
Treatment of Acute Mesenteric Ischemia: Individual Challenges for Interventional Radiologists and Abdominal Surgeons

 , , , ,
, , , ,
Abstract
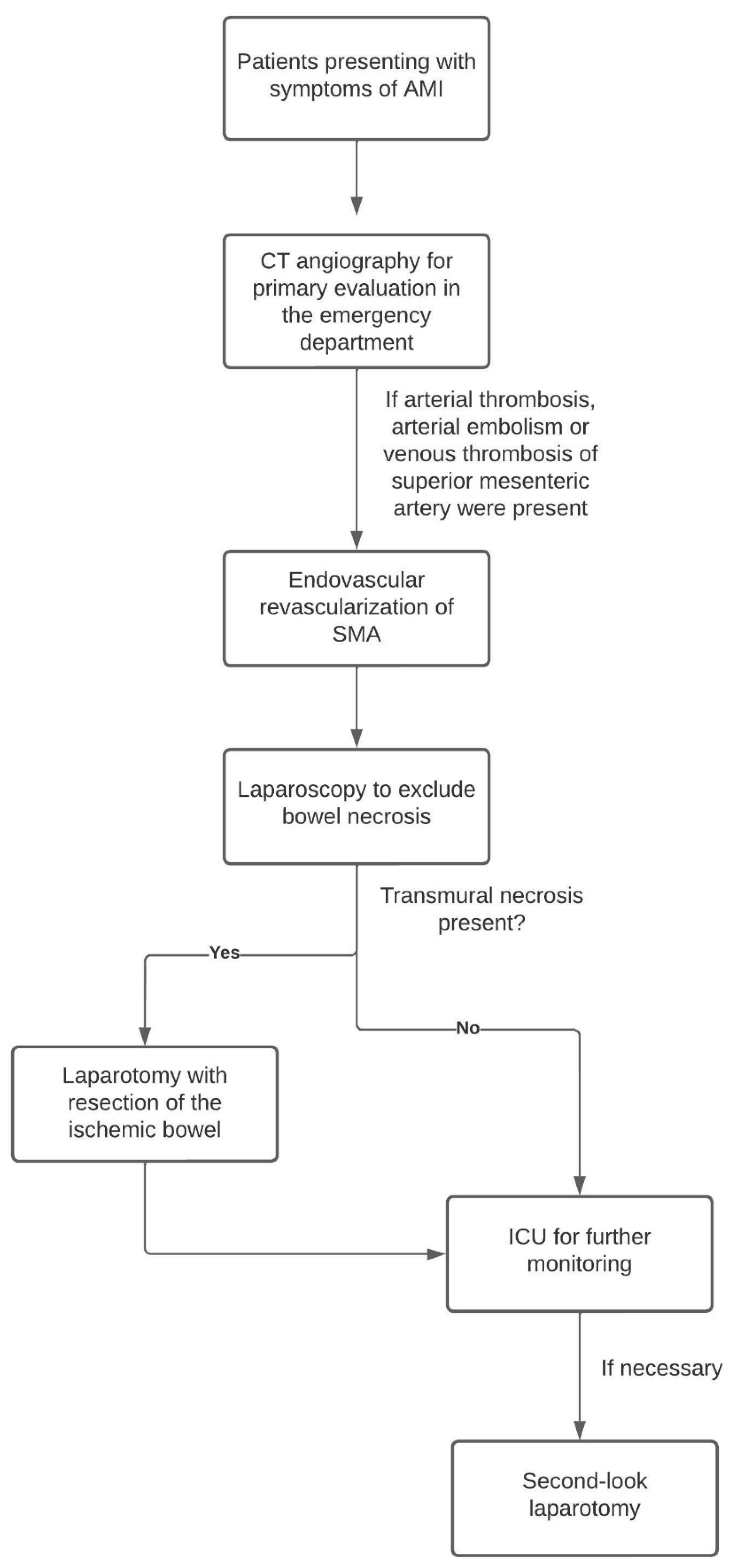
:1. Introduction
2. Material and Methods
2.1. Endovascular Procedure
2.2. Surgery
2.3. Anticoagulation
2.4. Outcome Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Patel, A.; Kaleya, R.N.; Sammartano, R.J. Pathophysiology of mesenteric ischemia. Surg. Clin. N. Am. 1992, 72, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.-W.; Chang, J.-B.; Longo, W.-E. Update in management of mesenteric ischemia. World J. Gastroenterol. 2006, 12, 3243–3247. [Google Scholar] [CrossRef] [PubMed]
- Horton, K.M.; Fishman, E.K. Multidetector CT angiography in the diagnosis of mesenteric ischemia. Radiol. Clin. N. Am. 2007, 45, 275–288. [Google Scholar] [CrossRef]
- Schoots, I.G.; Koffeman, G.I.; Legemate, D.A.; Levi, M.; Van Gulik, T.M. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. Br. J. Surg. 2004, 91, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, R.J.; Arnaoutakis, K.D.; Abularrage, C.J.; Efron, D.T.; Schneider, E.; Black, J.H., III. Comparison of open and endovascular treatment of acute mesenteric ischemia. J. Vasc. Surg. 2014, 59, 159–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acosta, S. Mesenteric Ischemia. Curr. Opin. Crit. Care 2015, 21, 171–178. Available online: https://journals.lww.com/co-criticalcare/Fulltext/2015/04000/Mesenteric_ischemia.12.aspx (accessed on 21 April 2015). [CrossRef]
- Clair, D.G.; Beach, J.M. Mesenteric Ischemia. N. Engl. J. Med. 2016, 374, 959–968. [Google Scholar] [CrossRef] [Green Version]
- Kundan, M.; Chebrolu, H.; Muniswamppa, C.; Kumar, N.; Chintamani, C.; Varma, V. Outcomes of Management of Patients with Acute Mesenteric Ischemia: A Prospective Study. Niger. J. Surg. Off. Publ. Niger. Surg. Res. Soc. 2021, 27, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Kärkkäinen, J.M.; Acosta, S. Acute mesenteric ischemia (part I)—Incidence, etiologies, and how to improve early diagnosis. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 15–25. [Google Scholar] [CrossRef]
