
Postoperative Analgesic Effectiveness of Peripheral Nerve Blocks in Cesarean Delivery: A Systematic Review and Network Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy and Study Selection
2.3. Data Extraction and Management
2.4. Quality Assessment
2.5. Quality of the Evidence
2.6. Statistical Analysis
3. Results
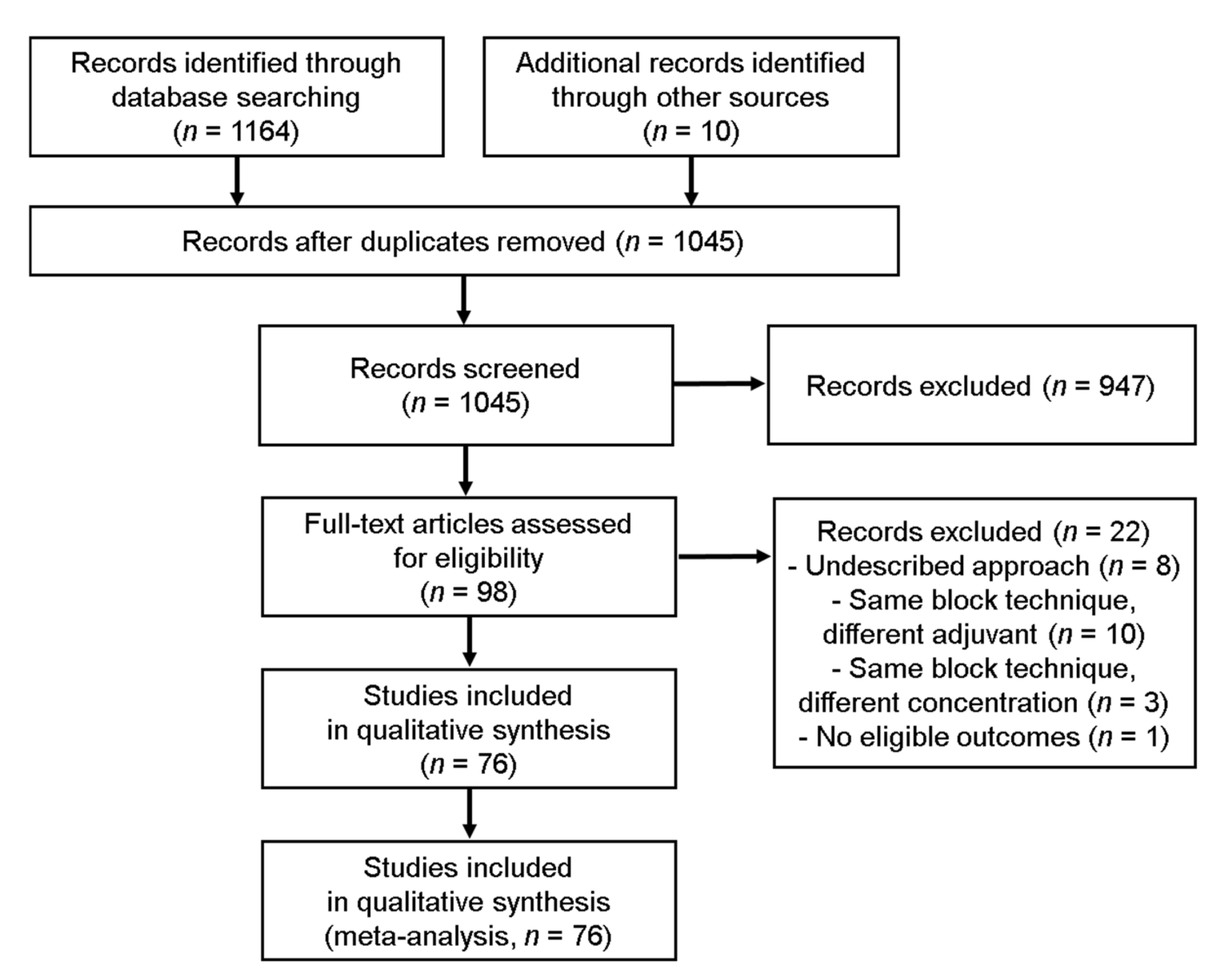
3.1. Study Selection
3.2. Study Characteristics
3.3. Study Quality Assessment
3.4. Synthesis of Results
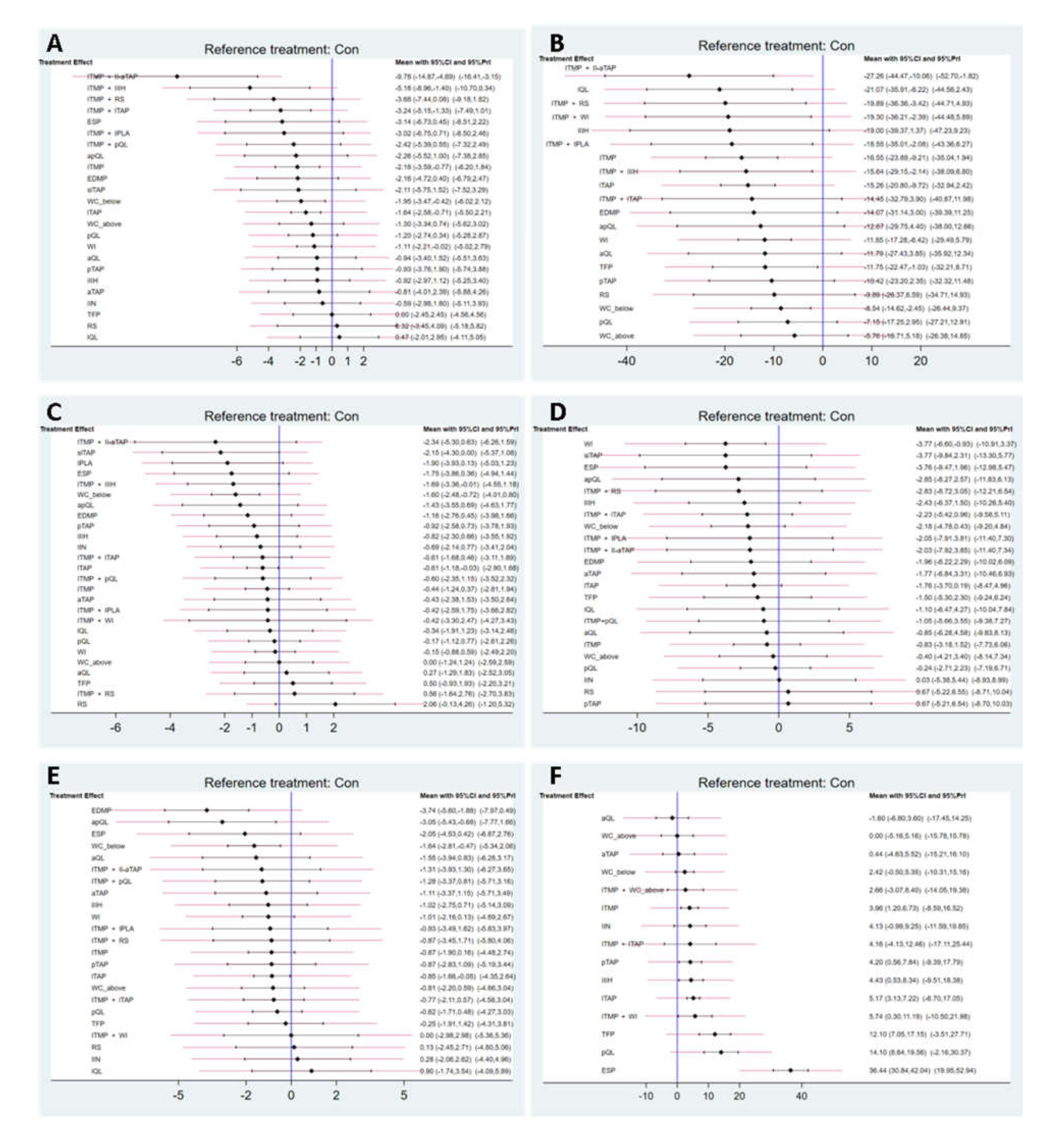
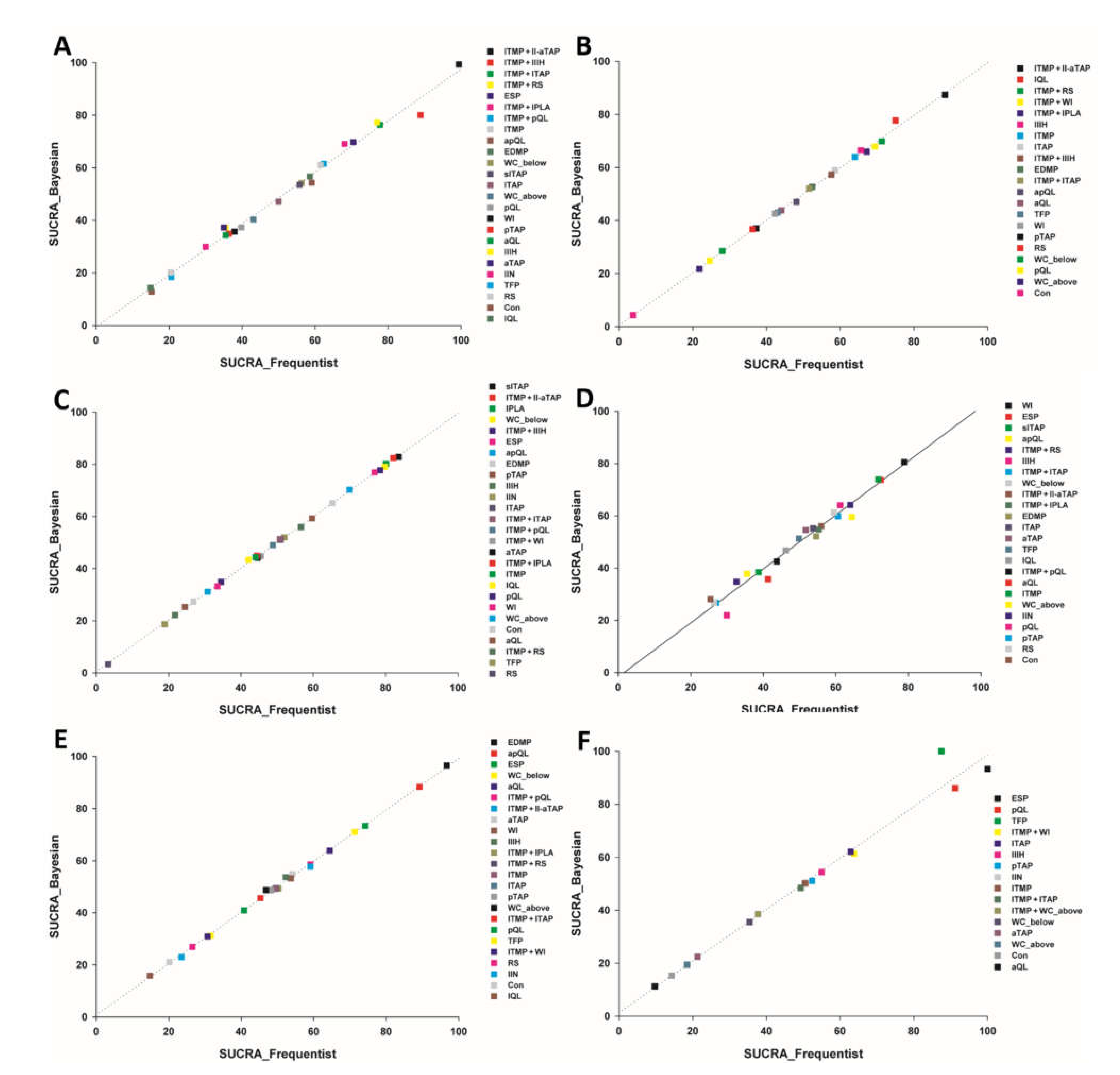
3.4.1. Primary Outcomes
Pain at Rest 6 h after Surgery
Postoperative Cumulative 24 h Morphine Equivalent Consumption (mg)
3.4.2. Secondary Outcomes
Pain at Rest 24 h after Surgery
Dynamic Pain 6 h after Surgery
Dynamic Pain 24 h after Surgery
Time to First Analgesic Request (h)
3.5. Quality of the Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nikolajsen, L.; Sørensen, H.C.; Jensen, T.S.; Kehlet, H. Chronic pain following Caesarean section. Acta Anaesthesiol. Scand. 2004, 48, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Jensen, T.S.; Woolf, C.J. Persistent postsurgical pain: Risk factors and prevention. Lancet 2006, 367, 1618–1625. [Google Scholar] [CrossRef]
- Gadsden, J.; Hart, S.; Santos, A.C. Post-cesarean delivery analgesia. Anesth. Analg. 2005, 101 (Suppl. S5), S62–S69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahl, J.B.; Jeppesen, I.S.; Jørgensen, H.; Wetterslev, J.; Møiniche, S. Intraoperative and postoperative analgesic efficacy and adverse effects of intrathecal opioids in patients undergoing cesarean section with spinal anesthesia: A qualitative and quantitative systematic review of randomized controlled trials. Anesthesiology 1999, 91, 1919–1927. [Google Scholar] [CrossRef] [Green Version]
- Arroyo-Fernández, F.J.; Calderón Seoane, J.E.; Torres Morera, L.M. Strategies of analgesic treatment after cesarean delivery. Current state and new alternatives. Rev. Esp. Anestesiol. Reanim. 2020, 67, 167–175. [Google Scholar] [CrossRef]
- Mitchell, K.D.; Smith, C.T.; Mechling, C.; Wessel, C.B.; Orebaugh, S.; Lim, G. A review of peripheral nerve blocks for cesarean delivery analgesia. Reg. Anesth. Pain Med. 2020, 45, 52–62. [Google Scholar] [CrossRef]
- Mishriky, B.M.; George, R.B.; Habib, A.S. Transversus abdominis plane block for analgesia after Cesarean delivery: A systematic review and meta-analysis. Can. J. Anaesth. 2012, 59, 766–778. [Google Scholar] [CrossRef] [Green Version]
- Sultan, P.; Patel, S.D.; Jadin, S.; Carvalho, B.; Halpern, S.H. Transversus abdominis plane block compared with wound infiltration for postoperative analgesia following Cesarean delivery: A systematic review and network meta-analysis. Can. J. Anaesth. 2020, 67, 1710–1727. [Google Scholar] [CrossRef]
- Xu, M.; Tang, Y.; Wang, J.; Yang, J. Quadratus lumborum block for postoperative analgesia after cesarean delivery: A systematic review and meta-analysis. Int. J. Obstet. Anesth. 2020, 42, 87–98. [Google Scholar] [CrossRef]
- Hussain, N.; Brull, R.; Weaver, T.; Zhou, M.; Essandoh, M.; Abdallah, F.W. Postoperative Analgesic Effectiveness of Quadratus Lumborum Block for Cesarean Delivery under Spinal Anesthesia. Anesthesiology 2021, 134, 72–87. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Chichester, UK, 2008. [Google Scholar]
- Cornell, J.E. The PRISMA extension for network meta-analysis: Bringing clarity and guidance to the reporting of systematic reviews incorporating network meta-analyses. Ann. Intern. Med. 2015, 162, 797–798. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaimani, A.; Higgins, J.P.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical tools for network meta-analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef] [PubMed]
- Van Valkenhoef, G.; Lu, G.; de Brock, B.; Hillege, H.; Ades, A.E.; Welton, N.J. Automating network meta-analysis. Res. Synth. Methods 2012, 3, 285–299. [Google Scholar] [CrossRef]
- Aydin, M.E.; Bedir, Z.; Yayik, A.M.; Celik, E.C.; Ates, I.; Ahiskalioglu, E.O.; Ahiskalioglu, A. Subarachnoid block and ultrasound-guided transversalis fascia plane block for caesarean section: A randomised, double-blind, placebo-controlled trial. Eur. J. Anaesthesiol. 2020, 37, 765–772. [Google Scholar] [CrossRef]
- Aydogmus, M.; Sinikoglu, S.; Naki, M.; Ocak, N.; Sanlı, N.; Alagol, A. Comparison of analgesic efficiency between wound site infiltration and ultra-sound-guided transversus abdominis plane block after cesarean delivery under spinal anaesthesia. Hippokratia 2014, 18, 28–31. [Google Scholar]
- Baaj, J.M.; Alsatli, R.A.; Majaj, H.A.; Babay, Z.A.; Thallaj, A.K. Efficacy of ultrasound-guided transversus abdominis plane (TAP) block for postcesarean section delivery analgesia—A double-blind, placebo-controlled, randomized study. Middle East J. Anaesthesiol. 2010, 20, 821–826. [Google Scholar]
- Bamigboye, A.A.; Justus, H.G. Ropivacaine abdominal wound infiltration and peritoneal spraying at cesarean delivery for preemptive analgesia. Int. J. Gynaecol. Obstet. 2008, 102, 160–164. [Google Scholar] [CrossRef]
- Barney, E.Z.; Pedro, C.D.; Gamez, B.H.; Fuller, M.E.; Dominguez, J.E.; Habib, A.S. Ropivacaine and Ketorolac Wound Infusion for Post-Cesarean Delivery Analgesia: A Randomized Controlled Trial. Obstet. Gynecol. 2020, 135, 427–435. [Google Scholar] [CrossRef]
- Belavy, D.; Cowlishaw, P.J.; Howes, M.; Phillips, F. Ultrasound-guided transversus abdominis plane block for analgesia after Caesarean delivery. Br. J. Anaesth. 2009, 103, 726–730. [Google Scholar] [CrossRef] [Green Version]
- Bell, E.A.; Jones, B.P.; Olufolabi, A.J.; Dexter, F.; Phillips-Bute, B.; Greengrass, R.A.; Penning, D.H.; Reynolds, J.D. Iliohypogastric-ilioinguinal peripheral nerve block for post-Cesarean delivery analgesia decreases morphine use but not opioid-related side effects. Can. J. Anaesth. 2002, 49, 694–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bensghir, M.; Elwali, A.; Miller, C.; Azendour, H.; Drissi, M.; Bakkali, H.; Belyamani, L.; Atmani, M.; Drissi Kamili, N. Effects of skin infiltration with ropivacaine 0.75% on postoperative pain after caesarean section. Gynecol. Obstet. Fertil. 2008, 36, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Bessmertnyj, A.E.; Antipin, E.E.; Uvarov, D.N.; Sedyh, S.V.; Nedashkovsky, E.V. Comparison of the Effectiveness of Ilioinguinal-Iliohypogastric Blockade and Transversus Abdominis Plane Block for Analgesia after Cesarean Section. Anesteziol. Reanimatol. 2015, 60, 51–54. [Google Scholar]
- Bollag, R.; Ansari, T.; Girgis, E. Quadratus lumborum block for postoperative pain after caesarean section: A randomised controlled trial. Eur. J. Anaesthesiol. 2015, 32, 812–818. [Google Scholar]
