
Computer-Aided Diagnosis of Gastrointestinal Protruded Lesions Using Wireless Capsule Endoscopy: A Systematic Review and Diagnostic Test Accuracy Meta-Analysis

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Adherence to the Statement of Systematic Review and Diagnostic Test Accuracy Meta-Analysis
2.2. Literature Searching Strategy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database: MEDLINE (through PubMed) |
| #1 “artificial intelligence”[tiab] OR “AI”[tiab] OR “deep learning”[tiab] OR “machine learning”[tiab] OR “computer”[tiab] OR “neural network”[tiab] OR “CNN”[tiab] OR “automatic”[tiab] OR “automated”[tiab]: 536153 #2 “capsule endoscopy”[tiab] OR “capsule endoscopy”[Mesh]: 5136 #3 “protruded”[tiab] OR “polyp”[tiab] OR “tumor”[tiab] OR “tumors”[Mesh] OR “polyps”[Mesh]: 1295552 #4 #1 AND #2 AND #3: 52 #5 #4 AND English[Lang]: 51 |
| Database: Web of Science |
| #1 artificial intelligence OR AI OR deep learning OR machine learning OR computer OR neural network OR CNN OR automatic OR automated: 130090 #2 capsule endoscopy: 3549 #3 protruded OR polyp OR tumor: 840061 #3 #1 AND #2 AND #3: 110 |
| Database: Cochrane Library |
| #1 artificial intelligence:ab,ti,kw or AI:ab,ti,kw or deep learning:ab,ti,kw or machine learning:ab,ti,kw or computer:ab,ti,kw or neural network:ab,ti,kw or CNN:ab,ti,kw or automatic:ab,ti,kw or automated:ab,ti,kw: 60782 #2 MeSH descriptor: [capsule endoscopy] explode all trees: 132 #3 capsule endoscopy:ab,ti,kw: 726 #4 #2 or #3: 726 #5 MeSH descriptor: [tumors] explode all trees: 83592 #6 MeSH descriptor: [polyps] explode all trees: 1165 #7 protruded:ab,ti,kw or tumor:ab,ti,kw or polyp:ab,ti,kw: #8 #5 or #6 or #7: 134070 #9 #1 and #4 and #8: 5 |
2.3. Inclusion Criteria
2.4. Methodological Quality
2.5. Data Extraction, Primary Outcomes, and Additional Analyses
2.6. Statistical Analysis
3. Results
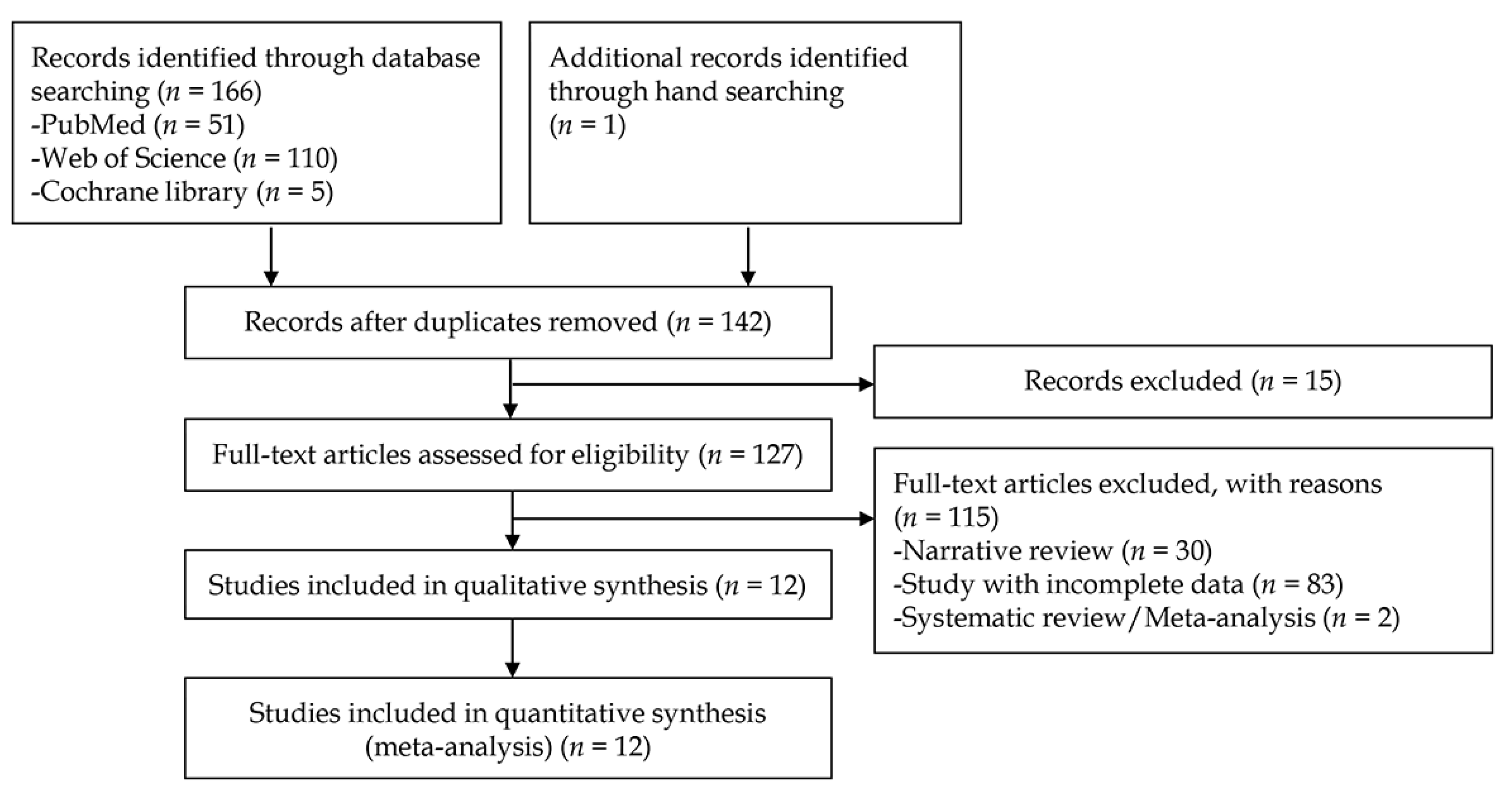
3.1. Study Selection Process

3.2. Clinical Characteristics