- Bala, M.; Kashuk, J.; Moore, E.E.; Kluger, Y.; Biffl, W.; Gomes, C.A.; Ben-Ishay, O.; Rubinstein, C.; Balogh, Z.J.; Civil, I.; et al. Acute mesenteric ischemia: Guidelines of the World Society of Emergency Surgery. World J. Emerg. Surg. WJES 2017, 12, 38. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Yoo, A.J.; Khatri, P.; Tomsick, T.A.; von Kummer, R.; Saver, J.L.; Marks, M.P.; Prabhakaran, S.; Kallmes, D.F.; Fitzsimmons, B.-F.M. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: A consensus statement. Stroke 2013, 44, 2650–2663. [Google Scholar] [CrossRef] [Green Version]
- Pedersoli, F.; Schönau, K.; Schulze-Hagen, M.; Keil, S.; Isfort, P.; Gombert, A.; Alizai, P.H.; Kuhl, C.K.; Bruners, P.; Zimmermann, M.; et al. Endovascular Revascularization with Stent Implantation in Patients with Acute Mesenteric Ischemia due to Acute Arterial Thrombosis: Clinical Outcome and Predictive Factors. Cardiovasc. Interv. Radiol. 2021, 44, 1030–1038. [Google Scholar] [CrossRef]
- Kanasaki, S.; Furukawa, A.; Fumoto, K.; Hamanaka, Y.; Ota, S.; Hirose, T.; Inoue, A.; Shirakawa, T.; Nguyen, L.D.H.; Tulyeubai, S. Acute Mesenteric Ischemia: Multidetector CT Findings and Endovascular Management. Radiogr. A Rev. Publ. Radiol. Soc. N. Am. 2018, 38, 945–961. [Google Scholar] [CrossRef]
- Wadman, M.; Syk, I.; Elmståhl, S. Survival after operations for ischaemic bowel disease. Eur. J. Surg. Acta Chir. 2000, 166, 872–877. [Google Scholar] [CrossRef]
- Block, T.A.; Acosta, S.; Björck, M. Endovascular and open surgery for acute occlusion of the superior mesenteric artery. J. Vasc. Surg. 2010, 52, 959–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klar, E.; Rahmanian, P.B.; Bücker, A.; Hauenstein, K.; Jauch, K.W.; Luther, B. Acute mesenteric ischemia: A vascular emergency. Dtsch. Arztebl. Int. 2012, 109, 249–256. [Google Scholar] [PubMed]
- Emile, S.H. Predictive Factors for Intestinal Transmural Necrosis in Patients with Acute Mesenteric Ischemia. World J. Surg. 2018, 42, 2364–2372. [Google Scholar] [CrossRef]
- Canfora, A.; Ferronetti, A.; Marte, G.; di Maio, V.; Mauriello, C.; Maida, P.; Bottino, V.; Aprea, G.; Amato, B. Predictive Factors of Intestinal Necrosis in Acute Mesenteric Ischemia. Open Med. (Wars. Pol.) 2019, 14, 883–889. [Google Scholar] [CrossRef]
