
Optic Nerve Sheath Diameter for Predicting Outcomes in Post-Cardiac Arrest Syndrome: An Updated Systematic Review and Meta-Analysis

 , , , , , ,
, , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources and Literature Search Strategy
2.4. Study Selection
2.5. Data Collection Process and Data Items
2.6. Risk of Bias in Individual Studies
2.7. Statistical Analysis
3. Results
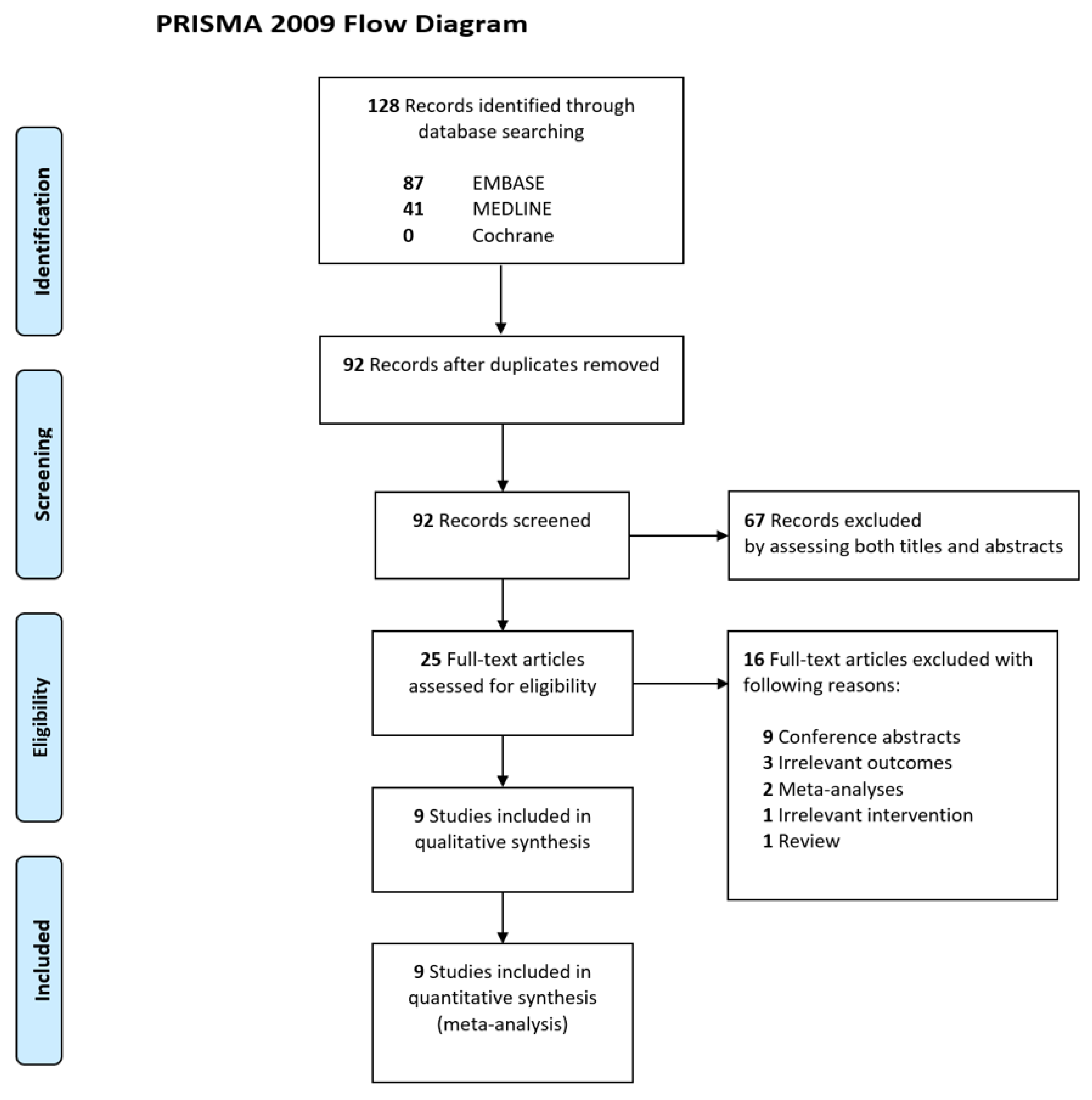
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
3.4. Quality of Evidence According to GRADE Levels
3.5. Results of Meta-Analyses
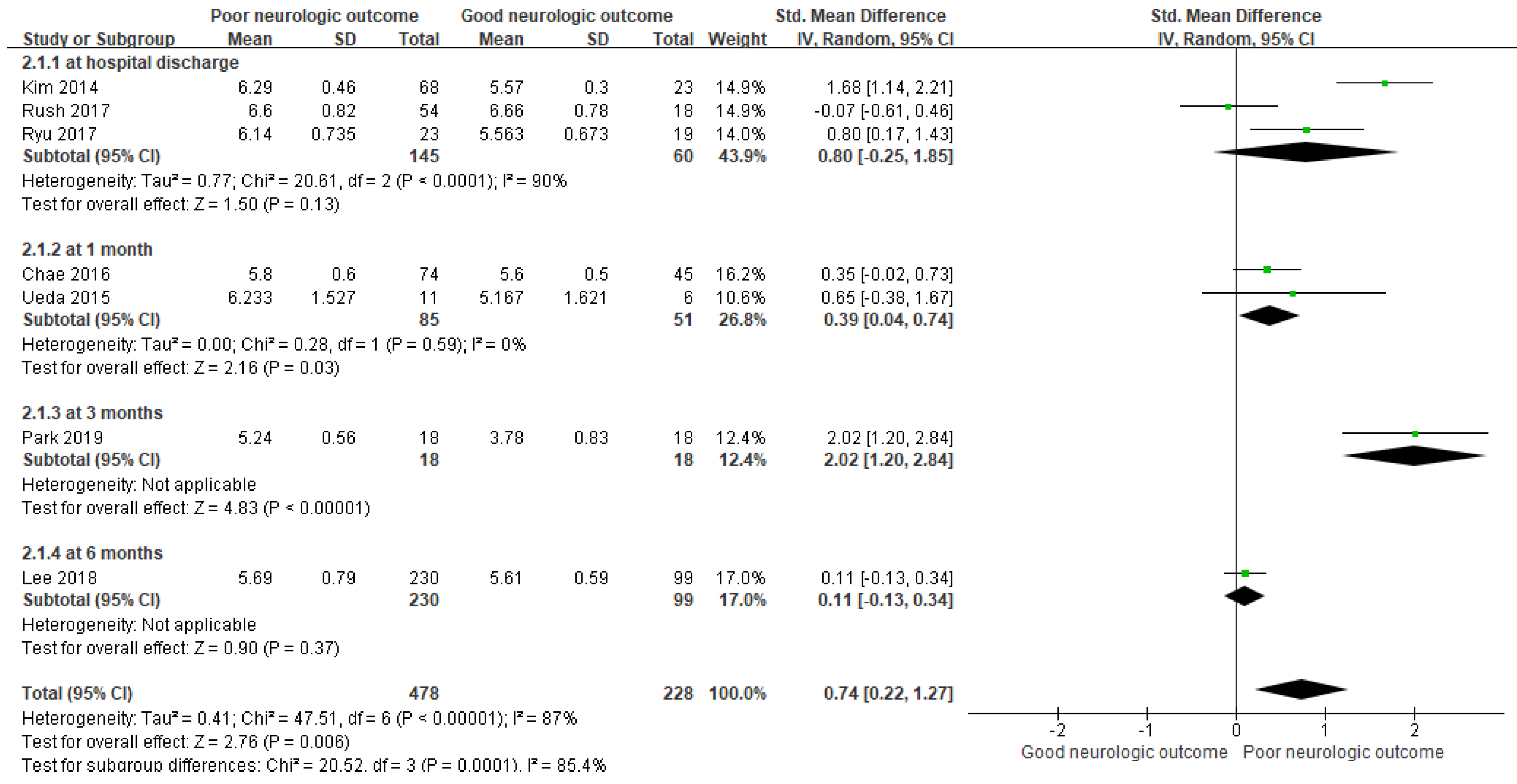
3.5.1. ONSD as a Predictor for PNO
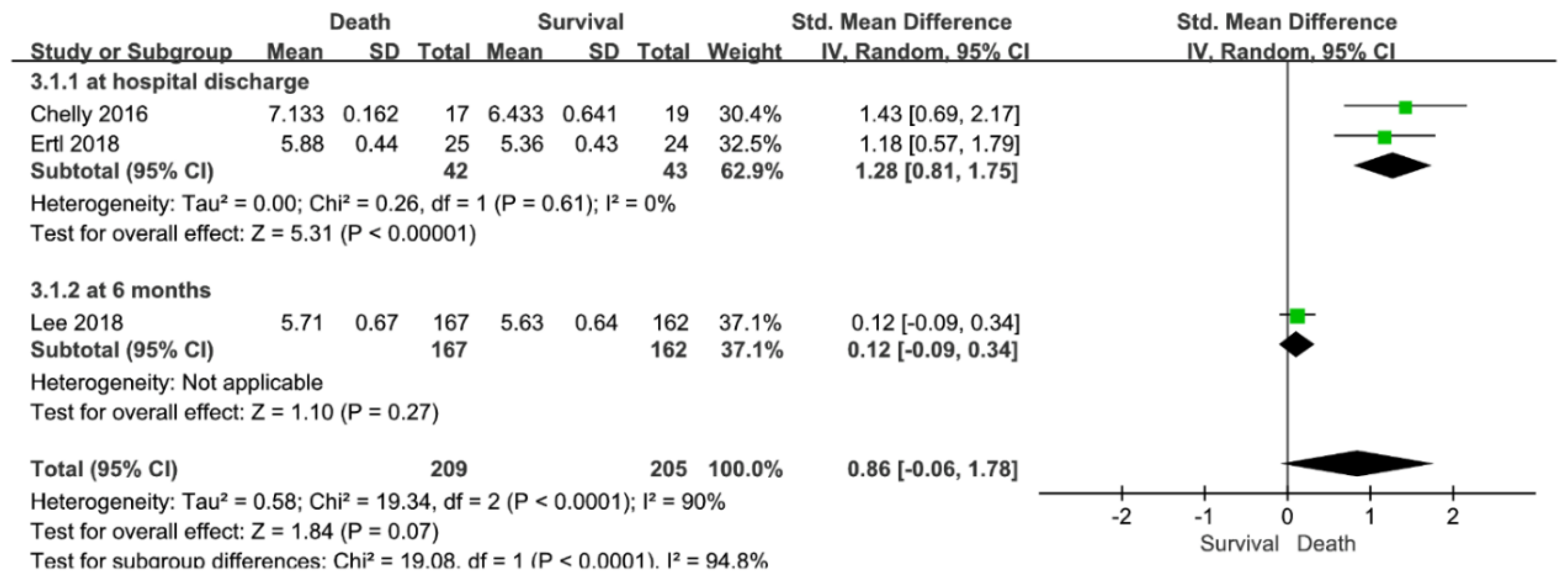
3.5.2. ONSD for Predicting Mortality
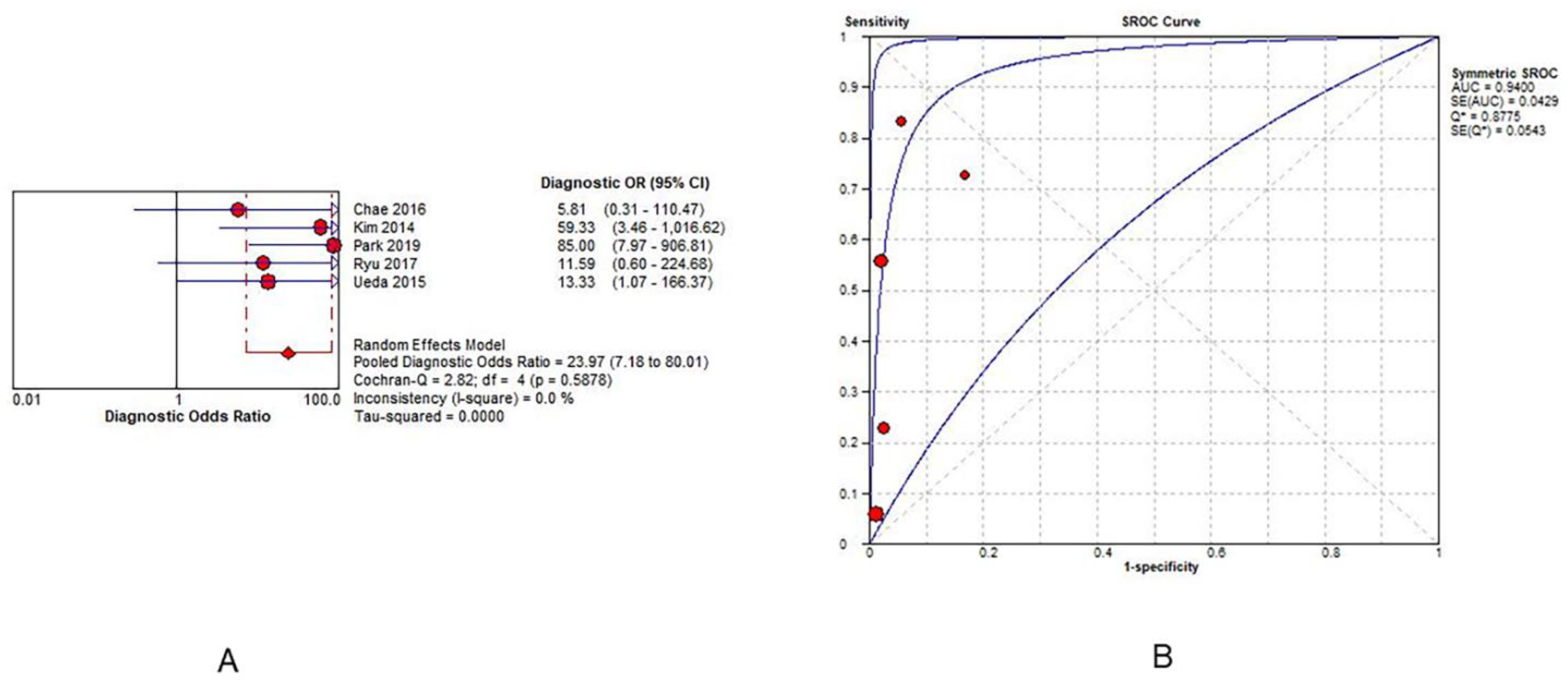
3.5.3. Prognostic Accuracy of ONSD in Predicting PNO
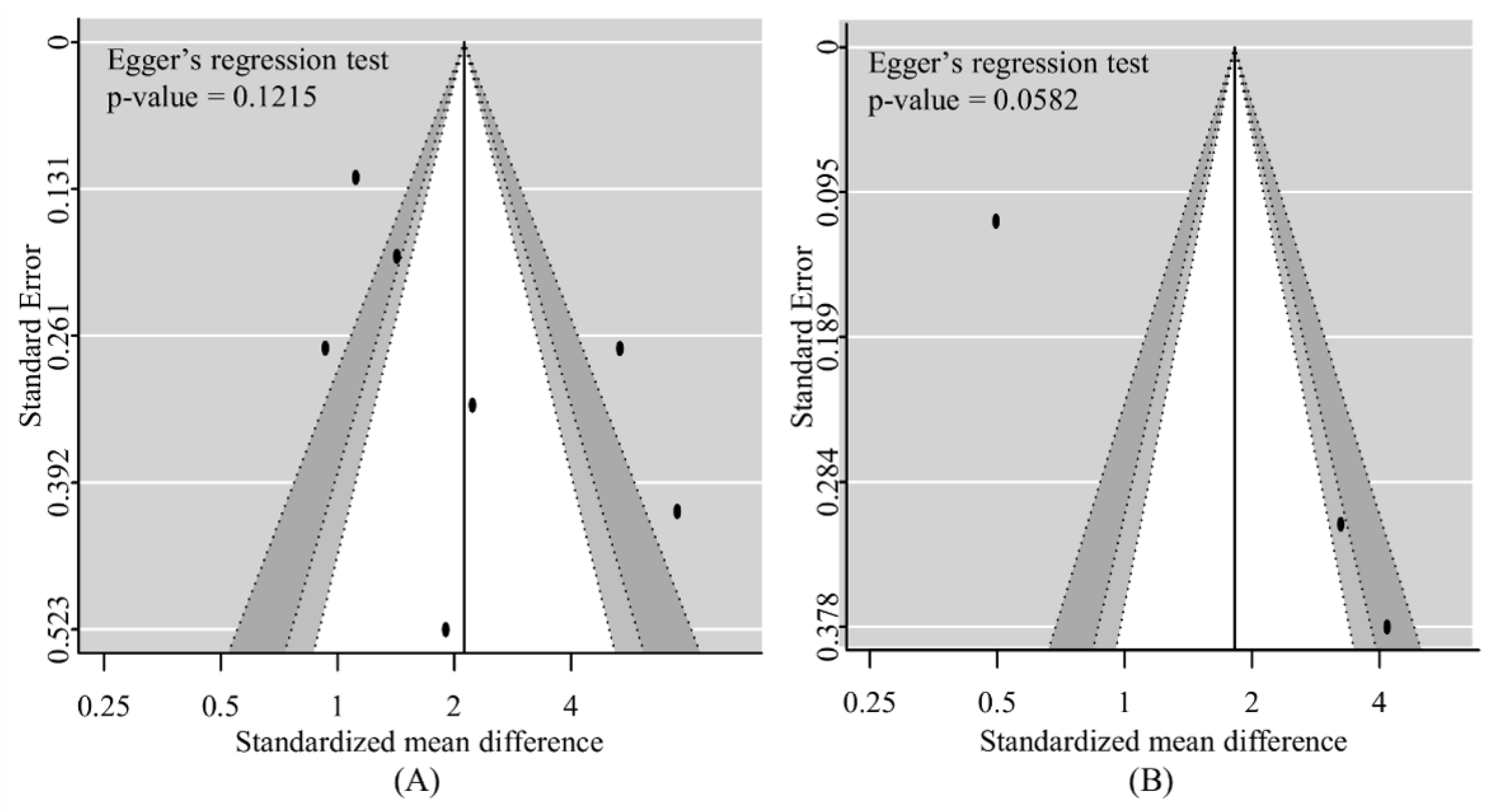
3.5.4. Risk of Bias across Studies
3.5.5. Additional Analyses
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chae, M.K.; Ko, E.; Lee, J.H.; Lee, T.R.; Yoon, H.; Hwang, S.Y.; Cha, W.C.; Shin, T.G.; Sim, M.S.; Jo, I.J.; et al. Better prognostic value with combined optic nerve sheath diameter and grey-to-white matter ratio on initial brain computed tomography in post-cardiac arrest patients. Resuscitation 2016, 104, 40–45. [Google Scholar] [CrossRef] [PubMed]
- You, Y.; Park, J.; Min, J.; Yoo, I.; Jeong, W.; Cho, Y.; Ryu, S.; Lee, J.; Kim, S.; Cho, S.; et al. Relationship between time related serum albumin concentration, optic nerve sheath diameter, cerebrospinal fluid pressure, and neurological prognosis in cardiac arrest survivors. Resuscitation 2018, 131, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Chelly, J.; Deye, N.; Guichard, J.