| Study/Year | Nationality of Data | Type of CAD Models | Type of Endoscopic Images | Training Dataset | Type of Test Datasets | Number of Protruded Lesions in Test Dataset | Number of Controls in Test Dataset | TP | FP | FN | TN | Target Conditions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Li B et al. (2009) [12] | unknown | Feature analysis (texture, color) with MLP | Still cut images | 150 polyp images and 150 normal mucosal images | Internal test | 150 | 150 | 134 | 6 | 16 | 124 | for small bowel polyp diagnosis |
| Hwang S (2011) [13] | unknown | BoW model-SVM | Still cut images | 25 polyp images and 50 normal mucosal images | Internal test | 50 | 100 | 33 | 5 | 17 | 95 | For small bowel polyp diagnosis |
| Karargyris A et al. (2011) [14] | US | Texture analysis with SVM | Still cut images | unclear | Internal test | 10 | 40 | 10 | 13 | 0 | 27 | For small bowel polyp diagnosis |
| Li B et al. (2011) [15] | China | Texture analysis with SVM | Still cut images | 550 tumor images and 550 normal mucosal images | Internal test | 50 | 50 | 45 | 1 | 5 | 49 | for small bowel tumor diagnosis |
| Li B et al. (2011) [16] | China | Texture analysis with an ensemble of kNN, MLP, or SVM | Still cut images | 450 tumor images and 450 normal mucosal images | Internal test | 150 | 150 | 138 | 17 | 12 | 133 | for small bowel tumor diagnosis |
| Barbosa DC et al. (2012) [17] | Portugal | Texture analysis with neural network | Still cut images | 700 tumor images and 2300 normal mucosal images | Internal test | 700 | 2300 | 657 | 159 | 43 | 2141 | for small bowel tumor diagnosis |
| Li B et al. (2012) [18] | China | Texture analysis with SVM | Stil lcut images | 540 tumor images and 540 normal mucosal images | Internal test | 60 | 60 | 51 | 11 | 9 | 49 | for small bowel tumor diagnosis |
| Li B et al. (2012) [19] | China | Texture analysis with SVM | Still cut images | 540 tumor images and 540 normal mucosal images | Internal test | 60 | 60 | 53 | 2 | 7 | 58 | for small bowel tumor diagnosis |
| Constantinescu AF et al. (2015) [20] | Romania | Texture analysis with neural network | Still cut images | unclear | Internal test | 32 | 58 | 30 | 5 | 2 | 53 | for intestinal polyp diagnosis |
| Kundu AK et al. (2020) [21] | from http://www.capsuleendoscopy.org | Linear discriminant analysis with SVM | Still cut images | 30 tumor images and 1617 normal mucosal images | Internal test | 30 | 1617 | 26 | 130 | 4 | 1487 | for small bowel tumor diagnosis |
