
Multifactorial Analysis of Endodontic Microsurgery Using Finite Element Models

 ,
,  ,
, 
 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Premolar Model
2.2. Biomechanical Factors
2.3. Design of Experiments Validation
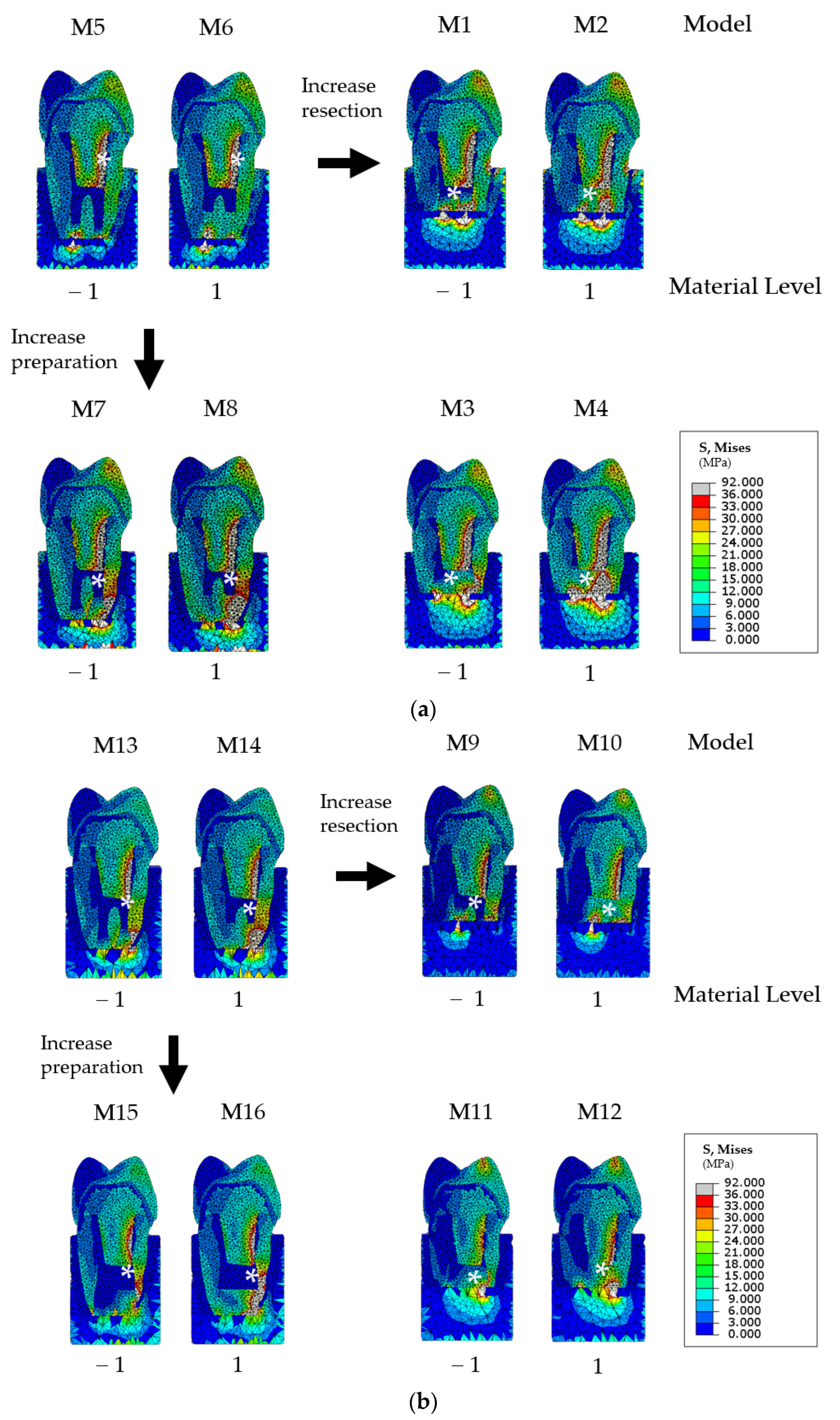
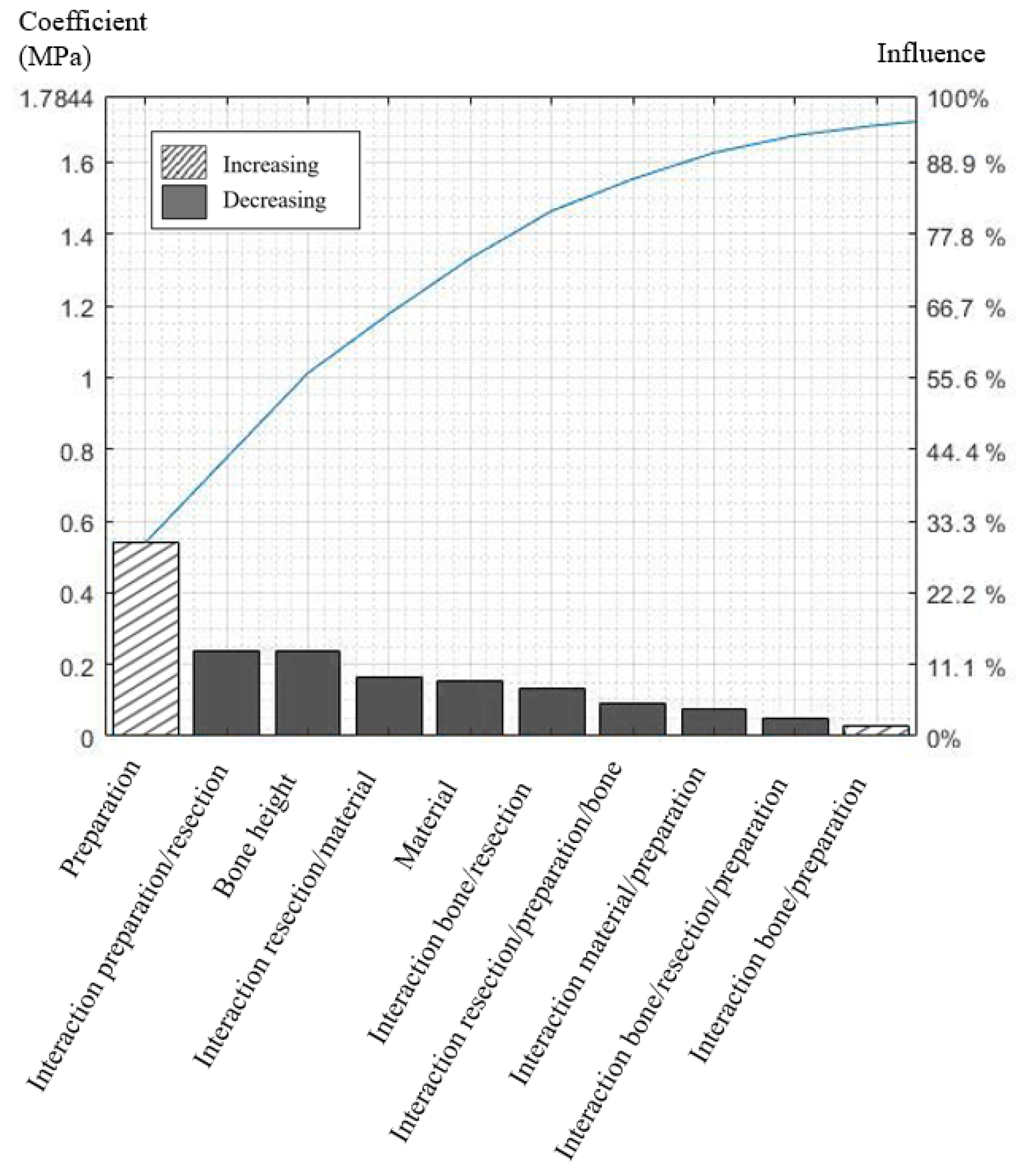
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Von Arx, T.; Jensen, S.S.; Hänni, S.; Friedman, S. Five-Year Longitudinal Assessment of the Prognosis of Apical Microsurgery. J. Endod. 2012, 38, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Von Arx, T.; Maldonado, P.; Bornstein, M.M. Occurrence of Vertical Root Fractures after Apical Surgery: A Retrospective Analysis. J. Endod. 2020, 47, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Sarnadas, M.; Marques, J.A.; Baptista, I.P.; Santos, J.M. Impact of Periodontal Attachment Loss on the Outcome of Endodontic Microsurgery: A Systematic Review and Meta-Analysis. Medicina 2021, 57, 922. [Google Scholar] [CrossRef] [PubMed]
- Pinto, D.; Marques, A.; Pereira, J.; Palma, P.; Santos, J. Long-Term Prognosis of Endodontic Microsurgery—A Systematic Review and Meta-Analysis. Medicina 2020, 56, 447. [Google Scholar] [CrossRef]
- Kohli, M.R.; Berenji, H.; Setzer, F.C.; Lee, S.-M.; Karabucak, B. Outcome of Endodontic Surgery: A Meta-analysis of the Literature—Part 3: Comparison of Endodontic Microsurgical Techniques with 2 Different Root-end Filling Materials. J. Endod. 2018, 44, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.; Hong, H.-T.; Roh, B.-D.; Chun, H.-J. Influence of Apical Root Resection on the Biomechanical Response of a Single-rooted Tooth: A 3-dimensional Finite Element Analysis. J. Endod. 2014, 40, 1489–1493. [Google Scholar] [CrossRef]
- Ran, S.J.; Yang, X.; Sun, Z.; Zhang, Y.; Chen, J.X.; Wang, D.M.; Liu, B. Effect of length of apical root resection on the biomechanical response of a maxillary central incisor in various occlusal relationships. Int. Endod. J. 2019, 53, 111–121. [Google Scholar] [CrossRef]
