
Sex Differences in Patent Ductus Arteriosus Incidence and Response to Pharmacological Treatment in Preterm Infants: A Systematic Review, Meta-Analysis and Meta-Regression



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sources and Search Strategy
2.2. Study Selection and Definitions
2.3. Data Extraction and Assessment of Study Quality
2.4. Statistical Analysis
3. Results
3.1. Description of Studies and Quality Assessment
3.2. Meta-Analysis
3.3. Subgroup Analysis and Meta-Regression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hundscheid, T.; Onland, W.; Van Overmeire, B.; Dijk, P.; van Kaam, A.H.; Dijkman, K.P.; Kooi, E.M.; Villamor, E.; Kroon, A.A.; Visser, R. Early treatment versus expectative management of patent ductus arteriosus in preterm infants: A multicentre, randomised, non-inferiority trial in Europe (BeNeDuctus trial). BMC Pediatrics 2018, 18, 262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reese, J.; Laughon, M.M. The patent ductus arteriosus problem: Infants who still need treatment. J. Pediatrics 2015, 167, 954–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallmon, H.; Koehne, P.; Hansmann, G. Recent advances in the treatment of preterm newborn infants with patent ductus arteriosus. Clin. Perinatol. 2016, 43, 113–129. [Google Scholar] [CrossRef]
- Villamor, E.; Moreno, L.; Mohammed, R.; Pérez-Vizcaíno, F.; Cogolludo, A. Reactive oxygen species as mediators of oxygen signaling during fetal-to-neonatal circulatory transition. Free Radic. Biol. Med. 2019, 142, 82–96. [Google Scholar] [CrossRef]
- Stoller, J.Z.; DeMauro, S.B.; Dagle, J.M.; Reese, J. Current perspectives on pathobiology of the ductus arteriosus. J. Clin. Exp. Cardiol. 2012, 8, S8-001. [Google Scholar] [CrossRef] [Green Version]
- Gillam-Krakauer, M.; Reese, J. Diagnosis and management of patent ductus arteriosus. Neoreviews 2018, 19, e394–e402. [Google Scholar] [CrossRef]
- Hajj, H.; Dagle, J.M. Genetics of patent ductus arteriosus susceptibility and treatment. Semin. Perinatol. 2012, 36, 98–104. [Google Scholar] [CrossRef]
- Schneider, D.J. The patent ductus arteriosus in term infants, children, and adults. Semin. Perinatol. 2012, 36, 146–153. [Google Scholar] [CrossRef] [PubMed]
- de Waal, K.; Prasad, R.; Kluckow, M. Patent ductus arteriosus management and the drift towards therapeutic nihilism–What is the evidence? Semin. Perinatol. 2021, 26, 101219. [Google Scholar] [CrossRef]
- El-Khuffash, A.; Rios, D.R.; McNamara, P.J. Toward a Rational Approach to Patent Ductus Arteriosus Trials: Selecting the Population of Interest. J. Pediatrics 2021, 233, 11–13. [Google Scholar] [CrossRef]
- Putting gender on the agenda. Nature 2010, 465, 665. [CrossRef] [PubMed]
- Kardys, I.; Vliegenthart, R.; Oudkerk, M.; Hofman, A.; Witteman, J.C. The female advantage in cardiovascular disease: Do vascular beds contribute equally? Am. J. Epidemiol. 2007, 166, 403–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Oyen, H.; Nusselder, W.; Jagger, C.; Kolip, P.; Cambois, E.; Robine, J.-M. Gender differences in healthy life years within the EU: An exploration of the “health–survival” paradox. Int. J. Public Health 2013, 58, 143–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Townsend, E.A.; Miller, V.M.; Prakash, Y. Sex differences and sex steroids in lung health and disease. Endocr. Rev. 2012, 33, 1–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, S.-Y.; Cho, S.J.; Kong, K.A.; Park, E.A. Gestational age-specific sex difference in mortality and morbidities of preterm infants: A nationwide study. Sci. Rep. 2017, 7, 6161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, M.A.; Aly, H. Male gender is associated with intraventricular hemorrhage. Pediatrics 2010, 125, e333–e339. [Google Scholar] [CrossRef]
- O’Driscoll, D.N.; McGovern, M.; Greene, C.M.; Molloy, E.J. Gender disparities in preterm neonatal outcomes. Acta Paediatr. 2018, 107, 1494–1499. [Google Scholar] [CrossRef] [Green Version]
- Raju, T.N.; Buist, A.S.; Blaisdell, C.J.; Moxey-Mims, M.; Saigal, S. Adults born preterm: A review of general health and system-specific outcomes. Acta Paediatr. 2017, 106, 1409–1437. [Google Scholar] [CrossRef]
- van Westering-Kroon, E.; Huizing, M.J.; Villamor-Martínez, E.; Villamor, E. Male Disadvantage in Oxidative Stress-Associated Complications of Prematurity: A Systematic Review, Meta-Analysis and Meta-Regression. Antioxidants 2021, 10, 1490. [Google Scholar] [CrossRef]
- Nagasawa, H.; Hamada, C.; Wakabayashi, M.; Nakagawa, Y.; Nomura, S.; Kohno, Y. Time to spontaneous ductus arteriosus closure in full-term neonates. Open Heart 2016, 3, e000413. [Google Scholar] [CrossRef] [Green Version]
- Arena, J.F.P.; Smith, D.W. Sex liability to single structural defects. Am. J. Dis. Child. 1978, 132, 970–972. [Google Scholar] [CrossRef] [PubMed]
- Singham, K.; Wong, H. Patent ductus arteriosus in Malaysia. Aust. N. Z. J. Public Health 1979, 9, 174–176. [Google Scholar] [CrossRef] [PubMed]
- Aubry, P.; Demian, H. Sex differences in congenital heart disease. Ann. Cardiol. Angeiol. 2016, 65, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Sampayo, F.; Pinto, F.F. The sex distribution of congenital cardiopathies. Acta Med. Port. 1994, 7, 413–418. [Google Scholar] [CrossRef]
- Šamánek, M. Boy: Girl ratio in children born with different forms of cardiac malformation: A population-based study. Pediatric Cardiol. 1994, 15, 53–57. [Google Scholar] [CrossRef]
- Liu, C.; Zhu, X.; Li, D.; Shi, Y. Related Factors of Patent Ductus Arteriosus in Preterm Infants: A Systematic Review and Meta-Analysis. Front. Pediatrics 2020, 8, 605879. [Google Scholar] [CrossRef]
- Simon, S.R.; Van Zogchel, L.; Bas-Suárez, M.P.; Cavallaro, G.; Clyman, R.I.; Villamor, E. Platelet counts and patent ductus arteriosus in preterm infants: A systematic review and meta-analysis. Neonatology 2015, 108, 143–151. [Google Scholar] [CrossRef]
- Behbodi, E.; Villamor-Martínez, E.; Degraeuwe, P.L.; Villamor, E. Chorioamnionitis appears not to be a risk factor for patent ductus arteriosus in preterm infants: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 37967. [Google Scholar] [CrossRef] [Green Version]
- Villamor-Martinez, E.; Kilani, M.A.; Degraeuwe, P.L.; Clyman, R.I.; Villamor, E. Intrauterine growth restriction and patent ductus arteriosus in very and extremely preterm infants: A systematic review and meta-analysis. Front. Endocrinol. 2019, 10, 58. [Google Scholar] [CrossRef]
- González-Luis, G.; Ghirardello, S.; Bas-Suárez, P.; Cavallaro, G.; Mosca, F.; Clyman, R.I.; Villamor, E. Platelet counts and patent ductus arteriosus in preterm infants: An updated systematic review and meta-analysis. Front. Pediatrics 2021, 965, 613766. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Adrouche-Amrani, L.; Green, R.S.; Gluck, K.M.; Lin, J. Failure of a repeat course of cyclooxygenase inhibitor to close a PDA is a risk factor for developing chronic lung disease in ELBW infants. BMC Pediatrics 2012, 12, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahamed, M.; Verma, P.; Lee, S.; Vega, M.; Wang, D.; Kim, M.; Fuloria, M. Predictors of successful closure of patent ductus arteriosus with indomethacin. J. Perinatol. 2015, 35, 729. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, E.G.; Samra, N.M.; Amin, S.A.; Borayek, H.A.; Abdelrazek, G. Platelets and platelet derived growth factor and ductus arteriosus in preterm neonates. Prog. Pediatric Cardiol. 2020, 57, 101226. [Google Scholar] [CrossRef]
- Aikio, O.; Harkin, P.; Saarela, T.; Hallman, M. Early paracetamol treatment associated with lowered risk of persistent ductus arteriosus in very preterm infants. J. Matern. Fetal Neonatal Med. 2014, 27, 1252–1256. [Google Scholar] [CrossRef] [PubMed]
- Akar, S.; Topcuoglu, S.; Tuten, A.; Ozalkaya, E.; Karatepe, H.O.; Gokmen, T.; Ovali, F.; Karatekin, G. Is the First Postnatal Platelet Mass as an Indicator of Patent Ductus Arteriosus? Arch. Iran. Med. 2019, 22, 687. [Google Scholar] [PubMed]
- Alan, S.; Karadeniz, C.; Okulu, E.; Kılıc, A.; Erdeve, O.; Ucar, T.; Atasay, B.; Atalay, S.; Arsan, S. Management of patent ductus arteriosus in preterm infants: Clinical judgment might be a fair option. J. Matern. Fetal Neonatal Med. 2013, 26, 1850–1854. [Google Scholar] [CrossRef]
- Asrani, P.; Aly, A.M.; Jiwani, A.K.; Niebuhr, B.R.; Christenson, R.H.; Jain, S.K. High-sensitivity troponin T in preterm infants with a hemodynamically significant patent ductus arteriosus. J. Perinatol. 2018, 38, 1483–1489. [Google Scholar] [CrossRef]
- Antonucci, R.; Cuzzolin, L.; Arceri, A.; Dessì, A.; Fanos, V. Changes in urinary PGE 2 after ibuprofen treatment in preterm infants with patent ductus arteriosus. Eur. J. Clin. Pharmacol. 2009, 65, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Bas-Suárez, M.P.; González-Luis, G.E.; Saavedra, P.; Villamor, E. Platelet counts in the first seven days of life and patent ductus arteriosus in preterm very low-birth-weight infants. Neonatology 2014, 106, 188–194. [Google Scholar] [CrossRef]
- Becerra, G.H.; Bernárdez Zapata, I.; Iglesias Leboreiro, J.; Bahena, E.J.P.; Rendón Macías, M.E. Medical care of children‹ 30 weeks gestation with ductus arteriosus persistent. Rev. Mex. De Pediatría 2013, 80, 131–135. [Google Scholar]
- Bertino, E.; Coscia, A.; Boni, L.; Rossi, C.; Martano, C.; Giuliani, F.; Fabris, C.; Spada, E.; Zolin, A.; Milani, S. Weight growth velocity of very low birth weight infants: Role of gender, gestational age and major morbidities. Early Hum. Dev. 2009, 85, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Boghossian, N.S.; Geraci, M.; Edwards, E.M.; Horbar, J.D. Sex differences in mortality and morbidity of infants born at less than 30 weeks’ gestation. Pediatrics 2018, 142, e20182352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonamy, A.-K.E.; Gudmundsdottir, A.; Maier, R.F.; Toome, L.; Zeitlin, J.; Bonet, M.; Fenton, A.; Hasselager, A.B.; Van Heijst, A.; Gortner, L. Patent ductus arteriosus treatment in very preterm infants: A European population-based cohort study (EPICE) on variation and outcomes. Neonatology 2017, 111, 367–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boo, N.Y.; Mohd-Amin, I.; Bilkis, A.; Yong-Junina, F. Predictors of failed closure of patent ductus arteriosus with indomethacin. Singapore Med. J. 2006, 47, 763. [Google Scholar] [CrossRef] [PubMed]
- Bravo Laguna, M.C. Evaluación del Tratamiento Farmacológico Convencional Para el Cierre del Ductus Arterioso Persistencte en el Recién Nacido Pretérmino: Impacto de Nuevas Líneas Terapéuticas. Ph.D. Thesis, Universidad Autonoma de Madrid, Madrid, Spain, 2011. Available online: https://repositorio.uam.es/bitstream/handle/10486/7350/41683_bravo_laguna_mari_carmen.pdf?sequence=1 (accessed on 15 June 2022).