| Saito H et al. (2020) [22] | Japan | CNN | Still cut images | 30,584 images of protruding lesions | Internal test | 7507 | 10000 | 6810 | 2019 | 697 | 7981 | for protruding lesion diagnosis (small bowel) |
| Yamada A et al. (2020) [23] | Japan | Single Shot MultiBox Detector | Still cut images | 15933 images | Internal test | 1850 | 2934 | 1462 | 380 | 388 | 2554 | for colorectal tumor diagnosis |
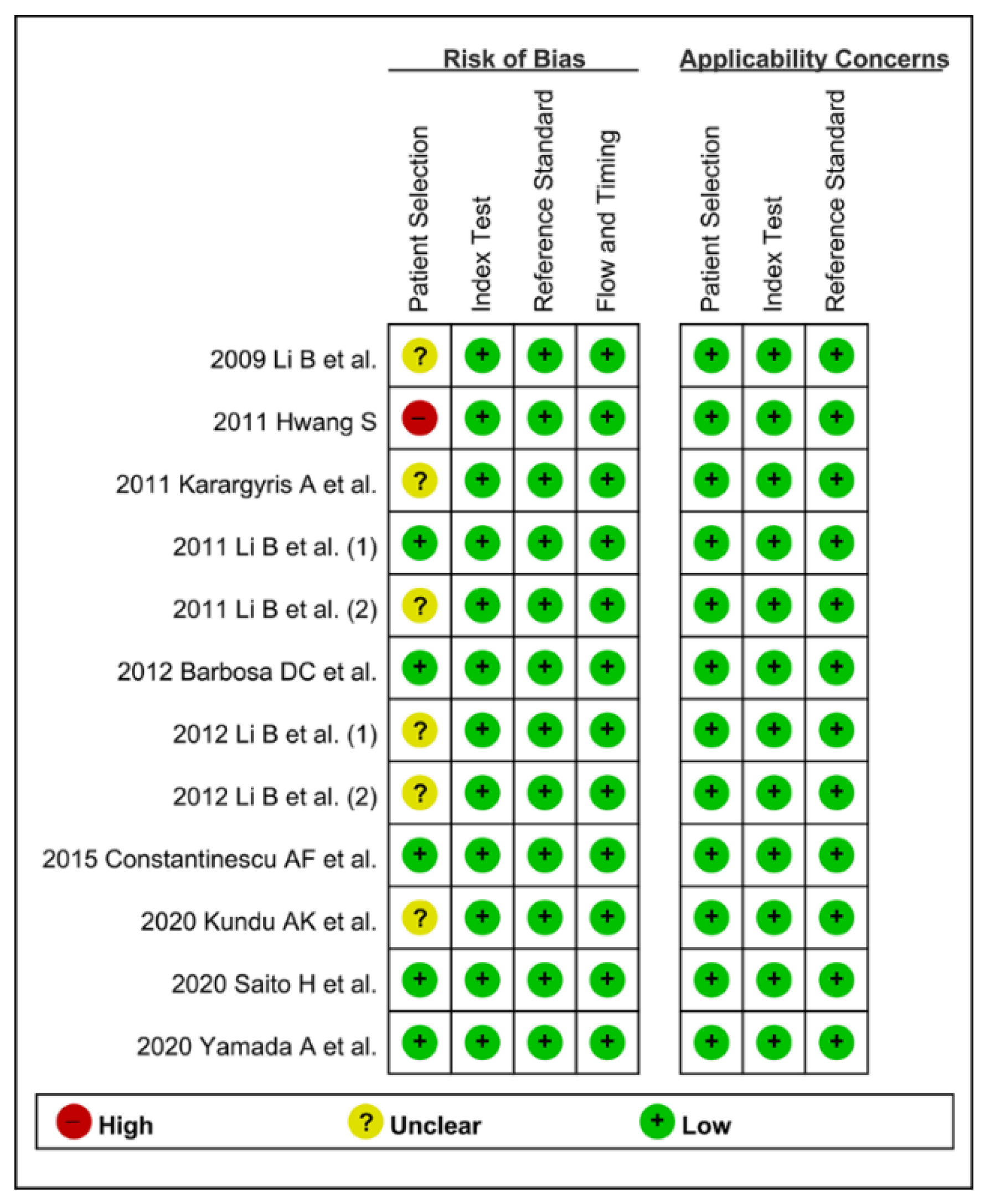
3.3. Methodological Quality Assessment

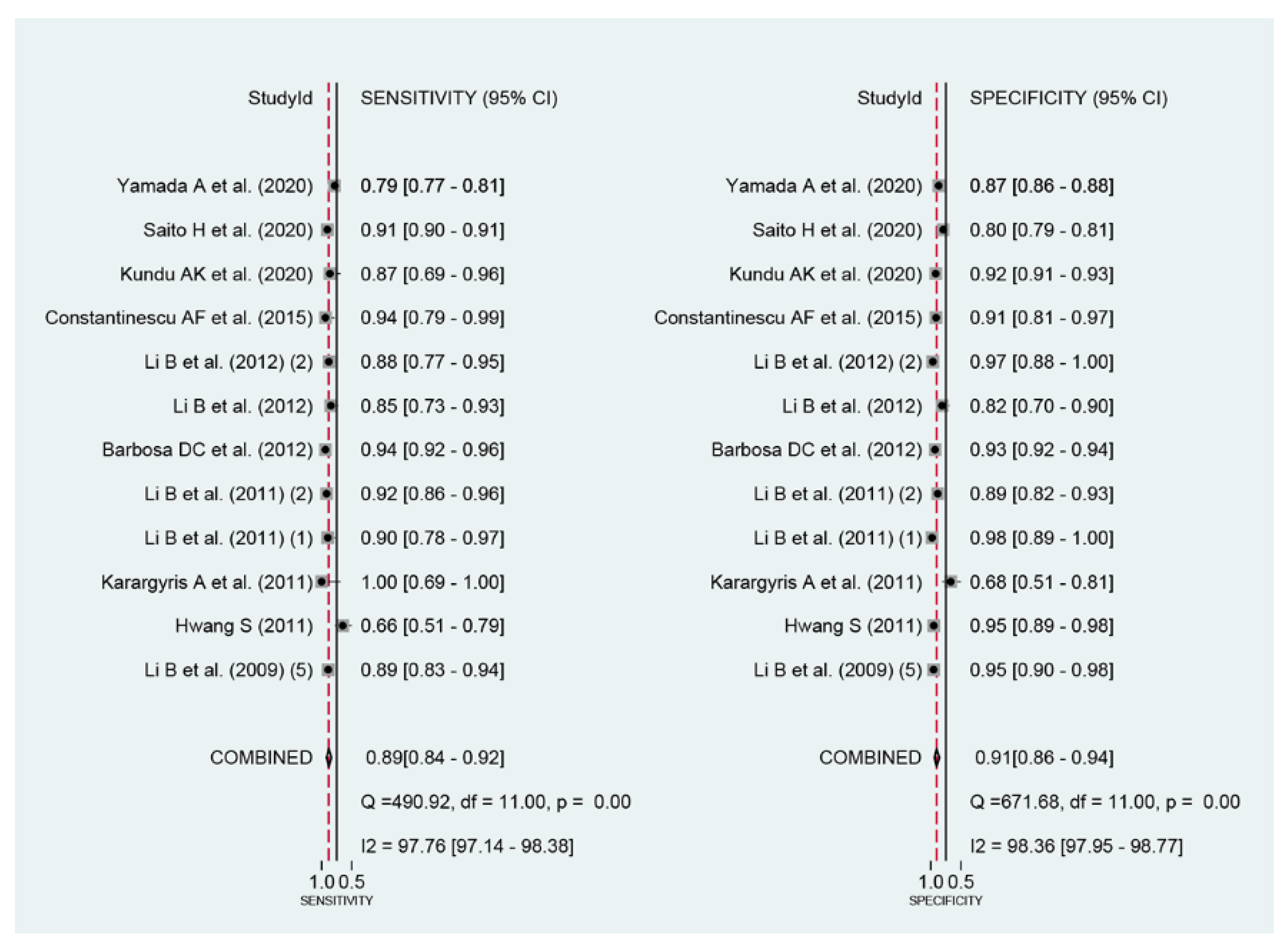
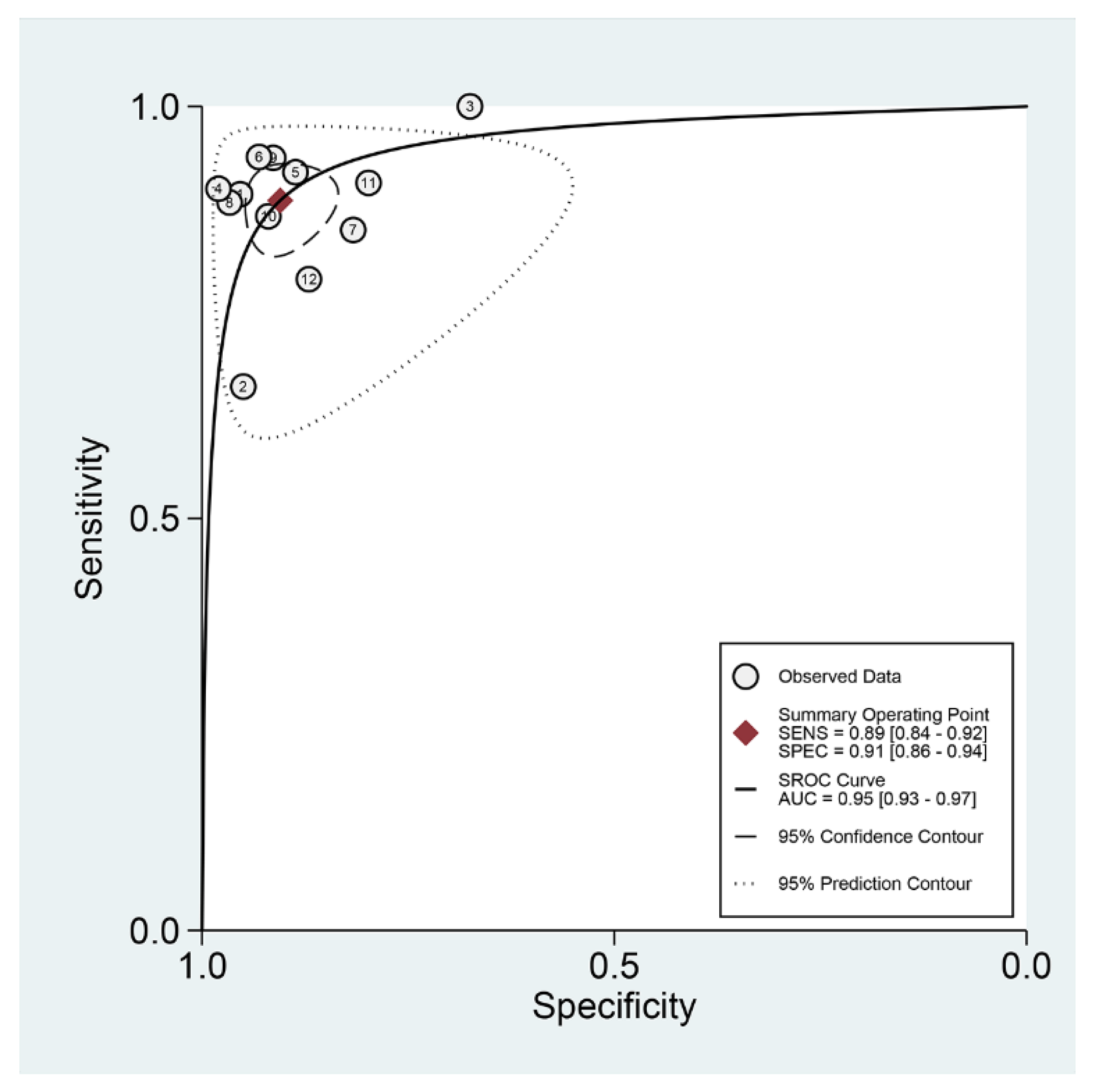
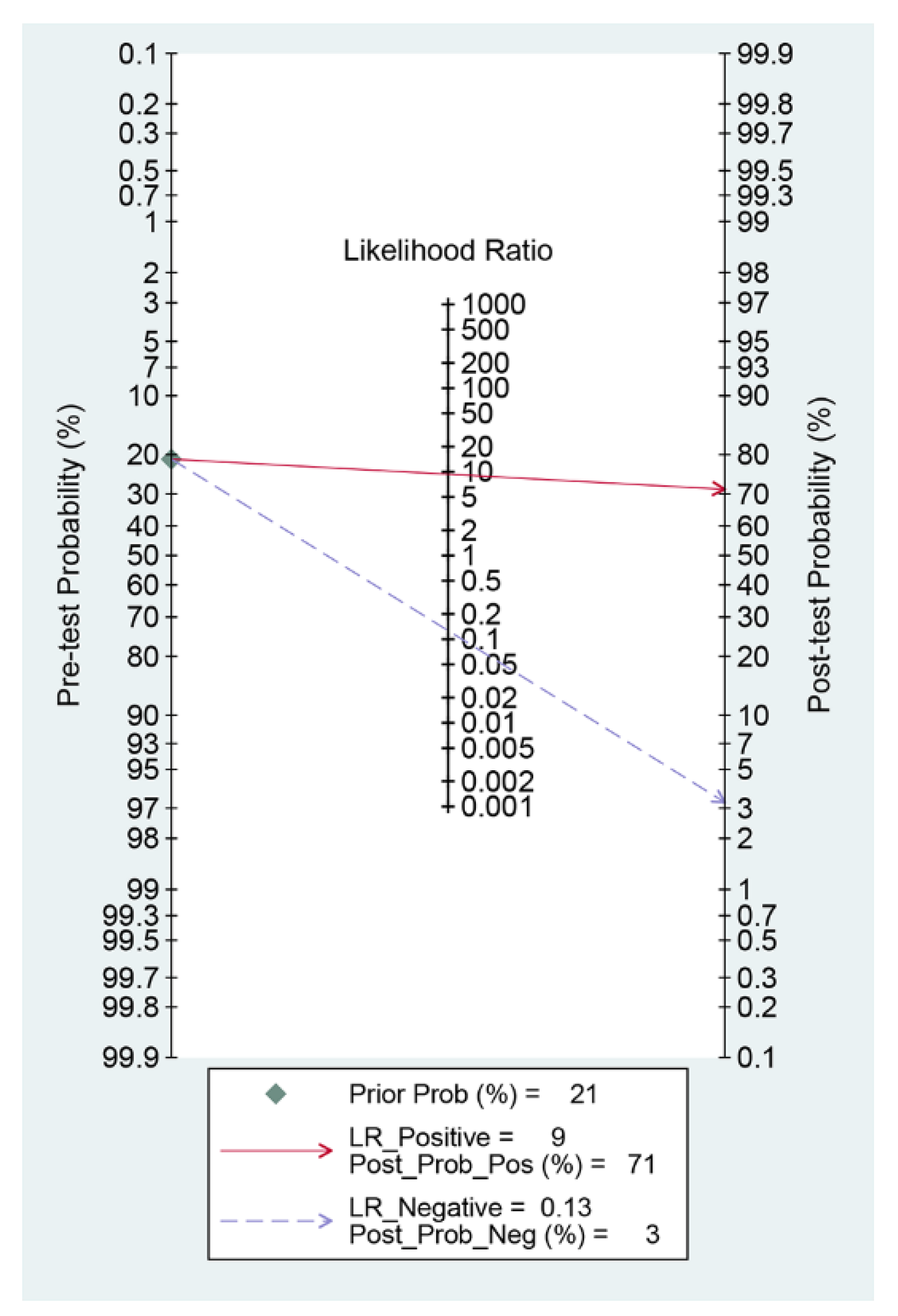
3.4. DTA Meta-Analysis



3.5. Heterogeneity Evaluation, Meta-Regression, and Subgroup Analysis
| Subgroup | Number of Included Studies | Sensitivity (95% CI) | Specificity (95% CI) | PLR | NLR | DOR | AUC |
|---|---|---|---|---|---|---|---|
| All the included studies | 12 | 0.89 (0.84–0.92) | 0.91 (0.86–0.94) | 9.3 (6.3–13.8) | 0.13 (0.09–0.18) | 74 (43–126) | 0.95 (0.93–0.97) |
| Ethnicity of data | |||||||
| Asian | 7 | 0.88 (0.83–0.91) | 0.90 (0.84–0.93) | 8.4 (5.4–13.2) | 0.14 (0.10–0.19) | 62 (33–117) | 0.94 (0.92–0.96) |
| Public database or unknown ethnicity | 2 | 0.84 (0.78–0.88) | 0.95 (0.92–0.98) | 16.3 (9.1–29.3) | 0.20 (0.06–0.65) | 81 (18–370) | Null |
| Western Published year | 3 | 0.94 (0.92–0.96) | 0.93 (0.92–0.94) | 7.5 (2.4–23.2) | 0.07 (0.05–0.09) | 199 (142–280) | 0.98 (0.97–0.99) |
| <10 years (published within 10 years) | 7 | 0.89 (0.84–0.93) | 0.89 (0.85–0.93) | 8.5 (5.8–12.4) | 0.12 (0.08–0.18) | 70 (36–135) | 0.95 (0.93–0.97) |
| >10 years | 5 | 0.91 (0.77–0.97) | 0.92 (0.82–0.96) | 10.9 (5.3–22.4) | 0.10 (0.04–0.25) | 107 (54–210) | 0.96 (0.94–0.98) |
| Total number of included images for the training dataset | |||||||
| 100≤ | 9 | 0.89 (0.86–0.92) | 0.91 (0.87–0.94) | 9.8 (6.5–14.6) | 0.12 (0.09–0.16) | 83 (46–151) | 0.95 (0.93–0.97) |
| <100 or unknown | 3 | 0.79 (0.70–0.87) | 0.88 (0.83–0.93) | 7.2 (1.9–26.9) | 0.15 (0.03–0.71) | 55 (23–134) | 0.95 (0.91–0.99) |
| Total number of included images for the test dataset | |||||||
| 100≤ | 11 | 0.88 (0.84–0.92) | 0.91 (0.88–0.94) | 10.2 (7.1–14.6) | 0.13 (0.09–0.18) | 79 (46–134) | 0.96 (0.93–0.97) |
