


Plasma Interleukin-6 Level Predicts the Risk of Arteriovenous Fistula Dysfunction in Patients Undergoing Maintenance Hemodialysis

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
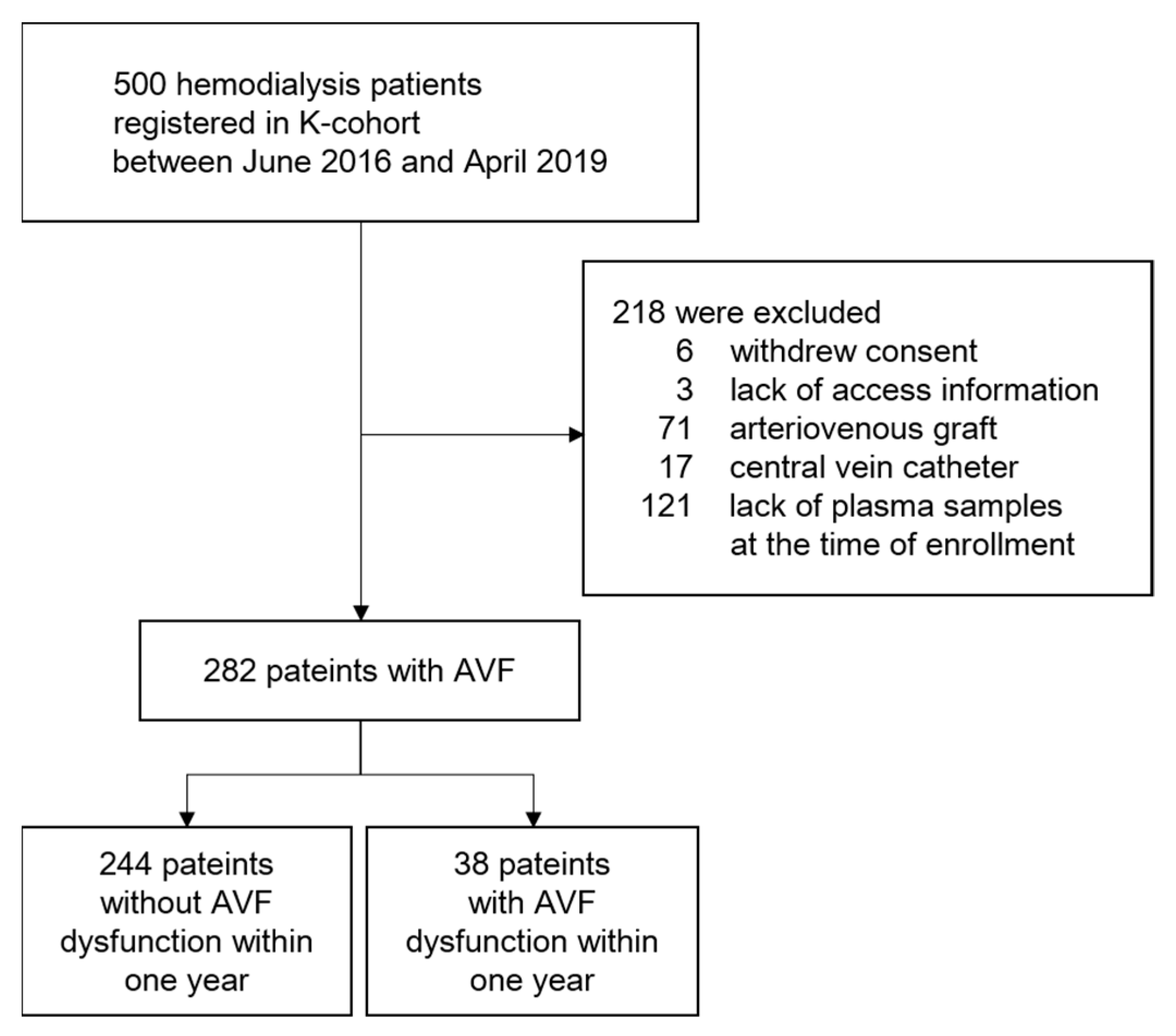
2.1. Study Population
2.2. Data Collection
2.3. Outcome Measures
2.4. Measurements of Circulating Inflammatory Cytokines and Chemokines
2.5. Statistical Analysis
3. Results
3.1. Baseline Clinical Parameters of Enrolled Patients
3.2. Risk Factors for the Occurrence of AVF Dysfunction
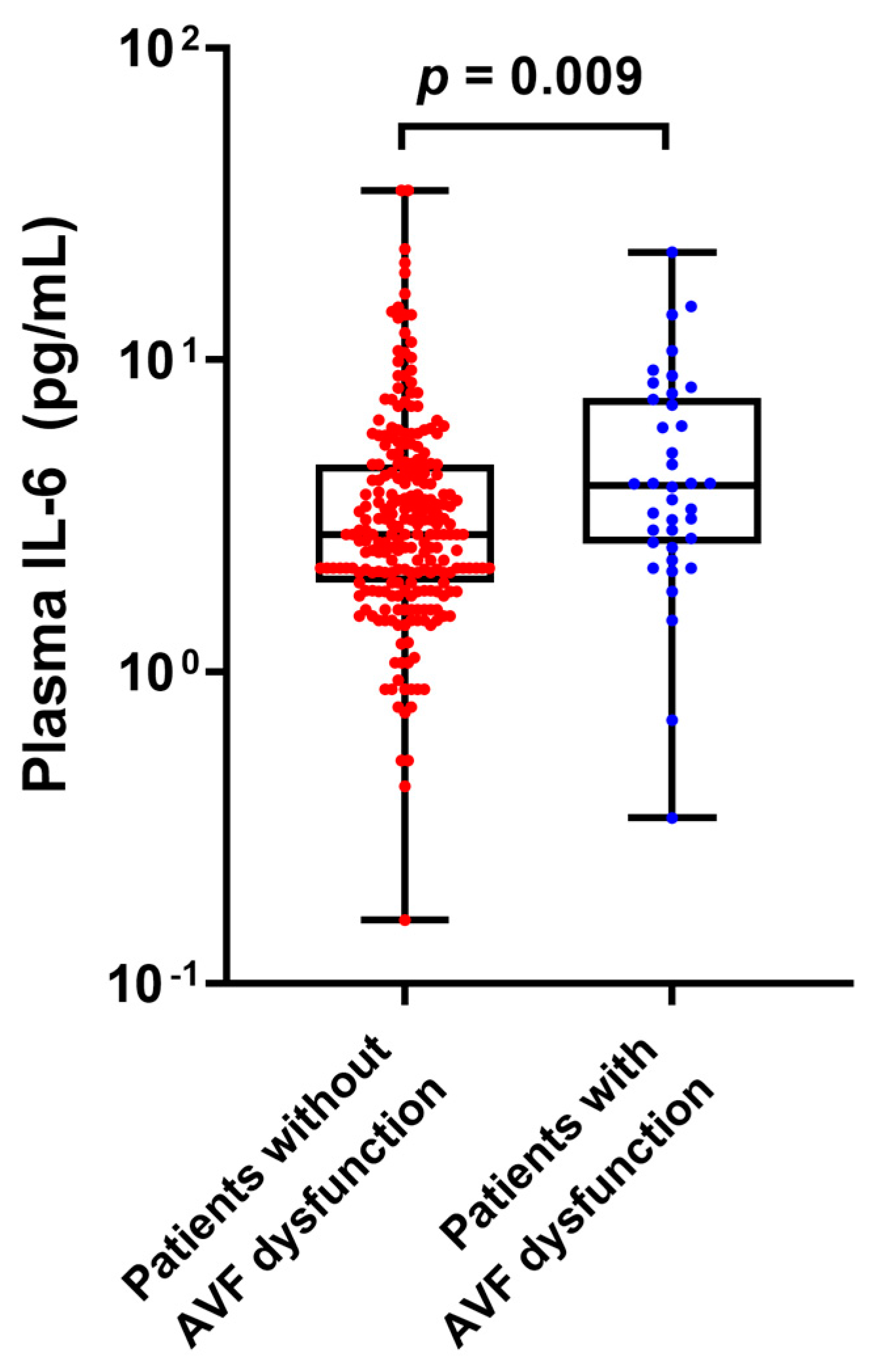
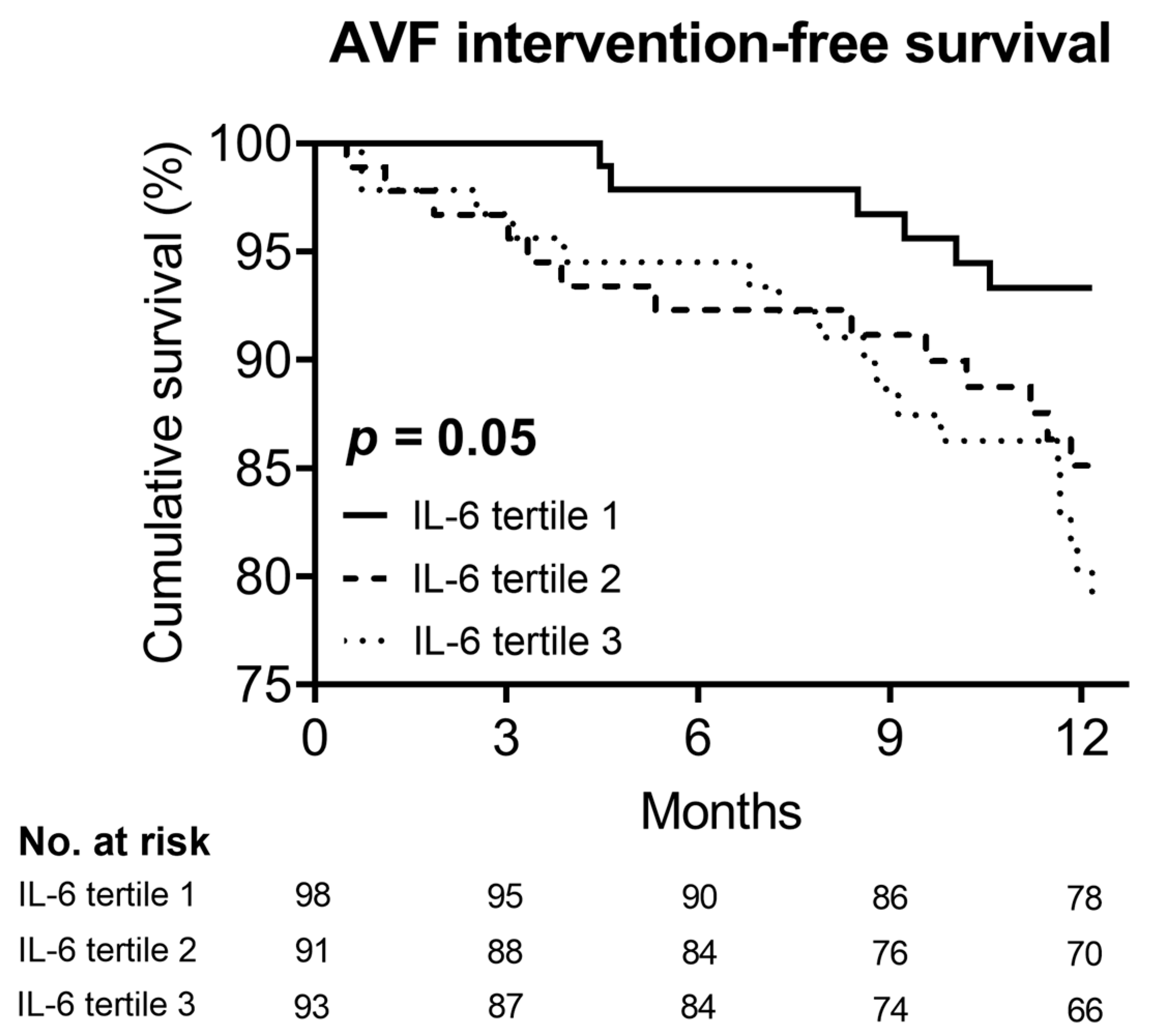
3.3. Association between Plasma IL-6 Level and AVF Dysfunction
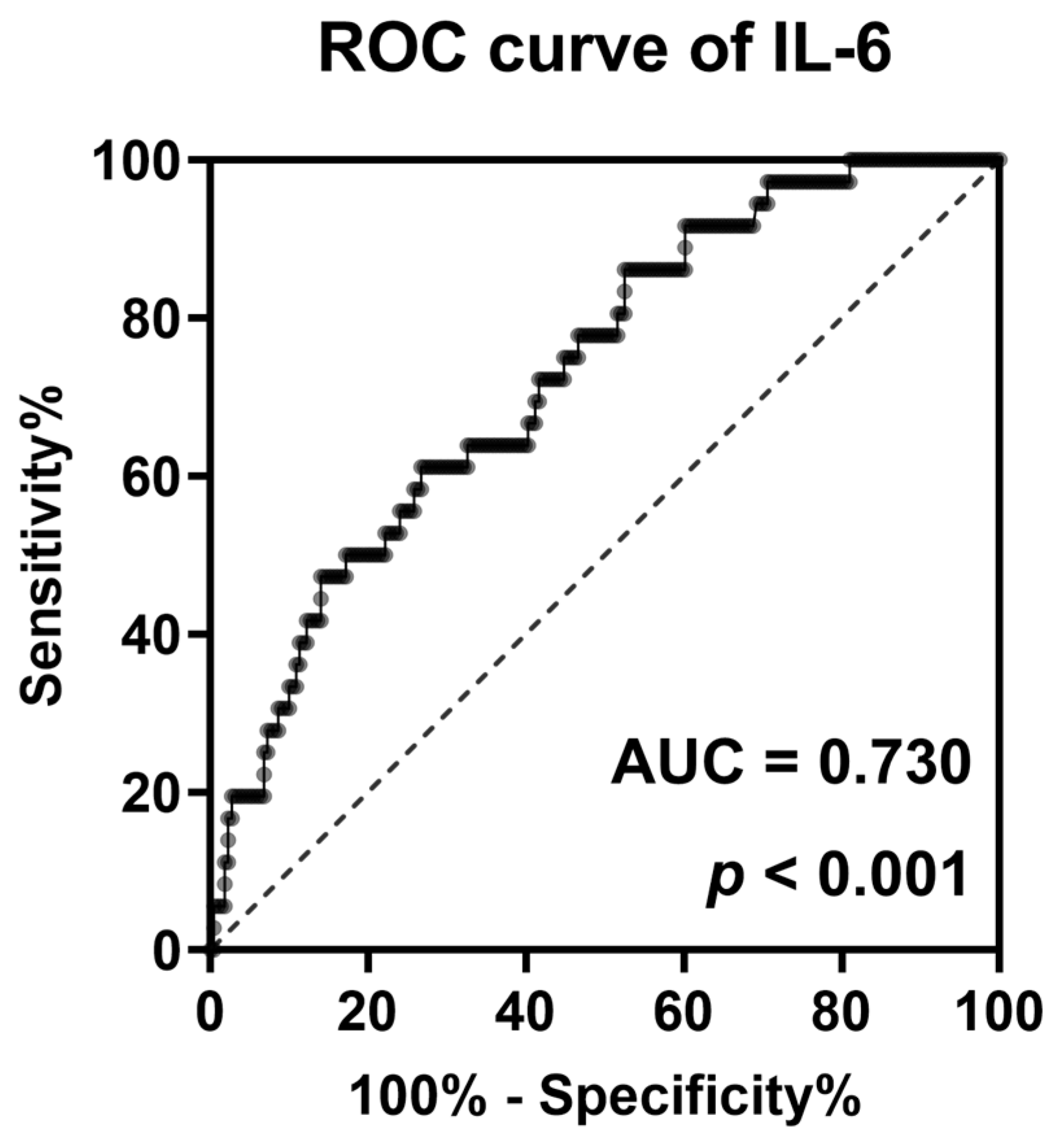
3.4. Discriminative Power of IL-6 to Identify AVF Dysfunction within One Year
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, J.Y.; Jin, D.C. Patient characteristics according to rehabilitation and employment status in Korean hemodialysis patients. Kidney Res. Clin. Pract. 2020, 39, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Himmelfarb, J.; Vanholder, R.; Mehrotra, R.; Tonelli, M. The current and future landscape of dialysis. Nat. Rev. Nephrol. 2020, 16, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Polkinghorne, K.R.; McDonald, S.P.; Atkins, R.C.; Kerr, P.G. Vascular access and all-cause mortality: A propensity score analysis. J. Am. Soc. Nephrol. 2004, 15, 477–486. [Google Scholar] [CrossRef] [Green Version]
- Feldman, H.I.; Kobrin, S.; Wasserstein, A. Hemodialysis vascular access morbidity. J. Am. Soc. Nephrol. 1996, 7, 523–535. [Google Scholar] [CrossRef]
- Saran, R.; Robinson, B.; Abbott, K.C.; Bragg-Gresham, J.; Chen, X.; Gipson, D.; Gu, H.; Hirth, R.A.; Hutton, D.; Jin, Y. US renal data system 2019 annual data report: Epidemiology of kidney disease in the United States. Am. J. Kidney Dis. 2020, 75, A6–A7. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.J.; Foley, R.N.; Chavers, B.; Gilbertson, D.; Herzog, C.; Johansen, K.; Kasiske, B.; Kutner, N.; Liu, J.; St Peter, W. ‘United States Renal Data System 2011 Annual Data Report: Atlas of chronic kidney disease & end-stage renal disease in the United States. Am. J. Kidney Dis. 2012, 59, e1–e420. [Google Scholar]
