
Management of Patients with Severe Asthma and Chronic Rhinosinusitis with Nasal Polyps: A Multidisciplinary Shared Approach

 , ,
, ,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
1.1. CRSwNP and Asthma: Common Pathophysiological Mechanisms
1.2. Multidisciplinary Approach: A Crucial Point in Comorbidities Management
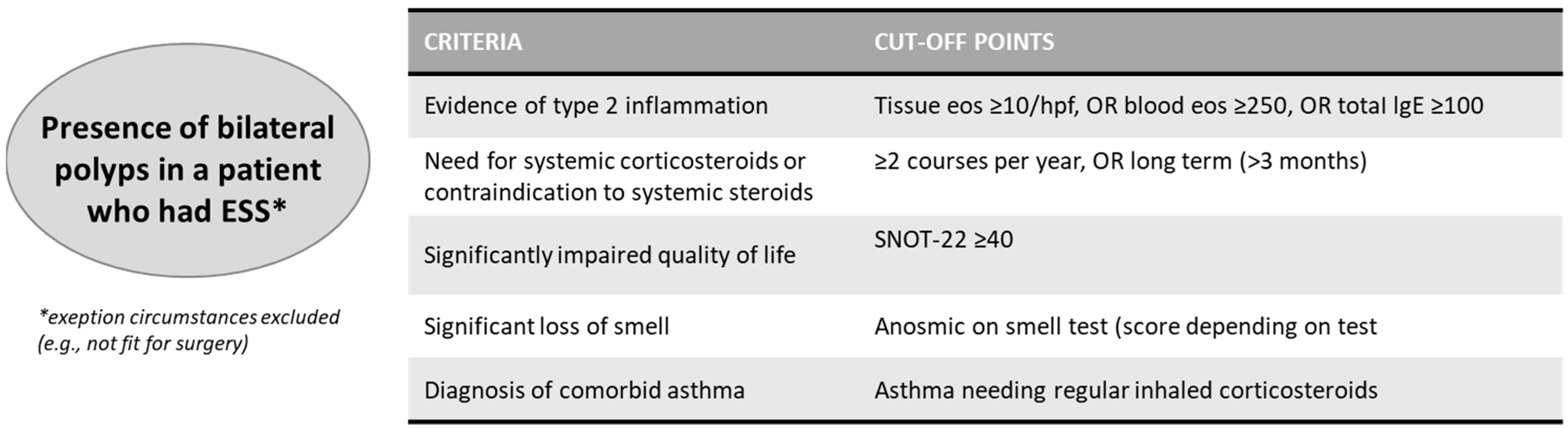
1.3. Indications for Biological Treatment in Severe Asthma and CRSwNP
2. Materials and Methods