-P.; Vodovar, D.; Vong, L.; Jochmans, S.; Thieulot-Rolin, N.; Sy, O.; Serbource-Goguel, J.; Vinsonneau, C.; et al. The optic nerve sheath diameter as a useful tool for early prediction of outcome after cardiac arrest: A prospective pilot study. Resuscitation 2016, 103, 7–13. [Google Scholar] [CrossRef]
- Kang, C.; Min, J.H.; Park, J.S.; You, Y.; Yoo, I.; Cho, Y.C.; Jeong, W.; Ahn, H.J.; Ryu, S.; Lee, J.; et al. Relationship between optic nerve sheath diameter measured by magnetic resonance imaging, intracranial pressure, and neurological outcome in cardiac arrest survivors who underwent targeted temperature management. Resuscitation 2019, 145, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Santori, G.; Czosnyka, M.; Corradi, F.; Bragazzi, N.; Padayachy, L.; Taccone, F.S.; Citerio, G. Optic nerve sheath diameter measured sonographically as non-invasive estimator of intracranial pressure: A systematic review and meta-analysis. Intensive Care Med. 2018, 44, 1284–1294. [Google Scholar] [CrossRef]
- Rush, B.; Wormsbecker, A.; Berger, L.; Wiskar, K.; Sekhon, M.S.; Griesdale, D.E. Optic nerve sheath diameter on computed tomography not predictive of neurological status post-cardiac arrest. Can. J. Emerg. Med. 2017, 19, 181–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H.; Jong, Y.S. Diagnostic performance of optic nerve sheath diameter for predicting neurologic outcome in post-cardiac arrest patients: A systematic review and meta-analysis. Resuscitation 2019, 138, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.W.; Zhang, S.; Gao, H.; Li, C.; Zhang, M.X. Prognostic Role of Optic Nerve Sheath Diameter for Neurological Outcomes in Post-Cardiac Arrest Patients: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2020, 2020, 5219367. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Holling, H.; Böhning, W.; Böhning, D. Likelihood-Based Clustering of Meta-Analytic SROC Curves. Psychometrika 2012, 77, 106–126. [Google Scholar] [CrossRef]
- Zamora, J.; Abraira, V.; Muriel, A.; Khan, K.; Coomarasamy, A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Med. Res. Methodol 2006, 6, 31. [Google Scholar] [CrossRef]
- Jones, C.M.; Athanasiou, T. Summary receiver operating characteristic curve analysis techniques in the evaluation of diagnostic tests. Ann. Thorac. Surg. 2005, 79, 16–20. [Google Scholar] [CrossRef]
- Ertl, M.; Weber, S.; Hammel, G.; Schroeder, C.; Krogias, C. Transorbital Sonography for Early Prognostication of Hypoxic-Ischemic Encephalopathy After Cardiac Arrest. J. Neuroimaging 2018, 28, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Hwan Kim, Y.; Ho Lee, J.; Kun Hong, C.; Won Cho, K.; Hoon Yeo, J.; Ju Kang, M.; Weon Kim, Y.; Yul Lee, K.; Joo Kim, J.; Youn Hwang, S. Feasibility of optic nerve sheath diameter measured on initial brain computed tomography as an early neurologic outcome predictor after cardiac arrest. Acad. Emerg. Med. 2014, 21, 1121–1128. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H.; Lee, S.H.; Oh, J.H.; Cho, I.S.; Lee, Y.H.; Han, C.; Choi, W.J.; Sohn, Y.D. Optic nerve sheath diameter measured using early unenhanced brain computed tomography shows no correlation with neurological outcomes in patients undergoing targeted temperature management after cardiac arrest. Resuscitation 2018, 128, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Cho, Y.; You, Y.; Min, J.H.; Jeong, W.; Ahn, H.J.; Kang, C.; Yoo, I.; Ryu, S.; Kim, S.W.; et