

Recurrence-Free Survival in Early and Locally Advanced Large Cell Neuroendocrine Carcinoma of the Lung after Complete Tumor Resection

 , , , , , ,
, , , , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Statistical Analysis
3. Results
3.1. Study Population and Treatment
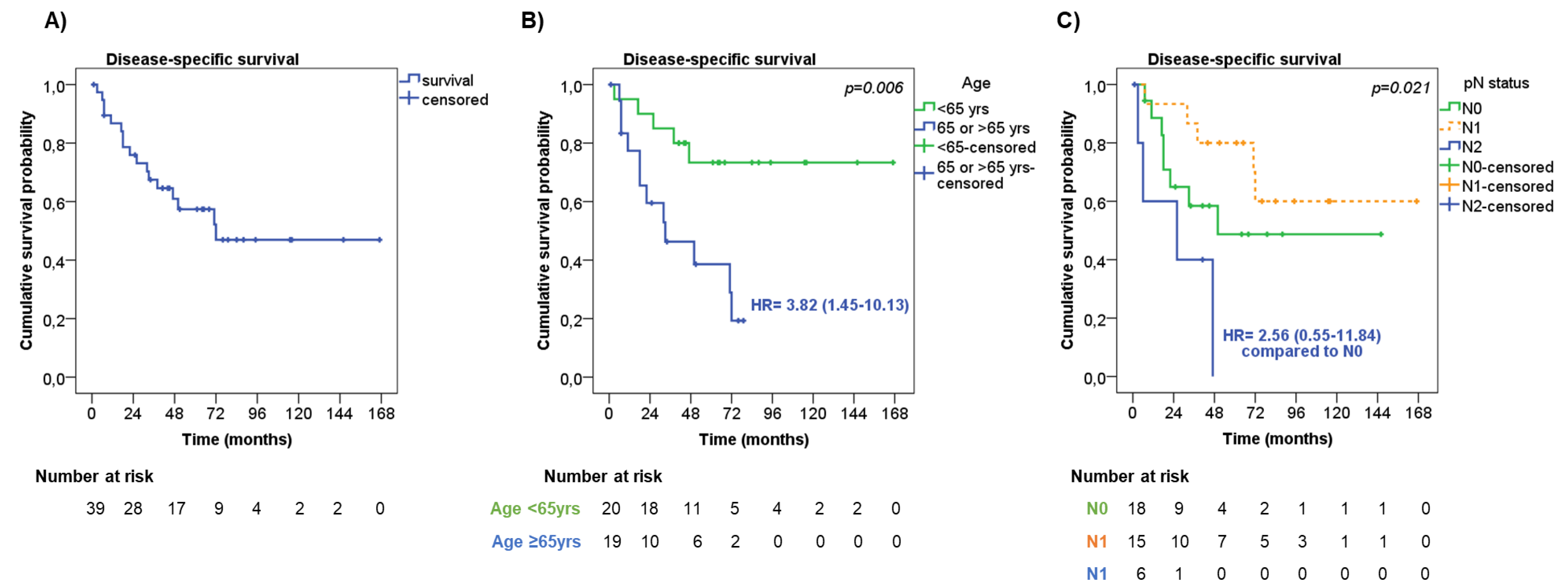
3.2. Clinical Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fasano, M.; Della Corte, C.M.; Papaccio, F.; Ciardiello, F.; Morgillo, F. Pulmonary Large-Cell Neuroendocrine Carcinoma: From Epidemiology to Therapy. J. Thorac. Oncol. 2015, 10, 1133–1141. [Google Scholar] [CrossRef] [Green Version]
- Derks, J.L.; Hendriks, L.E.; Buikhuisen, W.A.; Groen, H.J.; Thunnissen, E.; van Suylen, R.J.; Houben, R.; Damhuis, R.A.; Speel, E.J.; Dingemans, A.M. Clinical features of large cell neuroendocrine carcinoma: A population-based overview. Eur. Respir. J. 2016, 47, 615–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinslow, C.J.; May, M.S.; Saqi, A.; Shu, C.A.; Chaudhary, K.R.; Wang, T.J.C.; Cheng, S.K. Large-Cell Neuroendocrine Carcinoma of the Lung: A Population-Based Study. Clin. Lung Cancer. 2020, 21, e99–e113. [Google Scholar] [CrossRef] [PubMed]
- WHO. Classification of Tumours: Thoracic Tumours, 5th ed.; France, L., Ed.; International Agency for Research on Cancer: Lyon, France, 2021; Volume 5.