- Patient with asthma who needs to start a biologic therapy being visited at the allergy/pulmonary unit complaining about nasal symptoms.
- Patient with severe asthma with an ongoing biologic therapy, being visited at the allergy/pulmonary unit complaining about nasal symptoms.
- Patient with severe CRSwNP being visited at the ENT unit and complaining about asthma symptoms.
3. Results and Discussion of Patients’ Management Flows
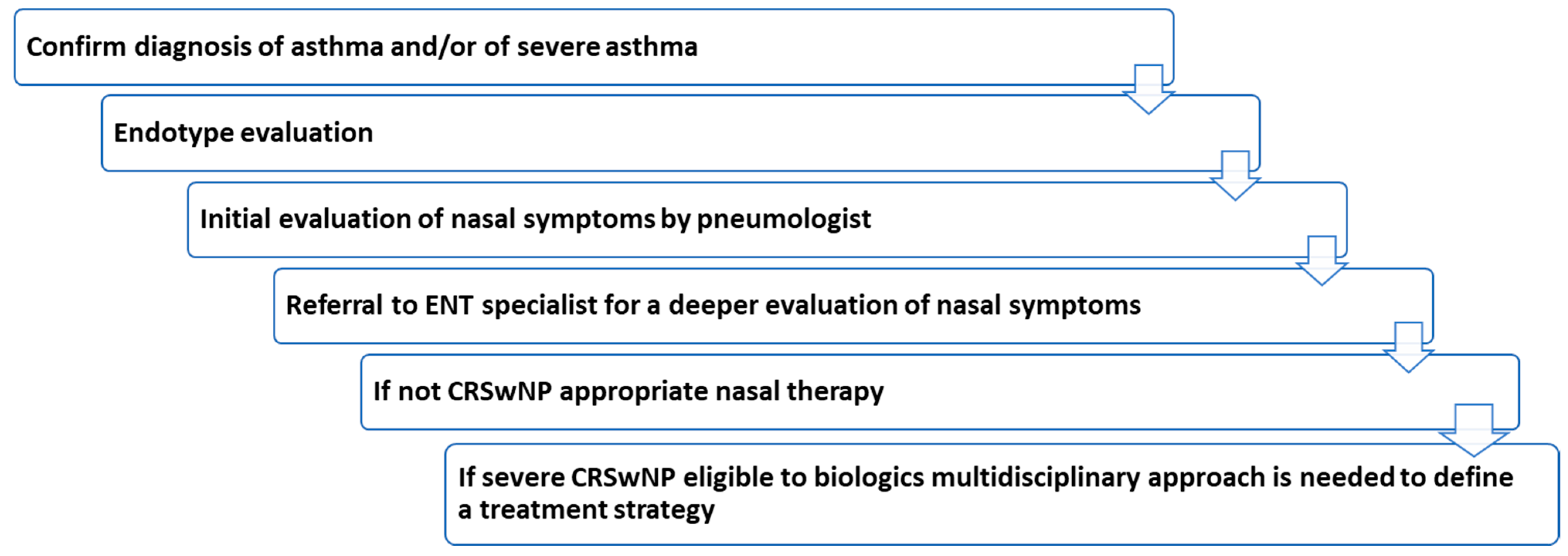