- Breatnach, C.R.; Franklin, O.; James, A.T.; McCallion, N.; Afif, E.-K. The impact of a hyperdynamic left ventricle on right ventricular function measurements in preterm infants with a patent ductus arteriosus. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F446–F450. [Google Scholar] [CrossRef]
- Breatnach, C.R.; Franklin, O.; McCallion, N.; Afif, E.-K. The effect of a significant patent ductus arteriosus on Doppler flow patterns of preductal vessels: An assessment of the brachiocephalic artery. J. Pediatrics 2017, 180, 279–281.e1. [Google Scholar] [CrossRef]
- Brooks, J.; Travadi, J.; Patole, S.; Doherty, D.; Simmer, K. Is surgical ligation of patent ductus arteriosus necessary? The Western Australian experience of conservative management. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, F235–F239. [Google Scholar] [CrossRef] [Green Version]
- Brunner, B.; Hoeck, M.; Schermer, E.; Streif, W.; Kiechl-Kohlendorfer, U. Patent ductus arteriosus, low platelets, cyclooxygenase inhibitors, and intraventricular hemorrhage in very low birth weight preterm infants. J. Pediatrics 2013, 163, 23–28. [Google Scholar] [CrossRef]
- Buddhe, S.; Dhuper, S.; Kim, R.; Weichbrod, L.; Mahdi, E.; Shah, N.; Kona, S.; Sokal, M. NT-proBNP levels improve the ability of predicting a hemodynamically significant patent ductus arteriosus in very low-birth-weight infants. J. Clin. Neonatol. 2012, 1, 82. [Google Scholar] [CrossRef] [Green Version]
- Cakir, U.; Tayman, C. A mystery of patent ductus arteriosus and serum osmolality in preterm infants. Am. J. Perinatol. 2019, 36, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-L.; Yang, R.-C.; Lee, W.-T.; Lee, P.-L.; Hsu, J.-H.; Wu, J.-R.; Dai, Z.-K. Lung function in very preterm infants with patent ductus arteriosus under conservative management: An observational study. BMC Pediatrics 2015, 15, 167. [Google Scholar] [CrossRef] [PubMed]
- Chessex, P.; Khashu, M.; Harrison, A.; Hosking, M.; Sargent, M.; Lavoie, J.-C. Early life events, sex, and arterial blood pressure in critically ill infants. Pediatric Crit. Care Med. 2010, 11, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Chock, V.Y.; Punn, R.; Oza, A.; Benitz, W.E.; Van Meurs, K.P.; Whittemore, A.S.; Behzadian, F.; Silverman, N.H. Predictors of bronchopulmonary dysplasia or death in premature infants with a patent ductus arteriosus. Pediatric Res. 2014, 75, 570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chock, V.Y.; Ramamoorthy, C.; Van Meurs, K.P. Cerebral oxygenation during different treatment strategies for a patent ductus arteriosus. Neonatology 2011, 100, 233–240. [Google Scholar] [CrossRef]
- Chock, V.Y.; Rose, L.A.; Mante, J.V.; Punn, R. Near-infrared spectroscopy for detection of a significant patent ductus arteriosus. Pediatric Res. 2016, 80, 675. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.M.; Lee, K.H.; Eun, B.L.; Yoo, K.H.; Hong, Y.S.; Son, C.S.; Lee, J.W. Utility of rapid B-type natriuretic peptide assay for diagnosis of symptomatic patent ductus arteriosus in preterm infants. Pediatrics 2005, 115, e255. [Google Scholar] [CrossRef] [Green Version]
- Clyman, R.I.; Hills, N.K. The effect of prolonged tracheal intubation on the association between patent ductus arteriosus and bronchopulmonary dysplasia (grades 2 and 3). J. Perinatol. 2020, 40, 1358–1365. [Google Scholar] [CrossRef]
- Collins, R.T., II; Lyle, R.E.; Rettiganti, M.; Gossett, J.M.; Robbins, J.M.; Casey, P.H. Long-Term Neurodevelopment of Low-Birthweight, Preterm Infants with Patent Ductus Arteriosus. J. Pediatrics 2018, 203, 170–176.e1. [Google Scholar] [CrossRef]
- Coviello, C.; Tataranno, M.L.; Corsini, I.; Leonardi, V.; Longini, M.; Bazzini, F.; Buonocore, G.; Dani, C. Isoprostanes as biomarker for patent ductus arteriosus in preterm infants. Front. Pediatrics 2020, 8, 555. [Google Scholar] [CrossRef]
- Dagle, J.M.; Lepp, N.T.; Cooper, M.E.; Schaa, K.L.; Kelsey, K.J.; Orr, K.L.; Caprau, D.; Zimmerman, C.R.; Steffen, K.M.; Johnson, K.J. Determination of genetic predisposition to patent ductus arteriosus in preterm infants. Pediatrics 2009, 123, 1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagle, J.M.; Ryckman, K.K.; Spracklen, C.N.; Momany, A.M.; Cotten, C.M.; Levy, J.; Page, G.P.; Bell, E.F.; Carlo, W.A.; Shankaran, S. Genetic variants associated with patent ductus arteriosus in extremely preterm infants. J. Perinatol. 2019, 39, 401. [Google Scholar] [CrossRef] [PubMed]
- Dani, C.; Bertini, G.; Corsini, I.; Elia, S.; Vangi, V.; Pratesi, S.; Rubaltelli, F.F. The fate of ductus arteriosus in infants at 23–27 weeks of gestation: From spontaneous closure to ibuprofen resistance. Acta Paediatr. 2008, 97, 1176–1180. [Google Scholar] [CrossRef] [PubMed]
- Demir, N.; Peker, E.; Ece, İ.; Ağengin, K.; Bulan, K.A.; Tuncer, O. Is platelet mass a more significant indicator than platelet count of closure of patent ductus arteriosus? J. Matern. Fetal Neonatal Med. 2016, 29, 1915–1918. [Google Scholar] [CrossRef]
- Derzbach, L.; Treszl, A.; Balogh, Á.; Vásárhelyi, B.; Tulassay, T.; Rigó, J.J. Gender dependent association between perinatal morbidity and estrogen receptor-alpha Pvull polymorphism. J. Perinat Med. 2005, 33, 461–462. [Google Scholar] [CrossRef]
- Dix, L.; Molenschot, M.; Breur, J.; de Vries, W.; Vijlbrief, D.; Groenendaal, F.; Van Bel, F.; Lemmers, P. Cerebral oxygenation and echocardiographic parameters in preterm neonates with a patent ductus arteriosus: An observational study. Arch. Dis. Child. Fetal Neonatal Ed. 2016, 101, F520–F526. [Google Scholar] [CrossRef]
- El-Khuffash, A.F.; Molloy, E.J. Influence of a patent ductus arteriosus on cardiac troponin T levels in preterm infants. J. Pediatrics 2008, 153, 350–353. [Google Scholar] [CrossRef]
- Elsmen, E.; Hansen Pupp, I.; Hellstrom-Westas, L. Preterm male infants need more initial respiratory and circulatory support than female infants. Acta Paediatr. 2004, 93, 529–533. [Google Scholar] [CrossRef]
- Engeseth, M.S.; Engan, M.; Clemm, H.; Vollsæter, M.; Nilsen, R.M.; Markestad, T.; Halvorsen, T.; Røksund, O.D. Voice and Exercise Related Respiratory Symptoms in Extremely Preterm Born Children After Neonatal Patent Ductus Arteriosus. Front. Pediatrics 2020, 8, 150. [Google Scholar] [CrossRef]
