
Prevalence of Cognitive Decline in Type 2 Diabetes Mellitus Patients: A Real-World Cross-Sectional Study in Mysuru, India

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methods
2.2. Participants
Test Group
- T2DM patients of any gender aged between 30 years and 60 years;
- T2DM patients with minimal literacy (able to read and write) in Kannada or English.
- Patients with a history or present condition of type 1 diabetes, secondary diabetes, or gestational diabetes;
- Patients with psychiatric illness or on medication having psychoactive activity;
- Patients suffering from severe diseases such as, but not confined to, cancer (diagnosed less than five years ago) or severe autoimmune diseases;
- Patients with neurological diseases;
- Patients whose caregivers did not give consent.
2.3. Settings
2.4. Study Size
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pradeepa, R.; Mohan, V. Epidemiology of type 2 diabetes in India. Indian J. Ophthalmol. 2021, 69, 2932. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2009, 32, S62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sapra, A.; Bhandari, P. Diabetes Mellitus; StatPearls Publishing: Tampa, FL, USA, 2021. [Google Scholar]
- Abrishami, Z.; Nasli-Esfahani, E.; Razmandeh, R.; Larijani, B.; Bandarian, F. Iran Diabetes Research Roadmap (IDRR) Study; Gap Analysis of Diabetes Complications in Iran: A Review Article. Iran. J. Public Health 2017, 46, 32–38. [Google Scholar]
- Beckman, J.A.; Creager, M.A. Vascular complications of diabetes. Circ. Res. 2016, 118, 1771–1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kravitz, E.; Schmeidler, J.; Schnaider Beeri, M. Type 2 diabetes and cognitive compromise: Potential roles of diabetes-related therapies. Endocrinol. Metab. Clin. N. Am. 2013, 42, 489–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheen, Y.J.; Sheu, W.H.H. Association between hypoglycemia and dementia in patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2016, 116, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Areosa Sastre, A.; Vernooij, R.W.M.; González-Colaço Harmand, M.; Martínez, G. Effect of the treatment of Type 2 diabetes mellitus on the development of cognitive impairment and dementia. Cochrane Database Syst. Rev. 2017, 6, CD003804. [Google Scholar] [CrossRef]
