
Prevalence of New-Onset Atrial Fibrillation and Associated Outcomes in Patients with Sepsis: A Systematic Review and Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Studies Selection
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Quality Assessment
2.5. Outcomes Definition
2.6. Statistical Analysis
3. Results
3.1. Systematic Review of the Included Studies
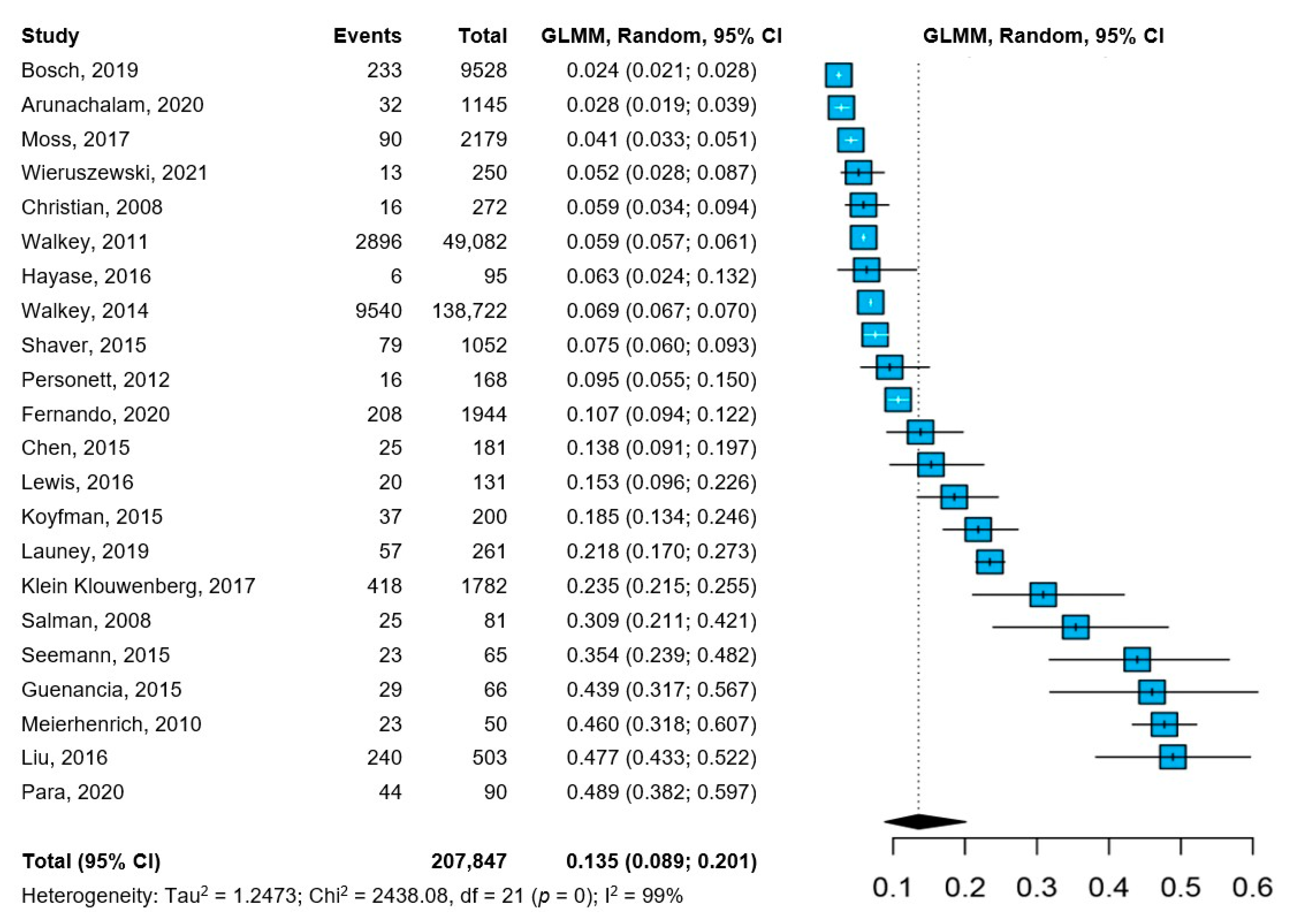
3.2. Prevalence of NOAF in Patients with Sepsis
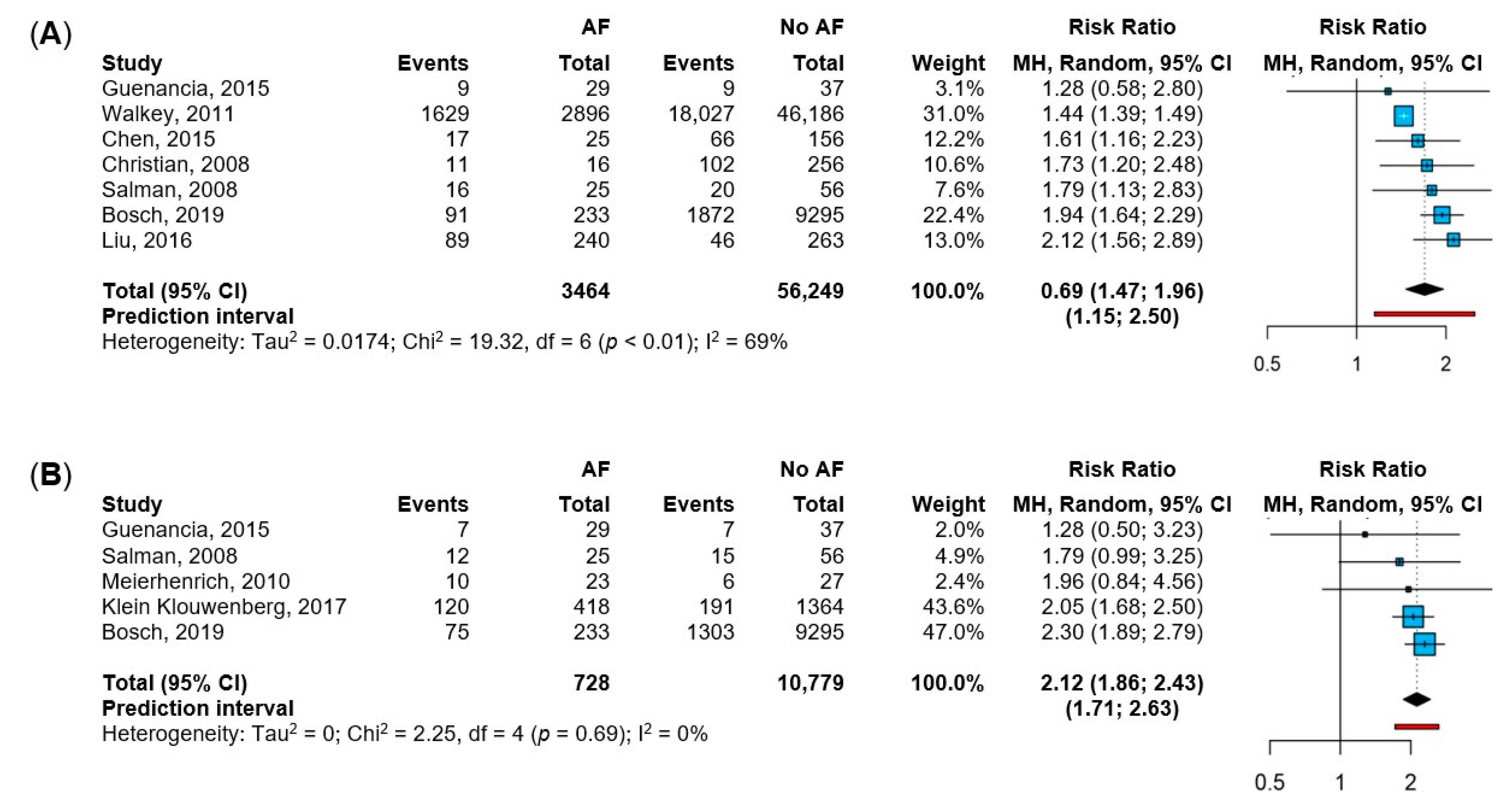
3.3. In-Hospital and ICU Mortality
4. Discussion
4.1. Prevalence of NOAF Is Heterogeneous among Sepsis Patients
4.2. NOAF Entails Worse Prognosis during Sepsis
4.3. Future Perspectives on NOAF Management
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA J. Am. Med. Assoc. 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Bauer, M.; Gerlach, H.; Vogelmann, T.; Preissing, F.; Stiefel, J.; Adam, D. Mortality in Sepsis and Septic Shock in Europe, North America and Australia between 2009 and 2019-Results from a Systematic Review and Meta-Analysis. Crit. Care 2020, 24, 239. [Google Scholar] [CrossRef]
- Merx, M.W.; Weber, C. Sepsis and the Heart. Circulation 2007, 116, 793–802. [Google Scholar] [CrossRef] [Green Version]
- Walkey, A.J.; McManus, D. When Rhythm Changes Cause the Blues: New-Onset Atrial Fibrillation during Sepsis. Am. J. Respir. Crit. Care Med. 2017, 195, 152–153. [Google Scholar] [CrossRef] [Green Version]
- Boos, C.J. Infection and Atrial Fibrillation: Inflammation Begets AF. Eur. Heart J. 2020, 41, 1120–1122. [Google Scholar] [CrossRef]
- Induruwa, I.; Hennebry, E.; Hennebry, J.; Thakur, M.; Warburton, E.; Khadjooi, K. Sepsis-Driven Atrial Fibrillation and Ischaemic Stroke. Is There Enough Evidence to Recommend Anticoagulation? Eur. J. Intern. Med. 2021; in press. [Google Scholar] [CrossRef]
- Tralhão, A.; Póvoa, P. Cardiovascular Events after Community-Acquired Pneumonia: A Global Perspective with Systematic Review and Meta-Analysis of Observational Studies. J. Clin. Med. 2020, 9, 414. [Google Scholar] [CrossRef] [Green Version]
- De Miguel-Yanes, J.M.; Jimenez-Garcia, R.; de Miguel-Diez, J.; Hernandez-Barrera, V.; Mendez-Bailon, M.; Zamorano-Leon, J.J.; Lopez-de-Andres, A. The Influence of Atrial Fibrillation on In-Hospital Mortality in People with Hospital-Acquired Pneumonia: An Observational, Sex-Stratified Study. J. Clin. Med. 2022, 11, 1179. [Google Scholar] [CrossRef]
- Romiti, G.F.; Corica, B.; Lip, G.Y.H.; Proietti, M. Prevalence and Impact of Atrial Fibrillation in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 2490. [Google Scholar] [CrossRef]