- Blanco, R.; Ansari, T.; Riad, W.; Shetty, N. Quadratus Lumborum Block Versus Transversus Abdominis Plane Block for Postoperative Pain After Cesarean Delivery: A Randomized Controlled Trial. Reg. Anesth. Pain Med. 2016, 41, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Bollag, L.; Richebe, P.; Siaulys, M.; Ortner, C.M.; Gofeld, M.; Landau, R. Effect of transversus abdominis plane block with and without clonidine on post-cesarean delivery wound hyperalgesia and pain. Reg. Anesth. Pain Med. 2012, 37, 508–514. [Google Scholar] [CrossRef]
- Canakci, E.; Gultekin, A.; Cebeci, Z.; Hanedan, B.; Kilinc, A. The Analgesic Efficacy of Transverse Abdominis Plane Block versus Epidural Block after Caesarean Delivery: Which One Is Effective? TAP Block? Epidural Block? Pain Res. Manag. 2018, 2018, 3562701. [Google Scholar] [CrossRef] [Green Version]
- Canovas, L.; Lopez, C.; Castro, M.; Rodriguez, A.B.; Perez, L. Contribution to post-caesarean analgesia of ultrasound-guided transversus abdominis plane block. Rev. Esp. Anestesiol. Reanim. 2013, 60, 124–128. [Google Scholar] [CrossRef]
- Chandon, M.; Bonnet, A.; Burg, Y.; Barnichon, C.; DesMesnards-Smaja, V.; Sitbon, B.; Foiret, C.; Dreyfus, J.F.; Rahmani, J.; Laloe, P.A.; et al. Ultrasound-guided Transversus Abdominis plane block versus continuous wound infusion for post-caesarean analgesia: A randomized trial. PLoS ONE 2014, 9, e103971. [Google Scholar]
- Corsini, T.; Cuvillon, P.; Forgeot, A.; Chapelle, C.; Seffert, P.; Chauleur, C. Single-dose intraincisional levobupivacaine infiltration in caesarean postoperative analgesia: A placebo-controlled double-blind randomized trial. Ann. Fr. Anesth. Reanim. 2013, 32, 25–30. [Google Scholar] [CrossRef]
- Costello, J.F.; Moore, A.R.; Wieczorek, P.M.; Macarthur, A.J.; Balki, M.; Carvalho, J.C. The transversus abdominis plane block, when used as part of a multimodal regimen inclusive of intrathecal morphine, does not improve analgesia after cesarean delivery. Reg. Anesth. Pain Med. 2009, 34, 586–589. [Google Scholar] [CrossRef] [PubMed]
- Demiraran, Y.; Albayrak, M.; Yorulmaz, I.S.; Ozdemir, I. Tramadol and levobupivacaine wound infiltration at cesarean delivery for postoperative analgesia. J. Anesth. 2013, 27, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Dereu, D.; Savoldelli, G.L.; Mercier, Y.; Combescure, C.; Mathivon, S.; Rehberg, B. The impact of a transversus abdominis plane block including clonidine vs. intrathecal morphine on nausea and vomiting after caesarean section: A randomised controlled trial. Eur. J. Anaesthesiol. 2019, 36, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Ducarme, G.; Sillou, S.; Wernet, A.; Davitian, C.; Poujade, O.; Ceccaldi, P.F.; Bougeois, B.; Luton, D. Single-shot ropivacaine wound infiltration during cesarean section for postoperative pain relief. Gynecol. Obstet. Fertil. 2012, 40, 10–13. [Google Scholar] [CrossRef]
- Eldaba, A.A.; Amr, Y.M.; Sobhy, R.A. Effect of wound infiltration with bupivacaine or lower dose bupivacaine/magnesium versus placebo for postoperative analgesia after cesarean section. Anesth. Essays Res. 2013, 7, 336–340. [Google Scholar]
- Eslamian, L.; Jalili, Z.; Jamal, A.; Marsoosi, V.; Movafegh, A. Transversus abdominis plane block reduces postoperative pain intensity and analgesic consumption in elective cesarean delivery under general anesthesia. J. Anesth. 2012, 26, 334–338. [Google Scholar] [CrossRef]
- Fakor, F.; Farzi, F.; Abdollahzadeh, M.; Golrizan, F.; Kazemnejad, E. The Effect of Transversus Abdominis Plane (TAP) Block with Bupivacaine 25% on Post Cesarean Pain. J. Guilan Univ. Med. Sci. 2014, 23, 53–60. [Google Scholar]
- Fusco, P.; Cofini, V.; Petrucci, E.; Scimia, P.; Pozone, T.; Paladini, G.; Carta, G.; Necozione, S.; Borghi, B.; Marinangeli, F. Transversus Abdominis Plane Block in the Management of Acute Postoperative Pain Syndrome after Caesarean Section: A Randomized Controlled Clinical Trial. Pain Physician 2016, 19, 583–591. [Google Scholar]
- Ganta, R.; Samra, S.K.; Maddineni, V.R.; Furness, G. Comparison of the effectiveness of bilateral ilioinguinal nerve block and wound infiltration for postoperative analgesia after caesarean section. Br. J. Anaesth. 1994, 72, 229–230. [Google Scholar] [CrossRef]
- Gao, Y.; Guo, M.; Du, C.; Zhang, H.; Zhang, H. Clinical study of ultrasound-guided transversus abdominis plane block for analgesia after cesarean section. Medicine 2019, 98, e17542. [Google Scholar] [CrossRef]
- Givens, V.A.; Lipscomb, G.H.; Meyer, N.L. A randomized trial of postoperative wound irrigation with local anesthetic for pain after cesarean delivery. Am. J. Obstet. Gynecol. 2002, 186, 1188–1191. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.K.; Dam, M.; Steingrimsdottir, G.E.; Laier, G.H.; Lebech, M.; Poulsen, T.D.; Chan, V.W.S.; Wolmarans, M.; Bendtsen, T.F.; Borglum, J. Ultrasound-guided transmuscular quadratus lumborum block for elective cesarean section significantly reduces postoperative opioid consumption and prolongs time to first opioid request: A double-blind randomized trial. Reg. Anesth. Pain Med. 2019, 44, 896–900. [Google Scholar] [CrossRef] [PubMed]
- Irwin, R.; Stanescu, S.; Buzaianu, C.; Rademan, M.; Roddy, J.; Gormley, C.; Tan, T. Quadratus lumborum block for analgesia after caesarean section: A randomised controlled trial. Anaesthesia 2020, 75, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jadon, A.; Jain, P.; Chakraborty, S.; Motaka, M.; Parida, S.S.; Sinha, N.; Agrawal, A.; Pati, A.K. Role of ultrasound guided transversus abdominis plane block as a component of multimodal analgesic regimen for lower segment caesarean section: A randomized double blind clinical study. BMC Anesthesiol. 2018, 18, 53. [Google Scholar] [CrossRef]
- Jolly, C.; Jathieres, F.; Keita, H.; Jaouen, E.; Guyot, B.; Torre, A. Cesarean analgesia using levobupivacaine continuous wound infiltration: A randomized trial. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 194, 125–130. [Google Scholar] [CrossRef]
- Kagwa, S.; Hoeft, M.A.; Firth, P.G.; Ttendo, S.; Modest, V.E. Ultrasound guided transversus abdominis plane versus sham blocks after caesarean section in an Ugandan village hospital: A prospective, randomised, double-blinded, single-centre study. Lancet 2015, 385, S36. [Google Scholar] [CrossRef]
- Kainu, J.P.; Sarvela, J.; Halonen, P.; Puro, H.; Toivonen, H.J.; Halmesmaki, E.; Korttila, K.T. Continuous wound infusion with ropivacaine fails to provide adequate analgesia after caesarean section. Int. J. Obstet. Anesth. 2012, 21, 119–124. [Google Scholar] [CrossRef]
- Kanazi, G.E.; Aouad, M.T.; Abdallah, F.W.; Khatib, M.I.; Adham, A.M.; Harfoush, D.W.; Siddik-Sayyid, S.M. The analgesic efficacy of subarachnoid morphine in comparison with ultrasound-guided transversus abdominis plane block after cesarean delivery: A randomized controlled trial. Anesth. Analg. 2010, 111, 475–481. [Google Scholar] [CrossRef]
- Kang, W.; Lu, D.; Yang, X.; Zhou, Z.; Chen, X.; Chen, K.; Zhou, X.; Feng, X. Postoperative analgesic effects of various quadratus lumborum block approaches following cesarean section: A randomized controlled trial. J. Pain Res. 2019, 12, 2305–2312. [Google Scholar] [CrossRef] [Green Version]
