
Effect of Tumor Targeted-Anthracycline Nanomedicine, HPMA Copolymer-Conjugated Pirarubicin (P-THP) against Gynecological Malignancies

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. In Vitro Cytotoxicity Assay
2.3. Intracellular Uptake Analysis of THP and P-THP
2.4. In Vivo Antitumor Effect of P-THP
3. Results
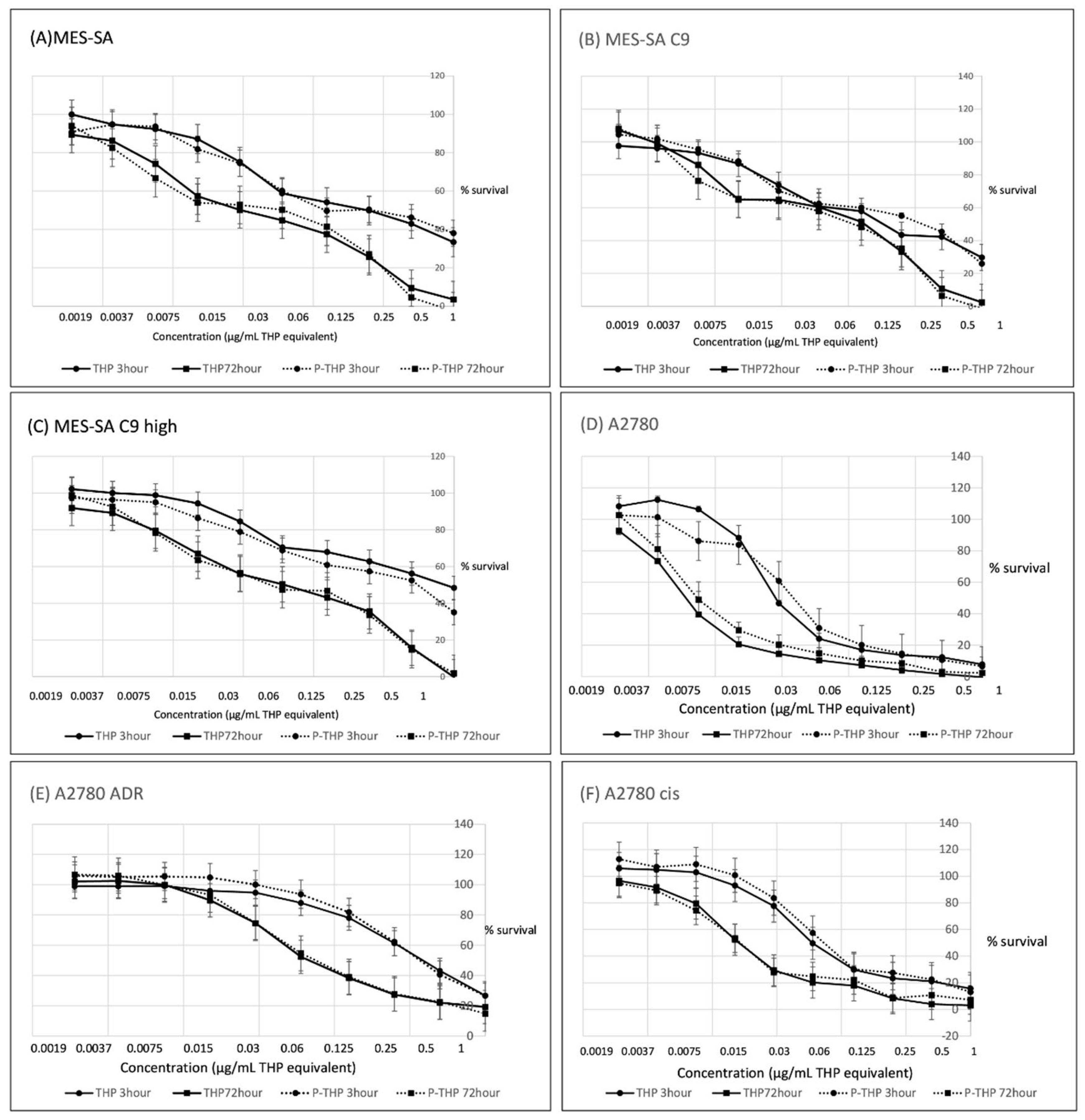
3.1. Cytotoxicity Assay for Gynecological Malignancies of P-THP In Vitro
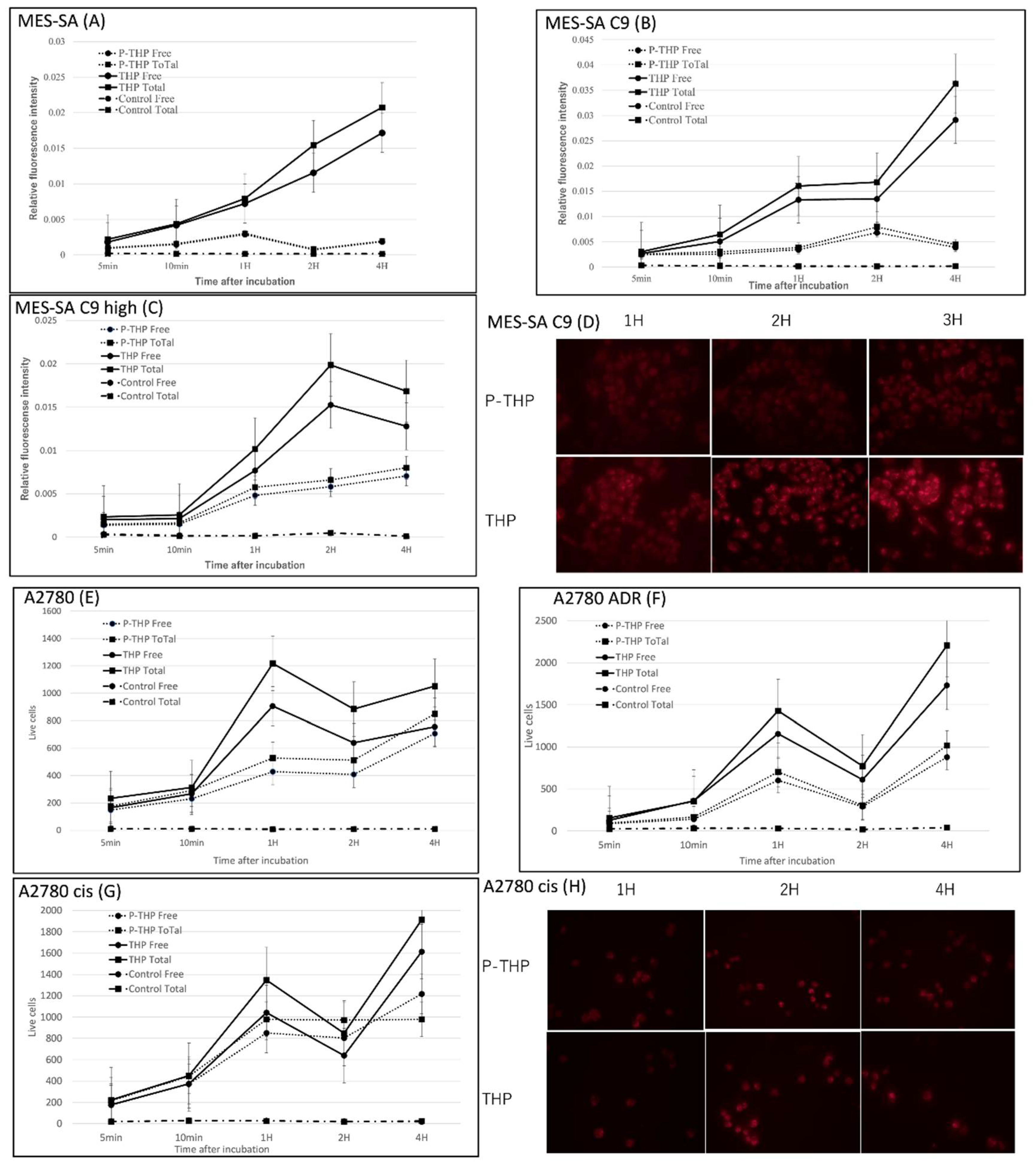
3.2. Intracellular Uptake of THP and P-THP
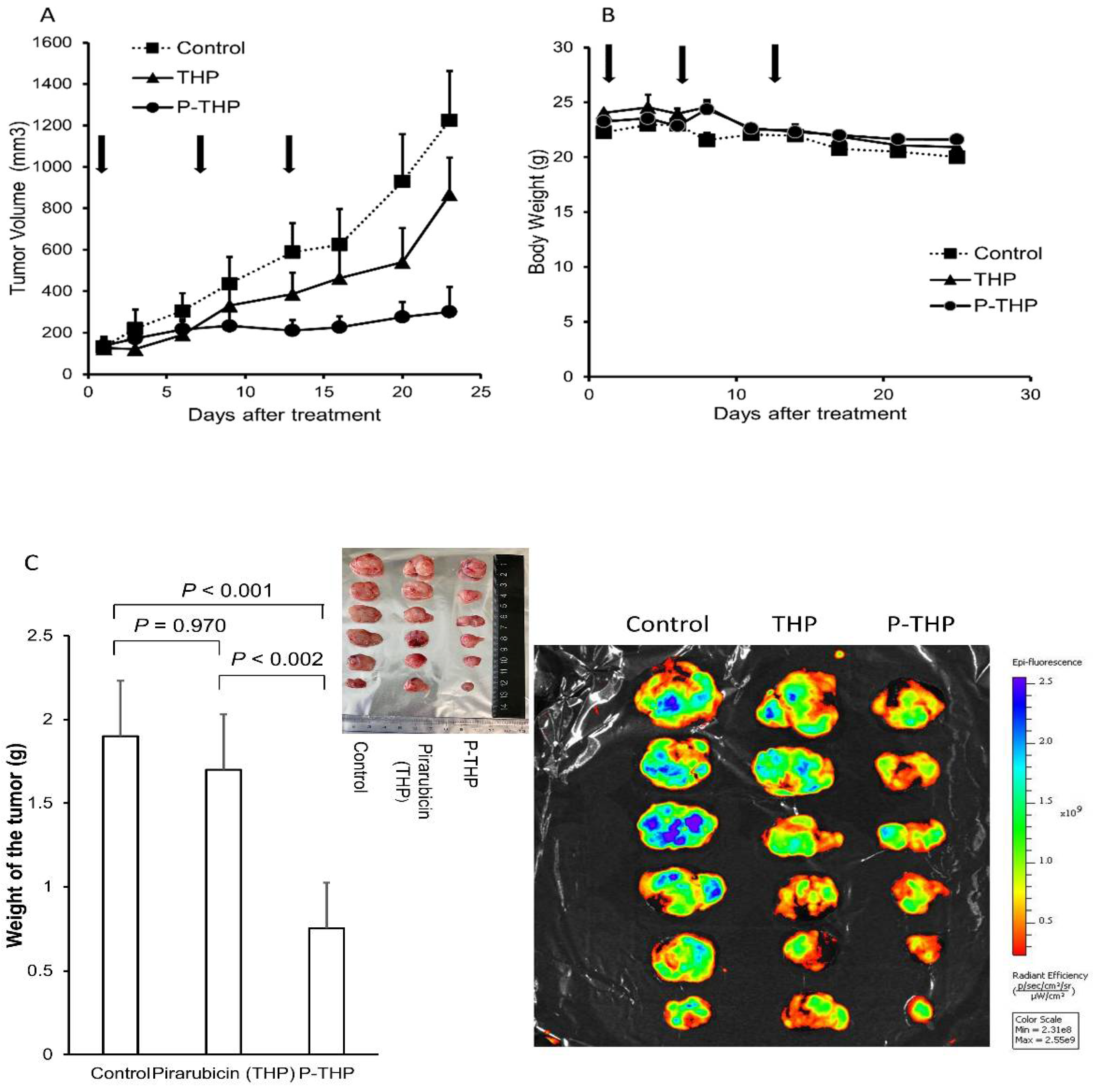
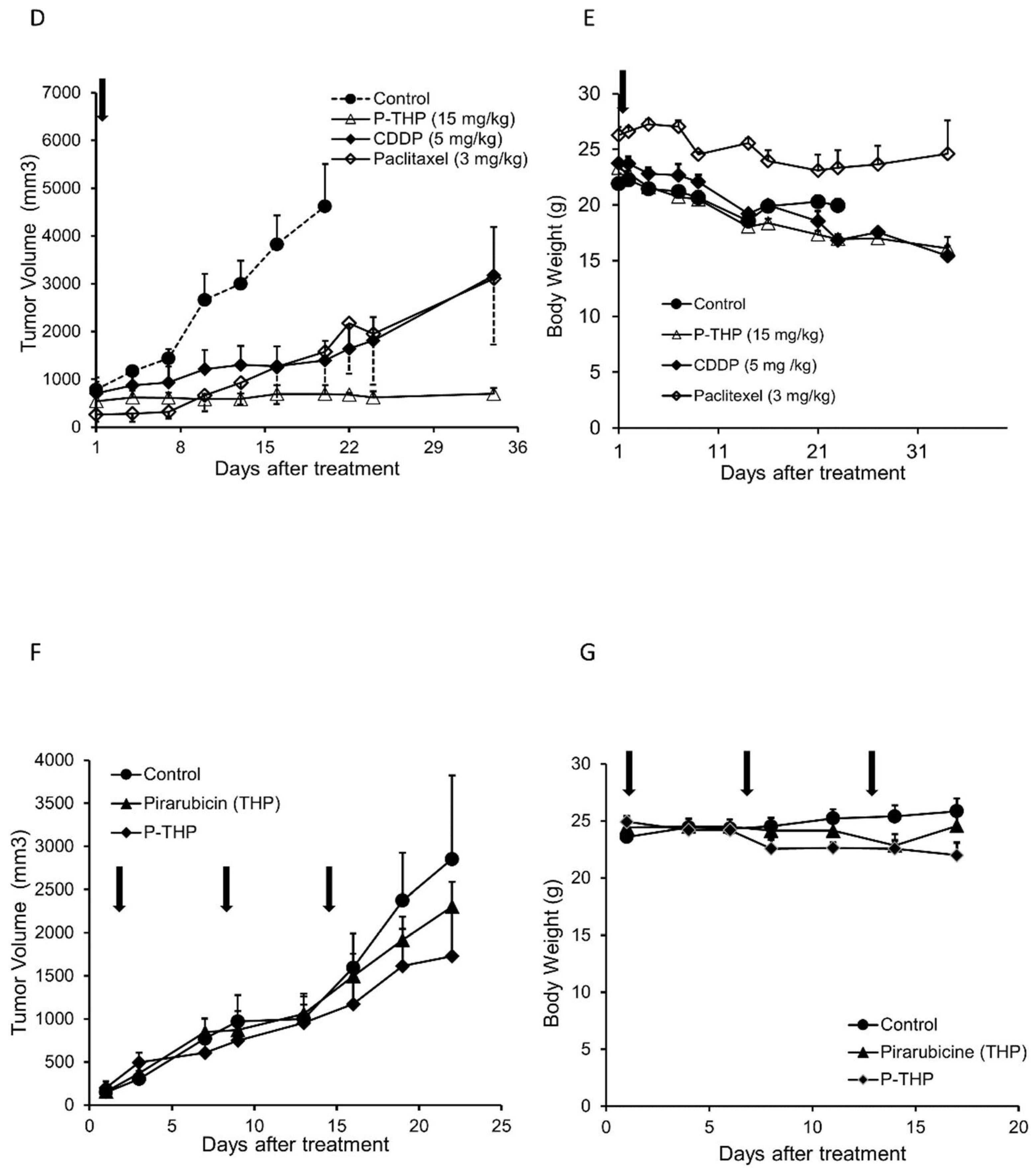
3.3. In Vivo Therapeutic Effects of P-THP against Gynecological Malignancies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Perol, D.; Gonzalez-Martin, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Maenpaa, J.; et al. Olaparib plus bevacizumab as first-line maintenance in ovarian cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Wagner, U.; Aavall-Lundqvist, E.; Gebski, V.; Heywood, M.; Vasey, P.A.; Volgger, B.; Vergote, I.; Pignata, S.; Ferrero, A.; et al. Pegylated liposomal doxorubicin and carboplatin compared with paclitaxel and carboplatin for patients with platinum-sensitive ovarian cancer in late relapse. J. Clin. Oncol. 2010, 28, 3323–3329. [Google Scholar] [CrossRef]
- Gabizon, A.; Catane, R.; Uziely, B.; Kaufman, B.; Safra, T.; Cohen, R.; Martin, F.; Huang, A.; Barenholz, Y. Prolonged circulation time and enhanced accumulation in malignant exudates of doxorubicin encapsulated in polyethylene-glycol coated liposomes. Cancer Res. 1994, 54, 987–992. [Google Scholar]