- Bosch, N.A.; Rucci, J.M.; Massaro, J.M.; Winter, M.R.; Quinn, E.K.; Chon, K.H.; McManus, D.D.; Walkey, A.J. Comparative Effectiveness of Heart Rate Control Medications for the Treatment of Sepsis-Associated Atrial Fibrillation. Chest 2021, 159, 1452–1459. [Google Scholar] [CrossRef]
- Walkey, A.J.; Evans, S.R.; Winter, M.R.; Benjamin, E.J. Practice Patterns and Outcomes of Treatments for Atrial Fibrillation during Sepsis a Propensity-Matched Cohort Study. Chest 2016, 149, 74–83. [Google Scholar] [CrossRef] [Green Version]
- Walkey, A.J.; Wiener, R.S.; Ghobrial, J.M.; Curtis, L.H.; Benjamin, E.J. Incident Stroke and Mortality Associated with New-Onset Atrial Fibrillation in Patients Hospitalized with Severe Sepsis. JAMA J. Am. Med. Assoc. 2011, 306, 2248–2255. [Google Scholar] [CrossRef] [Green Version]
- Viswanathan, M.; Ansari, M.T.; Berkman, N.D.; Chang, S.; Hartling, L.; McPheeters, M.; Santaguida, P.L.; Shamliyan, T.; Singh, K.; Tsertsvadze, A.; et al. Assessing the Risk of Bias of Individual Studies in Systematic Reviews of Health Care Interventions. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Stijnen, T.; Hamza, T.H.; Özdemir, P. Random Effects Meta-Analysis of Event Outcome in the Framework of the Generalized Linear Mixed Model with Applications in Sparse Data. Stat. Med. 2010, 29, 3046–3067. [Google Scholar] [CrossRef]
- IntHout, J.; Ioannidis, J.P.A.; Rovers, M.M.; Goeman, J.J. Plea for Routinely Presenting Prediction Intervals in Meta-Analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef] [Green Version]
- Riley, R.D.; Higgins, J.P.T.; Deeks, J.J. Interpretation of Random Effects Meta-Analyses. BMJ 2011, 342, 964–967. [Google Scholar] [CrossRef] [Green Version]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis in R: A Hands-On Guide; Chapman and Hall: London, UK; CRC: Boca Raton, FL, USA, 2021. [Google Scholar]
- Arunachalam, K.; Kalyan Sundaram, A.; Jha, K.; Thakur, L.; Pond, K. Evaluation of Anticoagulation Practice With New-Onset Atrial Fibrillation in Patients with Sepsis and Septic Shock in Medical Intensive Care Unit: A Retrospective Observational Cohort Study. Cureus 2020, 12, e10026. [Google Scholar] [CrossRef]
- Bosch, N.A.; Massaro, J.M.; Winter, M.R.; Quinn, E.K.; Chon, K.H.; McManus, D.D.; Walkey, A.J. New-Onset Atrial Fibrillation as a Sepsis-Defining Organ Failure. Ann. Am. Thorac. Soc. 2019, 16, 1332–1334. [Google Scholar] [CrossRef]
- Chen, A.Y.; Sokol, S.S.; Kress, J.P.; Lat, I. New-Onset Atrial Fibrillation Is an Independent Predictor of Mortality in Medical Intensive Care Unit Patients. Ann. Pharmacother. 2015, 49, 523–527. [Google Scholar] [CrossRef]