3.1. Patient with Severe Asthma Who Needs to Start a Biologic Therapy at the Allergy/Pulmonary Unit Complaining about Nasal Symptoms
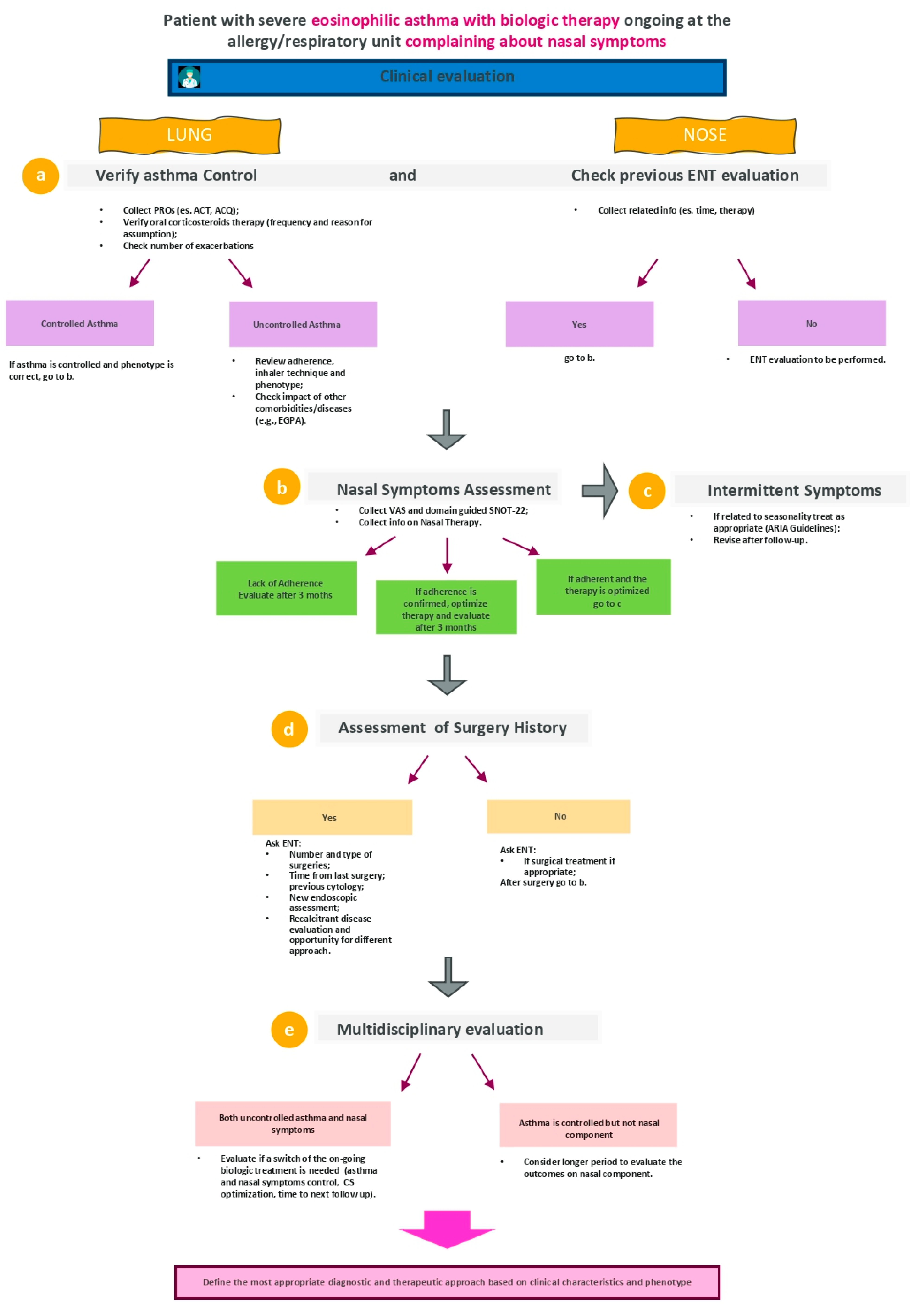
3.2. Patient with Severe Asthma with Ongoing Biologic Therapy at the Allergy/Pulmonary Unit Complaining about Nasal Symptoms
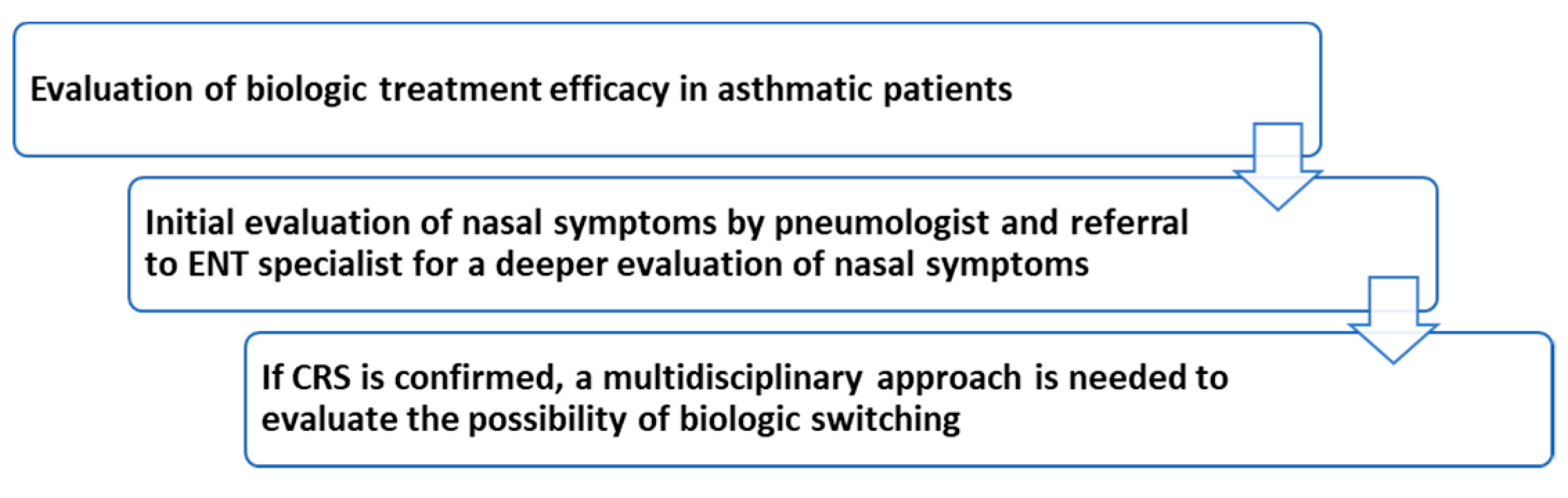
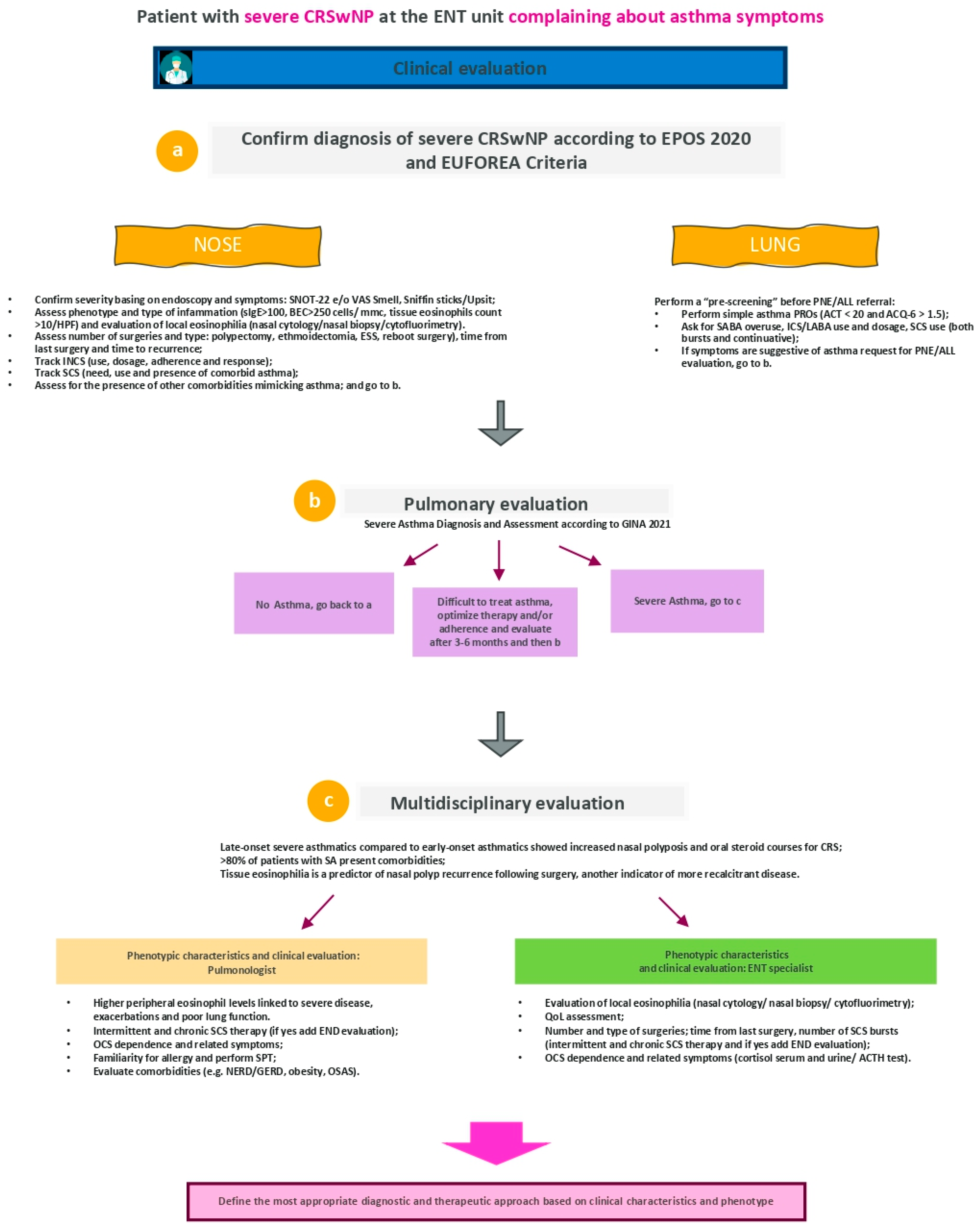
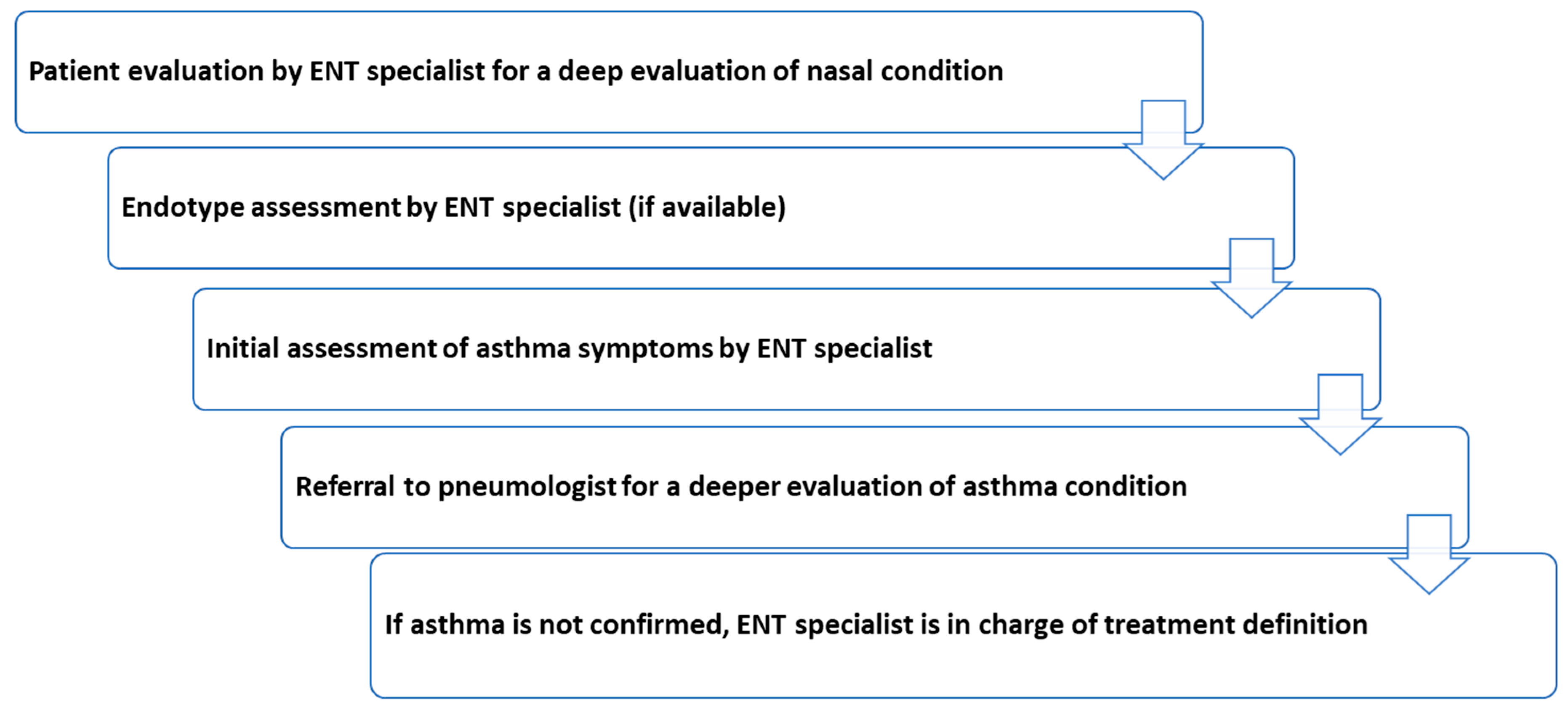
3.3. Patient with Severe CRSwNP at the ENT Unit Complaining about Asthma Symptoms
4. Final Considerations
- A close collaboration between pulmonologist, ENT specialist and allergist/immunologist is required for patients with asthma complaining nasal symptoms and vice versa, since the first patient take-charge when asthma or CRS diagnosis has to be done. These professionals should be working within the same center or in close collaboration with a multidimensional network.