- Gregg, E.W.; Brown, A. Cognitive and physical disabilities and aging-related complications of diabetes. Clin. Diabetes 2003, 21, 113–118. [Google Scholar] [CrossRef] [Green Version]
- Biessels, G.J.; Van der Heide, L.P.; Kamal, A.; Bleys, R.L.A.W.; Gispen, W.H. Ageing and diabetes: Implications for brain function. Eur. J. Pharmacol. 2002, 441, 1–14. [Google Scholar] [CrossRef]
- Duarte, A.I.; Candeias, E.; Correia, S.C.; Santos, R.X.; Carvalho, C.; Cardoso, S.; Plácido, A.; Santos, M.S.; Oliveira, C.R.; Moreira, P.I. Crosstalk between diabetes and brain: Glucagon-like peptide-1 mimetics as a promising therapy against neurodegeneration. Biochim. Biophys. Acta 2013, 1832, 527–541. [Google Scholar] [CrossRef] [Green Version]
- Pasquier, F.; Boulogne, A.; Leys, D.; Fontaine, P. Diabetes mellitus and dementia. Diabetes Metab. 2006, 32, 403–414. [Google Scholar] [CrossRef]
- Shanik, M.H.; Xu, Y.; Skrha, J.; Dankner, R.; Zick, Y.; Roth, J. Insulin resistance and hyperinsulinemia: Is hyperinsulinemia the cart or the horse? Diabetes Care 2008, 31 (Suppl. S2), S262–S268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seaquist, E.R. The Final Frontier: How Does Diabetes Affect the Brain? Diabetes 2010, 59, 4–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrinivas Sangappa Tamboli, R.B. Prevalence of Diabetes Mellitus in Families and Population of Rural District of Southern Karnataka: Community Based Study. Asian J. Pharm. Clin. Res. 2018, 11, 94–99. [Google Scholar] [CrossRef]
- Rotonen, S.; Auvinen, J.; Bloigu, A.; Härkönen, P.; Jokelainen, J.; Timonen, M.; Keinänen-Kiukaanniemi, S. Long-term dysglycemia as a risk factor for faster cognitive decline during aging: A 12-year follow-up study. Diabetes Res. Clin. Pract. 2021, 180, 109045. [Google Scholar] [CrossRef] [PubMed]
- Mirahmadizadeh, A.; Khorshidsavar, H.; Seif, M.; Sharifi, M.H. Adherence to Medication, Diet and Physical Activity and the Associated Factors Amongst Patients with Type 2 Diabetes. Diabetes Ther. 2020, 11, 479–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Maurer, M.A.; Shiyanbola, O.O.; Mott, M.L.; Means, J. Engaging Patient Advisory Boards of African American Community Members with Type 2 Diabetes in Implementing and Refining a Peer-Led Medication Adherence Intervention. Pharmacy 2022, 10, 37. [Google Scholar] [CrossRef]
