
The Interplay of PR Interval and AV Pacing Delays Used for Cardiac Resynchronization Therapy in Heart Failure Patients: Association with Clinical Response in a Retrospective Analysis of a Large Observational Study


 , ,
, , 
 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Project Framework
2.2. Patient Population
2.3. Research Hypothesis, Methods, and Endpoints
2.4. Statistical Analysis
3. Results
3.1. LV Reverse Remodeling
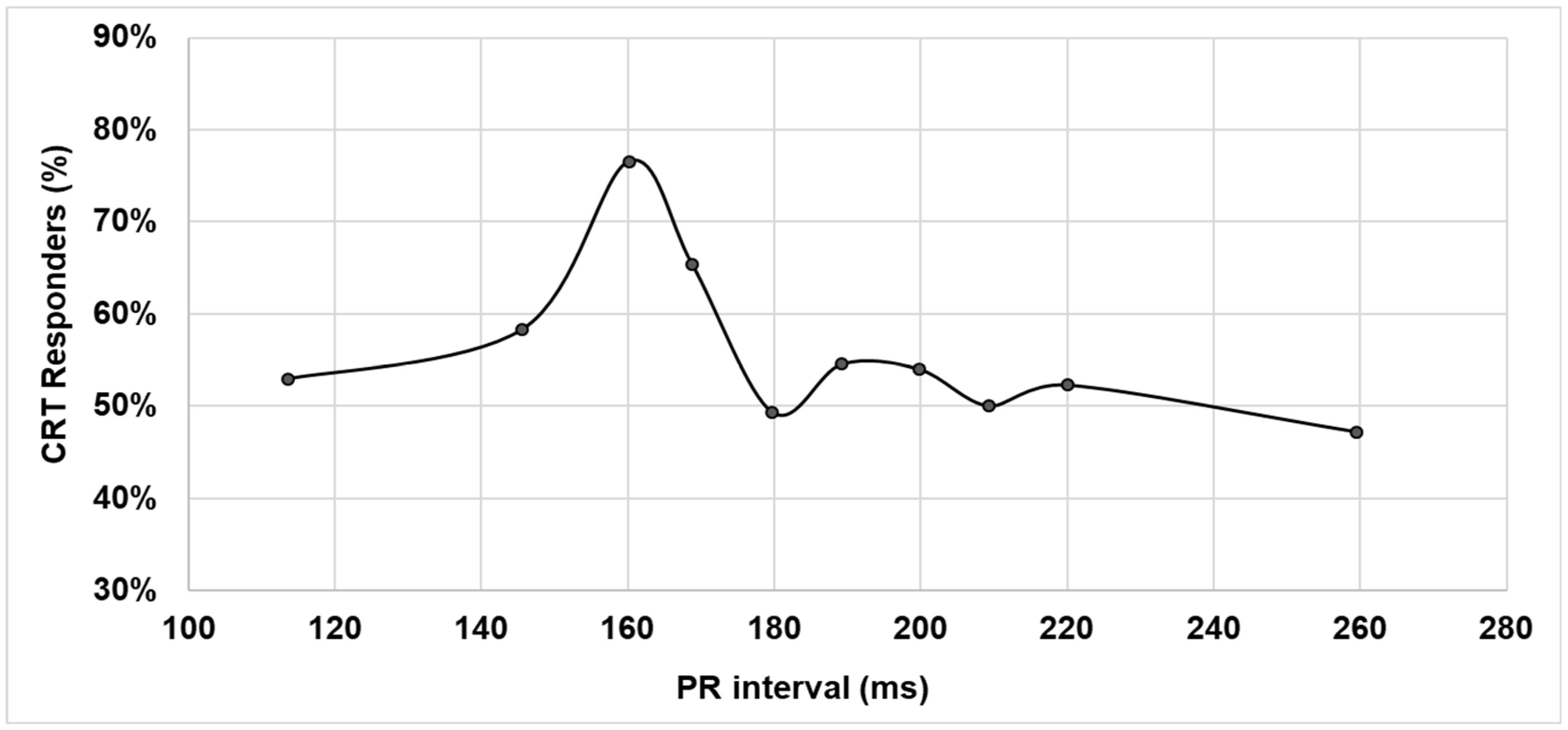
3.2. LV Reverse Remodeling and PR Interval
3.3. Clinical Outcomes
4. Discussion
4.1. LV Reverse Remodeling as a Function of PR Interval
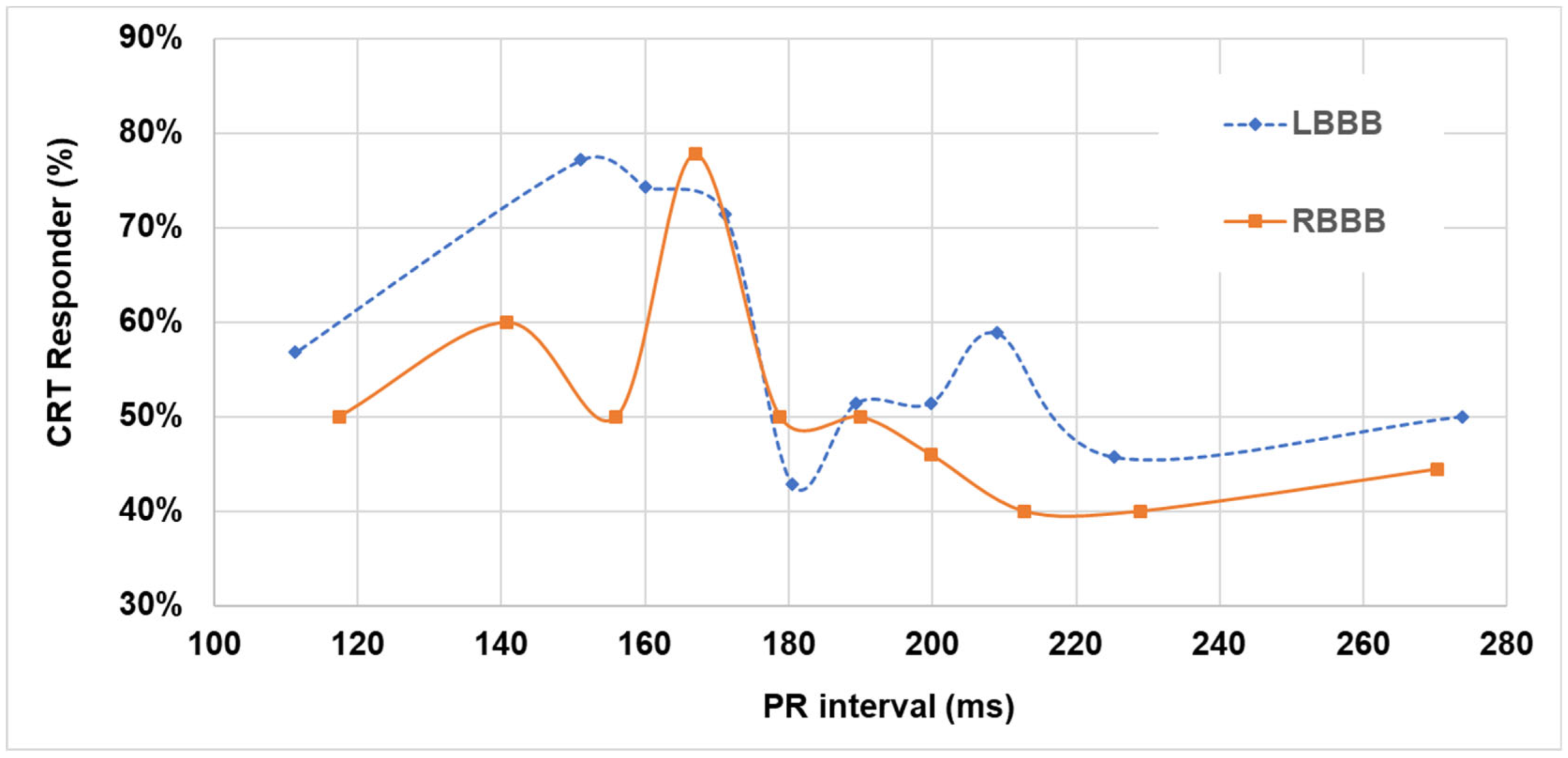
4.2. LV Reverse Remodeling as a Function of Baseline PR Interval and QRS Morphology
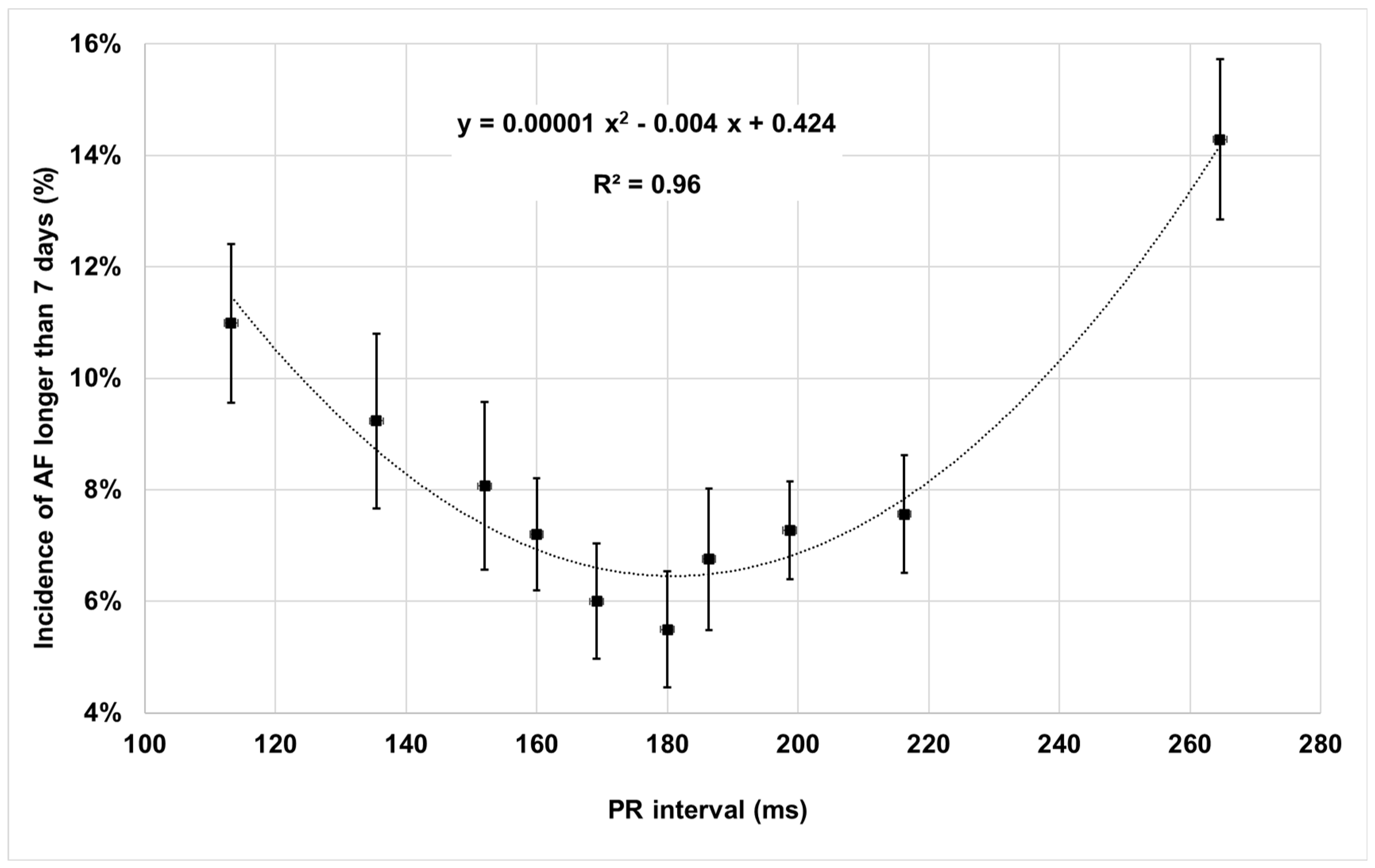
4.3. Clinical Outcomes as a Function of Baseline PR Interval
4.4. Clinical Implications
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Research Participating Centers
References
- Kusumoto, F.M.; Schoenfeld, M.H.; Barrett, C.; Edgerton, J.R.; Ellenbogen, K.A.; Gold, M.R.; Goldschlager, N.F.; Hamilton, R.M.; Joglar, J.A.; Kim, R.J.; et al. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: Executive summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. Heart Rhythm 2019, 16, e227–e279. [Google Scholar] [PubMed]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef] [PubMed]
- Cazeau, S.; Leclercq, C.; Lavergne, T.; Walker, S.; Varma, C.; Linde, C.; Garrigue, S.; Kappenberger, L.; Haywood, G.A.; Santini, M.; et al. Multisite Stimulation in Cardiomyopathies (MUSTIC) Study Investigators. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N. Engl. J. Med. 2001, 344, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Fisher, W.G.; Smith, A.L.; Delurgio, D.B.; Leon, A.R.; Loh, E.; Kocovic, D.Z.; Packer, M.; Clavell, A.L.; Hayes, D.L.; et al. MIRACLE Study Group. Multicenter InSync Randomized Clinical Evaluation. Cardiac resynchronization in chronic heart failure. N. Engl. J. Med. 2002, 346, 1845–1853. [Google Scholar] [CrossRef]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; DeMets, D.; White, B.G.; et al. Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) Investigators. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N. Engl. J. Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef]