| <100 | 1 | Null | Null | Null | Null | Null | Null |
| Methodological quality of included studies | |||||||
| High-quality | 5 | 0.90 (0.84–0.94) | 0.90 (0.84–0.94) | 9.2 (5.3–15.8) | 0.11 (0.07–0.18) | 84 (34–208) | 0.96 (0.94–0.97) |
| Unclear or low-quality | 7 | 0.88 (0.80–0.93) | 0.91 (0.84–0.95) | 9.4 (5.6–15.9) | 0.13 (0.08–0.21) | 72 (39–131) | 0.95 (0.93–0.97) |
| Type of CAD models | |||||||
| Neural network-based | 4 | 0.92 (0.91–0.94) | 0.91 (0.84–0.95) | 9.7 (5.5–17.3) | 0.08 (0.06–0.11) | 116 (53–254) | 0.95 (0.93–0.97) |
| Machine learning-based | 8 | 0.86 (0.79–0.91) | 0.90 (0.84–0.94) | 8.8 (5.3–14.5) | 0.16 (0.10–0.23) | 57 (30–108) | 0.94 (0.92–0.96) |
| Type of target lesions | |||||||
| Tumors | 7 | 0.89 (0.85–0.93) | 0.91 (0.89–0.93) | 10.0 (7.8–12.7) | 0.12 (0.08–0.17) | 85 (46–156) | 0.95 (0.93–0.97) |
| Polyps | 4 | 0.94 (0.68–0.99) | 0.91 (0.79–0.96) | 10.3 (4.6–23.0) | 0.07 (0.01–0.39) | 148 (40–548) | 0.97 (0.95–0.98) |
| Other protruded lesion | 1 | Null | Null | Null | Null | Null | Null |
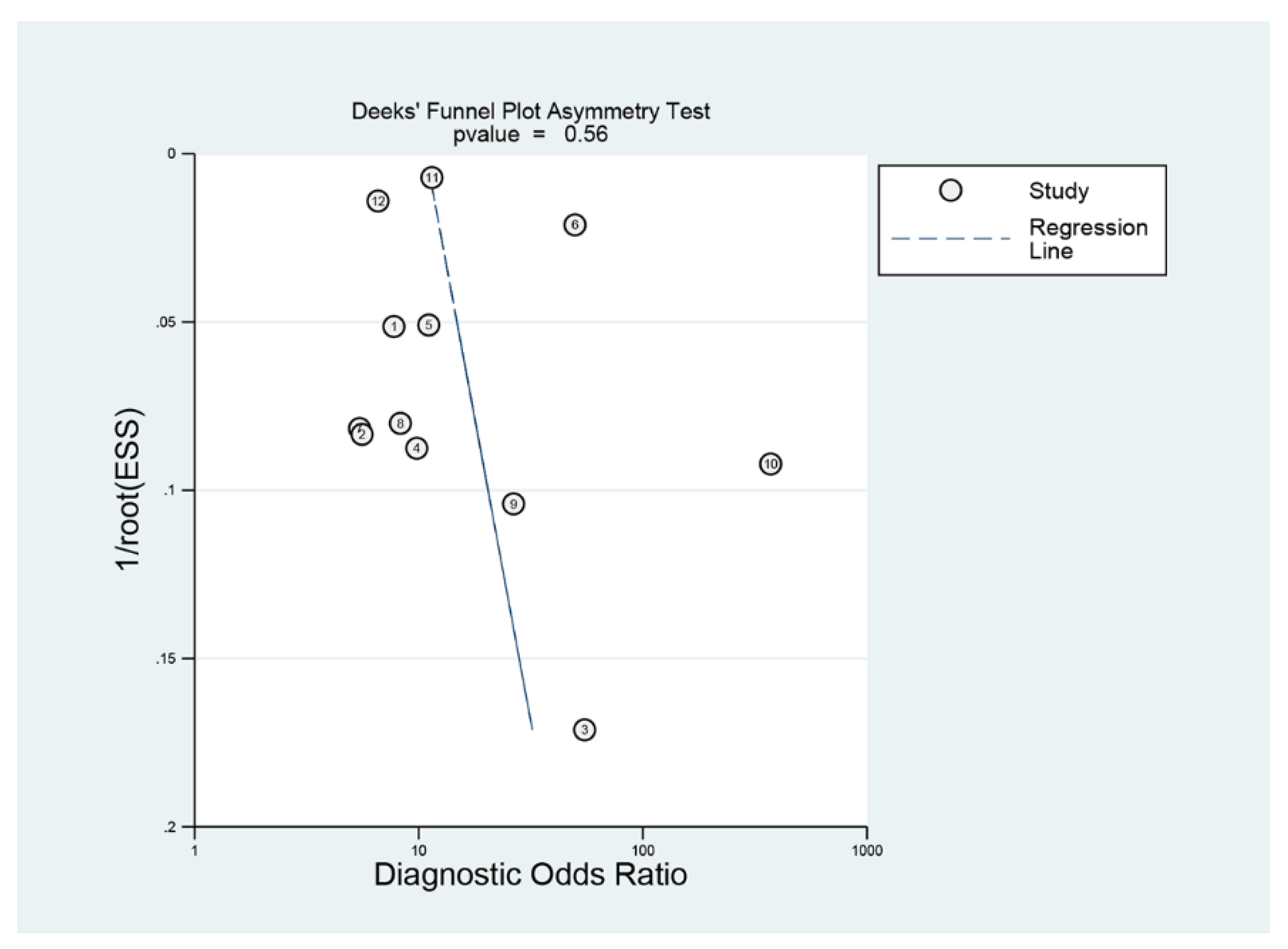
3.6. Publication Bias

4. Discussion
4.1. Main Findings
4.2. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Wang, A.; Banerjee, S.; Barth, B.A.; Bhat, Y.M.; Chauhan, S.; Gottlieb, K.; Konda, V.; Maple, J.T.; Murad, F.; Pfau, P.R.; et al. Wireless capsule endoscopy. Gastrointest. Endosc. 2013, 78, 805–815. [Google Scholar] [CrossRef] [PubMed]
- McAlindon, M.E.; Ching, H.L.; Yung, D.; Sidhu, R.; Koulaouzidis, A. Capsule endoscopy of the small bowel. Ann. Transl. Med. 2016, 4, 369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bang, C.S. Deep Learning in Upper Gastrointestinal Disorders: Status and Future Perspectives. Korean J. Gastroenterol. 2020, 75, 120–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.J.; Bang, C.S. Application of artificial intelligence in gastroenterology. World J. Gastroenterol. 2019, 25, 1666–1683. [Google Scholar] [CrossRef]
- Cho, B.-J.; Bang, C.S.; Lee, J.J.; Seo, C.W.; Kim, J.H. Prediction of Submucosal Invasion for Gastric Neoplasms in Endoscopic Images Using Deep-Learning. J. Clin. Med. 2020, 9, 1858. [Google Scholar] [CrossRef]