- Wong, V.; Ward, R.; Taylor, J.; Selvakumar, S.; How, T.V.; Bakran, A. Factors associated with early failure of arteriovenous fistulae for haemodialysis access. Eur. J. Vasc. Endovasc. Surg. 1996, 12, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Smith, G.E.; Gohil, R.; Chetter, I.C. Factors affecting the patency of arteriovenous fistulas for dialysis access. J. Vasc. Surg. 2012, 55, 849–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagliardi, G.M.; Rossi, S.; Condino, F.; Mancuso, D.; Greco, F.; Tenuta, R.; Savino, O.; Bonofiglio, R.; Domma, F.; Latorre, G. Malnutrition, infection and arteriovenous fistula failure: Is there a link? J. Vasc. Access 2011, 12, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Feldman, H.I.; Joffe, M.; Rosas, S.E.; Burns, J.E.; Knauss, J.; Brayman, K. Predictors of successful arteriovenous fistula maturation. Am. J. Kidney Dis. 2003, 42, 1000–1012. [Google Scholar] [CrossRef]
- Shah, P.K. Inflammation, neointimal hyperplasia, and restenosis: As the leukocytes roll, the arteries thicken. Circulation 2003, 107, 2175–2177. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Kim, S.Y.; Moon, H.; Seo, J.W.; Kim, D.J.; Park, S.H.; Kim, Y.G.; Moon, J.Y.; Kim, J.S.; Jeong, K.H.; et al. Endocan as a marker of microvascular inflammation in kidney transplant recipients. Sci. Rep. 2019, 9, 1854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.H.; Kim, J.S.; Kim, S.Y.; Kim, Y.G.; Moon, J.Y.; Jeong, K.H.; Lee, T.W.; Ihm, C.G.; Lee, S.H. Plasma endocan level and prognosis of immunoglobulin A nephropathy. Kidney Res. Clin. Pract. 2016, 35, 152–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.K.; Lee, Y.H.; Kim, J.S.; Kim, Y.G.; Lee, S.Y.; Ahn, S.Y.; Lee, D.Y.; Jeong, K.H.; Lee, S.H.; Hwang, H.S.; et al. Circulating Vascular Adhesion Protein-1 Level Predicts the Risk of Cardiovascular Events and Mortality in Hemodialysis Patients. Front. Cardiovasc. Med. 2021, 8, 701079. [Google Scholar] [CrossRef]
- Hwang, H.S.; Kim, J.S.; Kim, Y.G.; Lee, S.Y.; Ahn, S.Y.; Lee, H.J.; Lee, D.Y.; Lee, S.H.; Moon, J.Y.; Jeong, K.H. Circulating PCSK9 Level and Risk of Cardiovascular Events and Death in Hemodialysis Patients. J. Clin. Med. 2020, 9, 244. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.H.; Kim, K.P.; Park, S.H.; Kim, D.J.; Kim, Y.G.; Moon, J.Y.; Jung, S.W.; Kim, J.S.; Jeong, K.H.; Lee, S.Y.; et al. Urinary chemokine C-X-C motif ligand 16 and endostatin as predictors of tubulointerstitial fibrosis in patients with advanced diabetic kidney disease. Nephrol. Dial. Transplant. 2021, 36, 295–305. [Google Scholar] [CrossRef]