- Kim, S.; Park, S.-Y.; Lee, Y.; Lee, C.-J.; Karabucak, B.; Kim, H.-C.; Kim, E. Stress Analyses of Retrograde Cavity Preparation Designs for Surgical Endodontics in the Mesial Root of the Mandibular Molar: A Finite Element Analysis—Part I. J. Endod. 2019, 45, 442–446. [Google Scholar] [CrossRef]
- Kim, S.; Chen, D.; Park, S.-Y.; Lee, C.-J.; Kim, H.-C.; Kim, E. Stress Analyses of Retrograde Cavity Preparation Designs for Surgical Endodontics in the Mesial Root of the Mandibular Molar: A Finite Element Analysis—Part II. J. Endod. 2020, 46, 539–544. [Google Scholar] [CrossRef]
- Lin, C.-L.; Chang, W.-J.; Lin, Y.-S.; Chang, Y.-H.; Lin, Y.-F. Evaluation of the relative contributions of multi-factors in an adhesive MOD restoration using FEA and the Taguchi method. Dent. Mater. 2009, 25, 1073–1081. [Google Scholar] [CrossRef]
- Jacinto, H.; Kéchichian, R.; Desvignes, M.; Prost, R.; Valette, S. A web interface for 3D visualization and interactive segmentation of medical images. In Proceedings of the 17th International Conference on 3D Web Technology, Los Angeles, CA, USA, 4 August 2012; pp. 51–58. [Google Scholar] [CrossRef] [Green Version]
- Ortún-Terrazas, J.; Cegoñino, J.; Santana-Penin, U.; Santana-Mora, U.; del Palomar, A.P. Approach towards the porous fibrous structure of the periodontal ligament using micro-computerized tomography and finite element analysis. J. Mech. Behav. Biomed. Mater. 2018, 79, 135–149. [Google Scholar] [CrossRef] [PubMed]
- Richert, R.; Farges, J.-C.; Tamimi, F.; Naouar, N.; Boisse, P.; Ducret, M. Validated Finite Element Models of Premolars: A Scoping Review. Materials 2020, 13, 3280. [Google Scholar] [CrossRef] [PubMed]
- Hondrum, S.O. Temporary Dental Restorative Materials for Military Field Use. Mil. Med. 1998, 163, 381–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.-Y.; Kim, E. Does apical root resection in endodontic microsurgery jeopardize the prosthodontic prognosis? Restor. Dent. Endod. 2013, 38, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, X.; Li, C.; Jia, L.; Wang, Y.; Liu, W.; Zhou, X.; Huang, D. Materials for retrograde filling in root canal therapy. Cochrane Database Syst. Rev. 2016, 12. [Google Scholar] [CrossRef]