- Zamboni, W.C. Liposomal, nanoparticle, and conjugated formulations of anticancer agents. Clin. Cancer Res. 2005, 11, 8230–8234. [Google Scholar] [CrossRef] [Green Version]
- Nakanishi, T.; Aoki, D.; Watanabe, Y.; Ando, Y.; Tomotsugu, N.; Sato, Y.; Saito, T. A Phase II clinical trial of pegylated liposomal doxorubicin and carboplatin in Japanese patients with platinum-sensitive recurrent ovarian, fallopian tube or primary peritoneal cancer. Jpn. J. Clin. Oncol. 2015, 45, 422–426. [Google Scholar] [CrossRef] [Green Version]
- Nomura, H.; Aoki, D.; Michimae, H.; Mizuno, M.; Nakai, H.; Arai, M.; Sasagawa, M.; Ushijima, K.; Sugiyama, T.; Saito, M.; et al. Effect of taxane plus platinum regimens vs doxorubicin plus cisplatin as adjuvant chemotherapy for endometrial cancer at a high risk of progression: A randomized clinical trial. JAMA Oncol. 2019, 5, 833–840. [Google Scholar] [CrossRef]
- Makker, V.; Colombo, N.; Casado Herraez, A.; Santin, A.D.; Colomba, E.; Miller, D.S.; Fujiwara, K.; Pignata, S.; Baron-Hay, S.; Ray-Coquard, I.; et al. Lenvatinib plus pembrolizumab for advanced endometrial cancer. N. Engl. J. Med. 2022, 386, 437–448. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair-deficient cancer: Results from the Phase II KEYNOTE-158 study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ott, P.A.; Bang, Y.J.; Berton-Rigaud, D.; Elez, E.; Pishvaian, M.J.; Rugo, H.S.; Puzanov, I.; Mehnert, J.M.; Aung, K.L.; Lopez, J.; et al. Safety and antitumor activity of pembrolizumab in advanced programmed death ligand 1-positive endometrial cancer: Results from the KEYNOTE-028 study. J. Clin. Oncol. 