- Kessous, R.; Wiznitzer, A.; Polachek, H.; Weintraub, A.Y.; Zlotnik, A.; Pariente, G.; Aricha-Tamir, B.; Press, F.; Leizerovich, A.; Sheiner, E. Preoperative analgesia with local lidocaine infiltration for post cesarean delivery pain management. J. Matern. Fetal Neonatal Med. 2012, 25, 1131–1134. [Google Scholar] [CrossRef]
- Kiran, L.V.; Sivashanmugam, T.; Kumar, V.R.H.; Krishnaveni, N.; Parthasarathy, S. Relative Efficacy of Ultrasound-guided Ilioinguinal-iliohypogastric Nerve Block versus Transverse Abdominis Plane Block for Postoperative Analgesia following Lower Segment Cesarean Section: A Prospective, Randomized Observer-blinded Trial. Anesth. Essays Res. 2017, 11, 713–717. [Google Scholar] [PubMed] [Green Version]
- Klasen, F.; Bourgoin, A.; Antonini, F.; Dazeas, E.; Bretelle, F.; Martin, C.; Baumstarck, K.; Leone, M. Postoperative analgesia after caesarean section with transversus abdominis plane block or continuous infiltration wound catheter: A randomized clinical trial. TAP vs. infiltration after caesarean section. Anaesth. Crit. Care Pain Med. 2016, 35, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Krohg, A.; Ullensvang, K.; Rosseland, L.A.; Langesaeter, E.; Sauter, A.R. The Analgesic Effect of Ultrasound-Guided Quadratus Lumborum Block After Cesarean Delivery: A Randomized Clinical Trial. Anesth. Analg. 2018, 126, 559–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwikiriza, A.; Kiwanuka, J.K.; Firth, P.G.; Hoeft, M.A.; Modest, V.E.; Ttendo, S.S. The analgesic effects of intrathecal morphine in comparison with ultrasound-guided transversus abdominis plane block after caesarean section: A randomised controlled trial at a Ugandan regional referral hospital. Anaesthesia 2019, 74, 167–173. [Google Scholar]
- Lalmand, M.; Wilwerth, M.; Fils, J.F.; Van der Linden, P. Continuous Ropivacaine Subfascial Wound Infusion Compared with Intrathecal Morphine for Postcesarean Analgesia: A Prospective, Randomized Controlled, Double-Blind Study. Anesth. Analg. 2017, 125, 907–912. [Google Scholar] [CrossRef]
- Lavand’homme, P.M.; Roelants, F.; Waterloos, H.; De Kock, M.F. Postoperative analgesic effects of continuous wound infiltration with diclofenac after elective cesarean delivery. Anesthesiology 2007, 106, 1220–1225. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.J.; Palte, H.D.; Chehade, J.M.; Arheart, K.L.; Ranasinghe, J.S.; Penning, D.H. Ultrasound-guided bilateral transversus abdominis plane blocks in conjunction with intrathecal morphine for postcesarean analgesia. J. Clin. Anesth. 2013, 25, 475–482. [Google Scholar] [CrossRef]
- Loane, H.; Preston, R.; Douglas, M.J.; Massey, S.; Papsdorf, M.; Tyler, J. A randomized controlled trial comparing intrathecal morphine with transversus abdominis plane block for post-cesarean delivery analgesia. Int. J. Obstet. Anesth. 2012, 21, 112–118. [Google Scholar] [CrossRef]
- Lui, M.W.; Li, T.K.T.; Lui, F.; Ong, C.Y.T. A randomised, controlled trial of rectus sheath bupivacaine and intrathecal bupivacaine, without or with intrathecal morphine, vs. intrathecal bupivacaine and morphine after caesarean section. Anaesthesia 2017, 72, 1225–1229. [Google Scholar] [CrossRef]
- Magnani, E.; Corosu, R.; Mancino, P.; Borgia, M.L. Postoperative analgesia after cesarean section by continued administration of levobupivacaine with the On-Q Painbuster system over the fascia vs ketorolac + morphine i.v. Clin. Exp. Obstet. Gynecol. 2006, 33, 223–225. [Google Scholar]
- Malawat, A.; Verma, K.; Jethava, D.; Jethava, D.D. Erector spinae plane block and transversus abdominis plane block for postoperative analgesia in cesarean section: A prospective randomized comparative study. J. Anaesthesiol. Clin. Pharmacol. 2020, 36, 201–206. [Google Scholar] [PubMed]
- Mankikar, M.G.; Sardesai, S.P.; Ghodki, P.S. Ultrasound-guided transversus abdominis plane block for post-operative analgesia in patients undergoing caesarean section. Indian J. Anaesth. 2016, 60, 253–257. [Google Scholar] [CrossRef] [PubMed]
- McKeen, D.M.; George, R.B.; Boyd, J.C.; Allen, V.M.; Pink, A. Transversus abdominis plane block does not improve early or late pain outcomes after Cesarean delivery: A randomized controlled trial. Can. J. Anaesth. 2014, 61, 631–640. [Google Scholar] [CrossRef] [PubMed]
- McMorrow, R.C.; Ni Mhuircheartaigh, R.J.; Ahmed, K.A.; Aslani, A.; Ng, S.C.; Conrick-Martin, I.; Dowling, J.J.; Gaffney, A.; Loughrey, J.P.; McCaul, C.L. Comparison of transversus abdominis plane block vs spinal morphine for pain relief after Caesarean section. Br. J. Anaesth. 2011, 106, 706–712. [Google Scholar] [CrossRef] [Green Version]
- Mecklem, D.W.; Humphrey, M.D.; Hicks, R.W. Efficacy of bupivacaine delivered by wound catheter for post-Caesarean section analgesia. Aust. N. Z. J. Obstet. Gynaecol. 1995, 35, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Mieszkowski, M.M.; Mayzner-Zawadzka, E.; Tuyakov, B.; Mieszkowska, M.; Zukowski, M.; Wasniewski, T.; Onichimowski, D. Evaluation of the effectiveness of the Quadratus Lumborum Block type I using ropivacaine in postoperative analgesia after a cesarean section—A controlled clinical study. Ginekol. Pol. 2018, 89, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Naghshineh, E.; Shiari, S.; Jabalameli, M. Preventive effect of ilioinguinal nerve block on postoperative pain after cesarean section. Adv. Biomed. Res. 2015, 4, 229. [Google Scholar]
- Niklasson, B.; Borjesson, A.; Carmnes, U.B.; Segerdahl, M.; Ohman, S.G.; Blanck, A. Intraoperative injection of bupivacaine-adrenaline close to the fascia reduces morphine requirements after cesarean section: A randomized controlled trial. Acta Obstet. Gynecol. Scand. 2012, 91, 1433–1439. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, P.; Duarte, F.; Ribeiro, I.; Centeno, M.J.; Moreira, J. Ropivacaine continuous wound infusion versus epidural morphine for postoperative analgesia after cesarean delivery: A randomized controlled trial. Anesth. Analg. 2012, 114, 179–185. [Google Scholar] [CrossRef]
- Patel, R.; Carvalho, J.C.; Downey, K.; Kanczuk, M.; Bernstein, P.; Siddiqui, N. Intraperitoneal Instillation of Lidocaine Improves Postoperative Analgesia at Cesarean Delivery: A Randomized, Double-Blind, Placebo-Controlled Trial. Anesth. Analg. 2017, 124, 554–559. [Google Scholar] [CrossRef]
- Rackelboom, T.; Strat, S.L.; Silvera, S.; Schmitz, T.; Bassot, A.; Goffinet, F.; Ozier, Y.; Beaussier, M.; Mignon, A. Improving continuous wound infusion effectiveness for postoperative analgesia after cesarean delivery: A randomized controlled trial. Obstet. Gynecol. 2010, 116, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Reinikainen, M.; Syvaoja, S.; Hara, K. Continuous wound infiltration with ropivacaine for analgesia after caesarean section: A randomised, placebo-controlled trial. Acta Anaesthesiol. Scand. 2014, 58, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Salama, E.R. Ultrasound-guided bilateral quadratus lumborum block vs. intrathecal morphine for postoperative analgesia after cesarean section: A randomized controlled trial. Korean J. Anesthesiol. 2020, 73, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Sekhavat, L.; Behdad, S. Preoperative analgesia with local lidocaine for cesarean delivery pain relief. J. Matern. Fetal Neonatal Med. 2011, 24, 891–893. [Google Scholar] [CrossRef]
