension | 44 | 30.99 |
| Coronary disease | 6 | 4.20 |
| Cancer | 10 | 6.99 |
| Immunosuppression | 11 | 7.69 |
| Asthma | 20 | 13.99 |
| COPD | 5 | 3.50 |
| Obesity | 53 | 38.69 |
| Smoking Status | ||
| Never smoker | 80 | 56.74 |
| Ex-smoker | 44 | 31.21 |
| Current Smoker | 17 | 12.06 |
| Not known | 2 | |
| Hospitalization | ||
| COVID-19 Clinic | 118 | 81.88 |
| Intensive Care Unit | 25 | 18.12 |
| Male | Female | Total | ||
|---|---|---|---|---|
| HADS Depression | N (%) | N (%) | N (%) | p-Value |
| No depression | 75 (69.44) | 33 (30.56) | 108 (81.2) | |
| Mild | 8 (40.00) | 12 (60.00) | 20 (15.04) | =0.005 ** |
| Moderate | 0 (0.00) | 2 (100.00) | 2 (1.05) | |
| Severe | 1 (33.33) | 2 (66.67) | 3 (2.26) | |
| HADS Anxiety | ||||
| No Anxiety | 71 (73.20) | 26 (26.80) | 97 (73.93) | |
| Mild | 4 (28.57) | 10 (71.43) | 14 (10.53) | <0.001 *** |
| Moderate | 7 (46.67) | 8 (53.33) | 15 (11.28) | |
| Severe | 2 (28.57) | 5 (71.43) | 7 (5.26) | |
| AIS | ||||
| No insomnia | 64 (72.73) | 24 (27.27) | 88 (66.67) | <0.001 *** |
| Insomnia | 19 (43.18) | 25 (56.82) | 44 (33.33) | |
| IES-R | ||||
| No stress | 65 (79.27) | 17 (20.73) | 82 (62.6) | |
| Mild | 8 (47.06) | 9 (52.94) | 17 (12.98) | <0.001 *** |
| Moderate | 1 (10.00) | 9 (90.00) | 10 (7.63) | |
| Severe | 10 (45.45) | 12 (54.55) | 22 (16.79) | |
| Severity of COVID-19 Illness | ||||
| Mild | 1 (25.00) | 3 (75.00) | 4 (2.7) | |
| Moderate | 25 (50.00) | 25 (50.00) | 50 (34.96) | =0.007 ** |
| Severe | 48 (69.57) | 21 (30.43) | 69 (48.25) | |
| Critical | 17 (85.00) | 3 (15.00) | 20 (13.98) | |
| Mean ± SD | Mean ± SD | (Mean ± SD) | ||
| Fear | 3.16 ± 2.64 | 5 (5.59 ± 2.91) | (4.06 ± 2.98) | <0.001 *** |
| EQ-5D-5L (VAS) | Median | Mean ± SD | p-Value |
|---|---|---|---|
| HADS | |||
| No depression | 65 | 64.5 ± 19.6 | 0.05 |
| Mild | 70 | 59.6 ± 25.9 | |
| Moderate | -- | -- | |
| Severe depression | 30 | 30 ± 14.1 | |
| No anxiety | 70 | 65.9 ± 18.7 | 0.11 |
| Mild | 52.5 | 52.5 ± 17.7 | |
| Moderate | 50 | 52.8 ± 27.1 | |
| Severe anxiety | 45 | 58.3 ± 33.7 | |
| AIS | 0.12 | ||
| No insomnia | 70 | 65.4 ± 19.6 | |
| Insomnia | 55 | 58.2 ± 23.1 | |
| IES-R | 0.47 | ||
| No stress | 65 | 64.3 ± 19.4 | |
| Mild stress | 65 | 65 ± 18.9 | |
| Moderate stress | 70 | 62 ± 29.5 | |
| Severe stress | 47.5 | 54.2 ± 27.6 | |
| Smoking | |||
| Non-smoker | 65 | 61 ± 21.5 | 0.68 |
| Ex-smoker | 60 | 63.7 ± 23.5 | |
| Smoker | 70 | 66.4 ± 13.6 | |
| No comorbidities | 62.5 | 61.4 ± 20.4 | 0.76 |
| Comorbidities | 62.5 | 62.8 ± 21.9 | |
| No ICU admission | 70 | 65.7 ± 21.2 | 0.005 ** |
| ICU admission | 50 | 49.7 ± 19.3 | |
| Females | 60 | 60.4 ± 22.2 | 0.48 |
| Males | 65 | 63.5 ± 21.21 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pappa, S.; Barmparessou, Z.; Athanasiou, N.; Sakka, E.; Eleftheriou, K.; Patrinos, S.; Sakkas, N.; Pappas, A.; Kalomenidis, I.; Katsaounou, P. Depression, Insomnia and Post-Traumatic Stress Disorder in COVID-19 Survivors: Role of Gender and Impact on Quality of Life. J. Pers. Med. 2022, 12, 486. https://doi.org/10.3390/jpm12030486
Pappa S, Barmparessou Z, Athanasiou N, Sakka E, Eleftheriou K, Patrinos S, Sakkas N, Pappas A, Kalomenidis I, Katsaounou P. Depression, Insomnia and Post-Traumatic Stress Disorder in COVID-19 Survivors: Role of Gender and Impact on Quality of Life. Journal of Personalized Medicine. 2022; 12(3):486. https://doi.org/10.3390/jpm12030486
Chicago/Turabian StylePappa, Sofia, Zafeiria Barmparessou, Nikolaos Athanasiou, Elpitha Sakka, Kostas Eleftheriou, Stavros Patrinos, Nikolaos Sakkas, Apostolis Pappas, Ioannis Kalomenidis, and Paraskevi Katsaounou. 2022. "Depression, Insomnia and Post-Traumatic Stress Disorder in COVID-19 Survivors: Role of Gender and Impact on Quality of Life" Journal of Personalized Medicine 12, no. 3: 486. https://doi.org/10.3390/jpm12030486
APA StylePappa, S., Barmparessou, Z., Athanasiou, N., Sakka, E., Eleftheriou, K., Patrinos, S., Sakkas, N., Pappas, A., Kalomenidis, I., & Katsaounou, P. (2022). Depression, Insomnia and Post-Traumatic Stress Disorder in COVID-19 Survivors: Role of Gender and Impact on Quality of Life. Journal of Personalized Medicine, 12(3), 486. https://doi.org/10.3390/jpm12030486