2017, 35, 2535–2541. [Google Scholar] [CrossRef] [PubMed]
- Hensley, M.L.; Maki, R.; Venkatraman, E.; Geller, G.; Lovegren, M.; Aghajanian, C.; Sabbatini, P.; Tong, W.; Barakat, R.; Spriggs, D.R. Gemcitabine and docetaxel in patients with unresectable leiomyosarcoma: Results of a phase II trial. J. Clin. Oncol. 2002, 20, 2824–2831. [Google Scholar] [CrossRef] [PubMed]
- Seddon, B.; Strauss, S.J.; Whelan, J.; Leahy, M.; Woll, P.J.; Cowie, F.; Rothermundt, C.; Wood, Z.; Benson, C.; Ali, N.; et al. Gemcitabine and docetaxel versus doxorubicin as first-line treatment in previously untreated advanced unresectable or metastatic soft-tissue sarcomas (GeDDiS): A randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1397–1410. [Google Scholar] [CrossRef] [Green Version]
- Dozono, H.; Yanazume, S.; Nakamura, H.; Etrych, T.; Chytil, P.; Ulbrich, K.; Fang, J.; Arimura, T.; Douchi, T.; Kobayashi, H.; et al. HPMA copolymer-conjugated pirarubicin in multimodal treatment of a patient with stage IV prostate cancer and extensive lung and bone metastases. Target. Oncol. 2016, 11, 101–106. [Google Scholar] [CrossRef]
- Nakamura, H.; Etrych, T.; Chytil, P.; Ohkubo, M.; Fang, J.; Ulbrich, K.; Maeda, H. Two step mechanisms of tumor selective delivery of N-(2-hydroxypropyl)methacrylamide copolymer conjugated with pirarubicin via an acid-cleavable linkage. J. Control. Release 2014, 174, 81–87. [Google Scholar] [CrossRef]
