

Influence of Moisturizers on Skin Microcirculation: An Assessment Study Using Laser Speckle Contrast Imaging

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Committee
2.2. Power Analysis
2.3. Scar-Like Model
2.3.1. Participant Recruitment
2.3.2. Tape Stripping Procedure
2.3.3. Product Application and Measurements
2.4. Research Equipment
2.4.1. Laser Speckle Contrast Imaging (LSCI)
2.4.2. Tewameter TM 300®
2.4.3. Corneometer CM 825®
2.4.4. Products
2.5. Statistical Analysis
3. Results
3.1. Participants
3.2. Environmental Conditions
3.3. Objective Measurements
3.3.1. Occlusive Properties
Mean TEWL
Mean Percentage Reduction (MPR)
- where:
- i = ith volunteer
- n = total number of volunteers
- T(i,t) = TEWL of volunteer i at time t in hours
- T(i,0) = TEWL of volunteer i at baseline, after acclimatization
- T(i,1) = TEWL of volunteer i post-tape stripping, application time
- MPR(t) = Mean Percentage Reduction at t hours post-application
3.3.2. Skin Hydration
Mean Hydration Values
Cumulative Absolute Added Hydration
- where:
- i = i-th volunteer
- n = total number of volunteers
- HP(i,t) = hydration after application of product P of volunteer i at time t in hours, which indicates that HP(i,0) = hydration after application of product P of volunteer i at application time, and that HP(i,1) = hydration after application of Product P of volunteer i 1 h after application
- HSC(i,t) = hydration of the stripped control site of volunteer i at time t in hours, which indicates that HSC(i,0) = hydration of the stripped control site of volunteer i at application time
- CAAH(t′) = Cumulative Added Hydration at t hours post-application in arbitrary units (A.U.).
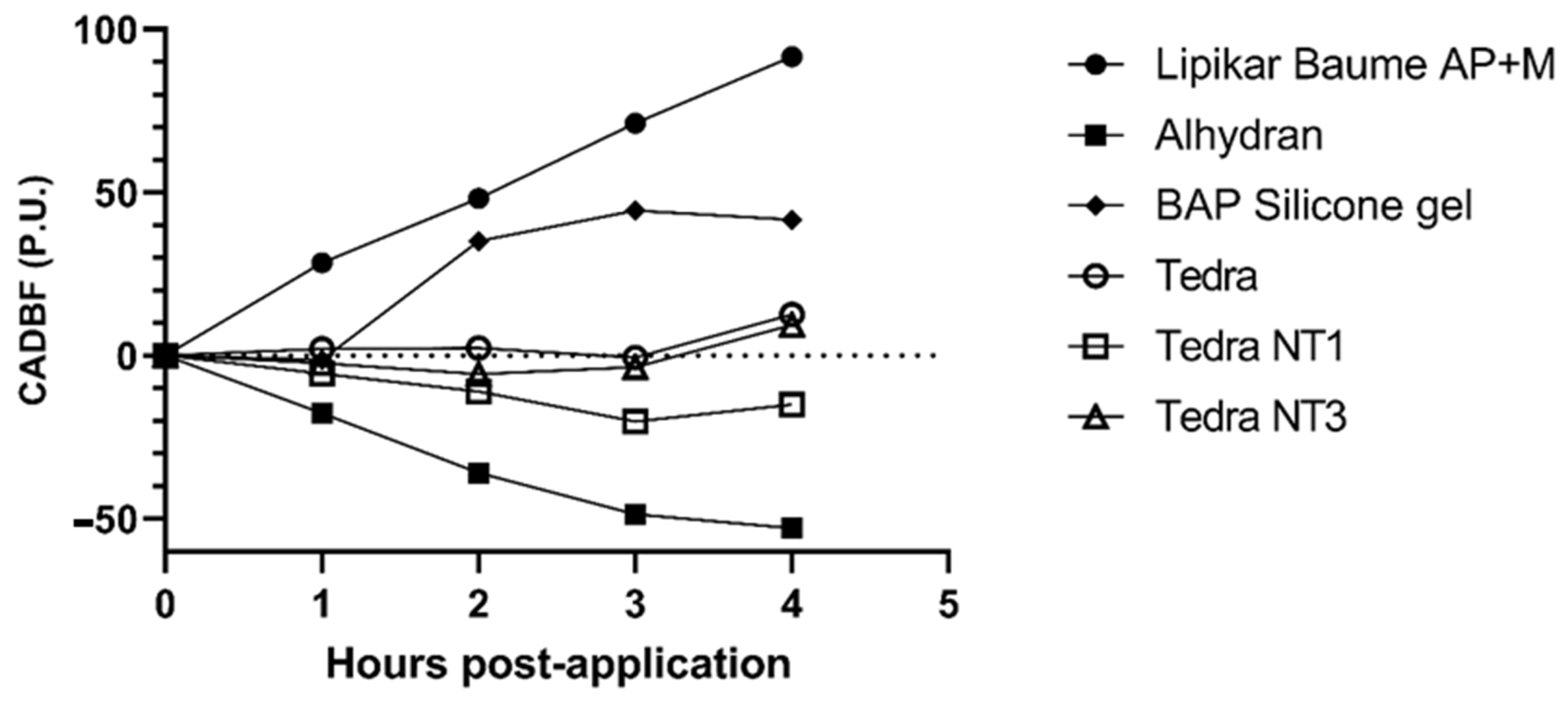
3.3.3. Microcirculatory Changes
Mean Perfusion Units
Cumulative Absolute Difference in Blood Flow
- where:
- i = i-th volunteer
- n = total number of volunteers
- PP(i,t) = perfusion after application of product P of volunteer i at time t in hours, which indicates that PP(i,0) = perfusion after application of Product P of volunteer i at application time and that PP(i,1) = perfusion after application of Product P of volunteer i 1 h after application
- PSC(i,t) = perfusion of the stripped control site of volunteer i at time t in hours, which indicates that PSC(i,0) = perfusion of the stripped control site of volunteer i at application time
- CADBF(t′) = Cumulative Absolute Difference in Blood Flow at t hours post-application in arbitrary perfusion units [P.U.].
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Alhydran® | Function | Lipikar® | Function | TEDRA® | Function | BAP Scar Care® Silicone Gel | Function |
|---|---|---|---|---|---|---|---|
| Aloe Barbadensis Leaf Juice (Aloe Vera gel from Aruba) | Moisturizer | Aqua/Water | Solvent | Aqua | Solvent | Poly-siloxanes | Occlusive, enhance spread ability |
| Water | Solvent | Butyrospermum Parkii Butter/Shea Butter | Moisturizer | Glycerin | Humectant | Vitamin E | Antioxidant |