- Engür, D.; Kaynak-Türkmen, M.; Deveci, M.; Yenisey, Ç. Platelets and platelet-derived growth factor in closure of the ductus arteriosus. Turk. J. Pediatrics 2015, 57, 242–247. [Google Scholar] [CrossRef]
- Fink, D.; Nitzan, I.; Bin-Nun, A.; Mimouni, F.; Hammerman, C. Ductus arteriosus outcome with focus on the initially patent but hemodynamically insignificant ductus in preterm neonates. J. Perinatol. 2018, 38, 1526. [Google Scholar] [CrossRef] [PubMed]
- Flood, T.; Guthrie, J.D. Echocardiographic markers for the prediction of nonclosure of the patent ductus arteriosus in premature neonates. J. Diagn. Med. Sonogr. 2015, 31, 22–27. [Google Scholar] [CrossRef]
- Furzan, J.A.; Reisch, J.; Tyson, J.E.; Laird, P.; Rosenfeld, C.R. Incidence and risk factors for symptomatic patent ductus arteriosus among inborn very-low-birth-weight infants. Early Hum. Dev. 1985, 12, 39–48. [Google Scholar] [CrossRef]
- Ghirardello, S.; Raffaeli, G.; Crippa, B.L.; Gulden, S.; Amodeo, I.; Consonni, D.; Cavallaro, G.; Schena, F.; Mosca, F. The Thromboelastographic Profile at Birth in Very Preterm Newborns with Patent Ductus Arteriosus. Neonatology 2020, 117, 316–323. [Google Scholar] [CrossRef]
- Godambe, S.; Newby, B.; Shah, V.; Shah, P.S. Effect of indomethacin on closure of ductus arteriosus in very-low-birthweight neonates. Acta Pædiatrica 2006, 95, 1389–1393. [Google Scholar] [CrossRef]
- Gomez-Pomar, E.; Makhoul, M.; Westgate, P.M.; Ibonia, K.T.; Patwardhan, A.; Giannone, P.J.; Bada, H.S.; Jawdeh, E.G.A. Relationship between perfusion index and patent ductus arteriosus in preterm infants. Pediatric Res. 2017, 81, 775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goudjil, S.; Imestouren, F.; Chazal, C.; Ghostine, G.; Wallois, F.; Leke, A.; Kongolo, G. Patent ductus arteriosus in preterm infants is associated with cardiac autonomic alteration and predominant parasympathetic stimulation. Early Hum. Dev. 2013, 89, 631–634. [Google Scholar] [CrossRef]
- Griesmaier, E.; Santuari, E.; Edlinger, M.; Neubauer, V.; Waltner-Romen, M.; Kiechl-Kohlendorfer, U. Differences in the maturation of amplitude-integrated EEG signals in male and female preterm infants. Neonatology 2014, 105, 175–181. [Google Scholar] [CrossRef]
- Grosfeld, J.L.; Chaet, M.; Molinari, F.; Engle, W.; Engum, S.A.; West, K.W.; Rescorla, F.J.; Scherer, L., III. Increased risk of necrotizing enterocolitis in premature infants with patent ductus arteriosus treated with indomethacin. Ann. Surg. 1996, 224, 350. [Google Scholar] [CrossRef]
- Halil, H.; Buyuktiryaki, M.; Atay, F.Y.; Yekta Oncel, M.; Uras, N. Reopening of the ductus arteriosus in preterm infants; Clinical aspects and subsequent consequences. J. Neonatal-Perinat. Med. 2018, 11, 273–279. [Google Scholar] [CrossRef]
- Halliday, H.; Hirata, T.; Brady, J. Indomethacin therapy for large patent ductus arteriosus in the very low birth weight infant: Results and complications. Pediatrics 1979, 64, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Hammoud, M.S.; Elsori, H.A.; Hanafi, E.A.; Shalabi, A.A.; Fouda, I.A.; Devarajan, L.V. Incidence and risk factors associated with the patency of ductus arteriosus in preterm infants with respiratory distress syndrome in Kuwait. Saudi Med. J. 2003, 24, 982–985. [Google Scholar] [PubMed]
- Härkin, P.; Härmä, A.; Aikio, O.; Valkama, M.; Leskinen, M.; Saarela, T.; Hallman, M. Paracetamol accelerates closure of the ductus arteriosus after premature birth: A randomized trial. J. Pediatrics 2016, 177, 72–77.e72. [Google Scholar] [CrossRef]
- Härkin, P.; Marttila, R.; Pokka, T.; Saarela, T.; Hallman, M. Morbidities associated with patent ductus arteriosus in preterm infants. Nationwide cohort study. J. Matern. Fetal Neonatal Med. 2018, 31, 2576–2583. [Google Scholar] [CrossRef] [PubMed]
- Harris, C.; Zivanovic, S.; Lunt, A.; Calvert, S.; Bisquera, A.; Marlow, N.; Peacock, J.L.; Greenough, A. Lung function and respiratory outcomes in teenage boys and girls born very prematurely. Pediatric Pulmonol. 2020, 55, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Harris, S.L.; More, K.; Dixon, B.; Troughton, R.; Pemberton, C.; Horwood, J.; Ellis, N.; Austin, N. Factors affecting N-terminal pro-B-type natriuretic peptide levels in preterm infants and use in determination of haemodynamic significance of patent ductus arteriosus. Eur. J. Pediatrics 2018, 177, 521–532. [Google Scholar] [CrossRef]
- Hintz, S.R.; Kendrick, D.E.; Vohr, B.R.; Poole, W.K.; Higgins, R.D.; Network, N.N.R. Gender differences in neurodevelopmental outcomes among extremely preterm, extremely-low-birthweight infants. Acta Paediatr. 2006, 95, 1239–1248. [Google Scholar] [CrossRef]
- Hoodbhoy, S.A.; Cutting, H.A.; Seddon, J.A.; Campbell, M.E. Cerebral and splanchnic hemodynamics after duct ligation in very low birth weight infants. J. Pediatrics 2009, 154, 196–200.e192. [Google Scholar] [CrossRef]
- Hsu, J.-H.; Yang, S.-N.; Chen, H.-L.; Tseng, H.-I.; Dai, Z.-K.; Wu, J.-R. B-type natriuretic peptide predicts responses to indomethacin in premature neonates with patent ductus arteriosus. J. Pediatrics 2010, 157, 79–84. [Google Scholar] [CrossRef]
- Hsu, K.-H.; Wu, T.-W.; Wu, I.-H.; Lai, M.-Y.; Hsu, S.-Y.; Huang, H.-W.; Mok, T.-Y.; Lee, C.-C.; Lien, R. Baseline cardiac output and its alterations during ibuprofen treatment for patent ductus arteriosus in preterm infants. BMC Pediatrics 2019, 19, 179. [Google Scholar] [CrossRef] [Green Version]
- Inayat, M.; Bany-Mohammed, F.; Valencia, A.; Tay, C.; Jacinto, J.; Aranda, J.V.; Beharry, K.D. Antioxidants and biomarkers of oxidative stress in preterm infants with symptomatic patent ductus arteriosus. Am. J. Perinatol. 2015, 32, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Isayama, T.; Mirea, L.; Mori, R.; Kusuda, S.; Fujimura, M.; Lee, S.K.; Shah, P.S.; Neonatal Research Network of Japan; Canadian Neonatal Network. Patent ductus arteriosus management and outcomes in Japan and Canada: Comparison of proactive and selective approaches. Am. J. Perinatol. 2015, 32, 1087–1094. [Google Scholar] [CrossRef] [PubMed]
