
Prediction of Successful Pharmacological Cardioversion in Acute Symptomatic Atrial Fibrillation: The Successful Intravenous Cardioversion for Atrial Fibrillation (SIC-AF) Score

 , , ,
, , ,  ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design/Setting
2.2. AF Registry
2.3. Prediction Model
2.4. Statistical Methods
3. Results
3.1. Model Development
3.2. Model Validation
4. Discussion
4.1. SIC-AF Predictors
4.2. Treatment Efficacy
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haendel, M.A.; Chute, C.G.; Robinson, P.N. Classification, Ontology and Precision Medicine. N. Engl. J. Med. 2018, 379, 1452–1462. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.C.; Lamas, G.A.; Balu, S.; Spalding, J.; Wang, Q.; Pashos, C.L. Direct Treatment Cost of Atrial Fibrillation in the Elderly American Population: A Medicare Perspective. J. Med. Econ. 2008, 11, 281–298. [Google Scholar] [CrossRef] [PubMed]
- Ringborg, A.; Nieuwlaat, R.; Lindgren, P.; Jönsson, B.; Fidan, D.; Maggioni, A.P.; Lopez-Sendon, J.; Stepinska, J.; Cokkinos, D.V.; Crijns, H.J. Costs of Atrial Fibrillation in Five European Countries: Results from the Euro Heart Survey on Atrial Fibrillation. Europace 2008, 10, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Friberg, J.; Buch, P.; Scharling, H.; Gadsbphioll, N.; Jensen, G.B. Rising Rates of Hospital Admissions for Atrial Fibrillation. Epidemiology 2003, 14, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Rozen, G.; Hosseini, S.M.; Kaadan, M.I.; Biton, Y.; Heist, E.K.; Vangel, M.; Mansour, M.C.; Ruskin, J.N. Emergency Department Visits for Atrial Fibrillation in the United States: Trends in Admission Rates and Economic Burden from 2007 to 2014. J. Am. Heart Assoc. 2018, 7, e00902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, D.; Talajic, M.; Nattel, S.; Wyse, D.G.; Dorian, P.; Lee, K.L.; Bourassa, M.G.; Arnold, J.M.O.; Buxton, A.E.; Camm, A.J.; et al. Rhythm Control versus Rate Control for Atrial Fibrillation and Heart Failure. N. Engl. J. Med. 2008, 358, 2667–2677. [Google Scholar] [CrossRef]
- Van Gelder, I.C.; Groenveld, H.F.; Crijns, H.J.G.M.; Tuininga, Y.; Tijssen, J.G.P.; Alings, A.M.; Hillege, H.L.; Bergsma-Kadijk, J.A.; Cornel, J.; Kamp, O.; et al. Lenient versus Strict Rate Control in Patients with Atrial Fibrillation. N. Engl. J. Med. 2010, 362, 1363–1373. [Google Scholar] [CrossRef] [Green Version]
- Kirchhof, P.; Bax, J.; Blomstrom-Lundquist, C.; Calkins, H.; Camm, A.J.; Cappato, R.; Cosio, F.; Crijns, H.; Diener, H.-C.; Goette, A.; et al. Early and Comprehensive Management of Atrial Fibrillation: Executive Summary of the Proceedings from the 2nd AFNET-EHRA Consensus Conference ‘Research Perspectives in AF’. Eur. Heart J. 2009, 30, 2969–2977. [Google Scholar] [CrossRef] [Green Version]