- Roesel, C.; Welter, S.; Kambartel, K.O.; Weinreich, G.; Krbek, T.; Serke, M.; Ibrahim, M.; Alnajdawi, Y.; Plones, T.; Aigner, C. Prognostic markers in resected large cell neuroendocrine carcinoma: A multicentre retrospective analysis. J. Thorac. Dis. 2020, 12, 466–476. [Google Scholar] [CrossRef] [PubMed]
- Raman, V.; Jawitz, O.K.; Yang, C.J.; Tong, B.C.; D’Amico, T.A.; Berry, M.F.; Harpole, D.H., Jr. Adjuvant Therapy for Patients With Early Large Cell Lung Neuroendocrine Cancer: A National Analysis. Ann. Thorac. Surg. 2019, 108, 377–383. [Google Scholar] [CrossRef]
- Veronesi, G.; Morandi, U.; Alloisio, M.; Terzi, A.; Cardillo, G.; Filosso, P.; Rea, F.; Facciolo, F.; Pelosi, G.; Gandini, S.; et al. Large cell neuroendocrine carcinoma of the lung: A retrospective analysis of 144 surgical cases. Lung Cancer 2006, 53, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.W.; Kim, H.K.; Kim, J.; Shim, Y.M.; Ahn, M.J.; Choi, Y.L. Outcomes of Curative-Intent Surgery and Adjuvant Treatment for Pulmonary Large Cell Neuroendocrine Carcinoma. World J. Surg. 2017, 41, 1820–1827. [Google Scholar] [CrossRef]
- Soldath, P.; Binderup, T.; Carstensen, F.; Clausen, M.M.; Kjaer, A.; Federspiel, B.; Knigge, U.; Langer, S.W.; Petersen, R.H. Long-term outcomes after video-assisted thoracoscopic surgery in pulmonary large-cell neuroendocrine carcinoma. Surg. Oncol. 2022, 41, 101728. [Google Scholar] [CrossRef]
- Lowczak, A.; Kolasinska-Cwikla, A.; Osowiecka, K.; Glinka, L.; Palucki, J.; Rzepko, R.; Doboszynska, A.; Cwikla, J.B. Outcomes of Patients with Pulmonary Large Cell Neuroendocrine Carcinoma in I-IV Stage. Medicina 2021, 57, 118. [Google Scholar] [CrossRef] [PubMed]
- Remon, J.; Soria, J.C.; Peters, S. Early and locally advanced non-small-cell lung cancer: An update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging, systemic and local therapy. Ann. Oncol. 2021, 32, 1637–1642. [Google Scholar] [CrossRef]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; Committee, E.G. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- Dingemans, A.C.; Fruh, M.; Ardizzoni, A.; Besse, B.; Faivre-Finn, C.; Hendriks, L.E.; Lantuejoul, S.; Peters, S.; Reguart, N.; Rudin, C.M.; et al. Small-cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up(☆). Ann. Oncol. 2021, 32, 839–853. [Google Scholar] [CrossRef]
- Peng, K.; Cao, H.; You, Y.; He, W.; Jiang, C.; Wang, L.; Jin, Y.; Xia, L. Optimal Surgery Type and Adjuvant Therapy for T1N0M0 Lung Large Cell Neuroendocrine Carcinoma. Front. Oncol. 2021, 11, 591823. [Google Scholar] [CrossRef] [PubMed]
- Iyoda, A.; Hiroshima, K.; Moriya, Y.; Iwadate, Y.; Takiguchi, Y.; Uno, T.; Nakatani, Y.; Yoshino, I. Postoperative recurrence and the role of adjuvant chemotherapy in patients with pulmonary large-cell neuroendocrine carcinoma. J. Thorac. Cardiovasc. Surg. 2009, 138, 446–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, J.Y.; Choi, S.H.; Kim, T.H.; Lee, J.; Pyo, J.H.; Kim, Y.T.; Lee, S.J.; Yoon, H.I.; Cho, J.; Lee, C.G. Clinical features and treatment outcomes of resected large cell neuroendocrine carcinoma of the lung. Radiat. Oncol. J. 2021, 39, 288–296. [Google Scholar] [CrossRef]