- Christian, S.-A.; Schorr, C.; Ferchau, L.; Jarbrink, M.E.; Parrillo, J.E.; Gerber, D.R. Clinical Characteristics and Outcomes of Septic Patients with New-Onset Atrial Fibrillation. J. Crit. Care 2008, 23, 532–536. [Google Scholar] [CrossRef]
- Fernando, S.M.; Mathew, R.; Hibbert, B.; Rochwerg, B.; Munshi, L.; Walkey, A.J.; Møller, M.H.; Simard, T.; Di Santo, P.; Ramirez, F.D.; et al. New-Onset Atrial Fibrillation and Associated Outcomes and Resource Use among Critically Ill Adults—A Multicenter Retrospective Cohort Study. Crit. Care 2020, 24, 15. [Google Scholar] [CrossRef] [Green Version]
- Guenancia, C.; Binquet, C.; Laurent, G.; Vinault, S.; Bruyère, R.; Prin, S.; Pavon, A.; Charles, P.-E.; Quenot, J.-P. Incidence and Predictors of New-Onset Atrial Fibrillation in Septic Shock Patients in a Medical ICU: Data from 7-Day Holter ECG Monitoring. PLoS ONE 2015, 10, e0127168. [Google Scholar] [CrossRef] [Green Version]
- Hayase, N.; Yamamoto, M.; Asada, T.; Isshiki, R.; Yahagi, N.; Doi, K. Association of Heart Rate with N-Terminal pro-B-Type Natriuretic Peptide in Septic Patients: A Prospective Observational Cohort Study. Shock 2016, 46, 642–648. [Google Scholar] [CrossRef]
- Klein Klouwenberg, P.M.C.; Frencken, J.F.; Kuipers, S.; Ong, D.S.Y.; Peelen, L.M.; Van Vught, L.A.; Schultz, M.J.; Van Der Poll, T.; Bonten, M.J.; Cremer, O.L.; et al. Incidence, Predictors, and Outcomes of New-Onset Atrial Fibrillation in Critically Ill Patients with Sepsis a Cohort Study. Am. J. Respir. Crit. Care Med. 2017, 195, 205–211. [Google Scholar] [CrossRef]
- Koyfman, L.; Brotfain, E.; Kutz, R.; Frenkel, A.; Schwartz, A.; Boniel, A.; Zlotnik, A.; Klein, M. Epidemiology of New-Onset Paroxysmal Atrial Fibrillation in the General Intensive Care Unit Population and after Discharge from ICU. A Retrospective Epidemiological Study. Anaesthesiol. Intensive Ther. 2015, 47, 309–314. [Google Scholar] [CrossRef] [Green Version]
- Launey, Y.; Lasocki, S.; Asehnoune, K.; Gaudriot, B.; Chassier, C.; Cinotti, R.; Maguet, P.L.; Laksiri, L.; Mimoz, O.; Tawa, A.; et al. Impact of Low-Dose Hydrocortisone on the Incidence of Atrial Fibrillation in Patients With Septic Shock: A Propensity Score-Inverse Probability of Treatment Weighting Cohort Study. J. Intensive Care Med. 2019, 34, 238–244. [Google Scholar] [CrossRef]
- Lewis, O.; Ngwa, J.; Gillum, R.F.; Thomas, A.; Davis, W.; Poddar, V.; Adams, G.R.; Mehari, A. Incidence, Risk Factors and Outcomes of New Onset Supraventricular Arrhythmias in African American Patients with Severe Sepsis. Ethn. Dis. 2016, 26, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.C.; Lin, W.Y.; Lin, C.S.; Huang, H.B.; Lin, T.C.; Cheng, S.M.; Yang, S.P.; Lin, J.C.; Lin, W.S. Prognostic Impact of Restored Sinus Rhythm in Patients with Sepsis and New-Onset Atrial Fibrillation. Crit. Care 2016, 20, 373. [Google Scholar] [CrossRef] [Green Version]