- Ito, M.; Tamura, M.; Namba, F. Neonatal Research Network of Japan. Role of sex in morbidity and mortality of very premature neonates. Pediatrics Int. 2017, 59, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Janz-Robinson, E.M.; Badawi, N.; Walker, K.; Bajuk, B.; Abdel-Latif, M.E.; Bowen, J.; Sedgley, S.; Carlisle, H.; Smith, J.; Craven, P. Neurodevelopmental outcomes of premature infants treated for patent ductus arteriosus: A population-based cohort study. J. Pediatrics 2015, 167, 1025–1032.e1023. [Google Scholar] [CrossRef]
- Jennische, M.; Sedin, G. Gender differences in outcome after neonatal intensive care: Speech and language skills are less influenced in boys than in girls at 6.5 years. Acta Paediatr. 2003, 92, 364–378. [Google Scholar] [CrossRef]
- Jhaveri, N.; Moon-Grady, A.; Clyman, R.I. Early surgical ligation versus a conservative approach for management of patent ductus arteriosus that fails to close after indomethacin treatment. J. Pediatrics 2010, 157, 381–387.e381. [Google Scholar] [CrossRef] [Green Version]
- Jim, W.-T.; Chiu, N.-C.; Chen, M.-R.; Hung, H.-Y.; Kao, H.-A.; Hsu, C.-H.; Chang, J.-H. Cerebral hemodynamic change and intraventricular hemorrhage in very low birth weight infants with patent ductus arteriosus. Ultrasound Med. Biol. 2005, 31, 197–202. [Google Scholar] [CrossRef]
- Jones, H.P.; Karuri, S.; Cronin, C.M.; Ohlsson, A.; Peliowski, A.; Synnes, A.; Lee, S.K. Actuarial survival of a large Canadian cohort of preterm infants. BMC Pediatrics 2005, 5, 40. [Google Scholar] [CrossRef] [Green Version]
- Juujärvi, S.; Saarela, T.; Hallman, M.; Aikio, O. Intravenous paracetamol was associated with closure of the ductus arteriosus in extremely premature infants. Acta Paediatr. 2018, 107, 605–610. [Google Scholar] [CrossRef]
- Kahvecioglu, D.; Erdeve, O.; Akduman, H.; Ucar, T.; Alan, S.; Çakır, U.; Yıldız, D.; Atasay, B.; Arsan, S.; Atalay, S. Influence of platelet count, platelet mass index, and platelet function on the spontaneous closure of ductus arteriosus in the prematurity. Pediatrics Neonatol. 2018, 59, 53–57. [Google Scholar] [CrossRef] [Green Version]
- Kara, M.; Bilen, M.M.; Tekgündüz, K.Ş.; Laloğlu, F.; Ceviz, N. Relation of shunt index with the patent ductus arteriosus among preterm infants under 30 weeks or 1500 g. J. Matern. Fetal Neonatal Med. 2019, 33, 4016–4021. [Google Scholar] [CrossRef] [PubMed]
- Karabulut, B.; Arcagök, B.C.; Simsek, A. Utility of the Platelet-to-Lymphocyte Ratio in Diagnosing and Predicting Treatment Success in Preterm Neonates with Patent Ductus Arteriosus. Fetal Pediatric Pathol. 2019, 40, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Katheria, V.; Poeltler, D.; Brown, M.; Hassen, K.; Patel, D.; Rich, W.; Finer, N.; Katheria, A. Early prediction of a significant patent ductus arteriosus in infants <32 weeks gestational age. J. Neonatal-Perinat. Med. 2018, 11, 265–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, S.; Stritzke, A.; Soraisham, A.S. Does Postmenstrual Age Affect Medical Patent Ductus Arteriosus Treatment Success in Preterm Infants? Am. J. Perinatol. 2019, 36, 1504–1509. [Google Scholar] [CrossRef]
- Kazanci, E.G.; Buyuktiryaki, M.; Unsal, H.; Tayman, C. Useful platelet indices for the diagnosis and follow-up of patent ductus arteriosus. Am. J. Perinatol. 2019, 36, 1521–1527. [Google Scholar] [CrossRef]
- Kent, A.L.; Wright, I.M.; Abdel-Latif, M.E. Mortality and adverse neurologic outcomes are greater in preterm male infants. Pediatrics 2012, 129, 124. [Google Scholar] [CrossRef]
- Kim, E.S.; Kim, E.-K.; Choi, C.W.; Kim, H.-S.; Kim, B.I.; Choi, J.-H.; Park, J.S.; Moon, K.C. Intrauterine inflammation as a risk factor for persistent ductus arteriosus patency after cyclooxygenase inhibition in extremely low birth weight infants. J. Pediatrics 2010, 157, 745–750.e741. [Google Scholar] [CrossRef]
- Kim, J.S.; Shim, E.J. B-type natriuretic Peptide assay for the diagnosis and prognosis of patent ductus arteriosus in preterm infants. Korean Circ. J. 2012, 42, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Kwinta, P.; Rudzinski, A.; Kruczek, P.; Kordon, Z.; Pietrzyk, J.J. Can early echocardiographic findings predict patent ductus arteriosus? Neonatology 2009, 95, 141–148. [Google Scholar] [CrossRef]
- Laughon, M.; Bose, C.; Clark, R. Treatment strategies to prevent or close a patent ductus arteriosus in preterm infants and outcomes. J. Perinatol. 2007, 27, 164. [Google Scholar] [CrossRef] [Green Version]
- Lauterbach, M.D.; Raz, S.; Sander, C.J. Neonatal hypoxic risk in preterm birth infants: The influence of sex and severity of respiratory distress on cognitive recovery. Neuropsychology 2001, 15, 411. [Google Scholar] [CrossRef] [PubMed]
- Ledo, A.; Aguar, M.; Núñez-Ramiro, A.; Saénz, P.; Vento, M. Abdominal near-infrared spectroscopy detects low mesenteric perfusion early in preterm infants with hemodynamic significant ductus arteriosus. Neonatology 2017, 112, 238–245. [Google Scholar] [CrossRef]
- Leonhardt, A.; Isken, V.; Kühl, P.; Seyberth, H. Prolonged indomethacin treatment in preterm infants with symptomatic patent ductus arteriosus: Efficacy, drug level monitoring, and patient selection. Eur. J. Pediatrics 1987, 146, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Letshwiti, J.B.; Sirc, J.; O’Kelly, R.; Miletin, J. Serial N-terminal pro-brain natriuretic peptide measurement as a predictor of significant patent ductus arteriosus in preterm infants beyond the first week of life. Eur. J. Pediatrics 2014, 173, 1491–1496. [Google Scholar] [CrossRef]
- Li, D.; Rosito, G.; Slagle, T. Probiotics for the prevention of necrotizing enterocolitis in neonates: An 8-year retrospective cohort study. J. Clin. Pharm. Ther. 2013, 38, 445–449. [Google Scholar] [CrossRef]
- Louis, D.; Wong, C.; Ye, X.Y.; McNamara, P.J.; Jain, A. Factors associated with non-response to second course indomethacin for PDA treatment in preterm neonates. J. Matern. Fetal Neonatal Med. 2018, 31, 1407–1411. [Google Scholar] [CrossRef]
- Madan, J.; Fiascone, J.; Balasubramanian, V.; Griffith, J.; Hagadorn, J.I. Predictors of ductal closure and intestinal complications in very low birth weight infants treated with indomethacin. Neonatology 2008, 94, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Madan, J.C.; Kendrick, D.; Hagadorn, J.I.; Frantz III, I.D.; Health, N.I.o.C.; Network, H.D.N.R. Patent ductus arteriosus therapy: Impact on neonatal and 18-month outcome. Pediatrics 2009, 123, 674. [Google Scholar] [CrossRef] [Green Version]