- Serifsoy, T.E.; Tulgar, S.; Selvi, O.; Senturk, O.; Ilter, E.; Peker, B.H.; Ozer, Z. Evaluation of ultrasound-guided transversalis fascia plane block for postoperative analgesia in cesarean section: A prospective, randomized, controlled clinical trial. J. Clin. Anesth. 2020, 59, 56–60. [Google Scholar] [CrossRef]
- Shahin, A.Y.; Osman, A.M. Intraperitoneal lidocaine instillation and postcesarean pain after parietal peritoneal closure: A randomized double-blind placebo-controlled trial. Clin. J. Pain 2010, 26, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Dhir, S.; Marmai, K.; Rehou, S.; Silva, M.; Bradbury, C. Efficacy of ultrasound-guided transversus abdominis plane blocks for post-cesarean delivery analgesia: A double-blind, dose-comparison, placebo-controlled randomized trial. Int. J. Obstet. Anesth. 2013, 22, 188–193. [Google Scholar] [CrossRef]
- Srivastava, U.; Verma, S.; Singh, T.K.; Gupta, A.; Saxsena, A.; Jagar, K.D.; Gupta, M. Efficacy of trans abdominis plane block for post cesarean delivery analgesia: A double-blind, randomized trial. Saudi J. Anaesth. 2015, 9, 298–302. [Google Scholar]
- Staker, J.J.; Liu, D.; Church, R.; Carlson, D.J.; Panahkhahi, M.; Lim, A.; LeCong, T. A triple-blind, placebo-controlled randomised trial of the ilioinguinal-transversus abdominis plane (I-TAP) nerve block for elective caesarean section. Anaesthesia 2018, 73, 594–602. [Google Scholar] [CrossRef]
- Svirskiǐ, D.A.; Antipin, E.E.; Uvarov, D.N.; Nedashkovskiǐ, E.V. Abdominal cross section space blockade as a component of the multimodal postoperative analgesia in patients after cesarean section: Blockade efficiency analysis. Anesteziol. Reanimatol. 2012, 6, 33–35. [Google Scholar]
- Pavy, T.; Gambling, D.; Kliffer, P.; Munro, A.; Merrick, P.M.; Douglas, J. Effect of preoperative skin infiltration with 0.5% bupivacaine on postoperative pain following cesarean section under spinal anesthesia. Int. J. Obstet. Anesth. 1994, 3, 199–202. [Google Scholar] [CrossRef]
- Tamura, T.; Yokota, S.; Ando, M.; Kubo, Y.; Nishiwaki, K. A triple-blinded randomized trial comparing spinal morphine with posterior quadratus lumborum block after cesarean section. Int. J. Obstet. Anesth. 2019, 40, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.T.; Teoh, W.H.; Woo, D.C.; Ocampo, C.E.; Shah, M.K.; Sia, A.T. A randomised trial of the analgesic efficacy of ultrasound-guided transversus abdominis plane block after caesarean delivery under general anaesthesia. Eur. J. Anaesthesiol. 2012, 29, 88–94. [Google Scholar] [CrossRef]
- Tawfik, M.M.; Mohamed, Y.M.; Elbadrawi, R.E.; Abdelkhalek, M.; Mogahed, M.M.; Ezz, H.M. Transversus Abdominis Plane Block Versus Wound Infiltration for Analgesia After Cesarean Delivery: A Randomized Controlled Trial. Anesth. Analg. 2017, 124, 1291–1297. [Google Scholar] [CrossRef]
- Telnes, A.; Skogvoll, E.; Lonnee, H. Transversus abdominis plane block vs. wound infiltration in Caesarean section: A randomised controlled trial. Acta Anaesthesiol. Scand. 2015, 59, 496–504. [Google Scholar] [CrossRef]
- Triyasunant, N.; Chinachoti, T.; Duangburong, S. Direct Field Block with 40 ML of 0.125% Bupivacaine in Conjunction with Intrathecal Morphine for Analgesia after Cesarean Section: A Randomized Controlled Trial. J. Med. Assoc. Thai. 2015, 98, 1001–1009. [Google Scholar] [PubMed]
- Trotter, T.N.; Hayes-Gregson, P.; Robinson, S.; Cole, L.; Coley, S.; Fell, D. Wound infiltration of local anaesthetic after lower segment caesarean section. Anaesthesia 1991, 46, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, M.C.; Steen, T.L.; Cobb, B.T.; Phelps, A.L.; Pomerantz, J.M.; Orebaugh, S.L.; Chelly, J.E. Efficacy of the bilateral ilioinguinal-iliohypogastric block with intrathecal morphine for postoperative cesarean delivery analgesia. Sci. World J. 2012, 2012, 107316. [Google Scholar] [CrossRef]
- Wagner-Kovacec, J.; Povalej-Brzan, P.; Mekis, D. Efficacy of continuous in-wound infusion of levobupivacaine and ketorolac for post-caesarean section analgesia: A prospective, randomised, double-blind, placebo-controlled trial. BMC Anesthesiol. 2018, 18, 165. [Google Scholar] [CrossRef] [Green Version]
- Wolfson, A.; Lee, A.J.; Wong, R.P.; Arheart, K.L.; Penning, D.H. Bilateral multi-injection iliohypogastric-ilioinguinal nerve block in conjunction with neuraxial morphine is superior to neuraxial morphine alone for postcesarean analgesia. J. Clin. Anesth. 2012, 24, 298–303. [Google Scholar] [CrossRef]
- Sutton, C.D.; Carvalho, B. Optimal Pain Management After Cesarean Delivery. Anesthesiol. Clin. 2017, 35, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Sultan, P.; Halpern, S.H.; Pushpanathan, E.; Patel, S.; Carvalho, B. The Effect of Intrathecal Morphine Dose on Outcomes After Elective Cesarean Delivery: A Meta-Analysis. Anesth. Analg. 2016, 123, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Forero, M.; Adhikary, S.D.; Lopez, H.; Tsui, C.; Chin, K.J. The Erector Spinae Plane Block: A Novel Analgesic Technique in Thoracic Neuropathic Pain. Reg. Anesth. Pain Med. 2016, 41, 621–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdallah, F.W.; Laffey, J.G.; Halpern, S.H.; Brull, R. Duration of analgesic effectiveness after the posterior and lateral transversus abdominis plane block techniques for transverse lower abdominal incisions: A meta-analysis. Br. J. Anaesth. 2013, 111, 721–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarraya, A.; Zghal, J.; Abidi, S.; Smaoui, M.; Kolsi, K. Subarachnoid morphine versus TAP blocks for enhanced recovery after caesarean section delivery: A randomized controlled trial. Anaesth. Crit. Care Pain Med. 2016, 35, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Kupiec, A.; Zwierzchowski, J.; Kowal-Janicka, J.; Goździk, W.; Fuchs, T.; Pomorski, M.; Zimmer, M.; Kübler, A. The analgesic efficiency of transversus abdominis plane (TAP) block after caesarean delivery. Ginekol. Polska 2018, 89, 421–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sriramka, B.; Sahoo, N.; Panigrahi, S. Analgesic Efficacy of Ultrasound-guided Transversus Abdominis Plane Block following Caesarean Section. Int. J. Perioper. Ultrasound Appl. Technol. 2012, 1, 5–8. [Google Scholar] [CrossRef]
- Tuncer, S.; Aysolmaz, G.; Reisli, R.; Erol, A.; Yalçin, N.; Yosunkaya, A. The effects of the administration of subfacial levobupivacaine infusion with the ON-Q pain pump system on postoperative analgesia and tramadol consumption in cesarean operations. Agri 2010, 22, 73–78. [Google Scholar]