- Yap, Y.S.; Chi, W.C.; Lin, C.H.; Liu, Y.C.; Wu, Y.W. Association of early failure of arteriovenous fistula with mortality in hemodialysis patients. Sci. Rep. 2021, 11, 5699. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, H.; Kim, D.K.; Oh, K.H.; Kim, Y.S.; Ahn, C.; Han, J.S.; Min, S.K.; Min, S.I.; Kim, H.C.; et al. Recurrent Vascular Access Dysfunction as a Novel Marker of Cardiovascular Outcome and Mortality in Hemodialysis Patients. Am. J. Nephrol. 2016, 44, 71–80. [Google Scholar] [CrossRef]
- Wu, C.K.; Lin, C.H.; Hsu, C.C.; Tarng, D.C.; Kor, C.T.; Chen, Y.C.; Wu, C.L.; Chang, C.C. Association of early loss of primary functional patency of arteriovenous access with mortality in incident hemodialysis patients: A nationwide population-based observational study. Medicine 2018, 97, e11630. [Google Scholar] [CrossRef]
- Tordoir, J.H.; Hofstra, L.; Leunissen, K.M.; Kitslaar, P.J. Early experience with stretch polytetrafluoroethylene grafts for haemodialysis access surgery: Results of a prospective randomised study. Eur. J. Vasc. Endovasc. Surg. 1995, 9, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Mattana, J.; Effiong, C.; Kapasi, A.; Singhal, P.C. Leukocyte-polytetrafluoroethylene interaction enhances proliferation of vascular smooth muscle cells via tumor necrosis factor-alpha secretion. Kidney Int. 1997, 52, 1478–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ezzahiri, R.; Lemson, M.S.; Kitslaar, P.J.; Leunissen, K.M.; Tordoir, J.H. Haemodialysis vascular access and fistula surveillance methods in The Netherlands. Nephrol. Dial. Transplant. 1999, 14, 2110–2115. [Google Scholar] [CrossRef] [Green Version]
- Brahmbhatt, A.; Remuzzi, A.; Franzoni, M.; Misra, S. The molecular mechanisms of hemodialysis vascular access failure. Kidney Int. 2016, 89, 303–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy-Chaudhury, P.; Sukhatme, V.P.; Cheung, A.K. Hemodialysis vascular access dysfunction: A cellular and molecular viewpoint. J. Am. Soc. Nephrol. 2006, 17, 1112–1127. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.P.; Liu, L.P.; Lu, Z.X. One-year patency rate of native arteriovenous fistulas reconstructed by vascular stripping in hemodialysis patients with venous neointimal hyperplasia. J. Vasc. Surg. 2015, 61, 192–196. [Google Scholar] [CrossRef] [Green Version]