- Meierhenrich, R.; Steinhilber, E.; Eggermann, C.; Weiss, M.; Voglic, S.; Bögelein, D.; Gauss, A.; Georgieff, M.; Stahl, W. Incidence and Prognostic Impact of New-Onset Atrial Fibrillation in Patients with Septic Shock: A Prospective Observational Study. Crit. Care 2010, 14, R108. [Google Scholar] [CrossRef] [Green Version]
- Moss, T.J.; Calland, J.F.; Enfield, K.B.; Gomez-Manjarres, D.C.; Ruminski, C.; DiMarco, J.P.; Lake, D.E.; Moorman, J.R. New-Onset Atrial Fibrillation in the Critically Ill. Crit. Care Med. 2017, 45, 790–797. [Google Scholar] [CrossRef]
- Para, O.; Caruso, L.; Corbo, L.; Bacci, F.; Pasqui, N.; Pieralli, F.; Ciarambino, T.; Nozzoli, C. Risk Factors and Outcomes of New-Onset Atrial Fibrillation in Patients Hospitalized in an Internal Medicine Ward: A Case-Control Study. Intern. Emerg. Med. 2020, 15, 251–256. [Google Scholar] [CrossRef]
- Personett, H.A.; Stollings, J.L.; Cha, S.S.; Oyen, L.J. Predictors of Prolonged Vasopressin Infusion for the Treatment of Septic Shock. J. Crit. Care 2012, 27, 318.e7–318.e12. [Google Scholar] [CrossRef] [PubMed]
- Salman, S.; Bajwa, A.; Gajic, O.; Afessa, B. Paroxysmal Atrial Fibrillation in Critically Ill Patients with Sepsis. J. Intensive Care Med. 2008, 23, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Seemann, A.; Boissier, F.; Razazi, K.; Carteaux, G.; de Prost, N.; Brun-Buisson, C.; Mekontso Dessap, A. New-Onset Supraventricular Arrhythmia during Septic Shock: Prevalence, Risk Factors and Prognosis. Ann. Intensive Care 2015, 5, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaver, C.M.; Chen, W.; Janz, D.R.; May, A.K.; Darbar, D.; Bernard, G.R.; Bastarache, J.A.; Ware, L.B. Atrial Fibrillation Is an Independent Predictor of Mortality in Critically Ill Patients. Crit. Care Med. 2015, 43, 2104–2111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walkey, A.J.; Hammill, B.G.; Curtis, L.H.; Benjamin, E.J. Long-Term Outcomes Following Development of New-Onset Atrial Fibrillation during Sepsis. Chest 2014, 146, 1187–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wieruszewski, E.D.; Jones, G.M.; Samarin, M.J.; Kimmons, L.A. Predictors of Dysrhythmias with Norepinephrine Use in Septic Shock. J. Crit. Care 2021, 61, 133–137. [Google Scholar] [CrossRef]
- Korantzopoulos, P.; Letsas, K.P.; Tse, G.; Fragakis, N.; Goudis, C.A.; Liu, T. Inflammation and Atrial Fibrillation: A Comprehensive Review. J. Arrhythmia 2018, 34, 394–401. [Google Scholar] [CrossRef]