- Patient reported outcomes are useful tools for patient QoL assessment and can be recorded by different specialists to allow collection and tracking changes in clinical symptoms over time and allowing better disease control among patients and specialists.
- Comorbidities should be always investigated as they affect both asthma and CRSwNP control and play a relevant role in patients’ characterization and in treatment selection.
- Information on previous and ongoing treatments (drug for asthma and/or corticosteroids also for nasal symptoms) have to be collected in terms of reason of use, frequency, adherence, inhalation technique (depending on type of therapy) as medical history can often direct care.
- Medical history should always include surgery (number and type of interventions; time from last surgery and time to recurrence).
- Nasal inflammation has to be carefully examined. Cytology and tissue eosinophilia can provide relevant and accurate information on patient condition; the detection of nasal eosinophilic inflammation represents an early marker for identification of a more aggressive inflammatory phenotype in patients with CRSwNP.
- Monoclonal antibodies have been demonstrated to be very useful in the management of chronic eosinophilic diseases such as asthma and are demonstrating effective results also in type-2 inflammatory CRSwNP. The benefit of biological therapies (with the relative clinical improvements) should be evaluated by a careful measurement of the patient’s multidimensionality, therefore not only considering pulmonary or nasal conditions but applying an integrated approach. Likewise, the limits of efficacy of biological therapy might be verified when patients are evaluated with a multidisciplinary collaboration.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, R.R.; Kingdom, T.T.; Smith, T.L.; Bleier, B.; DeConde, A.; Luong, A.U.; Poetker, D.M.; Soler, Z.; Welch, K.C.; Wise, S.K.; et al. International consensus statement on allergy and rhinology: Rhinosinusitis 2021. Int. Forum. Allergy Rhinol. 2021, 11, 213–739. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Han, J.K.; Wagenmann, M.; Hosemann, W.; Lee, S.E.; Backer, V.; Mullol, J.; Gevaert, P.; Klimek, L.; Prokopakis, E.; et al. EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: Definitions and management. J. Allergy Clin. Immunol. 2021, 147, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Massoth, L.; Anderson, C.; McKinney, K.A. Asthma and Chronic Rhinosinusitis: Diagnosis and Medical Management. Med. Sci. 2019, 7, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laidlaw, T.M.; Mullol, J.; Woessner, K.M.; Amin, N.; Mannent, L.P. Chronic rhinosinusitis with nasal polyps and asthma. J. Allergy Clin. Immunol. Pract. 2021, 9, 1133–1141. [Google Scholar] [CrossRef]
- Ramaswamy, U.S.; Patel, V.A.; Lee, S.E. Managing chronic rhinosinusitis in severe asthma. Curr. Opin. Pulm. Med. 2021, 27, 23–28. [Google Scholar] [CrossRef]
- Castagnoli, R.; Licari, A.; Brambilla, I.; Tosca, M.; Ciprandi, G.; Marseglia, G.L. An update on the role of chronic rhinosinusitis with nasal polyps as a co-morbidity in severe asthma. Expert Rev. Respir. Med. 2020, 14, 1197–1205. [Google Scholar] [CrossRef]
- Ramirez, G.A.; Yacoub, M.-R.; Ripa, M.; Mannina, D.; Cariddi, A.; Saporiti, N.; Dagna, L. Eosinophils from physiology to disease: A comprehensive review. Biomed. Res. Int. 2018, 2018, 9095275. [Google Scholar] [CrossRef] [Green Version]
- Passalacqua, G.; Ciprandi, G.; Canonica, G.W. United airways disease: Therapeutic aspects. Thorax 2000, 55, S26–S27. [Google Scholar] [CrossRef] [Green Version]
- Fokkens, W.J.; Lund, V.; Luong, A.U.; Orlandi, R.R. A Comparison of International Guidelines for Rhinosinusitis. J. Allergy Clin. Immunol. Pract. 2022, 10, 1418–1422. [Google Scholar] [CrossRef]