al. Optimal timing to measure optic nerve sheath diameter as a prognostic predictor in post-cardiac arrest patients treated with targeted temperature management. Resuscitation 2019, 143, 173–179. [Google Scholar] [CrossRef]
- Ryu, J.A.; Chung, C.R.; Cho, Y.H.; Sung, K.; Suh, G.Y.; Park, T.K.; Song, Y.B.; Hahn, J.Y.; Choi, J.H.; Gwon, H.C.; et al. The association of findings on brain computed tomography with neurologic outcomes following extracorporeal cardiopulmonary resuscitation. Crit. Care 2017, 21, 15. [Google Scholar] [CrossRef] [Green Version]
- Ueda, T.; Ishida, E.; Kojima, Y.; Yoshikawa, S.; Yonemoto, H. Sonographic Optic Nerve Sheath Diameter: A Simple and Rapid Tool to Assess the Neurologic Prognosis After Cardiac Arrest. J. Neuroimaging 2015, 25, 927–930. [Google Scholar] [CrossRef]
- Geeraerts, T.; Duranteau, J.; Benhamou, D. Ocular sonography in patients with raised intracranial pressure: The papilloedema revisited. Crit. Care 2008, 12, 150. [Google Scholar] [CrossRef] [PubMed]
- Selhorst, J.B.; Chen, Y. The optic nerve. Semin. Neurol. 2009, 29, 29–35. [Google Scholar] [CrossRef]
- Sheth, S.; Branstetter, B.F.; Escott, E.J. Appearance of normal cranial nerves on steady-state free precession MR images. Radiographics 2009, 29, 1045–1055. [Google Scholar] [CrossRef]
- Sekhon, M.S.; Griesdale, D.E.; Robba, C.; McGlashan, N.; Needham, E.; Walland, K.; Shook, A.C.; Smielewski, P.; Czosnyka, M.; Gupta, A.K.; et al. Optic nerve sheath diameter on computed tomography is correlated with simultaneously measured intracranial pressure in patients with severe traumatic brain injury. Intensive Care Med. 2014, 40, 1267–1274. [Google Scholar] [CrossRef]