| Ceteraryl Alcohol | Emollient | Glycerin | Humectant | Ceteraryl ethyl-hexanoate | Emollient | ||
| Caprylic/Capric Triglyceride | Emollient | Dimethicone | Occlusive | C14–22 Alcohols | Emollient | ||
| Decyl Oleate | Emollient | Niacinamide | Vitamin B3 | C10–18 Triglycerides | Emollient | ||
| Glyceryl Stearate | Emulsifier | Paraffin Liquid/Mineral Oil | Occlusive | Sodium Polyacrylate | Thickening agent | ||
| Cetearyl Isonoanoate | Emollient | Cetearyl Alcohol | Emollient | Dimethicone | Occlusive | ||
| Sorbitan Stearate | Emulsifier | Rapeseed Oil (Brassica Campestris Oleifera Oil) | Moisturizer | Phenoxyethanol | Preservative | ||
| Ceteareth-20 | Emulsifier | Ammonium Polyacryldimethyltauramide/Ammonium Polyacryloyldimethyl Taurate | Thickening agent | Tocopheryl Acetate—Vitamin E | Antioxidant | ||
| Propylene Glycol | Humectant | PEG-100 Stearate | Emulsifier | C12–20 Alkyl Glucoside | Emulsifier | ||
| Phenoxyethanol | Preservative | Glyceryl Stearate | Emulsifier | Caprylyl Glycol | Preservative | ||
| Ceteareth-12 | Emulsifier | Peg-20 Methyl Glucose Sesquistearate | Emulsifier | Chorphenesin | Preservative | ||
| Cetyl Palmitate | Emollient | Cera Microcristallina/Microcrystalline Wax | Binding Agent | Dimethiconol | Texture/Spread ability | ||
| Caprylyl Glycol | Humectant | Paraffin | Occlusive | Hydrochloric Acid | pH adjustment (Stability) | ||
| Chlorphenesin | Preservative | Sorbitan Tristearate | Emulsifier | Trideceth-6 | Emulsifier | ||
| Tocopheryl Acetate—Vitamin E | Antioxidant | Dimethiconol | Texture/Spread ability | Manganese Chloride Tetrahydrate | * | ||
| Ascorbic Acid—Vitamin C | Antioxidant | Mannose | Moisturizer | Potassium Chloride | Fluid Balance | ||
| Jojoba Oil (Simmondsia Chinensis Seed Oil) | Emollient | Disodium EDTA | Chelating agent (adds stability) | Sodium Metasilicate Pentahydrate | * | ||
| Disodium EDTA | Chelating agent (adds stability) | Capryloyl Glycine | Antimicrobial | Magnesium Chloride Hexahydrate | * | ||
| Vitreoscilla Ferment | Moisturizer | Lithium Chloride | * | ||||
| Xanthan Gum | Thickening Agent | ||||||
| Pentaerythrityl Tetra-Di-T-Butyl Hydroxy-hydrocinnamate | Antioxidant (stability) | ||||||
| Sodium Benzoate | Preservative |
References
- Klotz, T.; Kurmis, R.; Munn, Z.; Heath, K.; Greenwood, J. Moisturisers in scar management following burn: A survey report. Burns 2017, 43, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Wolfram, D.; Tzankov, A.; Pülzl, P.; Piza-Katzer, H. Hypertrophic scars and keloids—A review of their pathophysiology, risk factors, and therapeutic management. Dermatol. Surg. 2009, 35, 171–181. [Google Scholar] [CrossRef]
- Suetake, T.; Sasai, S.; Zhen, Y.X.; Ohi, T.; Tagami, H. Functional analysis of the stratum corneum in scars. Arch. Dermatol. 1996, 132, 1453–1458. [Google Scholar] [CrossRef] [PubMed]