- Cleland, J.G.; Daubert, J.C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L.; Cardiac Resynchronization-Heart Failure (CARE-HF) Study Investigators. Cardiac Resynchronization-Heart Failure (CARE-HF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N. Engl. J. Med. 2005, 352, 1539–1549. [Google Scholar] [CrossRef]
- Daubert, J.C.; Saxon, L.; Adamson, P.B.; Auricchio, A.; Berger, R.D.; Beshai, J.F.; Breithard, O.; Brignole, M.; Cleland, J.; DeLurgio, D.B.; et al. 2012 EHRA/HRS expert consensus statement on cardiac resynchronization therapy in heart failure: Implant and follow-up recommendations and management. European Heart Rhythm Association (EHRA); European Society of Cardiology (ESC); Heart Rhythm Society; Heart Failure Society of America (HFSA); American Society of Echocardiography (ASE); American Heart Association (AHA); European Association of Echocardiography (EAE) of ESC; Heart Failure Association of ESC (HFA). Europace 2012, 14, 1236–1286. [Google Scholar]
- Auricchio, A.; Lumens, J.; Prinzen, F.W. Does cardiac resynchronization therapy benefit patients with right bundle branch block. Circ. Arrhythmia Electrophysiol. 2014, 7, 532–542. [Google Scholar] [CrossRef]
- Pastore, G.; Morani, G.; Maines, M.; Marcantoni, L.; Bolzan, B.; Zanon, F.; Noventa, F.; Corbucci, G.; Baracca, E.; Picariello, C.; et al. Patients with right bundle branch block and concomitant delayed left ventricular activation respond to cardiac resynchronization therapy. Europace 2018, 20, 171–178. [Google Scholar] [CrossRef]
- Tompkins, C.; Kutyifa, V.; McNitt, S.; Polonsky, B.; Klein, H.U.; Moss, A.J.; Zareba, W. Effect on cardiac function of cardiac resynchronization therapy in patients with right bundle branch block (from the multicenter automatic defibrillator implantation trial with cardiac resynchronization Therapy [MADIT-CRT] Trial). Am. J. Cardiol. 2013, 112, 525–529. [Google Scholar] [CrossRef]
- Olshansky, B.; Day, J.; Sullivan, R.M.; Yong, P.; Galle, E.; Steinberg, J.S. Does cardiac resynchronization therapy provide unrecognized benefit in patients with prolonged PR intervals? The impact of restoring atrioventricular synchrony: An analysis from the COMPANION trial. Heart Rhythm 2012, 9, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Zareba, W.; Klein, H.; Cygankiewicz, I.; Hall, W.J.; McNitt, S.; Brown, M.; Cannom, D.; Daubert, J.P.; Eldar, M.; Gold, M.R.; et al. MADIT-CRT Investigators. Effectiveness of cardiac resynchronization therapy by QRS morphology in the Multicenter Automatic Defibrillator Implantation Trial-Cardiac Resynchronization Therapy (MADIT-CRT). Circulation 2011, 123, 1061–1072. [Google Scholar] [CrossRef] [PubMed]
- Kutyifa, V.; Stockburger, M.; Daubert, J.P.; Holmqvist, F.; Olshansky, B.; Schuger, C.; Klein, H.; Goldenberg, I.; Brenyo, A.; McNitt, S.; et al. PR interval identifies clinical response in patients with non-left bundle branch block. A multicenter automatic defibrillator implantation trial-cardiac resynchronization therapy substudy. Circ. Arrhythmia Electrophysiol. 2014, 7, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Brabham, W.W.; Gold, M.R. The role of AV and VV optimization for CRT. J. Arrhythmia 2013, 29, 153–161. [Google Scholar] [CrossRef]
- Varma, N.; Jones, P.; Wold, N.; Cronin, E.; Stein, K.J. How well do results from randomized clinical trials and/or recommendations for implantable cardioverter-defibrillator programming diffuse into clinical practice? translation assessed in a national cohort of patients with implantable cardioverter-defibrillators (ALTITUDE). Am. Heart Assoc. 2019, 8, e007392. [Google Scholar] [CrossRef]
- Surawicz, B.; Childers, R.; Deal, B.J.; Gettes, L.S.; Bailey, J.J.; Gorgels, A.; Hancock, E.W.; Josephson, M.; Kligfield, P.; Kors, J.A.; et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part III: Intraventricular conduction disturbances: A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: Endorsed by the International Society for Computerized Electrocardiology. J. Am. Coll. Cardiol. 2009, 53, 976–981. [Google Scholar]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.; et al. American Society of Echocardiography’s Nomenclature and Standards Committee.; Task Force on Chamber Quantification.; American College of Cardiology Echocardiography Committee; American Heart Association; European Association of Echocardiography, European Society of Cardiology Recommendations for chamber quantification. Eur. J. Echocardiogr. 2006, 7, 79–108. [Google Scholar]