- Gundlund, A.; Olesen, J.B.; Butt, J.H.; Christensen, M.A.; Gislason, G.H.; Torp-Pedersen, C.; Køber, L.; Kümler, T.; Fosbøl, E.L. One-Year Outcomes in Atrial Fibrillation Presenting during Infections: A Nationwide Registry-Based Study. Eur. Heart J. 2020, 41, 1112–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, R.; Hanna, B.; Singh, S.; Omar, A.; Deshmukh, A.; Kumar, G.; Foreman, M.G.; Sachdeva, R. Trends and Outcomes in Sepsis Hospitalizations With and Without Atrial Fibrillation: A Nationwide Inpatient Analysis. Crit. Care Med. 2019, 47, E630–E638. [Google Scholar] [CrossRef]
- Xiao, F.-P.; Chen, M.-Y.; Wang, L.; He, H.; Jia, Z.-Q.; Kuai, L.; Zhou, H.-B.; Liu, M.; Hong, M. Outcomes of New-Onset Atrial Fibrillation in Patients with Sepsis: A Systematic Review and Meta-Analysis of 225,841 Patients. Am. J. Emerg. Med. 2021, 42, 23–30. [Google Scholar] [CrossRef]
- Kuipers, S.; Klouwenberg, P.M.K.; Cremer, O.L. Incidence, Risk Factors and Outcomes of New-Onset Atrial Fibrillation in Patients with Sepsis: A Systematic Review. Crit. Care 2014, 18, 688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandhi, S.; Litt, D.; Narula, N. New-Onset Atrial Fibrillation in Sepsis Is Associated with Increased Morbidity and Mortality. Neth. Hear. J. 2015, 23, 82–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanjanahattakij, N.; Rattanawong, P.; Krishnamoorthy, P.; Horn, B.; Chongsathidkiet, P.; Garvia, V.; Putthapiban, P.; Sirinvaravong, N.; Figueredo, V.M. New-Onset Atrial Fibrillation Is Associated with Increased Mortality in Critically Ill Patients: A Systematic Review and Meta-Analysis. Acta Cardiol. 2019, 74, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Simmons, J.; Pittet, J.F. The Coagulopathy of Acute Sepsis. Curr. Opin. Anaesthesiol. 2015, 28, 227–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujishima, S. Organ Dysfunction as a New Standard for Defining Sepsis. Inflamm. Regen. 2016, 36, 24. [Google Scholar] [CrossRef] [Green Version]
- Simons, S.O.; Elliott, A.; Sastry, M.; Hendriks, J.M.; Arzt, M.; Rienstra, M.; Kalman, J.M.; Heidbuchel, H.; Nattel, S.; Wesseling, G.; et al. Chronic Obstructive Pulmonary Disease and Atrial Fibrillation: An Interdisciplinary Perspective. Eur. Heart J. 2021, 42, 532–540. [Google Scholar] [CrossRef]
- Romiti, G.F.; Corica, B.; Pipitone, E.; Vitolo, M.; Raparelli, V.; Basili, S.; Boriani, G.; Harari, S.; Lip, G.Y.H.; Proietti, M. Prevalence, Management and Impact of Chronic Obstructive Pulmonary Disease in Atrial Fibrillation: A Systematic Review and Meta-Analysis of 4,200,000 Patients. Eur. Heart J. 2021, 42, 3541–3554. [Google Scholar] [CrossRef]
- Zhou, X.; Dudley, S.C. Evidence for Inflammation as a Driver of Atrial Fibrillation. Front. Cardiovasc. Med. 2020, 7, 62. [Google Scholar] [CrossRef]