- Jeican, I.I.; Gheban, D.; Barbu-Tudoran, L.; Inișca, P.; Albu, C.; Ilieș, M.; Albu, S.; Vică, M.L.; Matei, H.V.; Tripon, S.; et al. Respiratory Nasal Mucosa in Chronic Rhinosinusitis with Nasal Polyps versus COVID-19: Histopathology, Electron Microscopy Analysis and Assessing of Tissue Interleukin-33. J. Clin. Med. 2021, 10, 4110. [Google Scholar] [CrossRef] [PubMed]
- De Corso, E.; Bellocchi, G.; De Benedetto, M.; Lombardo, N.; Macchi, A.; Malvezzi, L.; Passali, D. Biologics for severe uncontrolled chronic rhinosinusitis with nasal polyps: A change management approach. Consensus of the Joint Committee of Italian Society of Otorhinolaryngology on biologics in rhinology. Acta Otorhinolaryngol. Ital. 2021, 42, 1–16. [Google Scholar] [CrossRef] [PubMed]
- De Corso, E.; Settimi, S.; Tricarico, L.; Mele, D.A.; Mastrapasqua, R.F.; Di Cesare, T.; Galli, J. Predictors of Disease Control After Endoscopic Sinus Surgery Plus Long-Term Local Corticosteroids in CRSwNP. Am. J. Rhinol. Allergy 2021, 35, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.; Asero, R.; Bagnasco, D.; Blasi, F.; Bonini, M.; Bussi, M.; Canevari, R.F.; Canonica, G.W.; Castelnuovo, P.; ARIA Italia; et al. ARIA-ITALY multidisciplinary consensus on nasal polyposis and biological treatments. World Allergy Organ. J. 2021, 14, 100592. [Google Scholar] [CrossRef] [PubMed]
- Xolair (Omalizumab). Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/xolair-epar-product-information_en.pdf (accessed on 27 June 2022).
- Nucala (Mepolizumab). Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/nucala-epar-product-information_en.pdf (accessed on 27 June 2022).
- Cinquaero (Reslizumab). Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/cinqaero-epar-product-information_en.pdf (accessed on 27 June 2022).
- Fasenra (Benralizumab). Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/fasenra-epar-product-information_en.pdf (accessed on 27 June 2022).
- Dupixent (Dupilumab). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761055lbl.pdf (accessed on 27 June 2022).
- Tezspire (Tezepelumab). Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/761224s000lbl.pdf (accessed on 27 June 2022).
- Global Strategy for Asthma Management and Prevention. GINA Report 2021. Available online: https://ginasthma.org/gina-reports/ (accessed on 27 June 2022).
- Fadda, G.L.; Galizia, A.; Galizia, P.; Maugeri, L.; Alati, C.; Cavallo, G. Efficacy and use of benralizumab in patients with eosinophilic chronic rhinosinusitis. Otolaryngol. Case Rep. 2021, 18, 100257. [Google Scholar] [CrossRef]
- Samitas, K.; Zervas, E.; Gaga, M. T2-Low asthma: Current approach to diagnosis and therapy. Curr. Opin. Pulm. Med. 2017, 23, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Kuruvilla, M.E.; Lee, F.E.; Lee, G.B. Understanding Asthma Phenotypes, Endotypes, and Mechanisms of Disease. Clin. Rev. Allergy Immunol. 2019, 56, 219–233. [Google Scholar] [CrossRef]
- Pavlidis, S.; Takahashi, K.; Ng Kee Kwong, F. “T2-high” in severe asthma related to blood eosinophil, exhaled nitric oxide and serum periostin. Eur. Respir. J. 2019, 53, 1800938. [Google Scholar] [CrossRef]
- Menzella, F.; Biava, M.; Bagnasco, D.; Galeone, C.; Simonazzi, A.; Ruggiero, P.; Facciolongo, N. Efficacy and steroid-sparing effect of benralizumab: Has it an advantage over its competitors? Drugs Context 2019, 15, 212580. [Google Scholar] [CrossRef]
- Nakayama, T.; Yoshikawa, M.; Asaka, D.; Okushi, T.; Matsuwaki, Y.; Otori, N.; Moriyama, H. Mucosal eosinophilia and recurrence of nasal polyps—New classification of chronic rhinosinusitis. Rhinology 2011, 49, 392–396. [Google Scholar] [CrossRef]
- Hong, H.; Wang, D.; Tan, K.S.; Zheng, R.; Chen, F.; Gao, W.; Sun, Y. Sinus computed tomography predicts clinical response to corticosteroids in chronic rhinosinusitis with nasal polyps. Clin. Transl. Allergy 2018, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canonica, G.W.; Harrison, T.W.; Chanez, P.; Menzella, F.; Louis, R.; Cosio, B.G.; Garcia Gil, E. Benralizumab improves symptoms of patients with severe, eosinophilic asthma with a diagnosis of nasal polyposis. Allergy 2022, 77, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Varshney, H.; Varshney, J.; Biswas, S.; Ghosh, S.K. Importance of CT Scan of Paranasal Sinuses in the Evaluation of the Anatomical Findings in Patients Suffering from Sinonasal Polyposis. Indian J. Otolaryngol. Head Neck Surg. 2016, 68, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginat, D.T. Posttreatment Imaging of the Paranasal Sinuses Following Endoscopic Sinus Surgery. Neuroimaging Clin. 2015, 25, 653–665. [Google Scholar] [CrossRef]