- Sekhon, M.S.; McBeth, P.; Zou, J.; Qiao, L.; Kolmodin, L.; Henderson, W.R.; Reynolds, S.; Griesdale, D.E. Association between optic nerve sheath diameter and mortality in patients with severe traumatic brain injury. Neurocrit. Care 2014, 21, 245–252. [Google Scholar] [CrossRef]
- Helmke, K.; Hansen, H.C. Fundamentals of transorbital sonographic evaluation of optic nerve sheath expansion under intracranial hypertension II. Patient study. Pediatric Radiol. 1996, 26, 706–710. [Google Scholar] [CrossRef] [PubMed]
- Launey, Y.; Nesseler, N.; Le Maguet, P.; Mallédant, Y.; Seguin, P. Effect of osmotherapy on optic nerve sheath diameter in patients with increased intracranial pressure. J. Neurotrauma 2014, 31, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Mao, W. Regarding “Diagnostic performance of optic nerve sheath diameter for predicting neurologic outcome in post-cardiac arrest patients: A systematic review and meta-analysis”. Resuscitation 2020, 154, 25. [Google Scholar] [CrossRef] [PubMed]
- Na, M.K.; Kim, W.; Lim, T.H.; Jang, B.; Cho, Y.; Choi, K.S.; Shin, H.G.; Ahn, C.; Lee, J.; Kim, J.G. Gray matter to white matter ratio for predicting neurological outcomes in patients treated with target temperature management after cardiac arrest: A systematic review and meta-analysis. Resuscitation 2018, 132, 21–28. [Google Scholar] [CrossRef]
- Scheel, M.; Storm, C.; Gentsch, A.; Nee, J.; Luckenbach, F.; Ploner, C.J.; Leithner, C. The prognostic value of gray-white-matter ratio in cardiac arrest patients treated with hypothermia. Scand J. Trauma Resusc. Emerg Med. 2013, 21, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.G.; Ahn, C.; Shin, H.; Kim, W.; Lim, T.H.; Jang, B.H.; Cho, Y.; Choi, K.S.; Lee, J.; Na, M.K. Efficacy of the cooling method for targeted temperature management in post-cardiac arrest patients: A systematic review and meta-analysis. Resuscitation 2020, 148, 14–24. [Google Scholar] [CrossRef]
- Shin, H.; Kim, J.G.; Kim, W.; Lim, T.H.; Jang, B.H.; Cho, Y.; Choi, K.S.; Ahn, C.; Lee, J.; Na, M.K. Procalcitonin as a prognostic marker for outcomes in post-cardiac arrest patients: A systematic review and meta-analysis. Resuscitation 2019, 138, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Jun, J.S.; Kim, R. Ultrasonographic measurement of the optic nerve sheath diameter and its association with eyeball transverse diameter in 585 healthy volunteers. Sci. Rep. 2017, 7, 15906. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, J.; Shin, H.; Kim, C.; Choi, H.J.; Kang, B.S. Predictive Utility of Changes in Optic Nerve Sheath Diameter after Cardiac Arrest for Neurologic Outcomes. Int. J. Environ. Res. Public Health 2021, 18, 6567. [Google Scholar] [CrossRef]
- Wang, L.; Feng, L.; Yao, Y.; Deng, F.; Wang, Y.; Feng, J.; Xing, Y. Ultrasonographic Evaluation of Optic Nerve Sheath Diameter among Healthy Chinese Adults. Ultrasound Med. Biol. 2016, 42, 683–688. [Google Scholar] [CrossRef]
- Maude, R.R.; Hossain, M.A.; Hassan, M.U.; Osbourne, S.; Sayeed, K.L.; Karim, M.R.; Samad, R.; Borooah, S.; Dhillon, B.; Day, N.P. Transorbital sonographic evaluation of normal optic nerve sheath diameter in healthy volunteers in Bangladesh. PLoS ONE 2013, 8, e81013. [Google Scholar]