- Steinhagen, F.; Schmidt, S.V.; Schewe, J.C.; Peukert, K.; Klinman, D.M.; Bode, C. Immunotherapy in Sepsis—Brake or Accelerate? Pharmacol. Ther. 2020, 208, 107476. [Google Scholar] [CrossRef]
- Hohmann, C.; Pfister, R.; Mollenhauer, M.; Adler, C.; Kozlowski, J.; Wodarz, A.; Drebber, U.; Wippermann, J.; Michels, G. Inflammatory Cell Infiltration in Left Atrial Appendageal Tissues of Patients with Atrial Fibrillation and Sinus Rhythm. Sci. Rep. 2020, 10, 1685. [Google Scholar] [CrossRef]
- Hemilä, H.; Suonsyrjä, T. Vitamin C for Preventing Atrial Fibrillation in High Risk Patients: A Systematic Review and Meta-Analysis. BMC Cardiovasc. Disord. 2017, 17, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walkey, A.J.; Quinn, E.K.; Winter, M.R.; McManus, D.D.; Benjamin, E.J. Practice Patterns and Outcomes Associated with Use of Anticoagulation among Patients with Atrial Fibrillation during Sepsis. JAMA Cardiol. 2016, 1, 682–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darwish, O.S.; Strube, S.; Nguyen, H.M.; Tanios, M.A. Challenges of Anticoagulation for Atrial Fibrillation in Patients With Severe Sepsis. Ann. Pharmacother. 2013, 47, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- Romiti, G.F.; Proietti, M. Impact of Rate Control in Hospitalized Patients with Atrial Fibrillation and Sepsis. Eur. J. Intern. Med. 2021, 89, 126–128. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Bax, J.J.; Boriani, G.; Dan, G.A.; Fauchier, L.; Kalman, J.M.; Lane, D.A.; Lettino, M.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Region | Design | Setting | Sepsis (n) | NOAF (n) | Age (Y) | Females (%) | Septic Shock (%) | HTN (%) | DM (%) | Outcomes Included ǂ |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Arunachalam 2020 [18] | North America | Retrospective | ICU | 1145 | 32 | NR | NR | NR | NR | NR | None |
| Bosch 2019 [19] | North America | Retrospective | ICU | 9528 | 233 | 66.5 (16.5) | 46.4 | NR | NR | NR | In-hospital mortality, ICU mortality |
| Chen 2015 [20] | North America | Retrospective | ICU | 181 | 25 | NR | NR | 100 | NR | NR | In-hospital mortality |
| Christian 2008 [21] | North America | Retrospective | ICU | 272 | 16 | 62.4 (16.3) | NR | NR | NR | NR | In-hospital mortality |
| Fernando 2020 [22] | North America | Retrospective | ICU | 1944 | 208 | NR | NR | 66.0 | NR | NR | None |
| Guenancia 2015 [23] | Europe | Observational single center | ICU | 66 | 29 | 65.1 (14.4) | 36.4 | 100 | 51.5 | 21.2 | In-hospital mortality |
| Hayase 2016 [24] | Asia | Observational single center | ICU | 95 | 6 | 63.5 (15.1) | 32.6 | NR | NR | NR | None |