- Bang, C.S.; Lee, J.J.; Baik, G.H. Computer-aided diagnosis of esophageal cancer and neoplasms in endoscopic images: A systematic review and meta-analysis of diagnostic test accuracy. Gastrointest. Endosc. 2021, 93, 1006–1015.e13. [Google Scholar] [CrossRef]
- Cho, B.-J.; Bang, C.S.; Park, S.W.; Yang, Y.J.; Seo, S.I.; Lim, H.; Shin, W.G.; Hong, J.T.; Yoo, Y.T.; Hong, S.H.; et al. Automated classification of gastric neoplasms in endoscopic images using a convolutional neural network. Laryngo-Rhino-Otologie 2019, 51, 1121–1129. [Google Scholar] [CrossRef]
- Bang, C.S.; Lee, J.J.; Baik, G.H. Artificial Intelligence for the Prediction of Helicobacter Pylori Infection in Endoscopic Images: Systematic Review and Meta-Analysis of Diagnostic Test Accuracy. J. Med. Internet Res. 2020, 22, e21983. [Google Scholar] [CrossRef]
- Bang, C.S.; Lee, J.J.; Gwang, H.B. Computer-Aided Diagnosis of Diminutive Colorectal Polyps in Endoscopic Images: Systematic Review and Meta-analysis of Diagnostic Test Accuracy. J. Med. Internet Res. 2021, 23, e29682. [Google Scholar] [CrossRef]
- Berzin, T.M.; Parasa, S.; Wallace, M.B.; Gross, S.A.; Repici, A.; Sharma, P. Position statement on priorities for artificial intelligence in GI endoscopy: A report by the ASGE Task Force. Gastrointest. Endosc. 2020, 92, 951–959. [Google Scholar] [CrossRef]
- Bang, C.S.; Lim, H.; Jeong, H.M.; Hwang, S.H. Use of Endoscopic Images in the Prediction of Submucosal Invasion of Gastric Neoplasms: Automated Deep Learning Model Development and Usability Study. J. Med. Internet Res. 2021, 23, e25167. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Meng, M.Q.-H.; Xu, L. A comparative study of shape features for polyp detection in wireless capsule endoscopy images. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 3731–3774. [Google Scholar] [CrossRef]
- Hwang, S. Bag-of-visual-words approach to abnormal image detection in wireless capsule endoscopy videos. In Advances in Visual Computing; Lecture Notes in Computer Science; Bebis, G., Ed.; Springer: Berlin/Heidelberg, Germany, 2011; Volume 6939. [Google Scholar] [CrossRef]