- Basson, R.; Baguneid, M.; Foden, P.; Al Kredly, R.; Bayat, A. Functional Testing of a Skin Topical Formulation In Vivo: Objective and Quantitative Evaluation in Human Skin Scarring Using a Double-Blind Volunteer Study with Sequential Punch Biopsies. Adv. Wound Care 2019, 8, 208–219. [Google Scholar] [CrossRef] [PubMed]
- Mustoe, T.A. Evolution of Silicone Therapy and Mechanism of Action in Scar Management. Aesthetic Plast. Surg. 2008, 32, 82–92. [Google Scholar] [CrossRef] [PubMed]
- O’Shaughnessy, K.D.; De La Garza, M.; Roy, N.K.; Mustoe, T.A. Homeostasis of the epidermal barrier layer: A theory of how occlusion reduces hypertrophic scarring. Wound Repair Regen. 2009, 17, 700–708. [Google Scholar] [CrossRef] [PubMed]
- De Decker, I.; Hoeksema, H.; Verbelen, J.; Vanlerberghe, E.; De Coninck, P.; Speeckaert, M.M.; Blondeel, P.; Monstrey, S.; Claes, K.E. The use of fluid silicone gels in the prevention and treatment of hypertrophic scars: A systematic review and meta-analysis. Burns 2022, 48, 491–509. [Google Scholar] [CrossRef]
- Akdeniz, M.; Gabriel, S.; Lichterfeld-Kottner, A.; Blume-Peytavi, U.; Kottner, J. Transepidermal water loss in healthy adults: A systematic review and meta-analysis update. Br. J. Dermatol. 2018, 179, 1049–1055. [Google Scholar] [CrossRef]
- Alexander, H.; Brown, S.; Danby, S.; Flohr, C. Research Techniques Made Simple: Transepidermal Water Loss Measurement as a Research Tool. J. Investig. Dermatol. 2018, 138, 2295–2300.e1. [Google Scholar] [CrossRef] [PubMed]
- Fluhr, J.W.; Feingold, K.R.; Elias, P.M. Transepidermal water loss reflects permeability barrier status: Validation in human and rodent in vivo and ex vivo models. Exp. Dermatol. 2006, 15, 483–492. [Google Scholar] [CrossRef]
- Berardesca, E.; Loden, M.; Serup, J.; Masson, P.; Rodrigues, L.M. The revised EEMCO guidance for the in vivo measurement of water in the skin. Ski. Res. Technol. 2018, 24, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Tandara, A.A.; Kloeters, O.; Mogford, J.E.; Mustoe, T.A. Hydrated keratinocytes reduce collagen synthesis by fibroblasts via paracrine mechanisms. Wound Repair Regen. 2007, 15, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Tandara, A.A.; Mustoe, T.A. MMP- and TIMP-secretion by human cutaneous keratinocytes and fibroblasts—Impact of coculture and hydration. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Yu, J.; Xu, Y.; Chen, L.; Zhou, F.; Zhai, Q.; Wu, J.; Shu, B.; Qi, S. Epidermal HMGB1 Activates Dermal Fibroblasts and Causes Hypertrophic Scar Formation in Reduced Hydration. J. Investig. Dermatol. 2018, 138, 2322–2332. [Google Scholar] [CrossRef]
- Breternitz, M.; Flach, M.; Präßler, J.; Elsner, P.; Fluhr, J. Acute barrier disruption by adhesive tapes is influenced by pressure, time and anatomical location: Integrity and cohesion assessed by sequential tape stripping; a randomized, controlled study. Br. J. Dermatol. 2007, 156, 231–240. [Google Scholar] [CrossRef]