- Abusrewil, S.M.; McLean, W.; Scott, J.A. The use of Bioceramics as root-end filling materials in periradicular surgery: A literature review. Saudi Dent. J. 2018, 30, 273–282. [Google Scholar] [CrossRef]
- Rubinstein, R.A.; Kim, S. Long-Term Follow-Up of Cases Considered Healed One Year after Apical Microsurgery. J. Endod. 2002, 28, 378–383. [Google Scholar] [CrossRef]
- Lindeboom, J.A.; Frenken, J.W.; Kroon, F.H.; van den Akker, H.P. A comparative prospective randomized clinical study of MTA and IRM as root-end filling materials in single-rooted teeth in endodontic surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 100, 495–500. [Google Scholar] [CrossRef]
- Ha, W.N.; Nicholson, T.; Kahler, B.; Walsh, L.J. Methodologies for measuring the setting times of mineral trioxide aggregate and Portland cement products used in dentistry. Acta Biomater. Odontol. Scand. 2016, 2, 25–30. [Google Scholar] [CrossRef]
- Girish, K.; Mandava, J.; Chandra, R.R.; Ravi, R.; Anwarullah, A.; Athaluri, M. Effect of obturating materials on fracture resistance of simulated immature teeth. J. Conserv. Dent. 2017, 20, 115–119. [Google Scholar] [CrossRef]
- Elnaghy, A.M.; Elsaka, S. Fracture resistance of simulated immature teeth filled with Biodentine and white mineral trioxide aggregate-anin vitrostudy. Dent. Traumatol. 2015, 32, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Linsuwanont, P.; Kulvitit, S.; Santiwong, B. Reinforcement of Simulated Immature Permanent Teeth after Mineral Trioxide Aggregate Apexification. J. Endod. 2018, 44, 163–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azim, A.A.; Albanyan, H.; Azim, K.A.; Piasecki, L. The Buffalo study: Outcome and associated predictors in endodontic microsurgery- a cohort study. Int. Endod. J. 2020, 54, 301–318. [Google Scholar] [CrossRef] [PubMed]
- Rosen, E.; Beitlitum, I.; Tsesis, I. The preservation of teeth with root-originated fractures. Evid.-Based Endod. 2018, 3, 2. [Google Scholar] [CrossRef]