- Pluymaekers, N.A.; Dudink, E.A.; Luermans, J.G.; Meeder, J.G.; Lenderink, T.; Widdershoven, J.; Bucx, J.J.; Rienstra, M.; Kamp, O.; Van Opstal, J.M.; et al. Early or Delayed Cardioversion in Recent-Onset Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1499–1508. [Google Scholar] [CrossRef]
- Probst, M.A.; Noseworthy, P.A.; Brito, J.P.; Hess, E.P. Shared Decision-Making as the Future of Emergency Cardiology. Can. J. Cardiol. 2018, 34, 117–124. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, ehaa612. [Google Scholar] [CrossRef]
- Berg, D.D.; Ruff, C.T.; Jarolim, P.; Giugliano, R.P.; Nordio, F.; Lanz, H.J.; Mercuri, M.F.; Antman, E.M.; Braunwald, E.; Morrow, D.A. Performance of the ABC Scores for Assessing the Risk of Stroke or Systemic Embolism and Bleeding in Patients With Atrial Fibrillation in ENGAGE AF-TIMI 48. Circulation 2019, 139, 760–771. [Google Scholar] [CrossRef] [PubMed]
- Hijazi, Z.; Oldgren, J.; Lindbäck, J.; Alexander, J.H.; Connolly, S.J.; Eikelboom, J.W.; Ezekowitz, M.D.; Held, C.; Hylek, E.M.; Lopes, R.D.; et al. The Novel Biomarker-Based ABC (Age, Biomarkers, Clinical History)-Bleeding Risk Score for Patients with Atrial Fibrillation: A Derivation and Validation Study. Lancet 2016, 387, 2302–2311. [Google Scholar] [CrossRef]
- Hijazi, Z.; Oldgren, J.; Lindbäck, J.; Alexander, J.H.; Connolly, S.J.; Eikelboom, J.W.; Ezekowitz, M.D.; Held, C.; Hylek, E.M.; Lopes, R.D.; et al. A Biomarker-Based Risk Score to Predict Death in Patients with Atrial Fibrillation: The ABC (Age, Biomarkers, Clinical History) Death Risk Score. Eur. Heart J. 2017, 39, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Niederdöckl, J.; Simon, A.; Cacioppo, F.; Buchtele, N.; Merrelaar, A.; Schütz, N.; Schnaubelt, S.; O Spiel, A.; Roth, D.; Schörgenhofer, C.; et al. Predicting Spontaneous Conversion to Sinus Rhythm in Symptomatic Atrial Fibrillation: The ReSinus Score. Eur. J. Intern. Med. 2020, 83, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Niederdöckl, J.; Simon, A.; Schnaubelt, S.; Schuetz, N.; Laggner, R.; Sulzgruber, P.; Spiel, A.O.; Herkner, H.; Laggner, A.N.; Domanovits, H. Cardiac Biomarkers Predict Mortality in Emergency Patients Presenting with Atrial Fibrillation. Heart 2018, 105, 482–488. [Google Scholar] [CrossRef] [Green Version]
- Steyerberg, E.W.; Vergouwe, Y. Towards Better Clinical Prediction Models: Seven Steps for Development and an ABCD for Validation. Eur. Heart J. 2014, 35, 1925–1931. [Google Scholar] [CrossRef] [Green Version]
- Kafkas, N.V.; Patsilinakos, S.P.; Mertzanos, G.A.; Papageorgiou, K.I.; Chaveles, J.I.; Dagadaki, O.K.; Kelesidis, K.M. Conversion Efficacy of Intravenous Ibutilide Compared with Intravenous Amiodarone in Patients with Recent-Onset Atrial Fibrillation and Atrial Flutter. Int. J. Cardiol. 2007, 118, 321–325. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. J. Clin. Epidemiol. 2015, 68, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Wijffels, M.C.; Kirchhof, C.J.; Dorland, R.; Allessie, M.A. Atrial Fibrillation Begets Atrial Fibrillation: A Study in Awake Chronically Instrumented Goats. Circulation 1995, 92, 1954–1968. [Google Scholar] [CrossRef]