- Karargyris, A.; Bourbakis, N. Detection of Small Bowel Polyps and Ulcers in Wireless Capsule Endoscopy Videos. IEEE Trans. Biomed. Eng. 2011, 58, 2777–2786. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Meng, M.Q.-H. Contourlet-Based Features for Computerized Tumor Detection in Capsule Endoscopy Images. Ann. Biomed. Eng. 2011, 39, 2891–2899. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Meng, M.Q.-H.; Lau, J.Y. Computer-aided small bowel tumor detection for capsule endoscopy. Artif. Intell. Med. 2011, 52, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, D.C.; Roupar, D.B.; Ramos, J.C.; Tavares, A.C.; Lima, C.S. Automatic small bowel tumor diagnosis by using multi-scale wavelet-based analysis in wireless capsule endoscopy images. Biomed. Eng. Online 2012, 11, 3. [Google Scholar] [CrossRef] [Green Version]
- Li, B.-P.; Meng, M.Q.-H. Comparison of Several Texture Features for Tumor Detection in CE Images. J. Med. Syst. 2011, 36, 2463–2469. [Google Scholar] [CrossRef]
- Li, B.; Meng, M.Q. Tumor recognition in wireless capsule endoscopy images using textural features and SVM-based feature selection. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 323–329. [Google Scholar] [CrossRef]
- Constantinescu, A.F.; Ionescu, M.; Iovănescu, V.F.; Ciurea, M.E.; Ionescu, A.G.; Streba, C.T.; Bunescu, M.G.; Rogoveanu, I.; Vere, C.C. A computer-aided diagnostic system for intestinal polyps identified by wireless capsule endoscopy. Romanian J. Morphol. Embryol. 2016, 57, 979–984. [Google Scholar]
- Kundu, A.K.; Fattah, S.A.; Wahid, K.A. Multiple Linear Discriminant Models for Extracting Salient Characteristic Patterns in Capsule Endoscopy Images for Multi-Disease Detection. IEEE J. Transl. Eng. Health Med. 2020, 8, 3300111. [Google Scholar] [CrossRef]
- Saito, H.; Aoki, T.; Aoyama, K.; Kato, Y.; Tsuboi, A.; Yamada, A.; Fujishiro, M.; Oka, S.; Ishihara, S.; Matsuda, T.; et al. Automatic detection and classification of protruding lesions in wireless capsule endoscopy images based on a deep convolutional neural network. Gastrointest. Endosc. 2020, 92, 144–151.e1. [Google Scholar] [CrossRef]