- Filosso, P.L.; Guerrera, F.; Evangelista, A.; Galassi, C.; Welter, S.; Rendina, E.A.; Travis, W.; Lim, E.; Sarkaria, I.; Thomas, P.A.; et al. Adjuvant chemotherapy for large-cell neuroendocrine lung carcinoma: Results from the European Society for Thoracic Surgeons Lung Neuroendocrine Tumours Retrospective Database. Eur. J. Cardiothorac. Surg. 2017, 52, 339–345. [Google Scholar] [CrossRef] [Green Version]
- Saji, H.; Tsuboi, M.; Matsubayashi, J.; Miyajima, K.; Shimada, Y.; Imai, K.; Kato, Y.; Usuda, J.; Kajiwara, N.; Uchida, O.; et al. Clinical response of large cell neuroendocrine carcinoma of the lung to perioperative adjuvant chemotherapy. Anticancer. Drugs 2010, 21, 89–93. [Google Scholar] [CrossRef]
- Kujtan, L.; Muthukumar, V.; Kennedy, K.F.; Davis, J.R.; Masood, A.; Subramanian, J. The Role of Systemic Therapy in the Management of Stage I Large Cell Neuroendocrine Carcinoma of the Lung. J. Thorac. Oncol. 2018, 13, 707–714. [Google Scholar] [CrossRef] [Green Version]
- Iyoda, A.; Hiroshima, K.; Moriya, Y.; Takiguchi, Y.; Sekine, Y.; Shibuya, K.; Iizasa, T.; Kimura, H.; Nakatani, Y.; Fujisawa, T. Prospective study of adjuvant chemotherapy for pulmonary large cell neuroendocrine carcinoma. Ann. Thorac. Surg. 2006, 82, 1802–1807. [Google Scholar] [CrossRef]
- Cattoni, M.; Vallieres, E.; Brown, L.M.; Sarkeshik, A.A.; Margaritora, S.; Siciliani, A.; Filosso, P.L.; Guerrera, F.; Imperatori, A.; Rotolo, N.; et al. Large Cell Neuroendocrine Tumor Size >3 cm Negatively Impacts Long-Term Outcomes After R0 Resection. World J. Surg. 2019, 43, 1712–1720. [Google Scholar] [CrossRef]
- Casali, C.; Stefani, A.; Rossi, G.; Migaldi, M.; Bettelli, S.; Parise, A.; Morandi, U. The prognostic role of c-kit protein expression in resected large cell neuroendocrine carcinoma of the lung. Ann. Thorac. Surg. 2004, 77, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.K.; Qin, T.; Zeng, Y.D.; Zhao, Y.Y.; Hou, X.; Fang, W.F.; Hong, S.D.; Zhou, T.; Hu, Z.H.; Yang, Y.P.; et al. Clinical analysis of 50 Eastern Asian patients with primary pulmonary large-cell neuroendocrine carcinoma. Onco. Targets Ther. 2015, 8, 1219–1227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, Y.; Hu, F.; Li, C.; Xu, J.; Zhong, R.; Zhang, X.; Chu, T.; Han, B. Clinical Features and Outcomes Analysis of Surgical Resected Pulmonary Large-Cell Neuroendocrine Carcinoma With Adjuvant Chemotherapy. Front. Oncol. 2020, 10, 556194. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wittekind, C.; Compton, C.; Quirke, P.; Nagtegaal, I.; Merkel, S.; Hermanek, P.; Sobin, L.H. A uniform residual tumor (R) classification: Integration of the R classification and the circumferential margin status. Cancer 2009, 115, 3483–3488. [Google Scholar] [CrossRef]