- Allessie, M.A.; de Groot, N.M.; Houben, R.P.; Schotten, U.; Boersma, E.; Smeets, J.L.; Crijns, H.J. Electropathological Substrate of Long-Standing Persistent Atrial Fibrillation in Patients with Structural Heart Disease: Longitudinal Dissociation. Circulation. Arrhythmia Electrophysiol. 2010, 3, 606–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nattel, S.; Harada, M. Atrial Remodeling and Atrial Fibrillation. J. Am. Coll. Cardiol. 2014, 63, 2335–2345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ausma, J.; Wijffels, M.; Thoné, F.; Wouters, L.; Allessie, M.; Borgers, M. Structural Changes of Atrial Myocardium Due to Sustained Atrial Fibrillation in the Goat. Circulation 1997, 96, 3157–3163. [Google Scholar] [CrossRef]
- TThijssen, V.L.; Ausma, J.; Liu, G.S.; Allessie, M.A.; van Eys, G.J.; Borgers, M. Structural Changes of Atrial Myocardium during Chronic Atrial Fibrillation. Cardiovasc. Pathol. Off. J. Soc. Cardiovasc. Pathol. 2000, 9, 17–28. [Google Scholar] [CrossRef]
- Zhang, L.; Huang, B.; Scherlag, B.J.; Ritchey, J.W.; Embi, A.A.; Hu, J.; Hou, Y.; Po, S.S. Structural Changes in the Progression of Atrial Fibrillation: Potential Role of Glycogen and Fibrosis as Perpetuating Factors. Int. J. Clin. Exp. Pathol. 2015, 8, 1712–1718. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics and Baseline Characteristics | ||
|---|---|---|
| Derivation Cohort | Validation Cohort | |
| n = 1260 | n = 1146 | |
| General characteristics | ||
| Age, years (IQR) | 69 (58–76) | 68 (58–75) |
| Female sex, n (%) | 553 (43.9) | 453 (39.5) |
| Comorbidities | ||
| Heart failure, n (%) | 131 (10.4) | 316(27.6) |
| Hypertension, n (%) | 794 (63.0) | 663 (57.9) |
| Diabetes mellitus, n (%) | 175 (13.9) | 176 (15.4) |
| Prior stroke, n (%) | 111 (8.8) | 77 (6.7) |
| Coronary artery disease, n (%) | 223 (17.7) | 203 (17.7) |
| Prior myocardial infarction, n (%) | 120 (9.5) | 93 (8.1) |
| Peripheral artery disease, n (%) | 55 (4.4) | 49 (4.3) |
| COPD, n (%) | 94 (7.5) | 108 (9.4) |
| Valvular disease, n (%) | 352 (27.9) | 267 (23.3) |
| Current smoker, n (%) | 101 (8.0) | 30 (2.6) |
| AF history | ||
| First AF episode, n (%) | 182 (14.4) | 152 (13.2) |
| Heart rate, bpm (IQR) | 130 (111–146) | 127 (102–141) |
| Atrial flutter, n (%) | 276 (22) | 129 (11) |
| Duration of AF symptoms, h (IQR) | 6 (2–24) | 8 (3–24) |
| Prior electrical cardioversion, n (%) | 490 (39) | 235 (21) |
| CHA2DS2–VASc (IQR) | 3(1–4) | 2 (1–4) |
| Laboratory | ||
| Haematocrit, % (IQR) | 41(38–45) | 42 (38–45) |
| WBC, G/l (IQR) | 8 (7–10) | 8 (7–10) |
| Creatinine, mg/dl (IQR) | 1.0 (0.8–1.2) | 1.0 (0.9–1.2) |