- Marrone, D.; Pertosa, G.; Simone, S.; Loverre, A.; Capobianco, C.; Cifarelli, M.; Memoli, B.; Schena, F.P.; Grandaliano, G. Local activation of interleukin 6 signaling is associated with arteriovenous fistula stenosis in hemodialysis patients. Am. J. Kidney Dis. 2007, 49, 664–673. [Google Scholar] [CrossRef]
- Liang, A.; Wang, Y.; Han, G.; Truong, L.; Cheng, J. Chronic kidney disease accelerates endothelial barrier dysfunction in a mouse model of an arteriovenous fistula. Am. J. Physiol. Renal. Physiol. 2013, 304, F1413–F1420. [Google Scholar] [CrossRef] [Green Version]
- Misra, S.; Fu, A.A.; Rajan, D.K.; Juncos, L.A.; McKusick, M.A.; Bjarnason, H.; Mukhopadhyay, D. Expression of hypoxia inducible factor-1 alpha, macrophage migration inhibition factor, matrix metalloproteinase-2 and -9, and their inhibitors in hemodialysis grafts and arteriovenous fistulas. J. Vasc. Interv. Radiol. 2008, 19 Pt 1, 252–259. [Google Scholar] [CrossRef]
- Asare, Y.; Schmitt, M.; Bernhagen, J. The vascular biology of macrophage migration inhibitory factor (MIF). Expression and effects in inflammation, atherogenesis and angiogenesis. Thromb. Haemost. 2013, 109, 391–398. [Google Scholar] [CrossRef]
- Virzì, G.M.; Clementi, A.; de Cal, M.; Brocca, A.; Day, S.; Pastori, S.; Bolin, C.; Vescovo, G.; Ronco, C. Oxidative stress: Dual pathway induction in cardiorenal syndrome type 1 pathogenesis. Oxid. Med. Cell. Longev. 2015, 2015, 391790. [Google Scholar] [CrossRef] [PubMed]
- Volpato, S.; Guralnik, J.M.; Ferrucci, L.; Balfour, J.; Chaves, P.; Fried, L.P.; Harris, T.B. Cardiovascular disease, interleukin-6, and risk of mortality in older women: The women’s health and aging study. Circulation 2001, 103, 947–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenvinkel, P.; Heimbürger, O.; Jogestrand, T. Elevated interleukin-6 predicts progressive carotid artery atherosclerosis in dialysis patients: Association with Chlamydia pneumoniae seropositivity. Am. J. Kidney Dis. 2002, 39, 274–282. [Google Scholar] [CrossRef]