- Qian, H.; Zhang, Q.; Zhu, P.; Zhang, X.; Tian, L.; Feng, J.; Wu, Y.; Zhao, Z.; Luan, H. Ultrasound-guided transversus abdominis plane block using ropivacaine and dexmedetomidine in patients undergoing caesarian sections to relieve post-operative analgesia: A randomized controlled clinical trial. Exp. Ther. Med. 2020, 20, 1163–1168. [Google Scholar] [CrossRef]
- Buluc, H.; Ar, A.Y.; Turan, G.; Karadogan, F.; Sargin, M.A.; Akgun, N. The efficacy of transversus abdominis plane block for post-operative analgesia after the cesarean section performed under general anesthesia. North. Clin. Istanb. 2019, 6, 368–373. [Google Scholar] [CrossRef]
- Akkaya, A.; Yildiz, I.; Tekelioglu, U.Y.; Demirhan, A.; Bayir, H.; Ozlu, T.; Bilgi, M.; Kocoglu, H. Dexamethasone added to levobupivacaine in ultrasound-guided tranversus abdominis plain block increased the duration of postoperative analgesia after caesarean section: A randomized, double blind, controlled trial. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 717–722. [Google Scholar] [PubMed]
- Behdad, S.; Sekhavat, L.; Ayatollahi, V.; Meshkat, F.; Mortazavi, A. Comparison of postoperative analgesic effect of tramadol and bupivacaine subcutaneous infiltration in patients undergoing cesarean section. Acta Clin. Croat. 2013, 52. [Google Scholar]
- Eslamian, L.; Kabiri-Nasab, M.; Agha-Husseini, M.; Azimaraghi, O.; Barzin, G.; Movafegh, A. Adding Sufentanil to TAP Block Hyperbaric Bupivacaine Decreases Post-Cesarean Delivery Morphine Consumption. Acta Med. Iran. 2016, 54, 185–190. [Google Scholar] [PubMed]
- Gupta, A.; Gupta, A.; Yadav, N. Effect of dexamethasone as an adjuvant to ropivacaine on duration and quality of analgesia in ultrasound-guided transversus abdominis plane block in patients undergoing lower segment cesarean section—A prospective, randomised, single-blinded study. Indian J. Anaesth. 2019, 63, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Haliloglu, M.; Bilgen, S.; Menda, F.; Ozcan, P.; Ozbay, L.; Tatar, S.; Unal, D.O.; Koner, O. Analgesic efficacy of wound infiltration with tramadol after cesarean delivery under general anesthesia: Randomized trial. J. Obstet. Gynaecol. Res. 2016, 42, 816–821. [Google Scholar] [CrossRef]
- Ranjan, R.; John, R.; Ramachandran, T.; George, S.K. Analgesic efficacy of transverse abdominal plane block after elective cesarean delivery—Bupivacaine with fentanyl versus bupivacaine alone: A randomized, double-blind controlled clinical trial. Anesth. Essays Res. 2017, 11, 181–184. [Google Scholar] [CrossRef] [Green Version]
- Zachariah, S.K.; Joseph, B.; Abraham, S.P. The comparison of effects of fentanyl and dexmedetomidine as adjuvants to ropivacaine for ultrasound-guided transversus abdominis plane block for postoperative pain in cesarean section under spinal anesthesia –A randomized controlled trial. J. Anaesthesiol. Clin. Pharmacol. 2020, 36, 377–380. [Google Scholar] [CrossRef]
- Tharwat, A.A.; Yehia, A.H.; Wahba, K.A.; Ali, A.-E.G. Efficacy and safety of post-cesarean section incisional infiltration with lidocaine and epinephrine versus lidocaine alone in reducing postoperative pain: A randomized controlled double-blinded clinical trial. J. Turk. Gynecol. Assoc. 2016, 17, 1–5. [Google Scholar] [CrossRef]
- Katz, D.; Hamburger, J.; Gutman, D.; Wang, R.; Lin, H.; Marotta, M.; Zahn, J.; Beilin, Y. The Effect of Adding Subarachnoid Epinephrine to Hyperbaric Bupivacaine and Morphine for Repeat Cesarean Delivery: A Double-blind Prospective Randomized Control Trial. Obstet. Anesth. Dig. 2019, 39, 51–52. [Google Scholar] [CrossRef]
- Onishi, Y.; Kato, R.; Okutomi, T.; Tabata, K.-I.; Amano, K.; Unno, N. Transversus abdominis plane block provides postoperative analgesic effects after cesarean section: Additional analgesia to epidural morphine alone. J. Obstet. Gynaecol. Res. 2013, 39, 1397–1405. [Google Scholar] [CrossRef]
- Ekmekçi, P.; Çağlar, G.S.; Yilmaz, H.; Kazbek, B.K.; Gursoy, A.Y.; Kiseli, M.; Tüzüner, F.; Yılmaz, H.; Gursoy, A.Y. Effects of different doses of tramadol added to levobupivacaine in continuous wound infusion for postoperative pain treatment following cesarean section. J. Matern. Neonatal Med. 2016, 30, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.Z.E.A. Assessment of the analgesic potency of ropivacaine 0.2% versus ropivacaine 0.5% in transversus abdominis plane block after cesarean delivery. Egypt. J. Anaesth. 2016, 32, 385–390. [Google Scholar] [CrossRef] [Green Version]
- Aly, M.; Ibrahim, A.; Farrag, W.; Abdelsalam, K.; Mohamed, H.; Tawfik, A. Pruritus after intrathecal morphine for cesarean delivery: Incidence, severity and its relation to serum serotonin level. Int. J. Obstet. Anesthesia 2018, 35, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Kintu, A.; Abdulla, S.; Lubikire, A.; Nabukenya, M.T.; Igaga, E.; Bulamba, F.; Semakula, D.; Olufolabi, A.J. Postoperative pain after cesarean section: Assessment and management in a tertiary hospital in a low-income country. BMC Health Serv. Res. 2019, 19, 68. [Google Scholar] [CrossRef]
- Joshi, G.; Gandhi, K.; Shah, N.; Gadsden, J.; Corman, S.L. Peripheral nerve blocks in the management of postoperative pain: Challenges and opportunities. J. Clin. Anesth. 2016, 35, 524–529. [Google Scholar] [CrossRef] [Green Version]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- White, I.R.; Barrett, J.K.; Jackson, D.; Higgins, J.P.T. Consistency and inconsistency in network meta-analysis: Model estimation using multivariate meta-regression. Res. Synth. Methods 2012, 3, 111–125. [Google Scholar] [CrossRef] [Green Version]
- Salanti, G.; Ades, A.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Riley, R.D.; Higgins, J.; Deeks, J. Interpretation of random effects meta-analyses. BMJ 2011, 342, d549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rackelboom, T.; Le Strat, S.; Silvera, S.; Schmitz, T.; Bassot, A.; Goffinet, F.; Ozier, Y.; Beaussier, M.; Mignon, A. Improving Continuous Wound Infusion Effectiveness for Postoperative Analgesia After Cesarean Delivery. Obstet. Gynecol. 2010, 116, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Milan, Z.; Tabor, D.; McConnell, P.; Pickering, J.; Kocarev, M.; Du Feu, F.; Barton, S. Three different approaches to Transversus abdominis planeblock: A cadaveric study. Med. Glas. 2011, 8, 181–184. [Google Scholar]
- Hansen, C.K.; Dam, M.; Bendtsen, T.F.; Børglum, J. Ultrasound-Guided Quadratus Lumborum Blocks. Astron. Astrophys. 2016, 6, 39. [Google Scholar] [CrossRef] [Green Version]
- Elsharkawy, H.; El-Boghdadly, K.; Barrington, M. Quadratus Lumborum Block. Anesthesiol. 2019, 130, 322–335. [Google Scholar] [CrossRef]
- Patel, S.; El Sharawi, N.; Sultan, P. Local anaesthetic techniques for post-caesarean delivery analgesia. Int. J. Obstet. Anesthesia 2019, 40, 62–77. [Google Scholar] [CrossRef]