- Ganesan, A.N.; Chew, D.P.; Hartshorne, T.; Selvanayagam, J.B.; Aylward, P.H.; Sanders, P.; McGavigan, A.D. The impact of atrial fibrillation type on the risk of thromboembolism, mortality, and bleeding: A systematic review and meta-analysis. Eur. Heart J. 2016, 37, 1591–1602. [Google Scholar] [CrossRef]
- Yu, C.M.; Chau, E.; Sanderson, J.E.; Fan, K.; Tang, M.O.; Fung, W.H.; Lin, H.; Kong, S.L.; Lam, Y.M.; Hill, M.R.S.; et al. Tissue doppler echocardiographic evidence of reverse remodeling and improved synchronicity by simultaneously delaying regional contraction after biventricular pacing therapy in heart failure. Circulation 2002, 105, 438–445. [Google Scholar] [CrossRef]
- Rinaldi, C.A.; Burri, H.; Thibault, B.; Curnis, A.; Rao, A.; Gras, D.; Sperzel, J.; Singh, J.P.; Biffi, M.; Bordachar, P.; et al. A review of multisite pacing to achieve cardiac resynchronization therapy. Europace 2015, 17, 7–17. [Google Scholar] [CrossRef]
- Ellenbogen, K.A.; Gold, M.R.; Meyer, T.E.; Fernandez Lozano, I.; Mittal, S.; Waggoner, A.D.; Lemke, B.; Singh, J.P.; Spinale, F.G.; Van Eyk, J.E.; et al. Primary results from the SmartDelay determined AV optimization: A comparison to other AV delay methods used in cardiac resynchronization therapy (SMART-AV) trial: A randomized trial comparing empirical, echocardiography-guided, and algorithmic atrioventricular delay programming in cardiac resynchronization therapy. Circulation 2010, 122, 2660–2668. [Google Scholar]
- Abraham, W.T.; Gras, D.; Yu, C.M.; Guzzo, L.; Gupta, M.S.; FREEDOM Steering Committee. Rationale and design of a randomized clinical trial to assess the safety and efficacy of frequent optimization of cardiac resynchronization therapy: The Frequent Optimization Study Using the QuickOpt Method (FREEDOM) trial. Am. Heart J. 2010, 159, 944–948. [Google Scholar] [CrossRef] [PubMed]
- Ritter, P.; Delnoy, P.P.; Padeletti, L.; Lunati, M.; Naegele, H.; Borri-Brunetto, A.; Silvestre, J. A randomized pilot study of optimization of cardiac resynchronization therapy in sinus rhythm patients using a peak endocardial acceleration sensor vs. standard methods. Europace 2012, 14, 1324–1333. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.O.; Lemke, B.; Birnie, D.; Krum, H.; Lee, K.L.; Aonuma, K.; Gasparini, M.; Starling, R.C.; Milasinovic, G.; Rogers, T.; et al. Adaptive CRT Study Investigators. Investigation of a novel algorithm for synchronized left-ventricular pacing and ambulatory optimization of cardiac resynchronization therapy: Results of the adaptive CRT trial. Heart Rhythm 2012, 9, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Chirife, R.; Ortega, D.F.; Salazar, A.I. Nonphysiological left heart AV intervals as a result of DDD and AAI ‘physiological’ pacing. Pacing Clin. Electrophysiol. 1991, 14, 1752–1756. [Google Scholar] [CrossRef] [PubMed]
- Von Bibra, H.; Wirtzfeld, A.; Hall, R.; Ulm, K.; Blomer, H. Mitral valve closure and left ventricular filling time in patients with VDD pacemakers: Assessment of the onset of left ventricular systole and the end of diastole. Br. Heart J. 1986, 55, 355–363. [Google Scholar] [CrossRef]
- Gasparini, M.; Birnie, D.; Lemke, B.; Aonuma, K.; Lee, K.L.; Gorcsan, J., 3rd; Landolina, M.; Klepfer, R.; Meloni, S.; Cicconelli, M.; et al. Adaptive cardiac resynchronization therapy reduces atrial fibrillation incidence in heart failure patients with prolonged AV conduction. Circ. Arrhythmia Electrophysiol. 2019, 12, e007260. [Google Scholar] [CrossRef]
- Ypenburg, C.; van Bommel, R.J.; Borleffs, C.J.; Bleeker, G.B.; Boersma, E.; Schalij, M.J.; Bax, J.J. Long-term prognosis after cardiac resynchronization therapy is related to the extent of left ventricular reverse remodeling at midterm follow-up. J. Am. Coll. Cardiol. 2009, 53, 483–490. [Google Scholar] [CrossRef]
- Trucco, E.; Tolosana, J.M.; Arbelo, E.; Doltra, A.; Castel, M.A.; Benito, E.; Borràs, R.; Guasch, E.; Vidorreta, S.; Vidal, B.; et al. Improvement of reverse remodeling using electrocardiogram fusion-optimized intervals in cardiac resynchronization therapy: A randomized study. JACC Clin. Electrophysiol. 2018, 4, 181–189. [Google Scholar] [CrossRef]
- Varma, N.; O’Donnell, D.; Bassiouny, M.; Ritter, P.; Pappone, C.; Mangual, J.; Cantillon, D.; Badie, N.; Thibault, B.; Wisnoskey, B. Programming cardiac resynchronization therapy for electrical synchrony: Reaching beyond left bundle branch block and left ventricular activation delay. J. Am. Heart Assoc. 2018, 7, e007489. [Google Scholar] [CrossRef]