- Martin, C.G.; Snider, A.R.; Katz, S.M.; Peabody, J.L.; Brady, J.P. Abnormal cerebral blood flow patterns in preterm infants with a large patent ductus arteriosus. J. Pediatrics 1982, 101, 587–593. [Google Scholar] [CrossRef]
- Meinarde, L.; Hillman, M.; Rizzotti, A.; Basquiera, A.L.; Tabares, A.; Cuestas, E. C-reactive protein, platelets, and patent ductus arteriosus. Platelets 2016, 27, 821–823. [Google Scholar] [CrossRef]
- Mellander, M.; Leheup, B.; Lindstrom, D.P.; Palme, C.; Graham Jr, T.P.; Stahlman, M.T.; Cotton, R.B. Recurrence of symptomatic patent ductus arteriosus in extremely premature infants, treated with indomethacin. J. Pediatrics 1984, 105, 138–143. [Google Scholar] [CrossRef]
- Mine, K.; Ohashi, A.; Tsuji, S.; Nakashima, J.; Hirabayashi, M.; Kaneko, K. B-type natriuretic peptide for assessment of haemodynamically significant patent ductus arteriosus in premature infants. Acta Paediatr. 2013, 102, e347–e352. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, G.; Shankaran, S.; McDonald, S.A.; Das, A.; Ehrenkranz, R.A.; Goldberg, R.N.; Stoll, B.J.; Tyson, J.E.; Higgins, R.D.; Schendel, D. Association Between Blood Spot Transforming Growth Factor-β and Patent Ductus Arteriosus in Extremely Low-Birth Weight Infants. Pediatric Cardiol. 2013, 34, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemerofsky, S.L.; Parravicini, E.; Bateman, D.; Kleinman, C.; Polin, R.A.; Lorenz, J.M. The ductus arteriosus rarely requires treatment in infants >1000 grams. Am. J. Perinatol. 2008, 25, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, V.; Griesmaier, E.; Ralser, E.; Kiechl-Kohlendorfer, U. The effect of sex on outcome of preterm infants—A population-based survey. Acta Paediatr. 2012, 101, 906–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nizarali, Z.; Marques, T.; Costa, C.; Barroso, R.; Cunha, M. Patent Ductus Arteriosus: Perinatal Risk Factors. J. Neonatal Biol. 2012, 1, 109. [Google Scholar] [CrossRef] [Green Version]
- Nuntnarumit, P.; Khositseth, A.; Thanomsingh, P. N-terminal probrain natriuretic peptide and patent ductus arteriosus in preterm infants. J. Perinatol. 2009, 29, 137. [Google Scholar] [CrossRef] [Green Version]
- O’Rourke, D.J.; El-Khuffash, A.; Moody, C.; Walsh, K.; Molloy, E.J. Patent ductus arteriosus evaluation by serial echocardiography in preterm infants. Acta Paediatr. 2008, 97, 574–578. [Google Scholar] [CrossRef]
- Oh, S.H.; Lee, B.S.; Jung, E.; Oh, M.Y.; Do, H.-J.; Kim, E.A.-R.; Kim, K.-S. Plasma B-type natriuretic peptide cannot predict treatment response to ibuprofen in preterm infants with patent ductus arteriosus. Sci. Rep. 2020, 10, 4430. [Google Scholar] [CrossRef]
- Okur, N.; Tayman, C.; Büyüktiryaki, M.; Kadıoğlu Şimşek, G.; Ozer Bekmez, B.; Altuğ, N. Can lactate levels be used as a marker of patent ductus arteriosus in preterm babies? J. Clin. Lab. Anal. 2019, 33, e22664. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, A.; Soares, P.; Flor-de-Lima, F.; Neves, A.L.S.; Guimarães, H.l. PDA management in VLBW infants: Experience of a level III NICU. J. Pediatric Neonatal Individ. Med. 2016, 5, e050227. [Google Scholar]
- Olsson, K.W.; Jonzon, A.; Sindelar, R. Early haemodynamically significant patent ductus arteriosus does not predict future persistence in extremely preterm infants. Acta Paediatr. 2019, 108, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Olsson, K.W.; Larsson, A.; Jonzon, A.; Sindelar, R. Exploration of potential biochemical markers for persistence of patent ductus arteriosus in preterm infants at 22–27 weeks’ gestation. Pediatric Res. 2018, 86, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Olukman, O.; Ozdemir, R.; Karadeniz, C.; Calkavur, S.; Mese, T.; Vergin, C. Is there a relationship between platelet parameters and patency of ductus arteriosus in preterm infants? Blood Coagul. Fibrinolysis 2017, 28, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Bekmez, B.O.; Tayman, C.; Buyuktiryaki, M.; Cetinkaya, A.K.; Cakir, U.; Derme, T. A promising, novel index in the diagnosis and follow-up of patent ductus arteriosus: Red cell distribution width-to-platelet ratio. J. Clin. Lab. Anal. 2018, 32, e22616. [Google Scholar] [CrossRef] [Green Version]
- Patole, S.K.; Kumaran, V.; Travadi, J.N.; Brooks, J.M.; Doherty, D.A. Does patent ductus arteriosus affect feed tolerance in preterm neonates? Arch. Dis. Child. Fetal Neonatal Ed. 2007, 92, F53–F55. [Google Scholar] [CrossRef] [Green Version]
- Peacock, J.L.; Marston, L.; Marlow, N.; Calvert, S.A.; Greenough, A. Neonatal and infant outcome in boys and girls born very prematurely. Pediatric Res. 2012, 71, 305. [Google Scholar] [CrossRef] [Green Version]
- Pees, C.; Walch, E.; Obladen, M.; Koehne, P. Echocardiography predicts closure of patent ductus arteriosus in response to ibuprofen in infants less than 28 week gestational age. Early Hum. Dev. 2010, 86, 503–508. [Google Scholar] [CrossRef]
- Pereira, S.S.; Kempley, S.T.; Shah, D.K.; Morris, J.K.; Sinha, A.K. Early echocardiography does not predict subsequent treatment of symptomatic patent ductus arteriosus in extremely preterm infants. Acta Paediatr. 2018, 107, 1909–1916. [Google Scholar] [CrossRef]
- Polat, T.B.; Celik, I.H.; Erdeve, O. Early predictive echocardiographic features of hemodynamically significant patent ductus arteriosus in preterm VLBW infants. Pediatrics Int. 2016, 58, 589–594. [Google Scholar] [CrossRef]
- Pourarian, S.; Farahbakhsh, N.; Sharma, D.; Cheriki, S.; Bijanzadeh, F. Prevalence and risk factors associated with the patency of ductus arteriosus in premature neonates: A prospective observational study from Iran. J. Matern. Fetal Neonatal Med. 2017, 30, 1460–1464. [Google Scholar] [CrossRef] [PubMed]