- Von Arx, T.; Peñarrocha, M.; Jensen, S.S. Prognostic Factors in Apical Surgery with Root-end Filling: A Meta-analysis. J. Endod. 2010, 36, 957–973. [Google Scholar] [CrossRef]
- Richert, R.; Farges, J.-C.; Villat, C.; Valette, S.; Boisse, P.; Ducret, M. Decision Support for Removing Fractured Endodontic Instruments: A Patient-Specific Approach. Appl. Sci. 2021, 11, 2602. [Google Scholar] [CrossRef]
- Zhang, Y.-R.; Du, W.; Zhou, X.-D.; Yu, H.-Y. Review of research on the mechanical properties of the human tooth. Int. J. Oral Sci. 2014, 6, 61–69. [Google Scholar] [CrossRef] [Green Version]
- Lahoud, P.; Jacobs, R.; Boisse, P.; EzEldeen, M.; Ducret, M.; Richert, R. Precision medicine using patient-specific modelling: State of the art and perspectives in dental practice. Clin. Oral Investig. 2022, 1–12. [Google Scholar] [CrossRef]
- Richert, R.; Robinson, P.; Viguie, G.; Farges, J.-C.; Ducret, M. Multi-Fiber-Reinforced Composites for the Coronoradicular Reconstruction of Premolar Teeth: A Finite Element Analysis. BioMed Res. Int. 2018, 2018, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Setzer, F.C.; Kohli, M.R.; Shah, S.B.; Karabucak, B.; Kim, S. Outcome of Endodontic Surgery: A Meta-analysis of the Literature—Part 2: Comparison of Endodontic Microsurgical Techniques with and without the Use of Higher Magnification. J. Endod. 2011, 38, 1–10. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Material | Model |
|---|---|
| Dentine | Linear elastic isotropic E = 18,600 MPa, ν = 0.31 |
| Ligament | Hyper-elastic Ogden 1 μ = 0.12 MPa, α= 20.9 MPa, D = 10 |
| Trabecular bone | Linear elastic isotropic E = 1300 MPa, ν = 0.3 |
| Cortical bone | Linear elastic isotropic E = 13,000 MPa, ν = 0.3 |
| Zirconia Crown | Linear elastic isotropic E = 190,000 MPa, ν = 0.33 |
| Metal Post | Linear elastic isotropic E = 190,000 MPa, ν = 0.33 |
| Gutta | Linear elastic isotropic E = 69 MPa, ν = 0.45 |
| Cement | Linear elastic isotropic E = 3000 MPa, ν = 0.3 |
| Root canal Material 1 | Linear elastic isotropic E = 1000 MPa, ν = 0.3 |
| Root canal Material 2 | Linear elastic isotropic E = 22,000 MPa, ν = 0.3 |