| Klein Klouwenberg 2017 [25] | Europe | Retrospective | ICU | 1782 | 418 | 66 * | 41.9 | 29.9 | NR | 16.7 | ICU mortality |
| Koyfman 2015 [26] | Middle East | Retrospective | ICU | 200 | 37 | NR | NR | NR | NR | NR | None |
| Launey 2019 [27] | Europe | Observational multicenter | ICU | 261 | 57 | 63.9 (14.1) | 40.6 | 100 | 59.2 | 15.3 | None |
| Lewis 2016 [28] | North America | Retrospective | ICU | 131 | 20 | 61.6 (13.7) | 51.9 | NR | 71.7 | 40.4 | None |
| Liu 2016 [29] | Asia | Retrospective | ICU | 503 | 240 | 73.2 (14.0) | 38.4 | NR | 59.6 | 36.4 | In-hospital mortality |
| Meierheinrich 2010 [30] | Europe | Observational single center | ICU | 50 | 23 | 66 * | 34 | 100 | 56 | NR | ICU mortality |
| Moss 2017 [31] | North America | Retrospective | ICU | 2179 | 90 | NR | NR | NR | NR | NR | None |
| Para 2020 [32] | Europe | Retrospective | Non-ICU | 90 | 46 | NR | NR | NR | NR | NR | None |
| Personett 2012 [33] | North America | Retrospective | ICU | 168 | 16 | 44.4 (33.7) | 44.6 | 100 | NR | 25.6 | None |
| Salman 2008 [34] | North America | Retrospective | ICU | 81 | 25 | 59.2 (14.5) | 43.0 | 66.7 | 40.0 | 23.0 | In-hospital mortality, ICU mortality |
| Seemann 2015 [35] | Europe | Observational single center | ICU | 65 | 23 | NR | 44.6 | 100 | 35.4 | 20.0 | None |
| Shaver 2015 [36] | North America | Observational single center | ICU | 1052 | 79 | NR | NR | NR | NR | NR | None |
| Walkey 2014 [37] | North America | Administrative database | NR | 138,722 | 9540 | 80 (7.6) | 57.5 | NR | 90.5 | 55.1 | None |
| Walkey 2011 [12] | North America | Administrative database | NR | 49,082 | 2896 | 68.5 (16.4) | 48.3 | NR | 49.8 | 33.6 | In-hospital mortality |
| Wieruszewski 2021 [38] | North America | Retrospective | ICU | 250 | 13 | NR | 46.8 | 100 | NR | NR | None |
| Subgroups | Number of Studies | Pooled Prevalence | 95% CI | I2 |
|---|---|---|---|---|
| Geographical Location (p for subgroup differences ≤ 0.001) | ||||
| North America | 12 | 7.3 | 5.0–10.6 | 97.6 |
| Europe/Middle East | 7 | 32.1 | 23.8–41.6 | 89.9 |
| Asia | 2 | 20.3 | 3.9–61.9 | 97.3 |
| Study Type (p for subgroup differences ≤ 0.001) | ||||
| Administrative database | 2 | 6.4 | 5.7–7.1 | 98.2 |
| Observational | 6 | 22.2 | 11.2–39.2 | 96.5 |
| Retrospective | 14 | 12.1 | 7.0–20.1 | 99.2 |
| Sample size (p for subgroup differences ≤ 0.001) | ||||
| More than 1000 patients | 8 | 6.3 | 3.8–10.3 | 99.4 |
| 100–1000 patients | 8 | 14.4 | 8.5–23.5 | 97.2 |
| Less than 100 patients | 6 | 32.4 | 19.5–48.8 | 86.1 |
| Composition of the cohort (p for subgroup differences = 0.889) | ||||
| Only sepsis patients | 15 | 13.3 | 7.9–21.4 | 99.3 |
| Sepsis as a subgroup | 7 | 14.1 | 6.6–27.6 | 97.6 |