- Mahendran, R.; Chua, J.; Feng, L.; Kua, E.H.; Preedy, V.R. The Mini-Mental State Examination and Other Neuropsychological Assessment Tools for Detecting Cognitive Decline. Diet Nutr. Dement. Cogn. Decline 2015, 109, 1159–1174. [Google Scholar] [CrossRef]
- Jankovic, J.; Mazziotta, J.C.; Pomeroy, S.L.; Newman, N.J. Bradley and Daroff’s Neurology in Clinical Practice, 8th ed.; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Yerrapragada, D.B.; Rao, C.R.; Karunakaran, K.; Lee, H.S.E. Cognitive dysfunction among adults with type 2 diabetes mellitus in Karnataka, India. Ochsner J. 2019, 19, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Lalithambika, C.V.; Arun, C.S.; Saraswathy, L.A.; Bhaskaran, R. Cognitive impairment and its association with glycemic control in type 2 diabetes mellitus patients. Indian J. Endocrinol. Metab. 2019, 23, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Saedi, E.; Gheini, M.R.; Faiz, F.; Arami, M.A. Diabetes mellitus and cognitive impairments. World J. Diabetes 2016, 7, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, A.; Hegde, S.; Praharaj, S.K.; Prabhu, K.; Patole, C.; Shetty, A.K.; Mayya, S.S.; Acharya, R.V.; Hande, H.M.; Prabhu, M.M.; et al. Age related prevalence of mild cognitive impairment in type 2 diabetes mellitus patients in the indian population and association of serum lipids with cognitive dysfunction. Front. Endocrinol. 2021, 12, 1739. [Google Scholar] [CrossRef] [PubMed]
- Murman, D.L. The impact of age on cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef]
- Oguntibeju, O.O. Type 2 diabetes mellitus, oxidative stress and inflammation: Examining the links. Int. J. Physiol. Pathophysiol. Pharmacol. 2019, 11, 45–63. [Google Scholar] [PubMed]
- Shoily, S.S.; Ahsan, T.; Fatema, K.; Sajib, A.A. Common genetic variants and pathways in diabetes and associated complications and vulnerability of populations with different ethnic origins. Sci. Rep. 2021, 11, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Mehdi, S.; Manohar, K.; Shariff, A.; Kinattingal, N.; Wani, S.U.; Alshehri, S.; Imam, M.T.; Shakeel, F.; Krishna, K.L. Omega-3 Fatty Acids Supplementation in the Treatment of Depression: An Observational Study. J. Pers. Med. 2023, 13, 224. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographics | Test Group (Diabetics) | Control Group (Nondiabetics) | p-Value |