| Parameter | Low Level (−) | High Level (+) |
|---|---|---|
| A—Material | 1000 MPa | 22,000 MPa |
| B—Preparation | 1.5 mm | 2.2 mm |
| C—Resection length | 3 mm | 6 mm |
| D—Bone height | −2 mm | 0 mm |
| Low Bone Height | High Bone Height | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Model | Material | Preparation | Resection | Bone | VMS 1 | Model | Material | Preparation | Resection | Bone | VMS 1 |
| M1 | −1 | −1 | +1 | −1 | 1.76 MPa | M9 | −1 | −1 | +1 | +1 | 1.40 MPa |
| M2 | +1 | −1 | +1 | −1 | 1.75 MPa | M10 | +1 | −1 | +1 | +1 | 1.39 MPa |
| M3 | −1 | +1 | +1 | −1 | 2.59 MPa | M11 | −1 | +1 | +1 | +1 | 1.88 MPa |
| M4 | +1 | +1 | +1 | −1 | 2.26 MPa | M12 | +1 | +1 | +1 | +1 | 1.58 MPa |
| M5 | −1 | −1 | −1 | −1 | 3.14 MPa | M13 | −1 | −1 | −1 | +1 | 3.06 MPa |
| M6 | +1 | −1 | −1 | −1 | 3.17 MPa | M14 | +1 | −1 | −1 | +1 | 3.14 MPa |
| M7 | −1 | +1 | −1 | −1 | 3.62 MPa | M15 | −1 | +1 | −1 | +1 | 2.71 MPa |
| M8 | +1 | +1 | −1 | −1 | 2.52 MPa | M16 | +1 | +1 | −1 | +1 | 1.88 MPa |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richert, R.; Farges, J.-C.; Maurin, J.-C.; Molimard, J.; Boisse, P.; Ducret, M. Multifactorial Analysis of Endodontic Microsurgery Using Finite Element Models. J. Pers. Med. 2022, 12, 1012. https://doi.org/10.3390/jpm12061012
Richert R, Farges J-C, Maurin J-C, Molimard J, Boisse P, Ducret M. Multifactorial Analysis of Endodontic Microsurgery Using Finite Element Models. Journal of Personalized Medicine. 2022; 12(6):1012. https://doi.org/10.3390/jpm12061012
Chicago/Turabian StyleRichert, Raphael, Jean-Christophe Farges, Jean-Christophe Maurin, Jérôme Molimard, Philippe Boisse, and Maxime Ducret. 2022. "Multifactorial Analysis of Endodontic Microsurgery Using Finite Element Models" Journal of Personalized Medicine 12, no. 6: 1012. https://doi.org/10.3390/jpm12061012
APA StyleRichert, R., Farges, J. -C., Maurin, J. -C., Molimard, J., Boisse, P., & Ducret, M. (2022). Multifactorial Analysis of Endodontic Microsurgery Using Finite Element Models. Journal of Personalized Medicine, 12(6), 1012. https://doi.org/10.3390/jpm12061012