- De Decker, I.; Hoeksema, H.; Vanlerberghe, E.; Beeckman, A.; Verbelen, J.; De Coninck, P.; Speeckaert, M.M.; Blondeel, P.; Monstrey, S.; Claes, K.E. Occlusion and hydration of scars: Moisturizers versus silicone gels. Burns 2023, 49, 365–379. [Google Scholar] [CrossRef]
- De Paepe, K.; Sieg, A.; Le Meur, M.; Rogiers, V. Silicones as non-occlusive topical agents. Pharm. Ind. 2015, 77, 164–171. [Google Scholar]
- Hoeksema, H.; De Vos, M.; Verbelen, J.; Pirayesh, A.; Monstrey, S. Scar management by means of occlusion and hydration: A comparative study of silicones versus a hydrating gel-cream. Burns 2013, 39, 1437–1448. [Google Scholar] [CrossRef]
- Lodén, M. Barrier recovery and influence of irritant stimuli in skin treated with a moisturizing cream. Contact Dermat. 1997, 36, 256–260. [Google Scholar] [CrossRef]
- Mortz, C.G.; Andersen, K.E.; Halkier-Sorensen, L. The efficacy of different moisturizers on barrier recovery in hairless mice evaluated by non-invasive bioengineering methods. Contact Dermat. 1997, 36, 297–301. [Google Scholar] [CrossRef]
- Atiyeh, B.S.; El Khatib, A.M.; Dibo, S.A. Pressure garment therapy (PGT) of burn scars: Evidence-based efficacy. Ann. Burn. fire disasters 2013, 26, 205–212. [Google Scholar]
- Powell, H.M.; Nedelec, B. Mechanomodulation of Burn Scarring Via Pressure Therapy. Adv. Wound Care 2022, 11, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Liu, Y.; Huang, Y.; Xie, Y.; Shen, K.; Zhang, D.; Mou, Y. Mechanical compression upregulates MMP9 through SMAD3 but not SMAD2 modulation in hypertrophic scar fibroblasts. Connect. Tissue Res. 2014, 55, 391–396. [Google Scholar] [CrossRef]
- Miller, M.-C.; Nanchahal, J. Advances in the Modulation of Cutaneous Wound Healing and Scarring. BioDrugs 2005, 19, 363–381. [Google Scholar] [CrossRef]
- Spielman, A.F.; Griffin, M.F.; Parker, J.; Cotterell, A.C.; Wan, D.C.; Longaker, M.T. Beyond the Scar: A Basic Science Review of Wound Remodeling. Adv. Wound Care 2023, 12, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Sharp, P.A.; Pan, B.; Yakuboff, K.P.; Rothchild, D. Development of a Best Evidence Statement for the Use of Pressure Therapy for Management of Hypertrophic Scarring. J. Burn. Care Res. 2016, 37, 255–264. [Google Scholar] [CrossRef]
- Ai, J.-W.; Liu, J.-T.; Pei, S.-D.; Liu, Y.; Li, D.-S.; Lin, H.-M.; Pei, B. The effectiveness of pressure therapy (15–25 mmHg) for hypertrophic burn scars: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 40185. [Google Scholar] [CrossRef]
- Stewart, C.; Frank, R.; Forrester, K.; Tulip, J.; Lindsay, R.; Bray, R. A comparison of two laser-based methods for determination of burn scar perfusion: Laser Doppler versus laser speckle imaging. Burns 2005, 31, 744–752. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Liu, L.; Yang, R.; Ding, X.; Li, Y.; Liu, H.; Yan, H. Blood perfusion in hypertrophic scars and keloids studied by laser speckle contrast imaging. Ski. Res. Technol. 2021, 27, 789–796. [Google Scholar] [CrossRef]