- Reller, M.D.; Lorenz, J.M.; Kotagal, U.R.; Meyer, R.A.; Kaplan, S. Hemodynamically significant PDA: An echocardiographic and clinical assessment of incidence, natural history, and outcome in very low birth weight infants maintained in negative fluid balance. Pediatric Cardiol. 1985, 6, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Blanco, S.; Oulego-Erroz, I.; Gautreaux-Minaya, S.; Perez-Muñuzuri, A.; Couce-Pico, M.L. Early NT-proBNP levels as a screening tool for the detection of hemodynamically significant patent ductus arteriosus during the first week of life in very low birth weight infants. J. Perinatol. 2018, 38, 881. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, V.; Pedini, A.; Santoni, M.; Scutti, G.; Colaneri, M.; Pozzi, M.; Cogo, P.E.; Carnielli, V.P. Patent ductus arteriosus in preterm infants born before 30 weeks’ gestation: High rate of spontaneous closure after hospital discharge. Cardiol. Young 2018, 28, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Rooney, S.R.; Shelton, E.L.; Aka, I.; Shaffer, C.M.; Clyman, R.I.; Dagle, J.M.; Ryckman, K.; Lewis, T.R.; Reese, J.; Van Driest, S.L. CYP2C9* 2 is associated with indomethacin treatment failure for patent ductus arteriosus. Pharmacogenomics 2019, 20, 939–946. [Google Scholar] [CrossRef]
- Sadeck, L.S.; Leone, C.R.; Procianoy, R.S.; Guinsburg, R.; Marba, S.; Martinez, F.E.; Rugolo, L.M.; Moreira, M.E.L.; Fiori, R.M.; Ferrari, L.L. Effects of therapeutic approach on the neonatal evolution of very low birth weight infants with patent ductus arteriosus. J. Pediatr. 2014, 90, 616–623. [Google Scholar] [CrossRef] [Green Version]
- Sallmon, H.; Weber, S.C.; Dirks, J.; Schiffer, T.; Klippstein, T.; Stein, A.; Felderhoff-Müser, U.; Metze, B.; Hansmann, G.; Bührer, C. Association between platelet counts before and during pharmacological therapy for patent ductus arteriosus and treatment failure in preterm infants. Front. Pediatrics 2018, 6, 41. [Google Scholar] [CrossRef]
- Sallmon, H.; Weber, S.C.; Huning, B.; Stein, A.; Horn, P.A.; Metze, B.C.; Dame, C.; Buhrer, C.; Felderhoff-Muser, U.; Hansmann, G.; et al. Thrombocytopenia in the first 24 hours after birth and incidence of patent ductus arteriosus. Pediatrics 2012, 130, e623–e630. [Google Scholar] [CrossRef] [Green Version]
- Sanjeev, S.; Pettersen, M.; Lua, J.; Thomas, R.; Shankaran, S.; L’Ecuyer, T. Role of plasma B-type natriuretic peptide in screening for hemodynamically significant patent ductus arteriosus in preterm neonates. J. Perinatol. 2005, 25, 709–713. [Google Scholar] [CrossRef]
- Schwarz, C.E.; Preusche, A.; Wolf, M.; Poets, C.F.; Franz, A.R. Prospective observational study on assessing the hemodynamic relevance of patent ductus arteriosus with frequency domain near-infrared spectroscopy. BMC Pediatrics 2018, 18, 66. [Google Scholar] [CrossRef] [Green Version]
- Sellmer, A.; Bjerre, J.V.; Schmidt, M.R.; McNamara, P.J.; Hjortdal, V.E.; Høst, B.; Bech, B.H.; Henriksen, T.B. Morbidity and mortality in preterm neonates with patent ductus arteriosus on day 3. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F505–F510. [Google Scholar] [CrossRef]
- Semberova, J.; Sirc, J.; Miletin, J.; Kucera, J.; Berka, I.; Sebkova, S.; O’Sullivan, S.; Franklin, O.; Stranak, Z. Spontaneous closure of patent ductus arteriosus in infants ≤1500 g. Pediatrics 2017, 140, e20164258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seon, H.-S.; Lee, J.-B.; Kim, I.-U.; Kim, S.-H.; Lee, J.-H.; Kim, D.-H.; Kim, H.-S. Association with ductus arteriosus closure by ibuprofen and intrauterine inflammation in very low birth weight infants. Korean J. Perinatol. 2013, 24, 158–167. [Google Scholar] [CrossRef] [Green Version]
- Shah, N.A.; Hills, N.K.; Waleh, N.; McCurnin, D.; Seidner, S.; Chemtob, S.; Clyman, R. Relationship between circulating platelet counts and ductus arteriosus patency after indomethacin treatment. J. Pediatrics 2011, 158, 919–923.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skiöld, B.; Alexandrou, G.; Padilla, N.; Blennow, M.; Vollmer, B.; Ådén, U. Sex differences in outcome and associations with neonatal brain morphology in extremely preterm children. J. Pediatrics 2014, 164, 1012–1018. [Google Scholar] [CrossRef] [PubMed]
- Stark, M.J.; Hodyl, N.A.; Wright, I.M.; Clifton, V. The influence of sex and antenatal betamethasone exposure on vasoconstrictors and the preterm microvasculature. J. Matern. Fetal Neonatal Med. 2011, 24, 1215–1220. [Google Scholar] [CrossRef]
- Steiner, M.; Salzer-Muhar, U.; Swoboda, V.; Unterasinger, L.; Baumgartner, S.; Waldhoer, T.; Langgartner, M.; Klebermass-Schrehof, K.; Berger, A. Preterm infants who later require duct ligation show different vital signs and pH in early postnatal life. Acta Paediatr. 2015, 104, e7–e13. [Google Scholar] [CrossRef]
- Stevenson, D.K.; Verter, J.; Fanaroff, A.A.; Oh, W.; Ehrenkranz, R.A.; Shankaran, S.; Donovan, E.F.; Wright, L.L.; Lemons, J.A.; Tyson, J.E. Sex differences in outcomes of very low birthweight infants: The newborn male disadvantage. Arch. Dis. Child. Fetal Neonatal Ed. 2000, 83, F182–F185. [Google Scholar] [CrossRef] [Green Version]
- Strauss, T.; Pessach, I.; Jacoby, E.; Schushan-Eisen, I.; Mazkereth, R.; Kuint, J. Carina angle measurements for diagnosis of patent ductus arteriosus in preterm infants. Neonatology 2011, 99, 224–230. [Google Scholar] [CrossRef]
- Tauber, K.; Granina, E.; Doyle, R.; Munshi, U. Gestational and postnatal age influence B-type natriuretic peptide level used in diagnosis of a hemodynamically significant patent ductus arteriosus in preterm infants. J. Clin. Neonatol. 2016, 5, 143–149. [Google Scholar] [CrossRef]
- Terek, D.; Yalaz, M.; Ulger, Z.; Koroglu, O.A.; Kultursay, N. Medical closure of patent ductus arteriosus does not reduce mortality and development of bronchopulmonary dysplasia in preterm infants. J. Res. Med. Sci. 2014, 19, 1074. [Google Scholar] [CrossRef] [PubMed]
- Tioseco, J.A.; Aly, H.; Essers, J.; Patel, K.; El-Mohandes, A.A. Male sex and intraventricular hemorrhage. Pediatric Crit. Care Med. 2006, 7, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, A.; Nagasawa, H.; Yamamoto, Y.; Tatebayashi, K.; Suzuki, H.; Yamada, K.; Arai, M.; Kohno, Y. Clinical aspects of very-low-birthweight infants showing reopening of ductus arteriosus. Pediatrics Int. 2011, 53, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, R.; Knee, A.; Paris, Y.; Singh, R. Predictors of successful patent ductus arteriosus closure with acetaminophen in preterm infants. J. Perinatol. 2021, 41, 998–1006. [Google Scholar] [CrossRef]