- Lee, T.H.W.; Barrington, M.J.; Tran, T.M.N.; Wong, D.; Hebbard, P.D. Comparison of Extent of Sensory Block following Posterior and Subcostal Approaches to Ultrasound-Guided Transversus Abdominis Plane Block. Anaesth. Intensiv. Care 2010, 38, 452–460. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.L.; Dalley, A.F.; Agur, A.M.R. Clinically Oriented Anatomy, 8th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Anesthesia | Groups (n) | Management | Supplemental Postoperative Analgesia | Primary Outcome |
|---|---|---|---|---|---|
| Aydin et al., 2020 [16] | SA | TFP (30) Control (30) | 0.25% bupivacaine 40 mL N/S 40 mL | IV MP PCA (0-1-10); in PACU, fentanyl 50 mcg if pain score > 3;paracetamol 1 g IV q6 h | Postoperative opioid consumption |
| Aydogmus et al., 2014 [17] | SA | WI (35) slTAP (35) | 0.25% levobupivacaine 40 mL 0.25% levobupivacaine 40 mL | If pain score > 3, diclofenac 75 mg IM, then, tramadol 50 mg IV | Pain scores |
| Baaj et al., 2010 [18] | SA | lTAP (20) Control (20) | 0.25% bupivacaine 40 mL N/S 40 mL | IV MP PCA (0-1-10) | MP consumption over 24 h |
| Bamigboye et al., 2008 [19] | GA | WI (50) Control (50) | 0.75% ropivacaine 30 mL N/S 30 mL | Pethidine 100 mg IV q3–4 h; Diclofenac 75 mg IM q12 h; tramadol 37.5 mg and paracetamol 325 mg as needed | Severe pain at 1 h |
| Barney et al., 2020 [20] | CSE | WC_below (33) Control (38) | 0.2% ropivacaine 540 mg and ketorolac 30 mg (5 mL/h) N/S (5 mL/h) | Acetaminophen 975 mg rectal and Ketorolac 15 mg IV in OR; acetaminophen 975 mg q6 h; Ketorolac 15 mg q6 h; Ibuprofen 600 mg q6 h; Oxycodone 5 mg PO for NRS 4–6, 10 mg PO for NRS 7–10. | Pain score with movement at 24 h |
| Belavy et al., 2009 [21] | SA | lTAP (23) Control (24) | 0.5% ropivacaine 40 mL N/S 40 mL | Acetaminophen 1 g rectal; Diclofenac 100 mg after surgery; Acetaminophen 1 g q6 h | MP requirements in 24 h |
| Bell et al., 2002 [22] | SA | IIIH (31) | 0.5% bupivacaine + epinephrine 5 μg/mL 24 mL | IV MP PCA (0–0.02mg/kg−10); Naproxen 500 mg q12 h | 24 h IV PCA MP use |
| Control (28) | N/S 24 mL | ||||
| Bensghir et al., 2008 [23] | SA | WI (20) Control (22) | 0.75% ropivacaine 20 mL N/S 20 mL | Paracetamol 1 g q6 h; Ketoprofen 50 mg q6 h; MP 3 mg IV titration if NRS > 3; Tramadol 100 mg IV (max. 400 mg/dL) | No specific comment |
| Bessmertnyj et al., 2015 [24] | SA | IIIH (54) aTAP (53) Control (57) | 0.5% ropivacaine 20 mL 0.25% ropivacaine 40 mL No block | Ketorolac 30 mg IV q8 h; paracetamol 1 g PO q6 h; Tramadol 100 mg IM as needed only in control group | Pain score at rest |
| Blanco et al., 2015 [25] | SA | pQL (25) Control (23) | 0.125% bupivacaine 0.2 mL/kg N/S 0.2 mL/Kg | IV MP PCA (0-1-5); paracetamol 1 g PO q6 h; Diclofenac 50 mg q8 h | MP demands and doses |
| Blanco et al., 2016 [26] | SA | lQL (38) lTAP (38) | 0.125% bupivacaine 0.4 mL/kg 0.125% bupivacaine 0.4 mL/kg | Diclofenac 100 mg rectal and Paracetamol 1 g IV after surgery; IV MP PCA (0-1-5); Paracetamol 1 g PO q6 h; Diclofenac 50 mg q8 h | PCA MP consumption |
| Bollag et al., 2012 [27] | SA | ITMP + lTAP (25) | SA with MP 100 μg, TAP with 0.375% bupivacaine 40 mL + N/S 1 mL | Ketorolac 30 mg IV during the block; in PACU, MP IV as needed; Acetaminophen 1g q6 h; Diclofenac 75 mg q8 h; Tramadol 50 mg PO q8 h as needed | Wound hyperalgesia 48 h |
| ITMP (30) | MP 100 μg, TAP with N/S 41 mL | ||||
| Canakci et al., 2018 [28] | SAED | EDMP (40) lTAP (40) | MP 3 mg 0.25% bupivacaine 40 mL | Dex-ketoprofen 50 mg IV as needed | No specific comment |
| Canovas et al., 2013 [29] | SA | ITMP (30) lTAP (30) | MP 100 μg, TAP with N/S 40 mL 0.5% levobupivacaine 40 mL | IV MP PCA (0-1-10) | No specific comment |
| Chandon et al., 2014 [30] | SA | lTAP (36) WCI_below (29) | 0.375% levobupivacaine 40% 250 mg levobupivacaine in 200 mL (5 mL/h) | Paracetamol 1 g; Ketoprofen 50 mg; Nefopam 20 mg PO q6 h | Pain over 48 h |
| Corsini et al., 2013 [31] | SA | WI (56) Control (53) | 0.5% levobupivacaine 30 mL N/S 30 mL | Paracetamol 1 g IV after surgery; in PACU, MP 3 mg IV if VAS > 4; IV MP PCA (0-1-10); outside OR, Ketoprofen 100 mg q8 h, if VAS > 4 | MP consumption |
| Costello et al., 2009 [32] | SA | ITMP (49) | MP 100 μg, TAP with N/S 40 mL | Ketorolac 30 mg IV; Acetaminophen 1.3 g rectal in OR; in PACU, Diclofenac 50 mg PO q8 h; Acetaminophen 1 g PO q6 h; MP 2 mg IV as needed; then, MP S.Q.; MP 5 mg PO | VAS pain score on movement at 24 h |
| ITMP + lTAP (47) | MP 100 μg, 0.375% ropivacaine 40 mL | ||||
| Demiraran et al., 2013 [33] | GA | WI (30) Control (30) | 0.25% levobupivacaine 20 mL N/S 20 mL | IV PCA with Tramadol (5 mg/h−20 mg−15 min); Diclofenac 75 mg IV if VAS > 3 | 24 h tramadol consumption |
| Dereu et al., 2019 [34] | SA | ITMP (82) pTAP (84) | MP 100 μg, TAP with N/S 40 mL 0.5% ropivacaine 40 mL + clonidine 75 μg | Paraceamol 1 g IV and Ketorolac 30 mg IV 1 h after surgery; then, Paracetamol 1 g PO q6 h; Ibuprofen 600 mg PO q8 h | PONV at 24 h |
| Ducarme et al., 2012 [35] | SA | WI (56) ITMP (44) | 0.75% ropivacaine 20 mL MP 100 μg, block with N/S 20 mL | Paraceamol 1 g q6 h; Ketoprofen 50 mg q8 h; Nefopam 20 mg IV; if VAS > 3, MP 3 mg IV | Pain on movement and coughing |
| Eldaba et al., 2013 [36] | SA | WC_below (40) Control (40) | 0.5% bupivacaine 5 mL/h N/S 5 mL/h | IV MP PCA (0-2-10); Ketorolac 30 mg IV q8 h; Acetaminophen 500 mg IV q6 h | No specific comment |
| Eslamian et al., 2012 [37] | GA | lTAP (24) Control (24) | 0.25% bupivacaine 30 mL No block | Tramadol 50 mg IV if needed; Diclofenac 100 mg rectal qd | Pain intensity |
| Fakor et al., 2014 [38] | SA | lTAP (35) Control (35) | 0.25% bupivacaine 40 mL N/S 40 mL | Diclofenac 100 mg rectal if needed | No specific comment |
| Fusco et al., 2016 [39] | SA | slTAP (48) Control (48) | 0.375% levobupivacaine 40 mL N/S 40 mL | In PACU, if VAS > 3, Ketorolac 30 mg IV; then Acetaminophen 1 g IV q6 h if VAS 3–5 or Ketorolac 30 mg IV if VAS 5–7 or Tramadol 100 mg if VAS 7–10 | Pain during the first 72 h |
| Ganta et al., 1994 [40] | GA | IIN (21) WI (20) Control (21) | 0.5% bupivacaine 20 mL 0.5% bupivacaine 20 mL No block | No specific comment | No specific comment |
| Gao et al., 2019 [41] | SA | lTAP Control | 0.33% ropivacaine 60 mL No block | In control group, IV PCA with sufentanil | No specific comment |
| Givens et al., 2002 [42] | ED | WI (20) Control (16) | 0.25% bupivacaine 25 mL N/S 25 mL | IV MP PCA (0-1-6) | No specific comment |
| Hansen et al., 2019 [43] | SA | aQL (34) Control (34) | 0.375% ropivacaine 30 mL N/S 30 mL | IV MP PCA (0-5-20); Paracetamol 1 g PO q6 h; Ibuprofen 400 mg q8 h | Opioid consumption |
| Irwin et al., 2020 [44] | SA | pQL (44) Control (42) | 0.25% levobupivacaine 40 mL Sham block | Diclofenac 100 mg and Paracetamol 1 g IV after surgery; IV MP PCA (0-1-5); Paracetamol 1 g PO q6 h; Diclofenac 75 mg PO q12 h | 24 h MP consumption |
| Jadon et al., 2018 [45] | SA | lTAP (67) Control (67) | 0.375% ropivacaine 40 mL N/S 40 mL | Declofenac 75 mg IV before the completion of surgery; Diclofenac 75 mg q12 h; Tramadol 50 mg as needed | Time to first analgesic request |