- Yamada, A.; Niikura, R.; Otani, K.; Aoki, T.; Koike, K. Automatic detection of colorectal neoplasia in wireless colon capsule endoscopic images using a deep convolutional neural network. Laryngo-Rhino-Otologie 2021, 53, 832–836. [Google Scholar] [CrossRef] [PubMed]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies. The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Rutter, C.M.; Gatsonis, C.A. A hierarchical regression approach to meta-analysis of diagnostic test accuracy evaluations. Stat. Med. 2001, 20, 2865–2884. [Google Scholar] [CrossRef]
- Reitsma, J.B.; Glas, A.S.; Rutjes, A.W.S.; Scholten, R.J.; Bossuyt, P.M.; Zwinderman, A.H. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J. Clin. Epidemiol. 2005, 58, 982–990. [Google Scholar] [CrossRef]
- Harbord, R.M.; Whiting, P. Metandi: Meta-analysis of diagnostic accuracy using hierarchical logistic regression. STATA J. 2009, 9, 211–229. [Google Scholar] [CrossRef] [Green Version]
- Littenberg, B.; Moses, L.E. Estimating diagnostic accuracy from multiple conflicting reports: A new meta-analytic method. Med. Decis. Making 1993, 13, 313–321. [Google Scholar] [CrossRef]
- Koh, A.-R.; Kim, C.-H.; Bang, J.-H.; Jung, K.-W.; Yu, H.-K. The Correlation between Colon Polyps and Metabolic Syndrome Parameters, Serum Uric Acid Level in Health Screen Examinees. Korean J. Fam. Pr. 2018, 8, 15–20. [Google Scholar] [CrossRef]
- Hausmann, J.; Tal, A.; Gomer, A.; Philipper, M.; Moog, G.; Hohn, H.; Hesselbarth, N.; Plass, H.; Albert, J.; Finkelmeier, F. Colon Capsule Endoscopy: Indications, Findings, and Complications—Data from a Prospective German Colon Capsule Registry Trial (DEKOR). Clin. Endosc. 2021, 54, 92–99. [Google Scholar] [CrossRef]
- Nam, S.-J.; Lee, H.S.; Lim, Y.J. Evaluation of Gastric Disease with Capsule Endoscopy. Clin. Endosc. 2018, 51, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.-S.; Sun, T.-J.; Zhang, H.-D. Human gastric magnet-controlled capsule endoscopy conducted in a standing position: The phase 1 study. BMC Gastroenterol. 2019, 19, 184. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.; Guo, S.; Guo, J. Conceptual design of a novel magnetically actuated hybrid microrobot. In Proceedings of the IEEE International Conference on Mechatronics and Automation (ICMA), Takamatsu, Japan, 6–9 August 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 1001–1005. [Google Scholar] [CrossRef]