|---|---|---|---|
| Mean Age | 51 ± 9 | 50 ± 8 | <0.09 |
| Age group | <0.001 | ||
| 30–40 years | 18 | 54 | |
| 41–50 years | 25 | 39 | |
| 51–60 years | 57 | 07 | |
| Gender | <0.001 | ||
| Male | 53 | 77 | |
| Female | 47 | 23 | |
| Marital Status | <0.001 | ||
| Married | 99 | 84 | |
| Unmarried | 1 | 16 | |
| Mean Weight (kg) | 66.98 ± 11.47 | 66.20 ± 11.32 | 0.708 |
| Mean Height (cm) | 162.57 ± 7.95 | 167.91 ± 8.24 | <0.001 |
| BMI | <0.001 | ||
| Normal | 49 | 70 | |
| Underweight | 04 | 07 | |
| Overweight | 36 | 09 | |
| Obese | 11 | 14 | |
| Education | <0.001 | ||
| Grade 5 or below | 28 | 00 | |
| Grade 6 or above | 72 | 100 | |
| Area | <0.001 | ||
| Rural | 65 | 36 | |
| Urban | 35 | 64 | |
| Smoking | <0.001 | ||
| Current smokers | 5 | 27 | |
| Ex-smokers | 7 | 5 | |
| Nonsmokers | 88 | 68 |
| Cognitive Domain | Highest Score | Test Group (Diabetic) Mean Score (SD) | Control Group (Nondiabetic) Mean Score (SD) | p-Value |
|---|---|---|---|---|
| Total Score on MoCA | 30 | 18.99 (0.48) | 26.21 (0.46) | <0.001 |
| Visuospatial/Executive Function | 5 | 1.71 (0.17) | 4.02 (0.16) | <0.001 |
| Naming | 3 | 2.51 (0.07) | 2.89 (0.05) | 0.001 |
| Attention | 6 | 3.57 (0.16) | 5.21 (0.17) | <0.001 |
| Language | 3 | 1.75 (0.06) | 1.75 (0.17) | 1.000 |
| Abstraction | 2 | 1.07 (0.10) | 1.68 (0.11) | <0.001 |
| Delayed Recall | 5 | 1.9 (0.20) | 4.07 (0.20) | <0.001 |
| Orientation | 6 | 5.72 (0.10) | 5.86 (0.14) | 0.414 |
| Demographics | N = 100 | Mean MoCA Score (SD) | p-Value |
|---|---|---|---|
| Gender | |||
| Male | 53 | 19.23 (4.84) | 0.602 |
| Female | 47 | 18.72 (4.74) | |
| Age | |||
| 30–40 | 18 | 22.33 (3.11) | <0.001 |
| 41–50 | 25 | 19.96 (4.68) | |
| 51–60 | 57 | 17.51 (4.67) | |
| Marital Status | |||
| Married | 1 | 23.00 (0.0) | 0.402 |
| Unmarried | 99 | 18.95 (4.79) | |
| Education | |||
| Less or equal to 5 years of formal education | 28 | 17.71 (5.50) | 0.096 |
| More or equal to 6 years of formal education | 72 | 19.49 (4.41) | |
| Area | |||
| Rural | 65 | 18.69 (4.76) | 0.398 |
| Urban | 35 | 19.54 (4.84) | |
| Smoking | |||
| Current | 5 | 18.40 (4.45) | 0.957 |
| Ex | 7 | 18.86 (4.67) | |
| Non | 88 | 19.03 (4.85) | |
| DM Years | |||
| 0–5 | 61 | 19.57 (4.59) | 0.302 |