- Hopkins, C.; Lund, V. Does time from previous surgery predict subsequent treatment failure in Chronic Rhinosinusitis with Nasal Polyps? Rhinology 2021, 59, 277–283. [Google Scholar] [CrossRef]
- Scribano, E.; Ascenti, G.; Cascio, F.; Bellinvia, A.; Mazziotti, S.; Lamberto, S. The role of computed tomography after functional surgery on the paranasal sinuses. Normal findings and an assessment of the surgical failures. Radiol. Med. 1999, 98, 151–156. [Google Scholar]
- Reh, D.D.; Wang, Y.; Ramanathan, M.; Lane, A.P. Treatment-Recalcitrant chronic rhinosinusitis with polyps is associated with altered epithelial cell expression of interleukin-33. Am. J. Rhinol. Allergy 2010, 24, 105–109. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.A.; Orlandi, R.R.; Oakley, G.; Meeks, H.; Curtin, K.; Alt, J.A. Long-Term revision rates for endoscopic sinus surgery. Int. Forum Allergy Rhinol. 2019, 9, 402–408. [Google Scholar] [CrossRef]
- Proimos, E.; Papadakis, C.E.; Chimona, T.S.; Kiagiadaki, D.; Ferekidis, E.; Yiotakis, J. The effect of functional endoscopic sinus surgery on patients with asthma and CRS with nasal polyps. Rhinology 2010, 48, 331–338. [Google Scholar] [CrossRef]
- Wu, P.W.; Lee, T.J.; Wang, C.H.; Huang, C.C.; Chang, P.H.; Fu, C.H.; Huang, C.C. The Role of Surgery in Treating Nasal Obstruction to Control Asthma. J. Asthma Allergy 2020, 13, 625–632. [Google Scholar] [CrossRef]
- Hamada, K.; Oishi, K.; Chikumoto, A.; Murakawa, K.; Ohteru, Y.; Matsuda, K.; Matsunaga, K. Impact of sinus surgery on type 2 airway and systemic inflammation in asthma. J. Asthma 2021, 58, 750–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeican, I.I.; Trombitas, V.; Crivii, C.; Dumitru, M.; Aluaș, M.; Dogaru, G.; Silviu, A.L.B.U. Rehabilitation of patients with chronic rhinosinusitis after functional endoscopic sinus surgery. Balneo PRM Res. J. 2021, 12, 65–72. [Google Scholar] [CrossRef]
- Soler, Z.M.; Jones, R.; Le, P.; Rudmik, L.; Mattos, J.L.; Nguyen, S.A.; Schlosser, R.J. Sino-Nasal outcome test-22 outcomes after sinus surgery: A systematic review and meta-analysis. Laryngoscope 2018, 128, 581–592. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, B.C.P.; Svedsater, H.; Heddini, A.; Nelsen, L.; Balradj, J.S.; Alleman, C. Relationship between the Asthma Control Test (ACT) and other outcomes: A targeted literature review. BMC Pulm. Med. 2020, 20, 79. [Google Scholar] [CrossRef] [Green Version]
- Menzella, F.; Galeone, C.; Ghidoni, G.; Ruggiero, P.; Capobelli, S.; Simonazzi, A.; Facciolongo, N. Successful treatment with benralizumab in a patient with eosinophilic granulomatosis with polyangiitis refractory to mepolizumab. Multidiscip. Respir. Med. 2021, 16, 779. [Google Scholar] [CrossRef] [PubMed]
- Berti, A.; Cornec, D.; Moura, M.C.; Smyth, R.J.; Dagna, L.; Specks, U.; Keogh, K.A. Eosinophilic Granulomatosis with Polyangiitis: Clinical Predictors of Long-Term Asthma Severity. Chest 2020, 157, 1086–1099. [Google Scholar] [CrossRef]
- Novelli, F.; Bacci, E.; Latorre, M.; Seccia, V.; Bartoli, M.L.; Cianchetti, S.; Paggiaro, P. Comorbidities are associated with different features of severe asthma. Clin. Mol. Allergy 2018, 16, 25. [Google Scholar] [CrossRef]
- Calus, L.; Van Bruaene, N.; Bosteels, C.; Dejonckheere, S.; Van Zele, T.; Holtappels, G.; Gevaert, P. Twelve-Year follow-up study after endoscopic sinus surgery in patients with chronic rhinosinusitis with nasal polyposis. Clin. Transl. Allergy 2019, 9, 30. [Google Scholar] [CrossRef] [Green Version]