- Maeda, H. The 35th Anniversary of the Discovery of EPR Effect: A new wave of nanomedicines for tumor-targeted drug delivery-personal remarks and future prospects. J. Pers Med. 2021, 11, 229. [Google Scholar] [CrossRef]
- Nakamura, H.; Koziolova, E.; Etrych, T.; Chytil, P.; Fang, J.; Ulbrich, K.; Maeda, H. Comparison between linear and star-like HPMA conjugated pirarubicin (THP) in pharmacokinetics and antitumor activity in tumor bearing mice. Eur. J. Pharm. Biopharm. 2015, 90, 90–96. [Google Scholar] [CrossRef]
- Omura, G.A.; Blessing, J.A.; Major, F.; Lifshitz, S.; Ehrlich, C.E.; Mangan, C.; Beecham, J.; Park, R.; Silverberg, S. A randomized clinical trial of adjuvant adriamycin in uterine sarcomas: A gynecologic oncology group study. J. Clin. Oncol. 1985, 3, 1240–1245. [Google Scholar] [CrossRef]
- Beller, U.; Quinn, M.A.; Benedet, J.L.; Creasman, W.T.; Ngan, H.Y.; Maisonneuve, P.; Pecorelli, S.; Odicino, F.; Heintz, A.P. Carcinoma of the vulva. FIGO 26th annual report on the results of treatment in gynecological cancer. Int. J. Gynaecol. Obs. 2006, 95 (Suppl. S1), S7–S27. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: The AURELIA open-label randomized phase III trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Markman, M.; Hall, J.; Spitz, D.; Weiner, S.; Carson, L.; Van Le, L.; Baker, M. Phase II trial of weekly single-agent paclitaxel in platinum/paclitaxel-refractory ovarian cancer. J. Clin. Oncol. 