| Jolly et al.,2 015 [46] | SA | WC_below (34) Control (34) | 0.25% levobupivacaine 20 mL bolus, then 1.25 mg/mL, 5 mL/h No procedure | Nefopam 20 mg IV and Acetaminophen 1 g during the surgery; IV MP PCA (0-1.2-7); in PACU, Celecoxib 400 mg; then, Acetaminophen 1 g PO, Nefopam 20 mg PO q6 h | 24 h MP consumption |
| Kagwa et al., 2015 [47] | SA | pTAP (86) Control (84) | 0.25% bupivacaine 20–25 mL + 1:400,000 epinephrine Sham block | Paracetamol 1 g and Diclofenac 50 mg PO q8 r | Pain at rest and on movement |
| Kainu et al., 2012 [48] | CSE | ITMP (24) WC_below (22) Control (20) | MP 160 μg, N/S 5 mL/h WI 0.375% ropivacaine, 5 mL/h N/S 5 mL/h WI | IV oxycodone PCA (0-2-8); after 24 h, Oxycodone 5 or 10 mg PO | 24 h oxycodone consumption |
| Kanazi et al., 2010 [49] | SA | ITMP (28) pTAP (29) | MP 200 μg, TAP with N/S 40 mL 0.375% bupivacaine + epinephrine 5 μg/mL 40 mL | Diclofenac 100 mg rectal q12 h; Paracetamol 1 g IV q6 h; Tramadol 100 mg IV q8 h as needed | Time to first analgesic request |
| Kang et al., 2019 [50] | SA | pQL (22) aQL (23) apQL (22) EDMP (22) | 0.2% ropivacaine 60 mL 0.2% ropivacaine 60 mL 0.2% ropivacaine 60 mL MP 2 mg in 6 mL | Paracetamol 1 g PO q6 h; IV MP PCA (0-0.5-5) | Pain scores at rest and with movement Total MP consumption |
| Kessous et al., 2012 [51] | GASA | WI (77) Control (76) | 1% lidocaine 20 mL N/S 20 mL | Propoxyphene 40 mg and Paracetamol 500 mg for mild pain; meperidine 75 mg for severe pain | No specific comment |
| Kiran et al., 2017 [52] | SA | lTAP (30) IIIH (30) | 0.25% bupivacaine 40 mL 0.25% bupivacaine 40 mL | Paracetamol 1 g IV | Postoperative analgesic sparing |
| Klasen et al., 2016 [53] | SA | lTAP (25) WC_below (29) | 0.75% ropivacaine 3 mL/kg 0.2% ropivacaine 10 mL bolus +5 mL/h | Paracetamol 4 mg PO per day; Ketoprofen 200 mg per day; Nefopam 40 mg per day; IV MP PCA (0-1-10) | 48 h MP consumption |
| Krohg et al., 2018 [54] | SA | lQL (20) control (20) | 0.2% ropivacaine 0.4 mg/kg N/S 0.4 mL/kg | Paracetamol 1 g PO; Ibuprofen 400 mg PO q6 h; IV ketobemidone PCA (0-1-8) | 24 h ketobemidone consumption |
| Kwikiriza et al., 2019 [55] | SA | ITMP (65) pTAP (65) | MP 100 μg, Sham block 0.25% bupivacaine + epinephrine 1:200,000 30 mL | Paracetamol 1 g; Diclofenac 50 mg | No specific comment |
| Lalmand et al., 2017 [56] | SA | ITMP (61) WC_below (63) Control (58) | MP 100 μg, infusion with N/S 0.2% ropivacaine 15 mg bolus + 10 mL/hr Infusion with N/S | Acetaminophen 1 g q6 h; Diclofenac 75 mg q12 h; IV MP PCa (0-1-7) | Time to first analgesic request |
| Lavand’homme et al., 2007 [57] | SA | WC_above (30) Control (30) | 0.2% ropivacaine 240 mL, 5 mL/h N/S 240 mL, 5 mL/h | IV MP PCA (0-1-5); Diclofenac 75 mg IV q12 h; Acetaminophen 1 g q6 h as needed | 48 h MP consumption |
| Lee et al., 2013 [58] | CSE | ITMP + lTAP (25) | MP 250 μg, block with 0.5% ropivacaine 40 mL | In PACU, MP 2 mg IV as needed up to 6 mg; Acetaminophen 1 g PO q6 h for VRS 1–3; Ketorolac 30 mg IV or Ibuprofen 800 mg PO q6 h for VRS 4–5; MP 2 mg IV q10 min as needed or Acetaminophen 600 mg/codeine 60 mg or Oxycodone 10 mg/Acetaminophen 650 mg for VRS 6–10 | Pain score with movement at 24 h |
| ITMP (24) | MP 250 μg, block with N/S 40 mL | ||||
| Loane et al., 2012 [59] | SA | ITMP (33) lTAP (33) | MP 100 μg, sham block 0.5% ropivacaine 3 mg/kg | Naproxen 500 mg recal and Acetaminophen 975 mg IV after surgery; then, Naproxen 500 mg PO q12 h; Acetaminophein 1 g PO q6 h; Hydromorphone 2–4 mg PO q4 h as needed; if still inadequate, PC MP PCA (0-1.5-7) | 24 h MP equivalent consumption |
| Lui et al., 2017 [60] | SA | RS (46) | 0.25% bupivacaine 40 mL+ epinephrine 5 μg/mL | Paracetamol 1 g; Tramadol 50 mg | Pain on movement |
| ITMP + RS (47) ITMP (38) | MP 100 μg, block with same regimen MP 100 μg, block with N/S 40 mL | ||||
| Magnani et al., 2006 [61] | SA | ITMP + WC_ above (10) | MP 50 μg, infusion with 0.2% levobupivacaine 2 mL/h | No specific comment | No specific comment |
| ITMP (10) | MP 50 μg | ||||
| Malawat et al., 2020 [62] | SA | ESP (30) lTAP (30) | 0.2% ropivacaine 0.2 mL/kg 0.2% ropivacaine 0.2 mL/kg | Diclofenac 75 mg | Time to first analgesic request |
| Mankikar et al., 2016 [63] | SA | pTAP (30) Control (30) | 0.5% ropivacaine 30 mL N/S 30 mL | Paracetamol 1 g IV after surgery | No specific comment |
| McKeen et al., 2014 [64] | SA | ITMP + lTAP (35) | MP 100 μg, block with 0.25% ropivacaine 40 mL | Ketorolac 30 mg IV and Acetaminophen 1 g IV before block; Naproxen 250 mg q8 h; Acetaminophen 1 g q6 h; Oxycodone 2.5–5 mg q6 h as needed | Pain score, Quality of recovery, 24 h opioid consumption |
| ITMP (39) | MP 100 μg, block with N/S 40 mL | ||||
| McMorrow et al., 2011 [65] | SA | ITMP (20) | MP 100 μg, block with N/S | Paracetamol 1 g and Diclofenac 100 mg after surgery; Paracetamol 1 g PO q6 h; Diclofenac 100 mg rectal at 18 h; IV MP PCA (0-1-5) | Pain on movement |
| ITMP + lTAP (20) | MP 100 μg, block with 0.375% bupivacaine 2 mg/kg | ||||
| lTAP (20) Control (20) | 0.375% bupivacaine 2 mg/kg Block with N/S | ||||
| Mecklem et al.,1995 [66] | SA | RS (35) Control (35) | 0.25% bupivacaine 20 mL #8 N/S 20 mL #8 | IV MP PCA (0-1-5) | No specific comment |
| Mieszkowski et al., 2018 [67] | SA | lQL (30) Control (28) | 0.375% ropivacaine 48 mL No block | Paracetamol 1 g IV before block; Paracetamol 1 g IV q6 h; if NRS > 3, MP 5 mg S.C. | 48 h MP consumption |
| Naghshineh et al., 2015 [68] | GA | IIN (40) Control (40) | 0.5% bupivacaine 20 mL No block | Pethidine bolus | No specific comment |
| Niklasson et al., 2012 [69] | SA | WI (130) | 0.25% bupivacaine + epinephrine 5 μg/mL 40 mL | Paracetamol 1 g q6h; MP IV if needed; after 24 h, Codeine 75 mg PO q6 h; Ibuprofen 200 mg q6 h | 12 and 24 h MP consumption |
| Control (130) | N/S 40 mL | ||||
| O’Neill et al., 2012 [70] | SA CSE | WC_below (29) ED MP (29) | 1% ropivacaine 10 mL bolus, 5 mL/h MP 2 mg/mL q12 h #4 | Acetaminophen 1 g IV q6 h; Diclofenac 75 mg IM as needed | Pain score at rest at 24 h |
| Patel et al., 2017 [71] | SA | ITMP + IPLA (99) | MP 100 μg, 2% lidocaine 20 mL + 1:200,000 epinephrine | Ketorolac 30 mg IV and Acetaminophen 1.3 g suppository after surgery; in PACU MP 2 mg IV as needed; then, Diclofenac 50 mg PO q8 h; Acetaminophen 1 g q6 h; MP 2 mg S.C./IV or Hydromorphone 0.4 mg as needed | Pain score on movement at 24 h |
| ITMP (94) | MP 100 μg, N/S 20 mL | ||||
| Rackelboom et al., 2010 [72] | SA | ITMP + WC_ above (25) ITMP + WC_ below (25) | MP 100 μg, Ropivacaine 450 mg + Ketoprofen 200 mg + N/S 240 mL, 5 mL/h in both group | IV MP PCA (0-1.5-7) | 48 h MP consumption |
| Reinikainen et al., 2014 [73] | SA | WC_above (33) Control (34) | 0.75% ropivacaine 100 mL, 2 mL/h N/S 100 mL, 2 mL/h | Paracetamol 1 g q8 h; Ibuprofen 600 mg q8 h PO; Oxycodone 0.2 mg/kg IM (NRS > 3) or 0.05 mg/kg IV (NRS > 7) | 48 h oxycodone consumption |