- Briers, D.; Duncan, D.D.; Hirst, E.; Kirkpatrick, S.J.; Larsson, M.; Steenbergen, W.; Stromberg, T.; Thompson, O.B. Laser speckle contrast imaging: Theoretical and practical limitations. J. Biomed. Opt. 2013, 18, 066018. [Google Scholar] [CrossRef]
- Heeman, W.; Steenbergen, W.; van Dam, G.M.; Boerma, E.C. Clinical applications of laser speckle contrast imaging: A review. J. Biomed. Opt. 2019, 24, 080901. [Google Scholar] [CrossRef]
- Liu, Q.; Wang, X.; Jia, Y.; Long, X.; Yu, N.; Wang, Y.; Chen, B. Increased blood flow in keloids and adjacent skin revealed by laser speckle contrast imaging. Lasers Surg. Med. 2016, 48, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhang, M.; Yu, N.; Zhang, W.; Long, X.; Wang, Y.; Wang, X. Heterogeneous Features of Keloids Assessed by Laser Speckle Contrast Imaging: A Cross-Sectional Study. Lasers Surg. Med. 2021, 53, 865–871. [Google Scholar] [CrossRef]
- Aalm, R.; Jmga, S. Application of Medical Moisture Retention Cream (ALHYDRAN®), A New Option in the Treatment of Venous Eczema. J. Gerontol. Geriatr. Res. 2017, 6, 1000395. [Google Scholar] [CrossRef]
- Navarro-Triviño, F.J.; Ruiz-Villaverde, R. Allergic contact dermatitis caused by caprylic/capric triglyceride from an anti-aging cosmetic cream. Contact Dermat. 2020, 83, 508–510. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Chinchilla, P.; Poveda-Montoyo, I.; González, I.; Silvestre, J.F. Cetearyl isononanoate, an underestimated contact allergen? Contact Dermat. 2018, 79, 243–244. [Google Scholar] [CrossRef] [PubMed]
- Wohlrab, J.; Kreft, D. Niacinamide—Mechanisms of Action and Its Topical Use in Dermatology. Ski. Pharmacol. Physiol. 2014, 27, 311–315. [Google Scholar] [CrossRef]
- Tanno, O.; Ota, Y.; Kitamura, N.; Katsube, T.; Inoue, S. Nicotinamide increases biosynthesis of ceramides as well as other stratum corneum lipids to improve the epidermal permeability barrier. Br. J. Dermatol. 2000, 143, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Soma, Y.; Kashima, M.; Imaizumi, A.; Takahama, H.; Kawakami, T.; Mizoguchi, M. Moisturizing effects of topical nicotinamide on atopic dry skin. Int. J. Dermatol. 2005, 44, 197–202. [Google Scholar] [CrossRef]
- Jones, V.A.; Patel, P.M.; Wilson, C.; Wang, H.; Ashack, K.A. Complementary and alternative medicine treatments for common skin diseases: A systematic review and meta-analysis. JAAD Int. 2021, 2, 76–93. [Google Scholar] [CrossRef] [PubMed]
- Cestari, S.; Correia, P.; Kerob, D. Emollients “Plus” are Beneficial in Both the Short and Long Term in Mild Atopic Dermatitis. Clin. Cosmet. Investig. Dermatol. 2023, 16, 2093–2102. [Google Scholar] [CrossRef] [PubMed]