- Romagnuolo, L.; Tayal, V.; Tomaszewski, C.; Saunders, T.; Norton, H.J. Optic nerve sheath diameter does not change with patient position. Am. J. Emerg. Med. 2005, 23, 686–688. [Google Scholar] [CrossRef]
- Abegão Pinto, L.; Vandewalle, E.; Pronk, A.; Stalmans, I. Intraocular pressure correlates with optic nerve sheath diameter in patients with normal tension glaucoma. Graefe’s Arch. Clin. Exp. Ophthalmol. 2012, 250, 1075–1080. [Google Scholar] [CrossRef]
- Lee, B.K.; Kim, W.Y.; Shin, J.; Oh, J.S.; Wee, J.H.; Cha, K.C.; Park, Y.; Choi, J.H.; Jeung, K.W. Prognostic value of gray matter to white matter ratio in hypoxic and non-hypoxic cardiac arrest with non-cardiac etiology. Am. J. Emerg. Med. 2016, 34, 1583–1588. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Inclusion Period | Study Type | Sample Size, CA Type | PNO (CPC 3–5), n (%) | Death, n (%) | ONSD Measurement | Outcome Measurement | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Modality | Location | Time after ROSC | Timepoint | ||||||||
| Chae | 2016 | Korea | 2009–2013 | sROS | 119 | 74 (62.2) | NR | CT | 3 mm behind the globe | 0–6 h | 1 month |
| Chelly | 2016 | France | 2011–2013 | mPOS | 36 | 22 (61.1) † | 17 (47.2) | US | 3 mm behind the globe | 24 h | at hospital discharge |
| Ertl | 2018 | Germany | 2015–2017 | mPOS | 49 | NR | 25 (51.0) | US | 3 mm behind the globe | 0–24 h | at hospital discharge |
| Kim | 2014 | Korea | 2012–2013 | sROS | 91 | 68 (74.7) | NR | CT | 3 mm behind the globe | 0–24 h | at hospital discharge |
| Lee | 2018 | Korea | 2015–2016 | mPOS | 329 * | 230 (69.9) | 167 (50.8) | CT | 3 mm behind the globe | 0–2 h | 6 months |
| Park | 2019 | Korea | 2018–2019 | sPOS | 36 * | 18 (50.0) | NR | US | 3 mm behind the globe | 24 h | 3 months |