- Boriani, G.; Vitolo, M. Grey zones in the practice of permanent cardiac pacing: The case of preventive pacing for improving rhythm control in atrial fibrillation. Int. J. Clin. Pract. 2021, 75, e13728. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Y.; Malik, J.; Wu, H.T.; Wang, C.L. Is the median hourly ambulatory heart rate range helpful in stratifying mortality risk among newly diagnosed atrial fibrillation patients? J. Pers. Med. 2021, 11, 1202. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Vitolo, M. Atrial fibrillation in patients with cardiac implantable electronic devices: New perspectives with important clinical implications. Kardiol. Pol. 2019, 77, 1119–1120. [Google Scholar] [CrossRef] [PubMed]
- Manfrin, M.; Mugnai, G.; Rauhe, W.; Velagic, V.; Unterhuber, M. Left atrial pressure as a predictor of success in catheter ablation of atrial fibrillation in a real-life cohort. J. Clin. Med. 2021, 10, 3208. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Vitolo, M.; Diemberger, I.; Proietti, M.; Valenti, A.C.; Malavasi, V.L.; Lip, G.Y.H. Optimizing indices of atrial fibrillation susceptibility and burden to evaluate atrial fibrillation severity, risk and outcomes. Cardiovasc. Res. 2021, 117, 1–21. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Analyzed Cohort (1718 Patients) | |
|---|---|
| Patient demographics | |
| Age (years) mean ± SD | 66 ± 10 |
| Gender (male) (%) | 78.7% |
| Medical history | |
| Secondary prevention (%) | 12.4% |
| Atrial tachyarrhythmias (%) | 21.9% |
| Ischemic cardiopathy (%) | 53.0% |
| Myocardium infarction (%) | 47.0% |
| Right bundle branch block (%) | 17.6% |
| Left bundle branch block (%) | 70.8% |
| New York Heart Association Classes III–IV (%) | 71.6% |
| Hypertension (%) | 57.9% |
| Diabetes (%) | 28.8% |
| History of stroke/TIA (%) | 3.7% |
| Valvular disease (%) | 21.1% |
| ECG and echo measures | |
| QRS duration (ms), mean ± SD | 151 ± 29 |
| PR interval (ms), median (IQR) | 182 (160–204) |
| P wave duration (ms), median (IQR) | 80 (60–90) |
| Left ventricle ejection fraction (%), mean ± SD | 27 ± 6 |
| Left ventricle end-diastolic volume (ml), mean ± SD | 209 ± 78 |
| Left ventricle end-systolic volume (ml), mean ± SD | 154 ± 64 |
| Left ventricle end-diastolic diameter (mm), mean ± SD | 70 ± 40 |
| Left ventricle end-systolic diameter (mm), mean ± SD | 60 ± 39 |
| Left atrium diameter (mm), mean ± SD | 49 ± 16 |
| Baseline medical therapy | |
| Beta-blocker (%) | 73.7% |