- van de Bor, M.; Verloove-Vanhorick, S.P.; Brand, R.; Ruys, J.H. Patent ductus arteriosus in a cohort of 1338 preterm infants: A collaborative study. Paediatr. Perinat. Epidemiol. 1988, 2, 328–336. [Google Scholar] [CrossRef]
- Velazquez, D.M.; Reidy, K.J.; Sharma, M.; Kim, M.; Vega, M.; Havranek, T. The effect of hemodynamically significant patent ductus arteriosus on acute kidney injury and systemic hypertension in extremely low gestational age newborns. J. Matern. Fetal Neonatal Med. 2018, 32, 3209–3214. [Google Scholar] [CrossRef]
- Vieux, R.; Desandes, R.; Boubred, F.; Semama, D.; Guillemin, F.; Buchweiller, M.-C.; Fresson, J.; Hascoet, J.-M. Ibuprofen in very preterm infants impairs renal function for the first month of life. Pediatric Nephrol. 2010, 25, 267–274. [Google Scholar] [CrossRef]
- Visconti, L.F.; Morhy, S.S.; Deutsch, A.D.; Tavares, G.M.; Wilberg, T.J.; Rossi Fde, S. Clinical and echocardiographic characteristics associated with the evolution of the ductus arteriosus in the neonate with birth weight lower than 1500 g. Einstein 2013, 11, 317–323. [Google Scholar] [CrossRef]
- Weiss, H.; Cooper, B.; Brook, M.; Schlueter, M.; Clyman, R. Factors determining reopening of the ductus arteriosus after successful clinical closure with indomethacin. J. Pediatrics 1995, 127, 466–471. [Google Scholar] [CrossRef]
- Weisz, D.E.; Mirea, L.; Rosenberg, E.; Jang, M.; Ly, L.; Church, P.T.; Kelly, E.; Kim, S.J.; Jain, A.; McNamara, P.J. Association of patent ductus arteriosus ligation with death or neurodevelopmental impairment among extremely preterm infants. JAMA Pediatrics 2017, 171, 443–449. [Google Scholar] [CrossRef]
- Yang, C.-Z.; Lee, J. Factors affecting successful closure of hemodynamically significant patent ductus arteriosus with indomethacin in extremely low birth weight infants. World J. Clin. Pediatrics 2008, 4, 91–96. [Google Scholar] [CrossRef]
- Yoon, M.J.; Yoon, H.S.; Chung, S.H.; Han, M.Y.; Bae, C.W. The factors associated with the efficacy of indomethacin treatment in premature infants with patent ductus arteriosus. Korean J. Pediatrics 2007, 50, 531–535. [Google Scholar] [CrossRef]
- Yum, S.K.; Moon, C.-J.; Youn, Y.-A.; Lee, J.Y.; Sung, I.K. Echocardiographic assessment of patent ductus arteriosus in very low birthweight infants over time: Prospective observational study. J. Matern. Fetal Neonatal Med. 2018, 31, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Zanardo, V.; Vedovato, S.; Chiozza, L.; Faggian, D.; Favaro, F.; Trevisanuto, D. Pharmacological closure of patent ductus arteriosus: Effects on pulse pressure and on endothelin-1 and vasopressin excretion. Am. J. Perinatol. 2008, 25, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Zisk, J.L.; Genen, L.H.; Kirkby, S.; Webb, D.; Greenspan, J.; Dysart, K. Do premature female infants really do better than their male counterparts? Am. J. Perinatol. 2011, 28, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Zozaya, C.; Avila-Alvarez, A.; Arruza, L.; Rodrigo, F.G.-M.; Fernandez-Perez, C.; Castro, A.; Cuesta, M.T.; Vacas, B.; Couce, M.L.; Torres, M.V. The effect of morbidity and sex on postnatal growth of very preterm infants: A multicenter cohort study. Neonatology 2019, 115, 348–354. [Google Scholar] [CrossRef]
- Clyman, R.I. Patent ductus arteriosus, its treatments, and the risks of pulmonary morbidity. Semin. Perinatol. 2018, 42, 235–242. [Google Scholar] [CrossRef]
- Clyman, R.I.; Kaempf, J.; Liebowitz, M.; Erdeve, O.; Bulbul, A.; Håkansson, S.; Lindqvist, J.; Farooqi, A.; Katheria, A.; Sauberan, J. Prolonged tracheal intubation and the association between patent ductus arteriosus and bronchopulmonary dysplasia: A secondary analysis of the PDA-TOLERATE trial. J. Pediatrics 2021, 229, 283–288.e282. [Google Scholar] [CrossRef]
- Drevenstedt, G.L.; Crimmins, E.M.; Vasunilashorn, S.; Finch, C.E. The rise and fall of excess male infant mortality. Proc. Natl. Acad. Sci. USA 2008, 105, 5016–5021. [Google Scholar] [CrossRef] [Green Version]
- Flinsenberg, T.W.; Van der Sterren, S.; van Cleef, A.N.; Schuurman, M.J.; Ågren, P.; Villamor, E. Effects of sex and estrogen on chicken ductus arteriosus reactivity. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2010, 298, R1217–R1224. [Google Scholar] [CrossRef] [Green Version]
- Bruggeman, V.; Van As, P.; Decuypere, E. Developmental endocrinology of the reproductive axis in the chicken embryo. Comp. Biochem. Physiol. Part A Mol. Integr. Physiol. 2002, 131, 839–846. [Google Scholar] [CrossRef]
- Waxman, D.J.; Holloway, M.G. Sex differences in the expression of hepatic drug metabolizing enzymes. Mol. Pharmacol. 2009, 76, 215–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madla, C.M.; Gavins, F.K.; Merchant, H.A.; Orlu, M.; Murdan, S.; Basit, A.W. Let’s talk about sex: Differences in drug therapy in males and females. Adv. Drug Deliv. Rev. 2021, 175, 113804. [Google Scholar] [CrossRef] [PubMed]
- Franconi, F.; Campesi, I. Pharmacogenomics, pharmacokinetics and pharmacodynamics: Interaction with biological differences between men and women. Br. J. Pharmacol. 2014, 171, 580–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitra, S.; Florez, I.D.; Tamayo, M.E.; Mbuagbaw, L.; Vanniyasingam, T.; Veroniki, A.A.; Zea, A.M.; Zhang, Y.; Sadeghirad, B.; Thabane, L. Association of placebo, indomethacin, ibuprofen, and acetaminophen with closure of hemodynamically significant patent ductus arteriosus in preterm infants: A systematic review and meta-analysis. Jama 2018, 319, 1221–1238. [Google Scholar] [CrossRef]
- Gerges, S.H.; El-Kadi, A.O. Sex differences in eicosanoid formation and metabolism: A possible mediator of sex discrepancies in cardiovascular diseases. Pharmacol. Ther. 2021, 234, 108046. [Google Scholar] [CrossRef]
- Pace, S.; Sautebin, L.; Werz, O. Sex-biased eicosanoid biology: Impact for sex differences in inflammation and consequences for pharmacotherapy. Biochem. Pharmacol. 2017, 145, 1–11. [Google Scholar] [CrossRef]