- Ridker, P.M.; Rifai, N.; Stampfer, M.J.; Hennekens, C.H. Plasma concentration of interleukin-6 and the risk of future myocardial infarction among apparently healthy men. Circulation 2000, 101, 1767–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, A.; Odamaki, M.; Takita, T.; Maruyama, Y.; Kumagai, H.; Hishida, A. Association between interleukin-6 and carotid atherosclerosis in hemodialysis patients. Kidney Int. 2002, 61, 1143–1152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.J.; Ko, Y.S.; Ko, P.J.; Hsu, L.A.; Chen, C.F.; Yang, C.W.; Hsu, T.S.; Pang, J.H. Thrombosed arteriovenous fistula for hemodialysis access is characterized by a marked inflammatory activity. Kidney Int. 2005, 68, 1312–1319. [Google Scholar] [CrossRef] [Green Version]
- Dukkipati, R.; Molnar, M.Z.; Park, J.; Jing, J.; Kovesdy, C.P.; Kajani, R.; Kalantar-Zadeh, K. Association of vascular access type with inflammatory marker levels in maintenance hemodialysis patients. Semin. Dial. 2014, 27, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Morton, S.K.; Rodríguez, A.J.; Morris, D.R.; Bhandari, A.P.; Moxon, J.V.; Golledge, J. A Systematic Review and Meta-Analysis of Circulating Biomarkers Associated with Failure of Arteriovenous Fistulae for Haemodialysis. PLoS ONE 2016, 11, e0159963. [Google Scholar] [CrossRef] [Green Version]
- Wan, Q.; Li, L.; Yang, S.; Chu, F. Impact of Statins on Arteriovenous Fistulas Outcomes: A Meta-Analysis. Ther. Apher. Dial. 2018, 22, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Pisoni, R.; Barker-Finkel, J.; Allo, M. Statin therapy is not associated with improved vascular access outcomes. Clin. J. Am. Soc. Nephrol. 2010, 5, 1447–1450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, H.H.; Chang, Y.K.; Lu, C.W.; Huang, C.T.; Chien, C.T.; Hung, K.Y.; Huang, K.C.; Hsu, C.C. Statins Improve Long Term Patency of Arteriovenous Fistula for Hemodialysis. Sci. Rep. 2016, 6, 22197. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.W.; Hsu, L.W.; Chang, H.Y.; Huang, T.C.; Yu, J.R.; Liao, H.Y.; Lee, C.H.; Liu, P.Y. Elevated Platelet Galectin-3 and Rho-Associated Protein Kinase Activity Are Associated with Hemodialysis Arteriovenous Shunt Dysfunction among Subjects with Diabetes Mellitus. Biomed. Res. Int. 2019, 2019, 8952414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huijbregts, H.J.; Bots, M.L.; Wittens, C.H.; Schrama, Y.C.; Moll, F.L.; Blankestijn, P.J. Hemodialysis arteriovenous fistula patency revisited: Results of a prospective, multicenter initiative. Clin. J. Am. Soc. Nephrol. 2008, 3, 714–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schöttker, B.; Herder, C.; Rothenbacher, D.; Roden, M.; Kolb, H.; Müller, H.; Brenner, H. Proinflammatory cytokines, adiponectin, and increased risk of primary cardiovascular events in diabetic patients with or without renal dysfunction: Results from the ESTHER study. Diabetes Care 2013, 36, 1703–1711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lok, C.E.; Huber, T.S.; Lee, T.; Shenoy, S.; Yevzlin, A.S.; Abreo, K.; Allon, M.; Asif, A.; Astor, B.C.; Glickman, M.H.; et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am. J. Kidney Dis. 2020, 75 (Suppl. S2), S1–S164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nalesso, F.; Garzotto, F.; Petrucci, I.; Samoni, S.; Virzì, G.M.; Gregori, D.; Meola, M.; Ronco, C. Standardized Protocol for Hemodialysis Vascular Access Assessment: The Role of Ultrasound and ColorDoppler. Blood Purif. 2018, 45, 260–269. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients without | Patients with | p Value | |
|---|---|---|---|
| AVF Dysfunction | AVF Dysfunction | ||
| (n = 244) | (n = 38) | ||
| Age (year) | 60.7 ± 13.3 | 63.4 ± 11.3 | 0.162 |
| Male (n, %) | 162 (66.4) | 28 (73.7) | 0.373 |
| Body mass index (kg/m2) | 23.6 ± 5.5 | 23.7 ± 5.0 | 0.836 |
| Dialysis vintage (year) a | 2.1 (0.7, 4.9) | 1.7 (0.6, 3.8) | 0.203 |
| Charlson comorbidity index | 4.0 ± 1.6 | 4.3 ± 1.3 | 0.019 |
| Diabetes mellitus (n, %) | 134 (54.9) | 27 (71.1) | 0.062 |
| Previous history of CVD (n, %) b | 218 (89.3) | 36 (94.7) | 0.301 |
| Pre-dialysis systolic BP (mmHg) | 145.4 ± 20.0 | 136.8 ± 18.3 | 0.013 |
| Location of AVF (n, %) c | |||
| Forearm | 186 (76.5) | 26 (68.4) | 0.279 |
| Upper arm | 57 (23.5) | 12 (31.6) | |
| AVF vintage (year) a | 2.21 (0.7–4.0) | 2.08 (0.6–3.9) | 0.656 |
| Ultrafiltration (L/session) | 2.27 ± 1.04 | 2.46 ± 1.00 | 0.310 |