| Diuretic (%) | 85.2% |
| Antiarrhythmics (%) | 21.3% |
| ACE-inhibitor/ARB (%) | 81.4% |
| Digitalis (%) | 15.8% |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| PR > 200 ms | 0.68 (0.46–0.98) | 0.040 | ||
| 150 ms ≤ PR ≤ 170 ms | 2.17 (1.46–3.23) | <0.001 | 2.51 (1.41–4.47) | 0.002 |
| Age > 65 years | 0.82 (0.59–1.15) | 0.243 | ||
| Gender (male) | 0.64 (0.42–0.97) | 0.034 | ||
| Secondary prevention | 0.57 (0.34–0.98) | 0.042 | ||
| Atrial tachyarrhythmias | 0.70 (0.47–1.05) | 0.088 | ||
| Hypertension | 1.41 (0.93–2.16) | 0.107 | ||
| Diabetes | 0.66 (0.42–1.04) | 0.072 | 0.37 (0.20–0.67) | 0.001 |
| History of stroke/TIA | 0.58 (0.19–1.75) | 0.329 | ||
| Valvular disease | 0.69 (0.47–1.00) | 0.053 | 0.52 (0.29–0.93) | 0.027 |
| Ischemic cardiomyopathy | 0.48 (0.34–0.67) | <0.001 | 0.52 (0.30–0.89) | 0.018 |
| Myocardium infarction | 0.52 (0.37–0.75) | <0.001 | ||
| RBBB | 0.85 (0.55–1.32) | 0.477 | ||
| LBBB | 1.26 (0.89–1.77) | 0.193 | ||
| NYHA 3/4 | 0.76 (0.52–1.11) | 0.162 | ||
| QRS > 150 ms | 1.28 (0.92–1.78) | 0.147 | ||
| LVEF ≤ 25% | 0.88 (0.63–1.23) | 0.464 | ||
| ACE-inhibitor/ARB | 1.13 (0.71–1.78) | 0.614 | ||
| Beta-blocker | 1.34 (0.91–1.96) | 0.139 | ||
| Digitalis | 0.95 (0.59–1.54) | 0.846 | ||
| Diuretics | 0.79 (0.48–1.31) | 0.365 | ||
| Antiarrhythmics | 0.76 (0.51–1.13) | 0.178 | ||
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| PR > 200 ms | 1.50 (1.21–1.85) | <0.001 | ||
| 150 ms ≤ PR ≤ 170 ms | 0.74 (0.59–0.93) | 0.011 | 0.79 (0.63–0.99) | 0.046 |
| Age > 65 yrs | 1.57 (1.27–1.94) | <0.001 | 1.26 (1.00–1.59) | 0.050 |
| Gender (male) | 1.49 (1.14–1.94) | 0.004 | ||
| Secondary prevention | 1.62 (1.26–2.09) | <0.001 | 1.37 (1.03–1.84) | 0.032 |
| Atrial tachyarrhythmias | 1.72 (1.38–2.13) | <0.001 | 1.64 (1.30–2.08) | <0.001 |
| Hypertension | 1.11 (0.88–1.41) | 0.365 | ||
| Diabetes | 1.98 (1.58–2.48) | <0.001 | 2.15 (1.49–3.10) | <0.001 |
| History of stroke/TIA | 1.34 (0.82–2.19) | 0.236 | ||
| Valvular disease | 1.13 (0.89–1.44) | 0.316 | ||
| Ischemic cardiomyopathy | 1.64 (1.33–2.01) | <0.001 | 1.45 (1.15–1.83) | 0.002 |
| Myocardial infarction | 1.67 (1.36–2.05) | <0.001 | ||
| RBBB | 1.23 (0.91–1.66) | 0.175 | ||
| LBBB | 0.80 (0.65–0.99) | 0.041 | ||
| NYHA Class III or IV | 1.51 (1.20–1.91) | <0.001 | ||