2002, 20, 2365–2369. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y.; Maeda, H. A new concept for macromolecular therapeutics in cancer chemotherapy: Mechanism of tumoritropic accumulation of proteins and the antitumor agent smancs. Cancer Res. 1986, 46, 6387–6392. [Google Scholar] [PubMed]
- Fang, J.; Nakamura, H.; Maeda, H. The EPR effect: Unique features of tumor blood vessels for drug delivery, factors involved, and limitations and augmentation of the effect. Adv. Drug Deliv. Rev. 2011, 63, 136–151. [Google Scholar] [CrossRef] [PubMed]
- Islam, R.; Maeda, H.; Fang, J. Factors affecting the dynamics and heterogeneity of the EPR effect: Pathophysiological and pathoanatomic features, drug formulations and physicochemical factors. Expert Opin. Drug Deliv. 2022, 19, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Desmaele, D.; Gref, R.; Couvreur, P. Squalenoylation: A generic platform for nanoparticular drug delivery. J. Control. Release 2012, 161, 609–618. [Google Scholar] [CrossRef]
- Rammal, H.; Al Assaad, A.; Dosio, F.; Stella, B.; Maksimenko, A.; Mura, S.; Van Gulick, L.; Callewaert, M.; Desmaele, D.; Couvreur, P.; et al. Investigation of squalene-doxorubicin distribution and interactions within single cancer cell using Raman microspectroscopy. Nanomedicine 2021, 35, 102404. [Google Scholar] [CrossRef]