| Risk of Bias (p for subgroup differences = 0.649) | ||||
| Low Risk | 13 | 14.6 | 8.3–24.5 | 99.4 |
| High Risk | 9 | 12.1 | 6.4–21.6 | 96.5 |
| Variable | Coefficient | Standard Error | Lower 95%CI | Upper 95%CI | p | R2 |
|---|---|---|---|---|---|---|
| Univariate Analysis | ||||||
| Study Type | 0.211 | 0.139 | ||||
| Administrative (ref.) | - | - | - | - | ||
| Retrospective | 0.706 | 0.785 | −0.938 | 2.349 | ||
| Observational | 1.432 | 0.853 | −0.353 | 3.217 | ||
| Geographical Location | <0.001 | 0.576 | ||||
| North America (ref.) | - | - | - | - | ||
| Europe/Middle East | 1.804 | 0.354 | 1.064 | 2.545 | ||
| Asia | 1.282 | 0.586 | 0.055 | 2.509 | ||
| Sample Size | 0.001 | 0.489 | ||||
| More than 1000 (ref.) | - | - | - | - | ||
| 100–1000 | 0.914 | 0.408 | 0.060 | 1.768 | ||
| Less than 100 | 1.962 | 0.447 | 1.027 | 2.897 | ||
| Composition of the cohort | 0.890 | 0.000 | ||||
| Only sepsis patients (ref.) | - | - | - | - | ||
| Sepsis as a subgroup | 0.073 | 0.521 | −1.013 | 1.159 | ||
| Risk of Bias | 0.661 | 0.001 | ||||
| High Risk (ref.) | - | - | - | - | ||
| Low Risk | 0.219 | 0.491 | −0.807 | 1.243 | ||
| Multivariable Analysis | <0.001 | 0.698 | ||||
| Sample Size | ||||||
| More than 1000 (ref.) | - | - | - | - | - | |
| 100–1000 | 0.646 | 0.334 | −0.058 | 1.350 | 0.070 | |
| Less than 100 | 1.136 | 0.424 | 0.242 | 2.030 | 0.016 | |
| Geographical Location | ||||||
| North America (ref.) | - | - | - | - | - | |
| Europe/Middle East | 1.304 | 0.358 | 0.549 | 2.059 | 0.002 | |
| Asia | 0.788 | 0.539 | −0.350 | 1.926 | 0.162 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corica, B.; Romiti, G.F.; Basili, S.; Proietti, M. Prevalence of New-Onset Atrial Fibrillation and Associated Outcomes in Patients with Sepsis: A Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 547. https://doi.org/10.3390/jpm12040547
Corica B, Romiti GF, Basili S, Proietti M. Prevalence of New-Onset Atrial Fibrillation and Associated Outcomes in Patients with Sepsis: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(4):547. https://doi.org/10.3390/jpm12040547
Chicago/Turabian StyleCorica, Bernadette, Giulio Francesco Romiti, Stefania Basili, and Marco Proietti. 2022. "Prevalence of New-Onset Atrial Fibrillation and Associated Outcomes in Patients with Sepsis: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 4: 547. https://doi.org/10.3390/jpm12040547
APA StyleCorica, B., Romiti, G. F., Basili, S., & Proietti, M. (2022). Prevalence of New-Onset Atrial Fibrillation and Associated Outcomes in Patients with Sepsis: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine, 12(4), 547. https://doi.org/10.3390/jpm12040547