| QRS > 150 ms | 0.91 (0.75–1.11) | 0.361 | ||
| EF ≤ 25% | 1.25 (1.01–1.53) | 0.037 | ||
| ACE-inhibitor/ARB | 0.82 (0.64–1.05) | 0.117 | ||
| Beta-blocker | 0.56 (0.46–0.70) | <0.001 | ||
| Digitalis | 1.23 (0.93–1.62) | 0.141 | ||
| Diuretics | 1.44 (1.06–1.97) | 0.019 | ||
| Antiarrhythmics | 1.57 (1.26–1.95) | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gasparini, M.; Biffi, M.; Landolina, M.; Cattafi, G.; Rordorf, R.; Botto, G.L.; Battista Forleo, G.; Morani, G.; Santini, L.; Dello Russo, A.; et al. The Interplay of PR Interval and AV Pacing Delays Used for Cardiac Resynchronization Therapy in Heart Failure Patients: Association with Clinical Response in a Retrospective Analysis of a Large Observational Study. J. Pers. Med. 2022, 12, 1512. https://doi.org/10.3390/jpm12091512
Gasparini M, Biffi M, Landolina M, Cattafi G, Rordorf R, Botto GL, Battista Forleo G, Morani G, Santini L, Dello Russo A, et al. The Interplay of PR Interval and AV Pacing Delays Used for Cardiac Resynchronization Therapy in Heart Failure Patients: Association with Clinical Response in a Retrospective Analysis of a Large Observational Study. Journal of Personalized Medicine. 2022; 12(9):1512. https://doi.org/10.3390/jpm12091512
Chicago/Turabian StyleGasparini, Maurizio, Mauro Biffi, Maurizio Landolina, Giuseppe Cattafi, Roberto Rordorf, Giovanni Luca Botto, Giovanni Battista Forleo, Giovanni Morani, Luca Santini, Antonio Dello Russo, and et al. 2022. "The Interplay of PR Interval and AV Pacing Delays Used for Cardiac Resynchronization Therapy in Heart Failure Patients: Association with Clinical Response in a Retrospective Analysis of a Large Observational Study" Journal of Personalized Medicine 12, no. 9: 1512. https://doi.org/10.3390/jpm12091512
APA StyleGasparini, M., Biffi, M., Landolina, M., Cattafi, G., Rordorf, R., Botto, G. L., Battista Forleo, G., Morani, G., Santini, L., Dello Russo, A., Rossillo, A., Meloni, S., Grammatico, A., Vitolo, M., & Boriani, G. (2022). The Interplay of PR Interval and AV Pacing Delays Used for Cardiac Resynchronization Therapy in Heart Failure Patients: Association with Clinical Response in a Retrospective Analysis of a Large Observational Study. Journal of Personalized Medicine, 12(9), 1512. https://doi.org/10.3390/jpm12091512