- Nakamura, H.; Koziolová, E.; Chytil, P.; Tsukigawa, K.; Fang, J.; Haratake, M.; Ulbrich, K.; Etrych, T.; Maeda, H. Pronounced Cellular Uptake of Pirarubicin versus That of Other Anthracyclines: Comparison of HPMA Copolymer Conjugates of Pirarubicin and Doxorubicin. Mol Pharm. 2016, 13, 4106–4115. [Google Scholar] [CrossRef]
- Matsumura, Y.; Hamaguchi, T.; Ura, T.; Muro, K.; Yamada, Y.; Shimada, Y.; Shirao, K.; Okusaka, T.; Ueno, H.; Ikeda, M.; et al. Phase I clinical trial and pharmacokinetic evaluation of NK911, a micelle-encapsulated doxorubicin. Br. J. Cancer 2004, 91, 1775–1781. [Google Scholar] [CrossRef]
- Prabhakar, U.; Maeda, H.; Jain, R.K.; Sevick-Muraca, E.M.; Zamboni, W.; Farokhzad, O.C.; Barry, S.T.; Gabizon, A.; Grodzinski, P.; Blakey, D.C. Challenges and key considerations of the enhanced permeability and retention effect for nanomedicine drug delivery in oncology. Cancer Res. 2013, 73, 2412–2417. [Google Scholar] [CrossRef] [Green Version]
- Ewer, M.S.; Yeh, E.T.H. Cardiac complications of cancer treatment. In Holland-Frei Cancer Medicine, 6th ed.; Kufe, D.W., Pollock, R.E., Weichselbaum, R.R., Bast, R.C., Gansler, T.S.G., Holland, J.F., Frei, E., Eds.; BC Decker Inc.: London, UK, 2003. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Incubation Times | LC50 (μg/mL) | Incubation Times | LC50 (μg/mL) | ||
|---|---|---|---|---|---|
| THP | P-THP | ||||
| MES-SA | 3 h | 0.063 | MES-SA | 3 h | 0.253 |
| 72 h | 0.017 | 72 h | 0.042 | ||
| MES-SA C9 | 3 h | 0.207 | MES-SA C9 | 3 h | 0.251 |
| 72 h | 0.091 | 72 h | 0.045 | ||
| MES-SA C9 high | 3 h | 0.029 | MES-SA C9 high | 3 h | 0.378 |