| 6–10 | 26 | 17.92 (5.59) | |
| Above 10 | 13 | 18.38 (3.64) | |
| PPBS | |||
| 75–150 | 16 (16) | 17.75 (5.323) | <0.553 |
| 151–200 | 25 (25) | 19.04 (3.942) | |
| 201–250 | 19 (19) | 20.11 (4.999) | |
| Above 250 | 40 (40) | 18.93 (4.969) | |
| Regular Medication | |||
| Yes | 93 | 19.11 (4.75) | 0.373 |
| No | 7 | 17.43 (5.22) | |
| MoCA Score | No. of Patients | PPBS Mean (SD) | p Value |
|---|---|---|---|
| 0–25 | 92 | 249.85 (107.97) | <0.601 |
| Above 26 | 8 | 229.75 (85.08) |
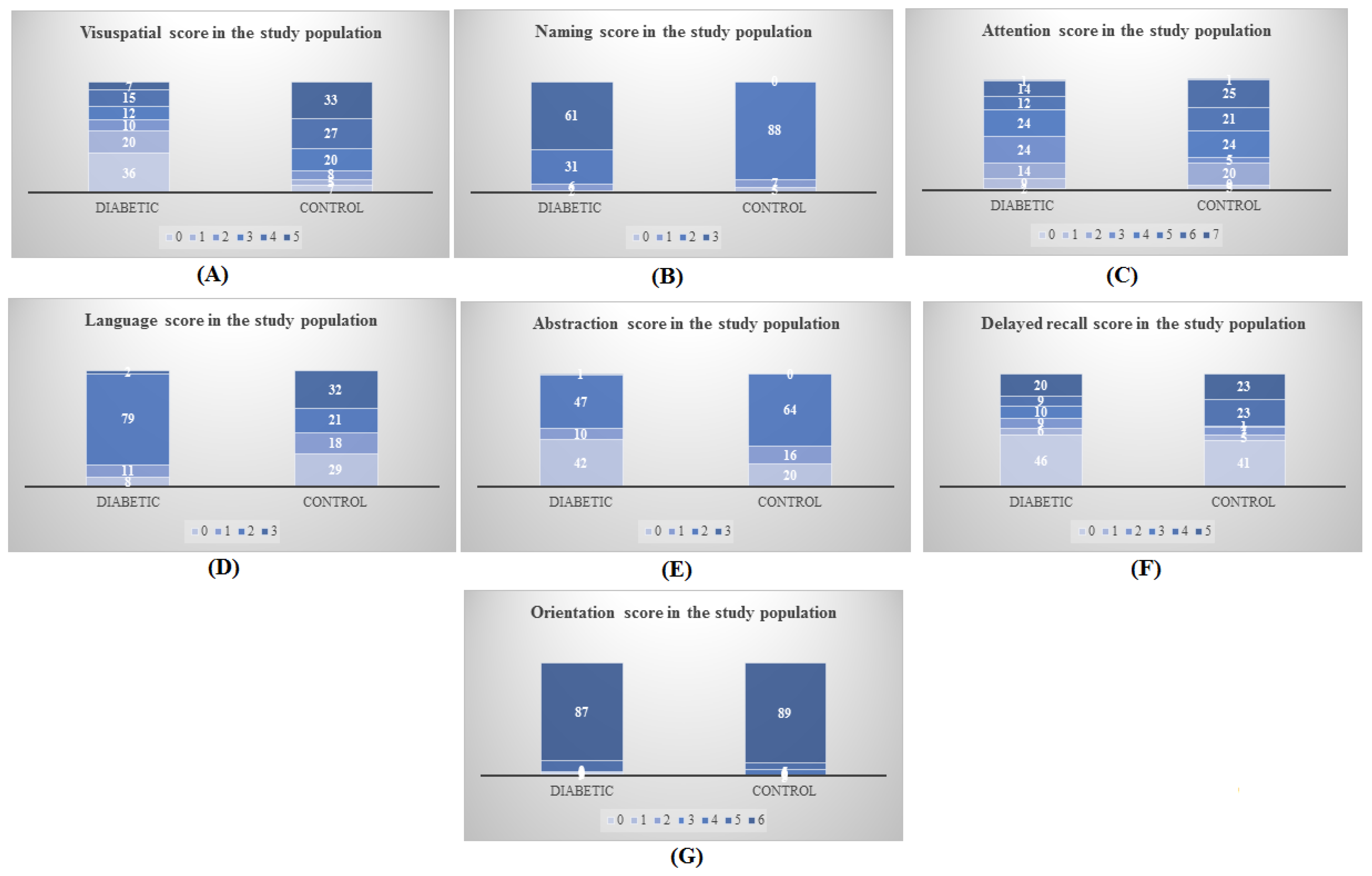
| Cognitive Domain | Score | Test | Control | p | ||||
|---|---|---|---|---|---|---|---|---|
| No of Patients Total | Cognitive Impairment n (%) | Normal Cognition n (%) | No of Patients Total | Cognitive Impairment n (%) | Normal Cognition n (%) | |||
| Visuospatial/Executive Function | 0 | 36 | 36 (100) | 0 (0) | 1 | 1 (100) | 0 (0) | |
| 1 | 20 | 19 (95) | 1 (5) | 0 | 0 (0) | 0 (0) | 0.5366 | |
| 2 | 10 | 10 (100) | 0 (0) | 2 | 2 (100) | 0 (0) | 0.1657 | |
| 3 | 12 | 11 (91.66) | 1 (8.33) | 9 | 9 (100) | 0 (0) | ||
| 4 | 15 | 11 (73.33) | 4 (26.66) | 14 | 0 (0) | 14 (100) | 0.3175 | |
| 5 | 7 | 5 (71.42) | 2 (28.57) | 18 | 0 (0) | 18 (100) | 0.0212 | |
| Naming | 0 | 2 | 2 (100) | 0 (0) | 0 | 0 (0) | 0 (0) | 0.6209 |
| 1 | 6 | 6 (100) | 0 (0) | 0 | 0 (0) | 0 (0) | 0.5381 | |
| 2 | 31 | 30 (96.77) | 1 (3.22) | 5 | 0 (0) | 5 (100) | 0.0720 | |
| 3 | 61 | 54 (88.52) | 7 (11.47) | 39 | 12 (30.76) | 27 (69.23) | <0.0001 | |
| Attention | 0 | 1 | 1 (100) | 0 (0) | 1 | 1 (100) | 0 (0) | |
| 1 | 10 | 10 (100) | 0 (0) | 0 | 0 (0) | 0 (0) | 0.5188 | |
| 2 | 14 | 14 (100) | 0 (0) | 0 | 0 (0) | 0 (0) | 0.5102 | |
| 3 | 24 | 24 (100) | 0 (0) | 0 | 0 (0) | 0 (0) | 0.5012 | |
| 4 | 24 | 21 (87.5) | 3 (12.5) | 9 | 1 (11.11) | 8 (88.88) | 0.0291 | |
| 5 | 12 | 11 (91.66) | 1 (8.33) | 11 | 0 (0) | 11 (100) | 0.0277 | |
| 6 | 14 | 10 (71.42) | 4 (28.57) | 23 | 10 (43.47) | 13 (56.52) | 0.0888 | |
| 7 | 1 | 1 (100) | 0 (0) | 1 | 0 (0) | 0 (0) | 0.7074 | |
| Language | 0 | 8 | 8 (100) | 0 (0) | 8 | 8 (100) | 0 (0) | |
| 1 | 11 | 11 (100) | 0 (0) | 11 | 1 (9.09) | 10 (90.90) | 0.0119 | |
| 2 | 79 | 72 (91.13) | 7 (8.86) | 9 | 2 (22.22) | 7 (77.77) | 0.0239 | |
| 3 | 2 | 1 (50) | 1 (50) | 16 | 1 (100) | 15 (93.75) | 0.0829 | |