- Becker, L.C.; Bergfeld, W.F.; Belsito, D.V.; Hill, R.A.; Klaassen, C.D.; Liebler, D.C.; Marks, J.J.G.; Shank, R.C.; Slaga, T.J.; Snyder, P.W.; et al. Safety Assessment of Glycerin as Used in Cosmetics. Int. J. Toxicol. 2019, 38, 6S–22S. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.-R.C.; Moon, H.K. Gravimetric analysis and differential scanning calorimetric studies on glycerin-induced skin hydration. Arch. Pharmacal Res. 2007, 30, 1489–1495. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, L.; Jemec, G. Plasticising effect of water and glycerin on human skin in vivo. J. Dermatol. Sci. 1999, 19, 48–52. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef]
- Klotz, T. The Effect of Moisturisers on Scars: A Systematic Review. Ph.D. Thesis, University of Adelaide, Adelaide, Australia, 2018. [Google Scholar]
- Rodrigues, L.M.; Pinto, P.C.; Magro, J.M.; Fernandes, M.; Alves, J. Exploring the influence of skin perfusion on transepidermal water loss. Ski. Res. Technol. 2004, 10, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Agner, T.; Held, E.; West, W.; Gray, J. Evaluation of an experimental patch test model for the detection of irritant skin reactions to moisturisers. Ski. Res. Technol. 2000, 6, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Forbat, E.; Al-Niaimi, F.; Ali, F.R. Use of nicotinamide in dermatology. Clin. Exp. Dermatol. 2017, 42, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Navarrete-Solís, J.; Castanedo-Cázares, J.P.; Torres-Álvarez, B.; Oros-Ovalle, C.; Fuentes-Ahumada, C.; González, F.J.; Martínez-Ramírez, J.D.; Moncada, B. A Double-Blind, Randomized Clinical Trial of Niacinamide 4% versus Hydroquinone 4% in the Treatment of Melasma. Dermatol. Res. Pract. 2011, 2011, 379173. [Google Scholar] [CrossRef] [PubMed]
- Rolfe, H.M. A review of nicotinamide: Treatment of skin diseases and potential side effects. J. Cosmet. Dermatol. 2014, 13, 324–328. [Google Scholar] [CrossRef]








| Data Overview | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TEDRA® | TEDRA® NT1 | TEDRA® NT3 | Alhydran® | BAP Silicone Gel | Lipikar® Baume | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| MPR in TEWL % (n = 36) | ||||||||||||
| T2 | 44.53 | 19.13 | 47.96 | 31.65 | 45.42 | 35.47 | 36.38 | 33.99 | 28.78 | 44.86 | 41.10 | 26.39 |
| T3 | 45.27 | 23.67 | 55.15 | 32.33 | 49.66 | 38.26 | 45.48 | 19.67 | 29.03 | 37.00 | 42.66 | 36.02 |
| T4 | 41.77 | 31.44 | 45.86 | 29.15 | 39.89 | 40.73 | 36.36 | 26.43 | 25.13 | 43.81 | 37.15 | 43.28 |
| T5 | 45.87 | 23.79 | 46.68 | 42.42 | 48.15 | 46.43 | 36.82 | 30.87 | 23.15 | 57.66 | 43.23 | 31.63 |
| CAAH A.U. (n = 36) | ||||||||||||
| T2 | 25.05 | 13.06 | 24.66 | 14.91 | 23.60 | 14.33 | 3.86 | 12.65 | −9.57 | 16.64 | 8.91 | 16.57 |
| T2–T3 | 47.62 | 25.22 | 48.16 | 29.68 | 46.79 | 28.19 | 6.28 | 21.98 | −9.13 | 26.96 | 19.67 | 32.49 |
| T2–T4 | 71.82 | 38.37 | 72.46 | 45.37 | 71.31 | 41.10 | 6.45 | 32.33 | −6.86 | 35.03 | 33.10 | 46.98 |
| T2–T5 | 96.52 | 53.05 | 97.50 | 59.48 | 95.25 | 53.55 | 5.51 | 41.82 | −2.72 | 41.08 | 52.20 | 59.31 |
| CADBF P.U. (n = 36) | ||||||||||||