- Pace, S.; Rossi, A.; Krauth, V.; Dehm, F.; Troisi, F.; Bilancia, R.; Weinigel, C.; Rummler, S.; Werz, O.; Sautebin, L. Sex differences in prostaglandin biosynthesis in neutrophils during acute inflammation. Sci. Rep. 2017, 7, 3759. [Google Scholar] [CrossRef]
- Ochoa, D.; Prieto-Pérez, R.; Román, M.; Talegón, M.; Rivas, A.; Galicia, I.; Abad-Santos, F.; Cabaleiro, T. Effect of gender and CYP2C9 and CYP2C8 polymorphisms on the pharmacokinetics of ibuprofen enantiomers. Pharm. J. 2015, 16, 939–948. [Google Scholar] [CrossRef]
- Soldin, O.P.; Chung, S.H.; Mattison, D.R. Sex differences in drug disposition. Biomed. Biotechnol. 2011, 2011, 187103. [Google Scholar] [CrossRef]
- Walker, J.S.; Carmody, J.J. Experimental pain in healthy human subjects: Gender differences in nociception and in response to ibuprofen. Anesth. Analg. 1998, 86, 1257–1262. [Google Scholar] [CrossRef]
- Ohlsson, A.; Roberts, R.S.; Schmidt, B.; Davis, P.; Moddeman, D.; Saigal, S.; Solimano, A.; Vincer, M.; Wright, L.; trial of Indomethacin Prophylaxis in Preterms (TIPP) Investigators. Male/female differences in indomethacin effects in preterm infants. J. Pediatrics 2005, 147, 860–862. [Google Scholar] [CrossRef] [PubMed]
- Ment, L.R.; Vohr, B.R.; Makuch, R.W.; Westerveld, M.; Katz, K.H.; Schneider, K.C.; Duncan, C.C.; Ehrenkranz, R.; Oh, W.; Philip, A.G. Prevention of intraventricular hemorrhage by indomethacin in male preterm infants. J. Pediatrics 2004, 145, 832–834. [Google Scholar] [CrossRef] [PubMed]
- Ritz, S.A.; Antle, D.M.; Côté, J.; Deroy, K.; Fraleigh, N.; Messing, K.; Parent, L.; St-Pierre, J.; Vaillancourt, C.; Mergler, D. First steps for integrating sex and gender considerations into basic experimental biomedical research. FASEB J. 2014, 28, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Martin, Y.N.; Pabelick, C.M. Sex differences in the pulmonary circulation: Implications for pulmonary hypertension. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H1253–H1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stallings, E.; Antequera, A.; López-Alcalde, J.; García-Martín, M.; Urrútia, G.; Zamora, J. Sex as a Prognostic Factor in Systematic Reviews: Challenges and Lessons Learned. J. Pers. Med. 2021, 11, 441. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Meta-Analysis | K | RR | 95% CI | p | Heterogeneity | ||
|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | I2 (%) | p | ||||
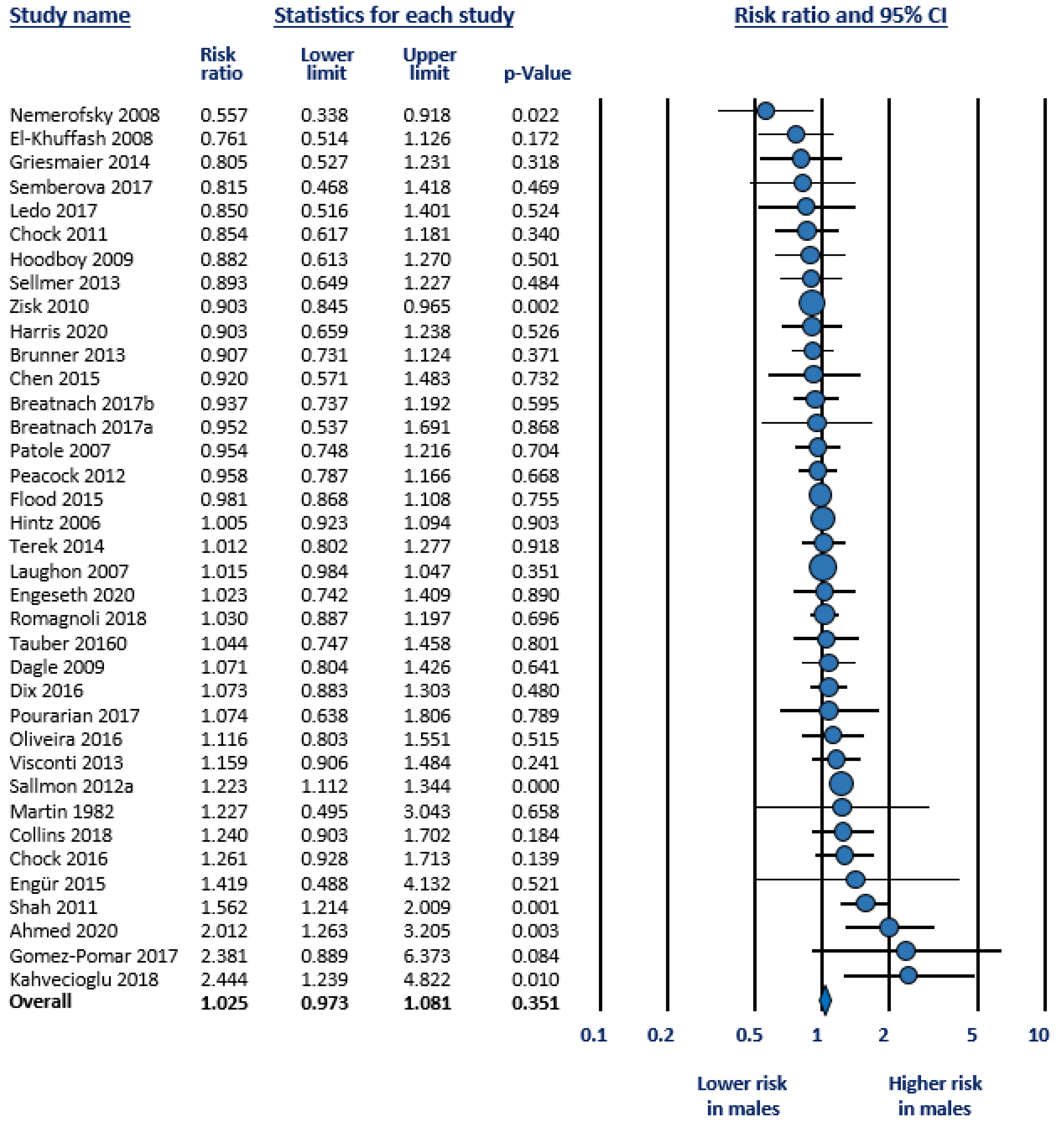
| Any PDA vs. closed DA | 37 | 1.025 | 0.973 | 1.081 | 0.351 | 53.2 | 0.000 |
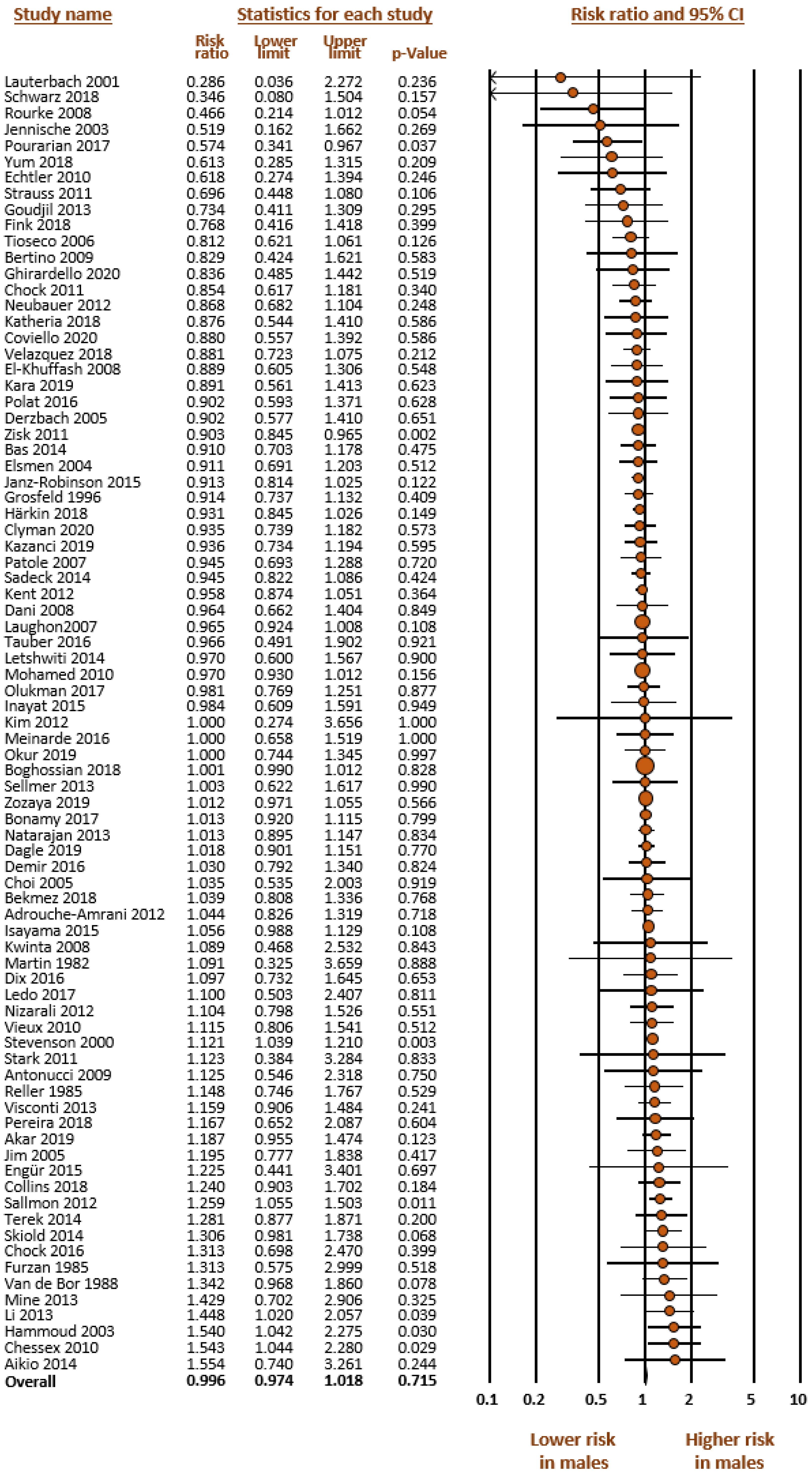
| hsPDA vs. (small PDA + closed DA) | 81 | 0.996 | 0.974 | 1.018 | 0.715 | 22.1 | 0.045 |
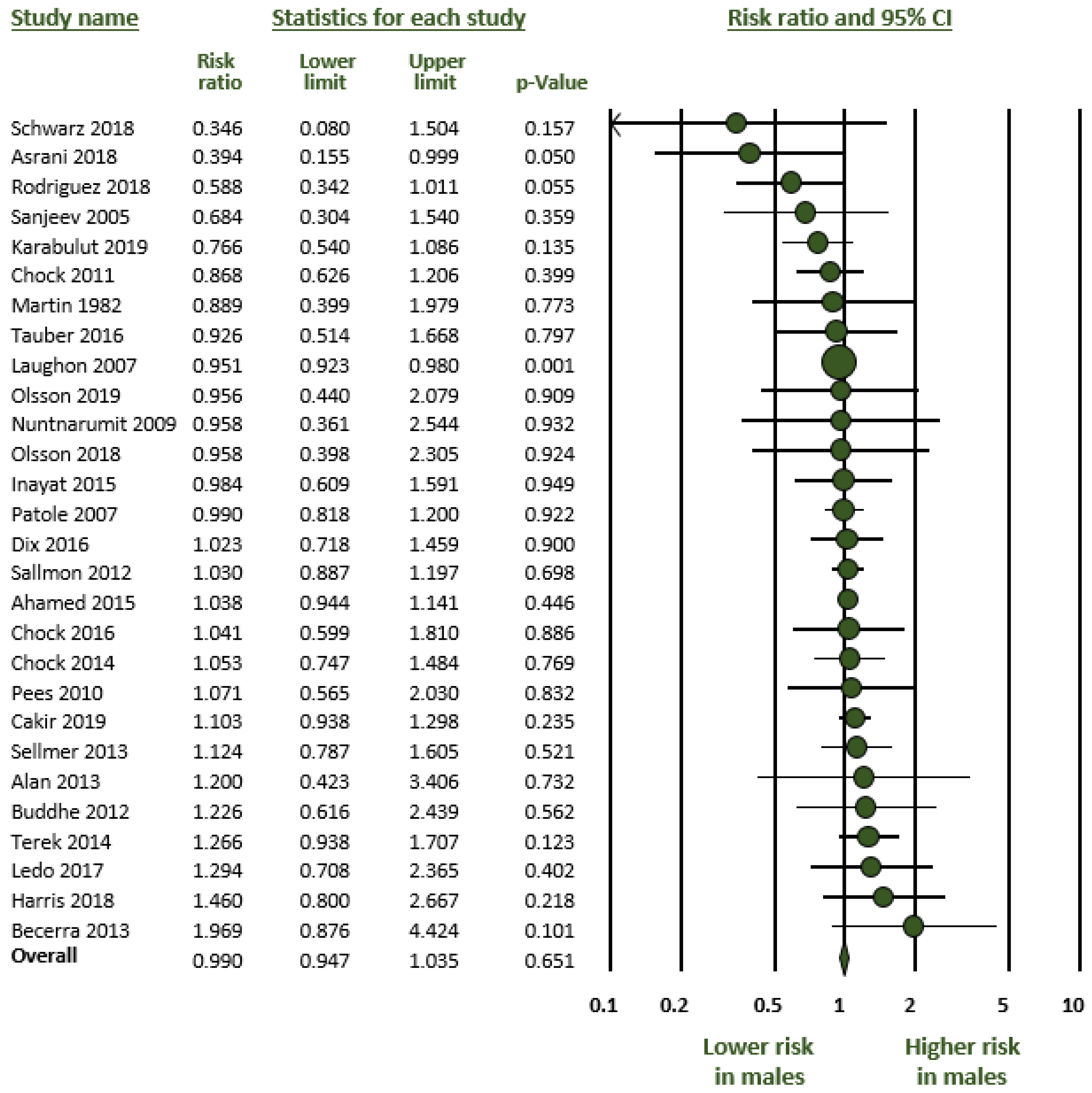
| hsPDA vs. small PDA | 28 | 0.990 | 0.947 | 1.035 | 0.651 | 6.0 | 0.374 |
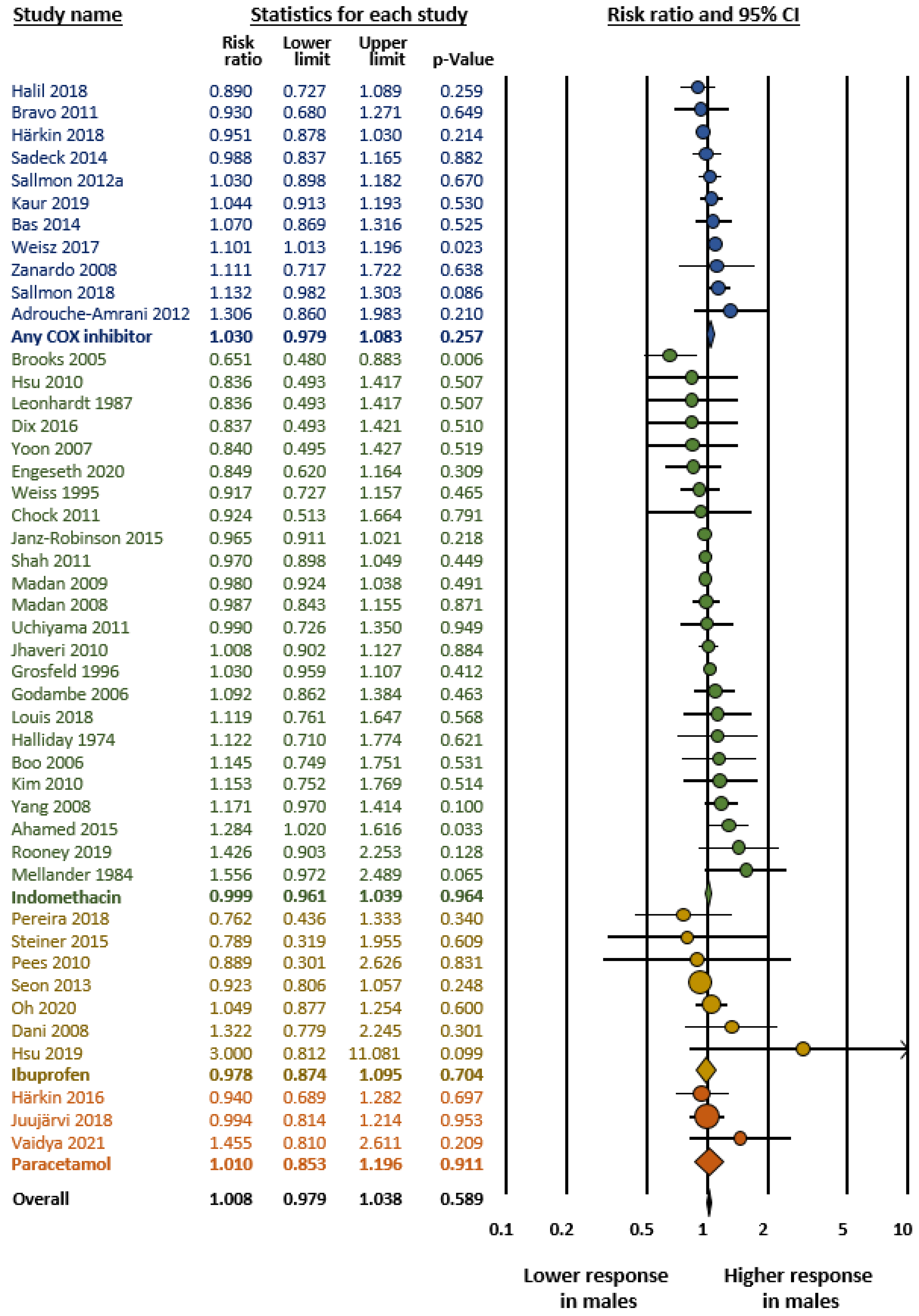
| Responders vs. non responders | 45 | 1.007 | 0.979 | 1.036 | 0.610 | 14.4 | 0.207 |
| Meta-Analysis | Subgroup | K | RR | 95% CI | p | Heterogeneity | ||
|---|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | I2 (%) | p | |||||
| Any PDA vs. closed DA | GA < 29 weeks | 26 | 1.023 | 0.958 | 1.092 | 0.502 | 51.7 | 0.001 |
| GA ≥ 29 weeks | 10 | 1.047 | 0.933 | 1.175 | 0.434 | 53.3 | 0.023 | |
| hsPDA vs. (small PDA + closed DA) | GA < 29 weeks | 50 | 1.006 | 0.979 | 1.033 | 0.688 | 17.7 | 0.143 |
| GA ≥ 29 weeks | 30 | 0.977 | 0.931 | 1.025 | 0.334 | 23.0 | 0.130 | |
| hsPDA vs. small PDA | GA < 29 weeks | 17 | 1.024 | 0.936 | 1.119 | 0.609 | 17.8 | 0.245 |
| GA ≥ 29 weeks | 11 | 0.975 | 0.932 | 1.019 | 0.265 | 0.0 | 0.690 | |
| Responders vs. non responders | GA < 29 weeks | 40 | 1.014 | 0.985 | 1.043 | 0.349 | 18.2 | 0.160 |
| GA ≥ 29 weeks | 5 | 0.936 | 0.854 | 1.027 | 0.162 | 0.0 | 0.937 | |
| Meta-Analysis | Continent | K | RR | 95% CI | p | Heterogeneity | ||
|---|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | I2 (%) | p | |||||
| Any PDA vs. closed DA | America | 14 | 1.034 | 0.959 | 1.116 | 0.383 | 64.9 | 0.000 |
| Asia | 5 | 1.104 | 0.892 | 1.368 | 0.363 | 38.8 | 0.163 | |
| Europe | 16 | 0.992 | 0.915 | 1.075 | 0.841 | 32.4 | 0.104 | |
| hsPDA vs. (small PDA + closed DA) | America | 26 | 0.988 | 0.958 | 1.019 | 0.448 | 37.5 | 0.029 |
| Asia | 19 | 1.021 | 0.937 | 1.112 | 0.640 | 11.8 | 0.310 | |
| Europe | 30 | 1.005 | 0.959 | 1.052 | 0.843 | 7.6 | 0.348 | |
| Oceania | 4 | 0.940 | 0.865 | 1.022 | 0.149 | 0.0 | 0.915 | |
| hsPDA vs. small PDA | America | 12 | 0.964 | 0.928 | 1.001 | 0.058 | 3.7 | 0.409 |
| Asia | 6 | 1.090 | 0.958 | 1.239 | 0.189 | 15.3 | 0.316 | |
| Europe | 9 | 1.012 | 0.898 | 1.140 | 0.849 | 0.07 | 0.537 | |
| Responders vs. non responders | America | 18 | 1.029 | 0.990 | 1.069 | 0.144 | 17.5 | 0.245 |
| Asia | 10 | 1.000 | 0.921 | 1.086 | 0.997 | 9.8 | 0.352 | |
| Europe | 15 | 0.996 | 0.938 | 1.058 | 0.905 | 0.0 | 0.779 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borges-Lujan, M.; Gonzalez-Luis, G.E.; Roosen, T.; Huizing, M.J.; Villamor, E. Sex Differences in Patent Ductus Arteriosus Incidence and Response to Pharmacological Treatment in Preterm Infants: A Systematic Review, Meta-Analysis and Meta-Regression. J. Pers. Med. 2022, 12, 1143. https://doi.org/10.3390/jpm12071143
Borges-Lujan M, Gonzalez-Luis GE, Roosen T, Huizing MJ, Villamor E. Sex Differences in Patent Ductus Arteriosus Incidence and Response to Pharmacological Treatment in Preterm Infants: A Systematic Review, Meta-Analysis and Meta-Regression. Journal of Personalized Medicine. 2022; 12(7):1143. https://doi.org/10.3390/jpm12071143
Chicago/Turabian StyleBorges-Lujan, Moreyba, Gema E. Gonzalez-Luis, Tom Roosen, Maurice J. Huizing, and Eduardo Villamor. 2022. "Sex Differences in Patent Ductus Arteriosus Incidence and Response to Pharmacological Treatment in Preterm Infants: A Systematic Review, Meta-Analysis and Meta-Regression" Journal of Personalized Medicine 12, no. 7: 1143. https://doi.org/10.3390/jpm12071143
APA StyleBorges-Lujan, M., Gonzalez-Luis, G. E., Roosen, T., Huizing, M. J., & Villamor, E. (2022). Sex Differences in Patent Ductus Arteriosus Incidence and Response to Pharmacological Treatment in Preterm Infants: A Systematic Review, Meta-Analysis and Meta-Regression. Journal of Personalized Medicine, 12(7), 1143. https://doi.org/10.3390/jpm12071143