| Single pool Kt/V | 1.59 ± 0.29 | 1.56 ± 0.28 | 0.561 |
| Blood flow rate (mL/min) | 269.0 ± 22.1 | 269.0 ± 28.6 | 0.964 |
| Hemodialysis duration (h) | 3.91 ± 0.21 | 3.94 ± 0.16 | 0.301 |
| Hemodiafiltration (n, %) | 56 (23.0) | 14 (36.8) | 0.065 |
| Statin use (n, %) | 106 (43.4) | 25 (65.8) | 0.010 |
| Anti-platelet agent use (n, %) | 173 (70.9) | 28 (73.7) | 0.724 |
| Erythropoiesis-stimulating agent use (%) | 226 (92.6) | 32 (84.2) | 0.084 |
| Hemoglobin (g/dL) | 10.4 ± 1.2 | 10.5 ± 1.4 | 0.834 |
| Intact parathyroid hormone (pg/dL) | 290.6 ± 228.2 | 196.4 ± 158.1 | 0.015 |
| Calcium (mg/dL) | 8.52 ± 0.83 | 8.51 ± 0.75 | 0.934 |
| Phosphorus (mg/dL) | 4.91 ± 1.34 | 4.36 ± 1.55 | 0.023 |
| Albumin (mg/dL) | 3.83 ± 0.30 | 3.77 ± 0.36 | 0.231 |
| Alkaline phosphatase (mg/dL) | 109.1 ± 78.9 | 104.3 ± 57.5 | 0.926 |
| LDL-cholesterol (mg/dL) | 77.1 ± 24.6 | 76.2 ± 31.0 | 0.842 |
| Erythrocyte sedimentation rate (mm/h) | 30.4 ± 22.7 | 33.0 ± 23.1 | 0.630 |
| hs-CRP (mg/dL) a | 0.80 (0.17–3.04) | 0.90 (0.45–3.13) | 0.518 |
| IL-6 (pg/mL) a | 2.76 (1.93–4.62) | 3.96 (2.58–7.56) | 0.009 |
| MCP-1 (pg/mL) a | 167.26 (133.42–216.58) | 154.25 (118.80–200.67) | 0.149 |
| TNF-α (pg/mL) a | 9.83 (6.36–13.23) | 10.15 (5.83–13.70) | 0.962 |
| Univariable Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | ||
| Age (year) | 1.02 (0.99–1.04) | 0.232 | |||
| Sex (male) | 1.42 (0.66–3.06) | 0.374 | |||
| Diabetes mellitus | 2.02 (0.96–4.25) | 0.065 | 2.20 (1.00–4.86) | 0.049 | |
| Charlson comorbidity index | 1.15 (0.93–1.43) | 0.192 | |||
| AVF vintage (year) | 0.97 (0.87–1.08) | 0.585 | |||
| Systolic BP (per 10 mmg decrease) | 1.27 (1.06–1.52) | 0.01 | 1.34 (1.10–1.19) | 0.003 | |
| Anti-platelet agent use | 1.15 (0.53–2.50) | 0.725 | |||
| Statin use | 2.50 (1.22–5.13) | 0.012 | 2.76 (1.28–5.93) | 0.01 | |
| Albumin (mg/dL) | 0.52 (0.18–1.51) | 0.231 | |||
| Calcium (> 9.5 mg/dL) | 0.71 (0.23–2.75) | 0.706 | |||
| Phosphorus (> 5.5 mg/dL) | 0.73 (0.19–1.07) | 0.073 | 0.48 (0.20–1.19) | 0.113 | |
| hs-CRP (log) | 1.05 (0.88–1.25) | 0.6 | |||
| IL-6 (pg/mL) | tertile1 | Ref | - | Ref | - |
| tertile2 | 2.17 (0.82–5.70) | 0.117 | 2.34 (0.85–6.44) | 0.099 | |
| tertile3 | 3.12 (1.24–7.87) | 0.016 | 3.58 (1.36–9.40) | 0.01 | |