- Altieri, B.; Barrea, L.; Modica, R.; Bottiglieri, F.; de Cicco, F.; Muscogiuri, G.; Circelli, L.; Savarese, G.; Di Somma, C.; Savastano, S.; et al. Vitamin D deficiency and tumor aggressiveness in gastroenteropancreatic neuroendocrine tumors. Endocrine 2021, 75, 623–634. [Google Scholar] [CrossRef]
- Barrea, L.; Altieri, B.; Muscogiuri, G.; Laudisio, D.; Annunziata, G.; Colao, A.; Faggiano, A.; Savastano, S. Impact of Nutritional Status on Gastroenteropancreatic Neuroendocrine Tumors (GEP-NET) Aggressiveness. Nutrients 2018, 10, 1854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muscogiuri, G.; Altieri, B.; Albertelli, M.; Dotto, A.; Modica, R.; Barrea, L.; Fanciulli, G.; Feola, T.; Baldelli, R.; Ruggeri, R.M.; et al. Epidemiology of pancreatic neuroendocrine neoplasms: A gender perspective. Endocrine 2020, 69, 441–450. [Google Scholar] [CrossRef]
- Barrea, L.; Muscogiuri, G.; Modica, R.; Altieri, B.; Pugliese, G.; Minotta, R.; Faggiano, A.; Colao, A.; Savastano, S. Cardio-Metabolic Indices and Metabolic Syndrome as Predictors of Clinical Severity of Gastroenteropancreatic Neuroendocrine Tumors. Front. Endocrinol. 2021, 12, 649496. [Google Scholar] [CrossRef]
- Deng, C.; Wu, S.G.; Tian, Y. Lung Large Cell Neuroendocrine Carcinoma: An Analysis of Patients from the Surveillance, Epidemiology, and End-Results (SEER) Database. Med. Sci. Monit. 2019, 25, 3636–3646. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, J.; Huang, C.; Tian, Z.; Zhou, X.; Guo, C.; Liu, H.; Li, S. Survival outcomes of surgery in patients with pulmonary large-cell neuroendocrine carcinoma: A retrospective single-institution analysis and literature review. Orphanet. J. Rare Dis. 2021, 16, 82. [Google Scholar] [CrossRef] [PubMed]
- Altieri, B.; Di Dato, C.; Martini, C.; Sciammarella, C.; Di Sarno, A.; Colao, A.; Faggiano, A.; Group, N. Bone Metastases in Neuroendocrine Neoplasms: From Pathogenesis to Clinical Management. Cancers 2019, 11, 1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowczak, A.; Kolasinska-Cwikla, A.; Cwikla, J.B.; Osowiecka, K.; Palucki, J.; Rzepko, R.; Glinka, L.; Doboszynska, A. Outcomes of Patients with Clinical Stage I-IIIA Large-Cell Neuroendocrine Lung Cancer Treated with Resection. J. Clin. Med. 2020, 9, 1370. [Google Scholar] [CrossRef] [PubMed]
- Xi, J.; Zhao, M.; Zheng, Y.; Liang, J.; Hu, Z.; Huang, Y.; Yang, Y.; Zhan, C.; Jiang, W.; Lu, T.; et al. Development and validation of a nomogram for predicting the overall survival of patients with lung large cell neuroendocrine carcinoma. Transl. Cancer Res. 2020, 9, 4943–4957. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Casali et al., Ann Thorac Surg. 2004 [22] | Zhang et al., Onco Targets Ther. 2015 [23] | Cattoni et al., World J Surg. 2019 [21] | Shen et al., Front Oncol. 2020 [24] | Current Study |
|---|---|---|---|---|---|
| Patients, n | 33 | 50 | 72 | 94 | 39 |
| Male, n (%) | 31 (93.9) | 47 (94.0) | 43 (59.7) | 84 (89.4) | 26 (66.7) |
| Age, median (range) yrs | 65 (42–80) | 59 (40–80) | 65 (58–71) a | 60 (35–80) | 64 (4–83) |