- Caluwaerts, M.; Castanares-Zapatero, D.; Laterre, P.-F.; Hantson, P. Prognostic factors of acute mesenteric ischemia in ICU patients. BMC Gastroenterol. 2019, 19, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grotelüschen, R.; Bergmann, W.; Welte, M.N.; Reeh, M.; Izbicki, J.R.; Bachmann, K. What predicts the outcome in patients with intestinal ischemia? A single center experience. J. Visc. Surg. 2019, 156, 405–411. [Google Scholar] [CrossRef]
- Oderich, G.S.; Macedo, R.; Stone, D.H.; Woo, E.Y.; Panneton, J.M.; Resch, T.; Dias, N.V.; Sonesson, B.; Schermerhorn, M.L.; Lee, J.T.; et al. Multicenter study of retrograde open mesenteric artery stenting through laparotomy for treatment of acute and chronic mesenteric ischemia. J. Vasc. Surg. 2018, 68, 470–480.e1. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (mean years ± SD) | 71.8 ± 14.4 |
| BMI (mean kg/m2 ± SD) | 25.8 ± 5.3 |
| Sex (m/f) | 32 females (55.2%) 26 males (44.8%) |
| Coronary heart disease present? | n = 25 (43.1%) |
| Hypertension present? | n = 33 (56.9%) |
| Diabetes present? | n = 11 (19.0%) |
| Atrial fibrillation present? | n = 21 (36.2%) |
| Chronic peripheral arterial occlusive disease present? | n = 15 (25.9%) |
| Dialysis present? | n = 9 (15.5%) |
| Access Vessel | |
| n = 31 (53.4%) |
| n = 27 (46.6%) |
| Sheath size | |
| n = 1 (1.7%) |
| n = 3 (5.2%) |
| n = 52 (89.6%) |
| n = 2 (3.4%) |
| Complications | |
| n = 0 (0%) |
| n = 0 (0%) |
| Administered Heparin during procedure | |
| n = 2 (3.4%) |
| n = 25 (60.3%) |
| n = 3 (5.2%) |
| n = 1 (1.7%) |
| n = 17 (29.3%) |
| Pre-interventional imaging | |
| n = 58 (100%) |
| Extent of bowel ischemia on CT | |
| n = 22 (37.9%) |
| n = 4 (6.9%) |
| n = 26 (44.8%) |
| n = 4 (6.9%) |
| n = 0 (0%) |
| n = 0 (0%) |
| Pre-existing AMS stenosis | |
| n = 43 (74.1%) |
| n = 15 (25.9%) |
| Type of occlusion | |
| n = 30 (51.7%) |
| n = 22 (37.9%) |
| n = 4 (6.9%) |
| n = 2 (3.4%) |
| Time onset of symptoms to intervention (mean min ± SD) | |
| 222 min ± 166 min | |
| Method(s) of recanalization | |
| n = 16 (27.6%) |
| n = 21 (36.2%) |
| n = 2 (3.4%) |
| n = 28 (48.3%) |
| n = 32 (55.2%) |
| Additional | |
| n = 31 (53.4%) |
| n = 14 (24.1%) |
TICI AMI before recanalization
| n = 2 (3.4%) n = 24 (41.4%) n = 25 (43.1%) n = 6 (10.3%) n = 1 (1.7%) n = 0 (0%) |
TICI AMI after recanalization
| n = 0 (0%) n = 4 (6.9%) n = 3 (5.2%) n = 17 (29.3%) n = 19 (32.8%) n = 15 (25.9%) |
| Time interval between end of intervention and start of laparoscopy (mean min ± SD) | 71 min ± 42 min |