| No. of Events (%) | Crude HR (95% CI) | p-Value | Adjusted HR (95% CI) a | p-Value | |
|---|---|---|---|---|---|
| IL-6 Tertile 1 | 7/98 (7.1%) | Reference | Reference | ||
| IL-6 Tertile 2 | 13/91 (14.3%) | 2.04 (0.81–5.12) | 0.128 | 1.99 (0.79–5.00) | 0.144 |
| IL-6 Tertile 3 | 18/93 (19.4%) | 2.86 (1.20–6.86) | 0.018 | 3.06 (1.25–7.49) | 0.015 |
| No. of Events (%) | Crude HR (95% CI) | p-Value | Adjusted HR (95% CI) a | p-Value | p for Interaction | |
|---|---|---|---|---|---|---|
| 0.953 | ||||||
| Low IL-6, without DM | 2/59 (3.4%) | Reference | - | Reference | ||
| High IL-6, without DM | 9/62 (14.5%) | 4.49 (0.97–20.79) | 0.055 | 4.81 (1.02–22.64) | 0.047 | |
| Low IL-6, with DM | 11/82 (13.4%) | 4.04 (0.90–18.24) | 0.069 | 4.36 (0.87–21.94) | 0.074 | |
| High IL-6, with DM | 16/79 (20.3%) | 6.38 (1.47–27.76) | 0.013 | 7.53 (1.49–38.15) | 0.015 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, J.; Lee, H.; Yang, T.; Lee, S.-Y.; Kim, Y.G.; Kim, J.S.; Ahn, S.; Kim, K.; Kang, S.H.; Lee, M.-J.; et al. Plasma Interleukin-6 Level Predicts the Risk of Arteriovenous Fistula Dysfunction in Patients Undergoing Maintenance Hemodialysis. J. Pers. Med. 2023, 13, 151. https://doi.org/10.3390/jpm13010151
Baek J, Lee H, Yang T, Lee S-Y, Kim YG, Kim JS, Ahn S, Kim K, Kang SH, Lee M-J, et al. Plasma Interleukin-6 Level Predicts the Risk of Arteriovenous Fistula Dysfunction in Patients Undergoing Maintenance Hemodialysis. Journal of Personalized Medicine. 2023; 13(1):151. https://doi.org/10.3390/jpm13010151
Chicago/Turabian StyleBaek, Jihyun, Hyeyeon Lee, Taeyoung Yang, So-Young Lee, Yang Gyun Kim, Jin Sug Kim, ShinYoung Ahn, Kipyo Kim, Seok Hui Kang, Min-Jeong Lee, and et al. 2023. "Plasma Interleukin-6 Level Predicts the Risk of Arteriovenous Fistula Dysfunction in Patients Undergoing Maintenance Hemodialysis" Journal of Personalized Medicine 13, no. 1: 151. https://doi.org/10.3390/jpm13010151
APA StyleBaek, J., Lee, H., Yang, T., Lee, S. -Y., Kim, Y. G., Kim, J. S., Ahn, S., Kim, K., Kang, S. H., Lee, M. -J., Lee, D. -Y., Jeong, H. Y., & Lee, Y. H. (2023). Plasma Interleukin-6 Level Predicts the Risk of Arteriovenous Fistula Dysfunction in Patients Undergoing Maintenance Hemodialysis. Journal of Personalized Medicine, 13(1), 151. https://doi.org/10.3390/jpm13010151