| 72 h | 0.026 | 72 h | 0.051 | ||
| A2780 | 3 h | 0.111 | A2780 | 3 h | 0.065 |
| 72 h | 0.018 | 72 h | 0.044 | ||
| A2780cis | 3 h | 0.050 | A2780cis | 3 h | 0.111 |
| 72 h | 0.068 | 72 h | 0.028 | ||
| A2780ADR | 3 h | 0.904 | A2780ADR | 3 h | 0.567 |
| 72 h | 0.192 | 72 h | 0.189 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yanazume, S.; Fang, J.; Islam, R.; Gao, S.; Kobayashi, H. Effect of Tumor Targeted-Anthracycline Nanomedicine, HPMA Copolymer-Conjugated Pirarubicin (P-THP) against Gynecological Malignancies. J. Pers. Med. 2022, 12, 814. https://doi.org/10.3390/jpm12050814
Yanazume S, Fang J, Islam R, Gao S, Kobayashi H. Effect of Tumor Targeted-Anthracycline Nanomedicine, HPMA Copolymer-Conjugated Pirarubicin (P-THP) against Gynecological Malignancies. Journal of Personalized Medicine. 2022; 12(5):814. https://doi.org/10.3390/jpm12050814
Chicago/Turabian StyleYanazume, Shintaro, Jun Fang, Rayhanul Islam, Shanghui Gao, and Hiroaki Kobayashi. 2022. "Effect of Tumor Targeted-Anthracycline Nanomedicine, HPMA Copolymer-Conjugated Pirarubicin (P-THP) against Gynecological Malignancies" Journal of Personalized Medicine 12, no. 5: 814. https://doi.org/10.3390/jpm12050814
APA StyleYanazume, S., Fang, J., Islam, R., Gao, S., & Kobayashi, H. (2022). Effect of Tumor Targeted-Anthracycline Nanomedicine, HPMA Copolymer-Conjugated Pirarubicin (P-THP) against Gynecological Malignancies. Journal of Personalized Medicine, 12(5), 814. https://doi.org/10.3390/jpm12050814