| Rush | 2017 | Canada | 2009–2013 | sROS | 72 | 54 (75.0) | 53 (73.6) † | CT | 3 mm behind the globe | 0–48 h | at hospital discharge |
| Ryu | 2017 | Korea | 2005–2015 | sROS | 42 | 23 (54.8) | 19 (45.2) † | CT | 3 mm behind the globe | 0–48 h | at hospital discharge |
| Ueda | 2015 | Japan | 2013–2014 | sROS | 17 | 11 (64.7) ** | NR | US | 3 mm behind the globe | 12–72 h | 1 month |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-G.; Kim, W.; Shin, H.; Lim, T.-H.; Jang, B.-H.; Cho, Y.; Choi, K.-S.; Na, M.-K.; Ahn, C.; Lee, J. Optic Nerve Sheath Diameter for Predicting Outcomes in Post-Cardiac Arrest Syndrome: An Updated Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 500. https://doi.org/10.3390/jpm12030500
Kim J-G, Kim W, Shin H, Lim T-H, Jang B-H, Cho Y, Choi K-S, Na M-K, Ahn C, Lee J. Optic Nerve Sheath Diameter for Predicting Outcomes in Post-Cardiac Arrest Syndrome: An Updated Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(3):500. https://doi.org/10.3390/jpm12030500
Chicago/Turabian StyleKim, Jae-Guk, Wonhee Kim, Hyungoo Shin, Tae-Ho Lim, Bo-Hyoung Jang, Youngsuk Cho, Kyu-Sun Choi, Min-Kyun Na, Chiwon Ahn, and Juncheol Lee. 2022. "Optic Nerve Sheath Diameter for Predicting Outcomes in Post-Cardiac Arrest Syndrome: An Updated Systematic Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 3: 500. https://doi.org/10.3390/jpm12030500
APA StyleKim, J. -G., Kim, W., Shin, H., Lim, T. -H., Jang, B. -H., Cho, Y., Choi, K. -S., Na, M. -K., Ahn, C., & Lee, J. (2022). Optic Nerve Sheath Diameter for Predicting Outcomes in Post-Cardiac Arrest Syndrome: An Updated Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 12(3), 500. https://doi.org/10.3390/jpm12030500