- Boal Carvalho, P.; Magalhães, J.; Dias, D.E.; Castro, F.; Monteiro, S.; Rosa, B.; Moreira, M.J.; Cotter, J. Suspected blood indicator in capsule endoscopy: A valuable tool for gastrointestinal bleeding diagnosis. Arq. Gastroenterol. 2017, 54, 16–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tal, A.O.; Filmann, N.; Makhlin, K.; Hausmann, J.; Friedrich-Rust, M.; Herrmann, E.; Zeuzem, S.; Albert, J.G. The capsule endoscopy “suspected blood indicator” (SBI) for detection of active small bowel bleeding: No active bleeding in case of negative SBI. Scand. J. Gastroenterol. 2014, 49, 1131–1135. [Google Scholar] [CrossRef] [PubMed]
- Bang, C.S.; Ahn, J.Y.; Kim, J.-H.; Kim, Y.-I.; Choi, I.J.; Shin, W.G. Establishing Machine Learning Models to Predict Curative Resection in Early Gastric Cancer with Undifferentiated Histology: Development and Usability Study. J. Med. Internet Res. 2021, 23, e25053. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.J.; Gong, E.J.; Bang, C.S.; Lee, J.J.; Suk, K.T.; Baik, G.H. Computer-Aided Diagnosis of Gastrointestinal Protruded Lesions Using Wireless Capsule Endoscopy: A Systematic Review and Diagnostic Test Accuracy Meta-Analysis. J. Pers. Med. 2022, 12, 644. https://doi.org/10.3390/jpm12040644
Kim HJ, Gong EJ, Bang CS, Lee JJ, Suk KT, Baik GH. Computer-Aided Diagnosis of Gastrointestinal Protruded Lesions Using Wireless Capsule Endoscopy: A Systematic Review and Diagnostic Test Accuracy Meta-Analysis. Journal of Personalized Medicine. 2022; 12(4):644. https://doi.org/10.3390/jpm12040644
Chicago/Turabian StyleKim, Hye Jin, Eun Jeong Gong, Chang Seok Bang, Jae Jun Lee, Ki Tae Suk, and Gwang Ho Baik. 2022. "Computer-Aided Diagnosis of Gastrointestinal Protruded Lesions Using Wireless Capsule Endoscopy: A Systematic Review and Diagnostic Test Accuracy Meta-Analysis" Journal of Personalized Medicine 12, no. 4: 644. https://doi.org/10.3390/jpm12040644
APA StyleKim, H. J., Gong, E. J., Bang, C. S., Lee, J. J., Suk, K. T., & Baik, G. H. (2022). Computer-Aided Diagnosis of Gastrointestinal Protruded Lesions Using Wireless Capsule Endoscopy: A Systematic Review and Diagnostic Test Accuracy Meta-Analysis. Journal of Personalized Medicine, 12(4), 644. https://doi.org/10.3390/jpm12040644