| Salama et al., 2020 [74] | SA | ITMP (30) pQL (30) control (30) | MP 100 μg, block with N/S 0.375% ropivacaine 48 mL Block with N/S 48 mL | Paracetamol 1 g IV and Diclofenac 100 mg suppository after surgery; IV MP PCA (0-1-5); if NRS > 3, Paracetamol 1 g IV | Pain score at rest and on movement |
| Sekhavat et al., 2011 [75] | GA | WI (52) Control (52) | 2% lidocaine 10 mL N/S 10 mL | Mefenamic acid 500 mg PO q4 h; MP 5 mg IM as needed | No specific comment |
| Serifsoy et al., 2020 [76] | GA | TFP (35) Control (35) | 0.5% bupivacaine 20 mL + 2% lidocaine 10 mL + N/S 20 mL No block | IV Tramadol PCA (0-10-20); in PACU, NRS > 4 Fentanyl 25 µg; then, Paracetamol 1 g IV q8 h; Diclofenac 75 mg IM (NRS > 4) | 24 h tramadol consumption |
| Shahin et al., 2010 [77] | SA | IPLA (176) Control (178) | 2% lidocaine 10 mL N/S 10 mL | Acetaminophen 1 g q6 h; Ibuprofen 10 mg suppository; Ibuprofen 500 mg PO q4–6 h; MP 2 mg IV as needed | Epigastric pain on 1st and 5th day |
| Singh et al., 2013 [78] | SA | ITMP + lTAP (20) | MP 150 μg, block with 0.5% ropivacaine 3 mg/kg in 60 mL | Ketorolac 30 mg IV during surgery; Ketorolac 30 mg IV; Acetaminophen 650 mg PO q6 h; Codeine 30 mg PO or Oxycodone 5–10 mg q4 h as needed | Pain score difference on movement at 24 h |
| ITMP (20) | MP 150 μg, block with N/S 60 mL | ||||
| Srivastava et al., 2015 [79] | SA | lTAP (31) control (31) | 0.25% bupivacaine 40 mL Sham block | Diclofenac 75 mg IV q8 h; IV Tramadol PCA (0-20-10) | Additional analgesics during 48 h |
| Staker et al., 2018 [80] | SA | ITMP + II-aTAP (50) | MP 150 μg, 0.33% ropivacaine 50 mL (200 mg) | Paracetamol 1.5 g suppository and Diclofenac 100 mg after surgery; in PACU, Fentanyl 10 μg (NRS < 7), 20 μg (NRS > 7); IV Fentanyl PCA (0–10 μg−5); Paracetamol 1 g PO q6 h; Diclofenac 50 mg PO q8 h | Difference in fentanyl dose at 24 h |
| ITMP (50) | MP 150 μg, Sham block | ||||
| Svirskiǐ et al., 2012 [81] | SA | lTAP (31) control (31) | 0.375% ropivacaine 40 mL No block | In TAP group: Ketoprofen 100 mg IV q12 h; Paracetamol 1 g IV q8 h In control group: Paracetamol 1 g q6 h; Ketoprofen 100 mg every 8–12 h; Tramadol 100 mg as needed | No specific comment |
| Pavy et al., 1994 [82] | SA | ITMP + WI (20) | MP 250–300 μg, infiltration with 0.5% bupivacaine 20–30 mL | Codeine 30 mg PO; Paracetamol 325 mg q3 h | No specific comment |
| ITMP (20) | MP 250–300 μg, N/S 20–30 mL | ||||
| Tamura et al., 2019 [83] | SA | ITMP + pQL (34) | MP 100 μg, block with 0.75% ropivacaine 0.9 mL/kg | Droperidol 1.25 mg and Fentanyl 90 μg and Acetaminophen 15 mg/kg IV after baby out; Pentazocine 15 mg IV (NRS 3–6), Pentazocine 15 mg and Acetaminophen 15 mg/kg IV (NRS > 6) | Pain score at 6 h |
| ITMP (38) pQL (36) control (38) | MP 100 μg, block with N/S 0.75% ropivacaine 0.9 mL/kg N/S 0.9 mL/kg | ||||
| Tan et al., 2012 [84] | GA | lTAP (20) control (20) | 0.25% levobupviacaine 40 mL No block | IV MP PCA (0-1-5) | 24 h MP consumption |
| Tawfik et al., 2017 [85] | SA | WI (39) lTAP (39) | 0.25% bupivacaine 30 mL 0.25% bupivacaine 40 mL | Ketorolac 30 mg IV q8 h; Paracetamol 1 g PO q8 h; IV Fentanyl PCA (0–20 μg−7) | 24 h fentanyl consumption |
| Telnes et al., 2015 [86] | SA | lTAP (28) | 0.25% bupivacaine 40 mL + epinephrine 5 μg/mL | Paracetamol 1 g PO q6 h; Diclofenac 50 mg PO q8 h; IV MP PCA (0-1-6) | 48 h MP consumption |
| WI (29) | 0.25% bupivacaine 20 mL + epinephrine 5 μg/mL | ||||
| Triyasunant et al., 2015 [87] | SA | ITMP + WI (28) | MP 200 μg, infiltration with 0.125% bupivacaine 40 mL | Parecoxib 40 mg IV (after surgery, 12 h); IV MP PCA (0-1-5) | Pain free period |
| ITMP (28) | MP 200 μg, no block | ||||
| Trotter et al., 1991 [88] | GA | WI (14) Control (14) | 0.5% bupivacaine 20 mL N/S 20 mL | IV MP PCA (0-2-10) | No specific comment |
| Vallejo et al., 2012 [89] | SA | ITMP + IIIH (17) | MP 150–200 μg, 0.5% bupivacaine 20 mL | Ketorolac 30 mg IV q6 h for 24 h; then, Ibuprofen, Oxycodone, Acetaminophen/Oxycodone, Acetaminophen/Hydrocodone PO | Pain score at 48 h |
| ITMP (17) | MP 150–200 μg, block with N/S 20 mL | ||||
| Wagner-Kovacec et al., 2018 [90] | SA | WC_above (15) Control (15) | 0.25% levobupivacaine 270 mL, 5 mL/h N/S 270 mL, 5 mL/h | Paracetamol 1 g IV q6 h; Piritramide 2 mg IV as needed | 24 and 48 h piritramide consumption |
| Wolfson et al., 2012 [91] | SA | ITMP + IIIH (17) | MP 200 μg, block with 0.5% bupivacaine 24 mL | Ketorolac 30 mg IV; Acetaminophen 1 mg/ Oxycodone 10 mg PO q6 h; IV MP PCA (0-2-10) | Pain score at rest at 24 h |
| ITMP (17) | MP 200 μg, N/S 24 mL |
| Outcomes | Number of Studies/Patients | Quality Assessment | Quality | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Downgrade | Upgrade | |||||||||
| Study Limitation | Inconsistency | Indirectness | Imprecision | Publication Bias | Large Effect | Dose-Response | Confounding | |||
| Pain at rest 6 h after surgery | 59/4622 | serious | not serious | not serious | not serious | not serious | no | no | no | ⨁⨁⨁◯ Moderate |
| Postoperative cumulative 24 h morphine equivalent consumption | 44/3360 | serious | not serious | not serious | not serious | not serious | no | no | no | ⨁⨁⨁◯ Moderate |
| Pain at rest 24 h after surgery | 59/4697 | serious | serious | not serious | not serious | not serious | no | no | no | ⨁⨁◯◯ Low |
| Dynamic pain at 6 h after surgery | 37/2837 | serious | serious | not serious | not serious | not serious | no | no | no | ⨁⨁◯◯ Low |
| Dynamic pain at 24 h after surgery | 44/3371 | serious | serious | not serious | not serious | not serious | no | no | no | ⨁⨁◯◯ Low |
| The time to first analgesic request | 24/1812 | serious | not serious | not serious | not serious | not serious | no | no | no | ⨁⨁⨁◯ Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryu, C.; Choi, G.J.; Jung, Y.H.; Baek, C.W.; Cho, C.K.; Kang, H. Postoperative Analgesic Effectiveness of Peripheral Nerve Blocks in Cesarean Delivery: A Systematic Review and Network Meta-Analysis. J. Pers. Med. 2022, 12, 634. https://doi.org/10.3390/jpm12040634
Ryu C, Choi GJ, Jung YH, Baek CW, Cho CK, Kang H. Postoperative Analgesic Effectiveness of Peripheral Nerve Blocks in Cesarean Delivery: A Systematic Review and Network Meta-Analysis. Journal of Personalized Medicine. 2022; 12(4):634. https://doi.org/10.3390/jpm12040634
Chicago/Turabian StyleRyu, Choongun, Geun Joo Choi, Yong Hun Jung, Chong Wha Baek, Choon Kyu Cho, and Hyun Kang. 2022. "Postoperative Analgesic Effectiveness of Peripheral Nerve Blocks in Cesarean Delivery: A Systematic Review and Network Meta-Analysis" Journal of Personalized Medicine 12, no. 4: 634. https://doi.org/10.3390/jpm12040634
APA StyleRyu, C., Choi, G. J., Jung, Y. H., Baek, C. W., Cho, C. K., & Kang, H. (2022). Postoperative Analgesic Effectiveness of Peripheral Nerve Blocks in Cesarean Delivery: A Systematic Review and Network Meta-Analysis. Journal of Personalized Medicine, 12(4), 634. https://doi.org/10.3390/jpm12040634