| Tumor relapse, n (%) | 15 (45.4) | n.a. | 34 (47) | 44 of 79 (55.7) | 21 (46.2) |
| Tumor stage, n (%): | |||||
| I | 21 (63.6) | 22 (44.0) | 32 (44.4) | 31 (33.0) | 13 (33.3) |
| II | 0 | 18 (36.0) | 24 (33.3) | 22 (23.4) | 15 (38.5) |
| III | 12 (36.4) | 10 (20.0) | 16 (22.2) | 41 (43.6) | 11 (28.2) |
| Median follow-up (range), months, | 24.9 (2–118) | n.a. | 47 (40–79) b | n.a. | 44 (4–169) |
| Median RFS, months | n.a. | 49.3 | n.a. | n.a. | 39 |
| 5-yrs RFS rate, % | n.a. | n.a. | n.a. | n.a. | 44.9 |
| Median DSS, months | n.a. | n.a. | n.a. | n.a. | 72 |
| 5-yrs DSS rate, % | n.a. | n.a. | 57.6 | n.a. | 57.4 |
| Median OS, months | n.a. | Not reached | n.a. | n.a. | 51 |
| 5-yrs OS rate, % | 51 | n.a. | 47.4 | n.a. | 47 |
| Adjuvant therapy, n (%) | n.a. | n.a. | 22 (30.5) | 75 (79.8) | 23 (60.0) |
| Evaluation of adjuvant treatment | n.a. | n.a. | No correlation between additional chemo-/radiotherapy with RFS and OS | Etoposide-platinum regimen was associated with better outcomes compared to other chemotherapies | No correlation between additional chemo-/radiotherapy with RFS and OS |
| Potential prognostic factors of RFS | n.a. | n.a. | Tumor size cut-off 3 cm (for systemic recurrence) * | pN | Age (cut-off 65 yrs) and pN |
| Potential prognostic factors of OS | c-kit expression * | Serum albumin | Not found | Different chemotherapies, T stage, and serum CEA levels | Age (cut-off 65 yrs) and pN |
| Parameters | n (%) |
|---|---|
| N patients | 39 |
| Sex: Male Female | 26 (66.7%) 13 (33.3%) |
| BMI: Normal weight Overweight or obesity Not reported | 21 (53.8%) 9 (23.1%) 9 (23.1%) |
| Smoking status: Non-smoker Current or former smoker | 5 (12.8%) 34 (87.2%) |
| Comorbidities: Type 2 diabetes mellitus Hypertension Cardiovascular events | 5 (12.8%) 12 (30.8%) 6 (15.4%) |
| Initial symptoms: Cough Hemoptysis Chest and back pain Fever Asymptomatic | 4 (10.3%) 3 (7.7%) 7 (17.9%) 12 (30.8%) 13 (33.3%) |
| TNM Tumor Stage: I II III | 13 (33.3%) 15 (38.5%) 11 (28.2%) |
| Surgical resection: Wedge resection Lobectomy Bilobectomy Pneumonectomy | 3 (7.7%) 27 (69.2%) 2 (5.1%) 7 (18.0%) |
| Lymph node dissection: Not performed Performed | 1 (2.6%) 38 (97.4%) |
| Adjuvant therapy: Chemotherapy only Radiotherapy only Chemotherapy + radiotherapy No adjuvant therapy | 13 (33.3%) 1 (2.6%) 9 (23.0%) 16 (41.0%) |
| Parameter | n | Univariate RFS | Multivariate RFS | ||
|---|---|---|---|---|---|
| p | HR (95%CI) | p | HR (95%CI) | ||
| Sex: M F | 26 13 | Ref. 0.23 | 0.54 (0.20–1.48) | - | |
| Age at diagnosis: <65 years ≥65 years | 20 19 | Ref. 0.07 | 2.26 (0.94–5.25) | Ref. 0.008 | 4.19 (1.46–12.07) |
| Tumor size: ≤3 cm >3 cm | 5 34 | Ref. 0.62 | 1.44 (0.33–6.22) | - | |
| Pleural invasion: No yes | 26 13 | Ref. 0.21 | 1.77 (0.73–4.28) | - | |
| TNM tumor stage: I II III | 13 15 11 | 0.65 0.99 0.44 | Ref. 0.99 (0.34–2.87) 1.54 (0.51–4.61) | - | |
| pN: N0 N1 N2 | 18 15 6 | 0.27 0.67 0.19 | Ref. 0.81 (0.31–2.13) 2.19 (0.67–7.20) | 0.008 0.65 0.003 | Ref. 1.26 (0.46–3.46) 13.56 (2.45–74.89) |