Bowel ischemia in laparoscopy
| n = 32 (55.2%) n = 26 (44.8%) |
Extend of bowel resection
| Mean about 110 cm n = 5 n = 3 |
| Death | Chi2 | p-Value |
|---|---|---|
| Aetiology of mesenteric ischemia | 2.52 | 0.28 |
| Extent of intestinal ischemia | 12.25 | 0.006 |
| Resection of colon | 1.37 | 0.24 |
| Patient history of coronary heart disease | 0.76 | 0.09 |
| Patient history of hypertension | 0.51 | 0.43 |
| Patient history of diabetes | 0.38 | 0.54 |
| Patient history of atrial fibrillation | 0.49 | 0.48 |
| Patient history of chronic peripheral occlusive disease | 0.6 | 0.44 |
| Patient history of dialysis | 0.55 | 0.46 |
| Correlation | Time from Symptom Onset | Survival | Resection of Ileum |
|---|---|---|---|
| Time from symptom onset | x | r = −0.220, p = 0.043 | r = −0.047, p = 0.73 |
| Survival | r = −0.220, p = 0.043 | x | r = 0.316, p = 0.01 |
| Resection of ileum | r = −0.047, p = 0.73 | r = 0.316, p = 0.01 | x |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Estler, A.; Estler, E.; Feng, Y.-S.; Seith, F.; Wießmeier, M.; Archid, R.; Nikolaou, K.; Grözinger, G.; Artzner, C. Treatment of Acute Mesenteric Ischemia: Individual Challenges for Interventional Radiologists and Abdominal Surgeons. J. Pers. Med. 2023, 13, 55. https://doi.org/10.3390/jpm13010055
Estler A, Estler E, Feng Y-S, Seith F, Wießmeier M, Archid R, Nikolaou K, Grözinger G, Artzner C. Treatment of Acute Mesenteric Ischemia: Individual Challenges for Interventional Radiologists and Abdominal Surgeons. Journal of Personalized Medicine. 2023; 13(1):55. https://doi.org/10.3390/jpm13010055
Chicago/Turabian StyleEstler, Arne, Eva Estler, You-Shan Feng, Ferdinand Seith, Maximilian Wießmeier, Rami Archid, Konstantin Nikolaou, Gerd Grözinger, and Christoph Artzner. 2023. "Treatment of Acute Mesenteric Ischemia: Individual Challenges for Interventional Radiologists and Abdominal Surgeons" Journal of Personalized Medicine 13, no. 1: 55. https://doi.org/10.3390/jpm13010055
APA StyleEstler, A., Estler, E., Feng, Y. -S., Seith, F., Wießmeier, M., Archid, R., Nikolaou, K., Grözinger, G., & Artzner, C. (2023). Treatment of Acute Mesenteric Ischemia: Individual Challenges for Interventional Radiologists and Abdominal Surgeons. Journal of Personalized Medicine, 13(1), 55. https://doi.org/10.3390/jpm13010055