| T2 | 2.00 | 36.11 | −5.54 | 37.79 | −2.36 | 43.16 | −17.63 | 42.59 | −1.31 | 50.84 | 28.40 | 51.28 |
| T2–T3 | 2.33 | 60.59 | −10.98 | 70.02 | −5.68 | 85.42 | −35.99 | 75.02 | 35.14 | 256.38 | 48.16 | 79.86 |
| T2–T4 | −0.59 | 100.65 | −20.21 | 121.21 | −3.51 | 142.93 | −48.59 | 117.04 | 44.41 | 261.18 | 71.22 | 103.41 |
| T2–T5 | 12.56 | 118.87 | −14.95 | 141.70 | 9.36 | 174.65 | −52.83 | 136.17 | 41.70 | 269.07 | 91.64 | 124.15 |
| Data Overview | |||||
|---|---|---|---|---|---|
| Reduction of TEWL (n = 36) | Friedman Test p-Value a, b | ||||
| T2 | 0.0176 | ||||
| T3 | 0.0074 | ||||
| T4 | 0.0444 | ||||
| T5 | 0.0441 | ||||
| Post hoc test p-value d | |||||
| Reduction of TEWL T2 c (n = 36) | Reduction of TEWL T3 c (n = 36) | Reduction of TEWL T4 c (n = 36) | Reduction of TEWL T5 c (n = 36) | ||
| TEDRA® vs. Alhydran® | 0.6041 | 0.8969 | 0.2705 | 0.0801 | |
| TEDRA® vs. Lipikar® | 0.5169 | 0.7954 | 0.4758 | 0.5596 | |
| TEDRA® vs. BAP | 0.0381 | 0.0445 | 0.0095 | 0.0165 | |
| TEDRA® vs. TEDRA® NT1 | 0.1360 | 0.0695 | 0.6041 | 0.7954 | |
| TEDRA® vs. TEDRA® NT3 | 0.8458 | 0.4758 | 0.4367 | 0.7459 | |
| Alhydran® vs. Lipikar® | 0.8969 | 0.6973 | 0.6973 | 0.2433 | |
| Alhydran® vs. BAP | 0.1198 | 0.0324 | 0.1360 | 0.5169 | |
| Alhdyran vs. TEDRA® NT1 | 0.0445 | 0.0919 | 0.1051 | 0.1360 | |
| Alhydran® vs. TEDRA® NT3 | 0.4758 | 0.5596 | 0.7459 | 0.0381 | |
| Lipikar® vs. BAP | 0.1539 | 0.0801 | 0.0601 | 0.0695 | |
| Lipikar® vs. TEDRA® NT1 | 0.0324 | 0.0381 | 0.2181 | 0.7459 | |
| Lipikar® vs. TEDRA® NT3 | 0.3994 | 0.3309 | 0.9483 | 0.3642 | |
| BAP vs. TEDRA® NT1 | 0.0004 | 0.0001 | 0.0019 | 0.0324 | |
| BAP vs. TEDRA® NT3 | 0.0233 | 0.0065 | 0.0695 | 0.0065 | |
| TEDRA® NT1 vs. TEDRA® NT3 | 0.1948 | 0.2705 | 0.1948 | 0.5596 | |
| Data Overview | |||||
|---|---|---|---|---|---|
| CAAH (n = 36) | Friedman Test p-Value a, b | ||||
| T2 | <0.0001 | ||||
| T2–T3 | <0.0001 | ||||
| T2–T4 | <0.0001 | ||||
| T2–T5 | <0.0001 | ||||
| Post hoc test p-value d | |||||
| CAAH T2 c (n = 36) | CAAH T2–T3 c (n = 36) | CAAH T2–T4 c (n = 36) | CAAH T2–T5 c (n = 36) | ||
| TEDRA® vs. Alhydran® | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| TEDRA® vs. Lipikar® | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| TEDRA® vs. BAP | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| TEDRA® vs. TEDRA® NT1 | 0.6735 | 0.7459 | 0.6041 | 0.6973 | |
| TEDRA® vs. TEDRA® NT3 | 0.6269 | 0.8969 | >0.9999 | 0.8969 | |
| Alhydran® vs. Lipikar® | 0.1539 | 0.0518 | 0.0233 | 0.0165 | |
| Alhydran® vs. BAP | 0.0381 | 0.1198 | 0.2181 | 0.4758 | |
| Alhdyran vs. TEDRA® NT1 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Alhydran® vs. TEDRA® NT3 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Lipikar® vs. BAP | 0.0005 | 0.0005 | 0.0005 | 0.0019 | |
| Lipikar® vs. TEDRA® NT1 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Lipikar® vs. TEDRA® NT3 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| BAP vs. TEDRA® NT1 | <0.0001 | <0,0001 | <0.0001 | <0.0001 | |