- Papaioannou, A.I.; Fouka, E.; Papakosta, D.; Papiris, S.; Loukides, S. Switching between biologics in severe asthma patients. When the first choice is not proven to be the best. Clin. Exp. Allergy 2021, 51, 221–227. [Google Scholar] [CrossRef]
- Spadaro, G.; Lagnese, G.; Punziano, A.; Poto, R.; Varricchi, G.; Detoraki, A. The immunology of switching biologics in severe eosinophilic asthma patients. J. Allergy Clin. Immunol. Pract. 2021, 9, 3528–3529. [Google Scholar] [CrossRef]
- Bachert, C.; Sousa, A.R.; Lund, V.J.; Scadding, G.K.; Gevaert, P.; Nasser, S.; Fokkens, W.J. Reduced need for surgery in severe nasal polyposis with mepolizumab: Randomized trial. J. Allergy Clin. Immunol. 2017, 140, 1024–1031.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bachert, C.; Desrosiers, M.Y.; Hellings, P.W.; Laidlaw, T.M. The Role of Biologics in Chronic Rhinosinusitis with Nasal Polyps. J. Allergy Clin. Immunol. Pract. 2021, 9, 1099–1106. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Monoclonal Antibody | Omalizumab [15] | Mepolizumab [16] | Reslizumab [17] | Benralizumab [18] | Dupilumab [19] | Tezepelumab [20] |
|---|---|---|---|---|---|---|
| Target | IgE | IL-5 | IL-5 | IL-5Rα | IL-4Rα, IL-13Rα | TSLP |
| Route of Administration and dosage related to approved indications | Subcutaneous injection every 2–4 weeks dosing and frequency level determined by serum total IgE and body weight. | Subcutaneous injections 100 mg monthly (SA, CRSwNP) 300 mg monthly HES, EGPA) | Intravenous injection 3 mg/kg every 4 weeks | Subcutaneous injection 30 mg once every 4 weeks for the first 3 doses, then subsequently once every 8 weeks | Subcutaneous injection, 400 mg then 200 mg every 2 weeks (AS) 600 mg then 300 mg every 2 weeks AS and OCS or AS and comorbidity (CRSwNP, AD) 600 mg then 300 mg every 2 weeks CRSwNP, AD | Subcutaneous injection 210 mg monthly |
| Currently approved indications | Severe allergic asthma CRSwNP Chronic Idiopathic Urticaria | Severe eosinophilic asthma CRSwNP HES EGPA | Severe eosinophilic asthma | Severe eosinophilic asthma | Severe allergic and eosinophilic asthma CRSwNP Atopic dermatitis EoE (FDA) | Severe asthma (FDA) |
| Other indications under evaluation § | Food allergy | COPD | N/A | CRSwNP EoE HES EGPA COPD EG/EGE NCFB CSU BP Atopic dermatitis | CRSsNP COPD Chronic pruritis Prurigo nodularis BP CSU Chronic inducible cold urticaria Allergic fungal rhinosinusitis Peanut allergy | CRSwNP CSU COPD EoE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seccia, V.; D’Amato, M.; Scioscia, G.; Bagnasco, D.; Di Marco, F.; Fadda, G.; Menzella, F.; Pasquini, E.; Pelaia, G.; Tremante, E.; et al. Management of Patients with Severe Asthma and Chronic Rhinosinusitis with Nasal Polyps: A Multidisciplinary Shared Approach. J. Pers. Med. 2022, 12, 1096. https://doi.org/10.3390/jpm12071096
Seccia V, D’Amato M, Scioscia G, Bagnasco D, Di Marco F, Fadda G, Menzella F, Pasquini E, Pelaia G, Tremante E, et al. Management of Patients with Severe Asthma and Chronic Rhinosinusitis with Nasal Polyps: A Multidisciplinary Shared Approach. Journal of Personalized Medicine. 2022; 12(7):1096. https://doi.org/10.3390/jpm12071096
Chicago/Turabian StyleSeccia, Veronica, Maria D’Amato, Giulia Scioscia, Diego Bagnasco, Fabiano Di Marco, Gianluca Fadda, Francesco Menzella, Ernesto Pasquini, Girolamo Pelaia, Eugenio Tremante, and et al. 2022. "Management of Patients with Severe Asthma and Chronic Rhinosinusitis with Nasal Polyps: A Multidisciplinary Shared Approach" Journal of Personalized Medicine 12, no. 7: 1096. https://doi.org/10.3390/jpm12071096
APA StyleSeccia, V., D’Amato, M., Scioscia, G., Bagnasco, D., Di Marco, F., Fadda, G., Menzella, F., Pasquini, E., Pelaia, G., Tremante, E., De Corso, E., & Bonini, M. (2022). Management of Patients with Severe Asthma and Chronic Rhinosinusitis with Nasal Polyps: A Multidisciplinary Shared Approach. Journal of Personalized Medicine, 12(7), 1096. https://doi.org/10.3390/jpm12071096