| NT–proBNP, pg/mL (IQR) | 1160 (409–2883) | 1185 (382–2951 |
| hs–Troponin T, ng/l (IQR) | 14 (9–26) | 15 (8–29) |
| CRP, mg/dl (IQR) | 0.3 (0.1–0.9) | 0.4 (0.2–1.3) |
| INR, (IQR) | 1.2 (1.0–2.4) | 2.5 (1.7–3.3) |
| Treatment | ||
| Rate control, n (%) | 192 (15.2) | 399 (34.8) |
| Rhythm control, n (%) | 1068 (84.8) | 747 (65.2) |
| Electrical cardioversion, n (%) | 647 (51.4) | 417 (36.4) |
| Vernakalant, n (%) | 113 (9.0) | 80 (7.0) |
| Ibutilide, n (%) | 100 (7.9) | 71 (6.2) |
| Amiodarone, n (%) | 208 (16.) | 179 (15.6) |
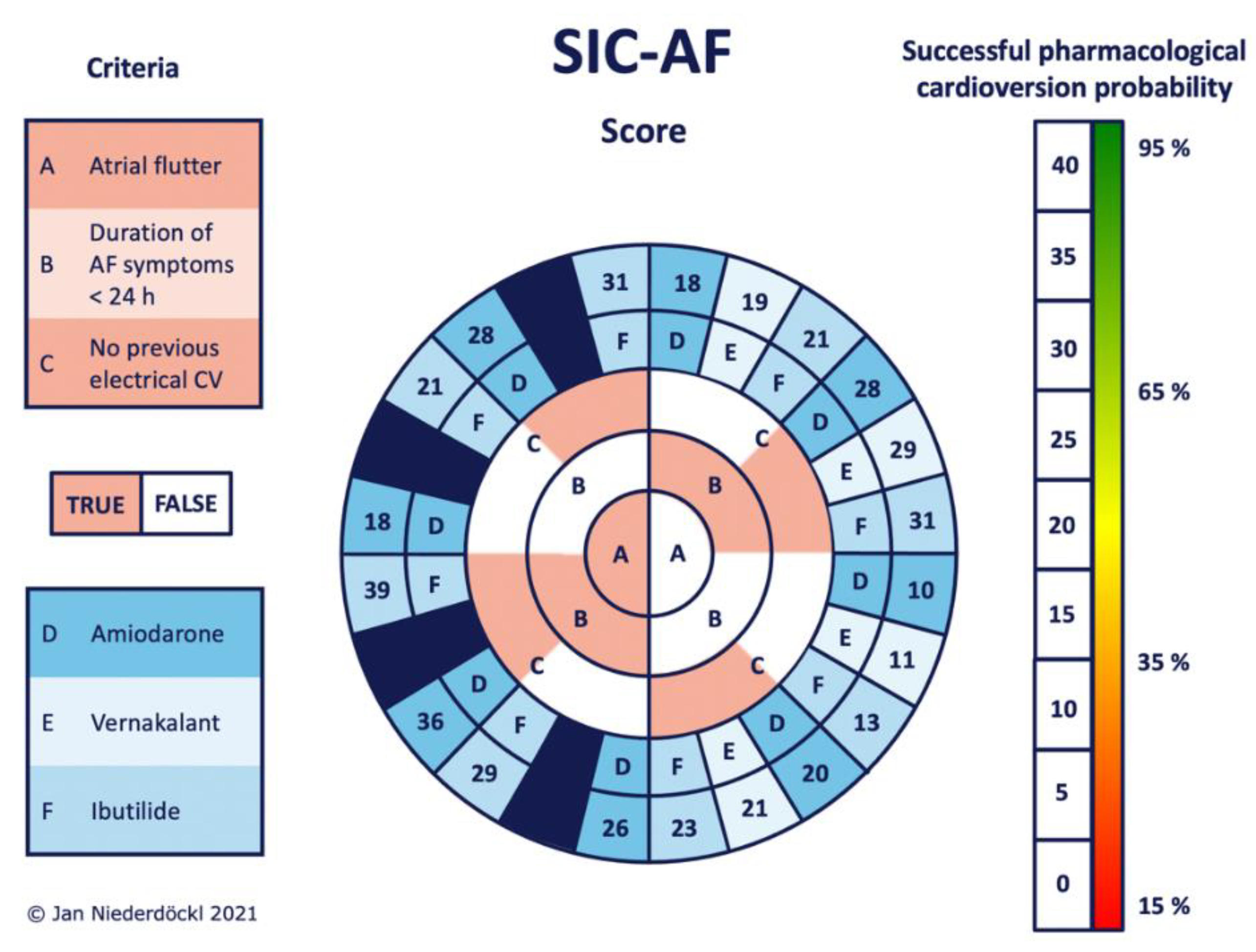
| Predictor | Coefficient | 95% CI | p | Score Points |
|---|---|---|---|---|
| Atrial flutter | 0.82 | (0.28–1.35) | 0.003 | 8 |
| Duration of AF symptoms < 24 h | 0.83 | (0.38–1.38) | <0.001 | 8 |
| No previous electrical cardioversion | 0.98 | (0.52–1.45) | <0.001 | 10 |
| Antiarrhythmic agent | ||||
| Amiodarone | Ref | 10 | ||
| Vernakalant | 1.13 | (0.59–1.67) | <0.001 | 11 |
| Ibutilide | 1.32 | (0.74–1.91) | <0.001 | 13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niederdöckl, J.D.; Simon, A.; Buchtele, N.; Schütz, N.; Cacioppo, F.; Oppenauer, J.; Gupta, S.; Lutnik, M.; Schnaubelt, S.; Spiel, A.; et al. Prediction of Successful Pharmacological Cardioversion in Acute Symptomatic Atrial Fibrillation: The Successful Intravenous Cardioversion for Atrial Fibrillation (SIC-AF) Score. J. Pers. Med. 2022, 12, 544. https://doi.org/10.3390/jpm12040544
Niederdöckl JD, Simon A, Buchtele N, Schütz N, Cacioppo F, Oppenauer J, Gupta S, Lutnik M, Schnaubelt S, Spiel A, et al. Prediction of Successful Pharmacological Cardioversion in Acute Symptomatic Atrial Fibrillation: The Successful Intravenous Cardioversion for Atrial Fibrillation (SIC-AF) Score. Journal of Personalized Medicine. 2022; 12(4):544. https://doi.org/10.3390/jpm12040544
Chicago/Turabian StyleNiederdöckl, Jan Daniel, Alexander Simon, Nina Buchtele, Nikola Schütz, Filippo Cacioppo, Julia Oppenauer, Sophie Gupta, Martin Lutnik, Sebastian Schnaubelt, Alexander Spiel, and et al. 2022. "Prediction of Successful Pharmacological Cardioversion in Acute Symptomatic Atrial Fibrillation: The Successful Intravenous Cardioversion for Atrial Fibrillation (SIC-AF) Score" Journal of Personalized Medicine 12, no. 4: 544. https://doi.org/10.3390/jpm12040544
APA StyleNiederdöckl, J. D., Simon, A., Buchtele, N., Schütz, N., Cacioppo, F., Oppenauer, J., Gupta, S., Lutnik, M., Schnaubelt, S., Spiel, A., Roth, D., Wimbauer, F., Fegers-Wustrow, I., Esefeld, K., Halle, M., Scharhag, J., Laschitz, T., Herkner, H., Domanovits, H., & Schwameis, M. (2022). Prediction of Successful Pharmacological Cardioversion in Acute Symptomatic Atrial Fibrillation: The Successful Intravenous Cardioversion for Atrial Fibrillation (SIC-AF) Score. Journal of Personalized Medicine, 12(4), 544. https://doi.org/10.3390/jpm12040544