| BAP vs. TEDRA® NT3 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| TEDRA® NT1 vs. TEDRA® NT3 | 0.9483 | 0.6500 | 0.6041 | 0.6041 | |
| Data Overview | |||||
|---|---|---|---|---|---|
| CADBF (n = 36) | Friedman Test p-Value a, b | ||||
| T2 | <0.0001 | ||||
| T2–T3 | <0.0001 | ||||
| T2–T4 | <0.0001 | ||||
| T2–T5 | <0.0001 | ||||
| Post hoc test p-value d | |||||
| CADBF T2 c (n = 36) | CADBF T2–T3 c (n = 36) | CADBF T2–T4 c (n = 36) | CADBF T2–T5 c (n = 36) | ||
| TEDRA® vs. Alhydran® | 0.0053 | 0.0023 | 0.0518 | 0.0043 | |
| TEDRA® vs. Lipikar® | 0.0087 | 0.0095 | 0.0023 | 0.0053 | |
| TEDRA® vs. BAP | 0.1123 | 0.3642 | 0.6973 | 0.5596 | |
| TEDRA® vs. TEDRA® NT1 | 0.2181 | 0.1734 | 0.1198 | 0.0518 | |
| TEDRA® vs. TEDRA® NT3 | 0.6041 | 0.6973 | 0.9483 | 0.8969 | |
| Alhydran® vs. Lipikar® | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Alhydran® vs. BAP | 0.2305 | 0.0324 | 0.0196 | 0.0233 | |
| Alhdyran vs. TEDRA® NT1 | 0.1198 | 0.0919 | 0.6973 | 0.3642 | |
| Alhydran® vs. TEDRA® NT3 | 0.0233 | 0.0079 | 0.0445 | 0.0065 | |
| Lipikar® vs. BAP | <0.0001 | 0.0005 | 0.0079 | 0.0007 | |
| Lipikar® vs. TEDRA® NT1 | 0.0001 | <0.0001 | <0.0001 | <0.0001 | |
| Lipikar® vs. TEDRA® NT3 | 0.0017 | 0.0029 | 0.0029 | 0.0035 | |
| BAP vs. TEDRA® NT1 | 0.7215 | 0.6500 | 0.0518 | 0.1734 | |
| BAP vs. TEDRA® NT3 | 0.2848 | 0.6041 | 0.7459 | 0.6500 | |
| TEDRA® NT1 vs. TEDRA® NT3 | 0.4758 | 0.3309 | 0.1051 | 0.0695 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Decker, I.; Klotz, T.; Vu, P.; Hoeksema, H.; De Mey, K.; Beeckman, A.; Vermeulen, B.; Speeckaert, M.; Blondeel, P.; Wagstaff, M.; et al. Influence of Moisturizers on Skin Microcirculation: An Assessment Study Using Laser Speckle Contrast Imaging. J. Pers. Med. 2023, 13, 1507. https://doi.org/10.3390/jpm13101507
De Decker I, Klotz T, Vu P, Hoeksema H, De Mey K, Beeckman A, Vermeulen B, Speeckaert M, Blondeel P, Wagstaff M, et al. Influence of Moisturizers on Skin Microcirculation: An Assessment Study Using Laser Speckle Contrast Imaging. Journal of Personalized Medicine. 2023; 13(10):1507. https://doi.org/10.3390/jpm13101507
Chicago/Turabian StyleDe Decker, Ignace, Tanja Klotz, Peter Vu, Henk Hoeksema, Kimberly De Mey, Anse Beeckman, Bob Vermeulen, Marijn Speeckaert, Phillip Blondeel, Marcus Wagstaff, and et al. 2023. "Influence of Moisturizers on Skin Microcirculation: An Assessment Study Using Laser Speckle Contrast Imaging" Journal of Personalized Medicine 13, no. 10: 1507. https://doi.org/10.3390/jpm13101507
APA StyleDe Decker, I., Klotz, T., Vu, P., Hoeksema, H., De Mey, K., Beeckman, A., Vermeulen, B., Speeckaert, M., Blondeel, P., Wagstaff, M., Monstrey, S., & Claes, K. E. Y. (2023). Influence of Moisturizers on Skin Microcirculation: An Assessment Study Using Laser Speckle Contrast Imaging. Journal of Personalized Medicine, 13(10), 1507. https://doi.org/10.3390/jpm13101507