| Type of surgery: wedge/lobectomy bilobectomy/pneumectomy | 30 9 | Ref. 0.16 | 0.41 (0.12–1.40) | Ref. 0.67 | 0.73 (0.17–3.17) |
| Adjuvant treatment: no adjuvant therapies chemotherapy or RT alone chemotherapy + RT | 16 14 9 | 0.24 0.15 0.92 | Ref. 2.06 (0.77–5.48) 0.94 (0.27–3.23) | 0.07 0.06 0.35 | Ref. 2.86 (0.96–8.54) 0.51 (0.12–2.11) |
| Parameter | n | Univariate DSS | Multivariate DSS | ||
|---|---|---|---|---|---|
| p | HR (95%CI) | p | HR (95%CI) | ||
| Sex: M F | 26 13 | Ref. 0.31 | 0.56 (0.18–1.71) | - | |
| Age at diagnosis: <65 years ≥65 years | 20 19 | Ref. 0.01 | 3.91 (1.37–11.20) | Ref. 0.002 | 9.30 (2.23–38.83) |
| Tumor size: ≤3 cm >3 cm | 5 34 | Ref. 0.84 | 1.17 (0.26–5.19) | - | |
| Pleural invasion: No yes | 26 13 | Ref. 0.24 | 1.78 (0.68–4.71) | - | |
| TNM tumor stage: I II III | 13 15 11 | 0.27 0.46 0.42 | Ref. 0.63 (0.18–2.19) 1.61 (0.51–5.11) | - | |
| pN: N0 N1 N2 | 18 15 6 | 0.04 0.19 0.09 | Ref. 0.47 (0.15–1.48) 2.87 (0.84–9.78) | 0.003 0.31 0.003 | Ref. 0.55 (0.17–1.75) 11.88 (2.28–61.84) |
| Type of surgery: wedge/lobectomy bilobectomy/pneumectomy | 30 9 | Ref. 0.21 | 0.39 (0.09–1.72) | - | |
| Adjuvant treatment: no adjuvant therapies chemotherapy or RT alone chemotherapy + RT | 16 14 9 | 0.67 0.38 0.76 | Ref. 1.66 (0.54–5.07) 1.23 (0.33–4.63) | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altieri, B.; La Salvia, A.; Modica, R.; Marciello, F.; Mercier, O.; Filosso, P.L.; de Latour, B.R.; Giuffrida, D.; Campione, S.; Guggino, G.; et al. Recurrence-Free Survival in Early and Locally Advanced Large Cell Neuroendocrine Carcinoma of the Lung after Complete Tumor Resection. J. Pers. Med. 2023, 13, 330. https://doi.org/10.3390/jpm13020330
Altieri B, La Salvia A, Modica R, Marciello F, Mercier O, Filosso PL, de Latour BR, Giuffrida D, Campione S, Guggino G, et al. Recurrence-Free Survival in Early and Locally Advanced Large Cell Neuroendocrine Carcinoma of the Lung after Complete Tumor Resection. Journal of Personalized Medicine. 2023; 13(2):330. https://doi.org/10.3390/jpm13020330
Chicago/Turabian StyleAltieri, Barbara, Anna La Salvia, Roberta Modica, Francesca Marciello, Olaf Mercier, Pier Luigi Filosso, Bertrand Richard de Latour, Dario Giuffrida, Severo Campione, Gianluca Guggino, and et al. 2023. "Recurrence-Free Survival in Early and Locally Advanced Large Cell Neuroendocrine Carcinoma of the Lung after Complete Tumor Resection" Journal of Personalized Medicine 13, no. 2: 330. https://doi.org/10.3390/jpm13020330
APA StyleAltieri, B., La Salvia, A., Modica, R., Marciello, F., Mercier, O., Filosso, P. L., de Latour, B. R., Giuffrida, D., Campione, S., Guggino, G., Fadel, E., Papotti, M., Colao, A., Scoazec, J. -Y., Baudin, E., & Faggiano, A. (2023). Recurrence-Free Survival in Early and Locally Advanced Large Cell Neuroendocrine Carcinoma of the Lung after Complete Tumor Resection. Journal of Personalized Medicine, 13(2), 330. https://doi.org/10.3390/jpm13020330