| Abstraction | 0 | 42 | 41 (97.61) | 1 (2.38) | 7 | 7 (100) | 0 (0) | 0.3173 |
| 1 | 10 | 9 (90) | 1 (10) | 0 | 0 (0) | 0 (0) | 0.5874 | |
| 2 | 47 | 41 (87.23) | 6 (12.76) | 37 | 5 (13.51) | 32 (86.46) | <0.0001 | |
| 3 | 1 | 1 (100) | 0 (0) | 7 | 7 (100) | 0 (0) | ||
| Delayed Recall | 0 | 46 | 46 (100) | 0 (0) | 3 | 3 (100) | 0 (0) | |
| 1 | 6 | 6 (100) | 0 (0) | 0 | 0 (0) | 0 (0) | 0.5381 | |
| 2 | 9 | 8 (88.88) | 1 (11.11) | 2 | 0 (0) | 2 (100) | 0.2093 | |
| 3 | 10 | 9 (90) | 1 (10) | 1 | 0 (0) | 1 (100) | 0.3137 | |
| 4 | 9 | 8 (88.88) | 1 (11.11) | 18 | 4 (22.22) | 14 (77.77) | 0.0024 | |
| 5 | 20 | 15 (75) | 5 (25) | 20 | 5 (25) | 15 (75) | 0.0071 | |
| Orientation | 0 | 2 | 2 (100) | 0 (0) | 1 | 1 (100) | 0 (0) | |
| 1 | 0 | 0 (0) | 0 (0) | 0 | 0 (0) | 0 (0) | ||
| 2 | 1 | 1 (100) | 0 (0) | 0 | 0 (0) | 0 (0) | 0.7074 | |
| 3 | 1 | 1 (100) | 0 (0) | 0 | 0 (0) | 0 (0) | 0.7074 | |
| 4 | 0 | 0 (0) | 0 (0) | 0 | 0 (0) | 0 (0) | ||
| 5 | 9 | 9 (100) | 0 (0) | 0 | 0 (0) | 0 (0) | 0.5221 | |
| 6 | 87 | 79 (90.80) | 8 (9.19) | 43 | 11 (25.58) | 32 (74.41) | <0.0001 | |
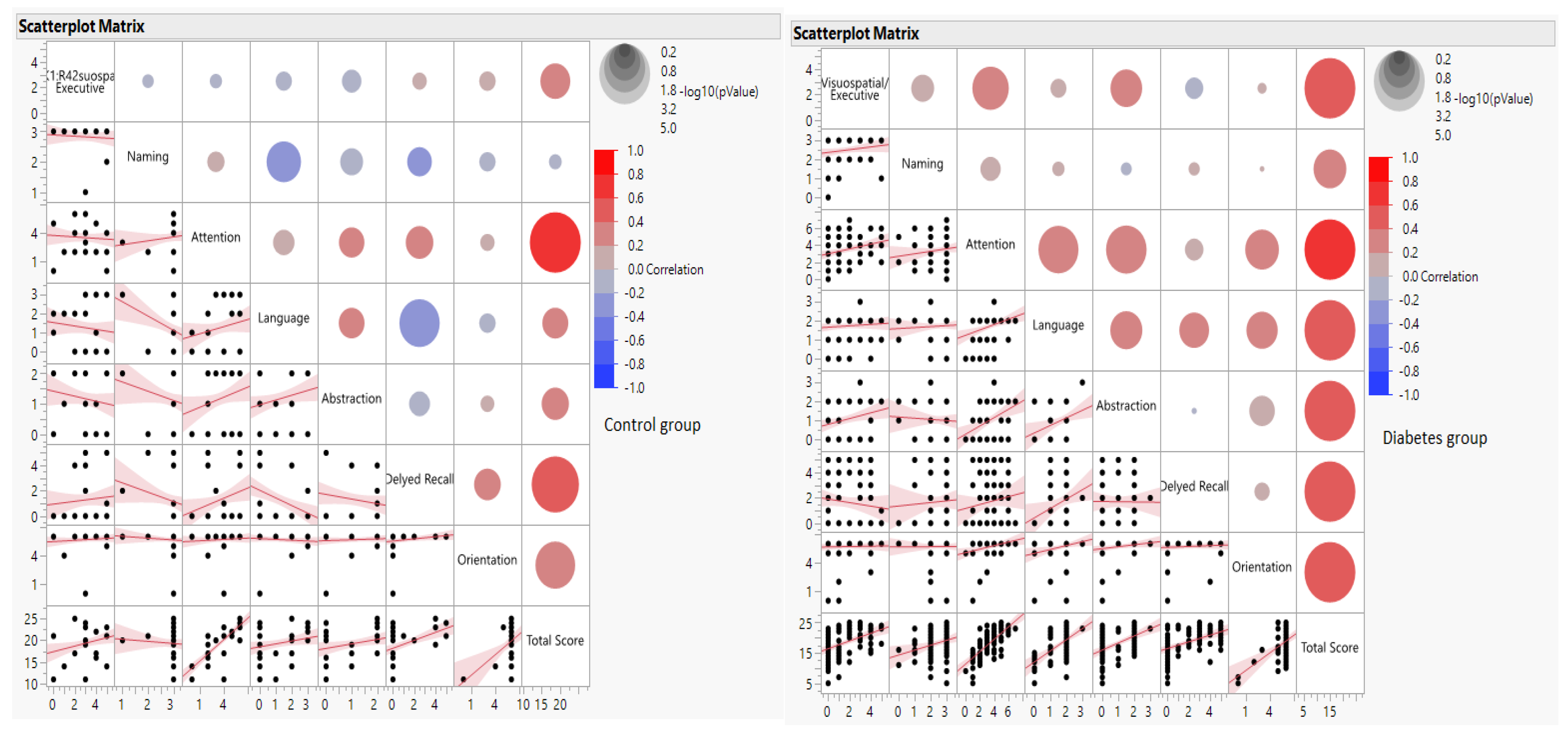
| Correlation with Total MOCA Score, r | Correlation Probability (p-Value) | |||
|---|---|---|---|---|
| Control | Diabetes | Control | Diabetes | |
| Visuospatial/Executive | 0.27 | 0.47 | 0.02 | <0.0001 |
| Naming | −0.07 | 0.26 | 0.55 | 0.01 |
| Attention | 0.79 | 0.71 | <0.0001 | <0.0001 |
| Language | 0.23 | 0.53 | 0.06 | <0.0001 |
| Abstraction | 0.24 | 0.51 | 0.04 | <0.0001 |
| Delayed Recall | 0.47 | 0.5 | <0.01 | <0.0001 |
| Orientation | 0.39 | 0.45 | 0.001 | <0.0001 |
| Total Score | 1 | 1 | <0.0001 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinattingal, N.; Mehdi, S.; Undela, K.; Wani, S.U.D.; Almuqbil, M.; Alshehri, S.; Shakeel, F.; Imam, M.T.; Manjula, S.N. Prevalence of Cognitive Decline in Type 2 Diabetes Mellitus Patients: A Real-World Cross-Sectional Study in Mysuru, India. J. Pers. Med. 2023, 13, 524. https://doi.org/10.3390/jpm13030524
Kinattingal N, Mehdi S, Undela K, Wani SUD, Almuqbil M, Alshehri S, Shakeel F, Imam MT, Manjula SN. Prevalence of Cognitive Decline in Type 2 Diabetes Mellitus Patients: A Real-World Cross-Sectional Study in Mysuru, India. Journal of Personalized Medicine. 2023; 13(3):524. https://doi.org/10.3390/jpm13030524
Chicago/Turabian StyleKinattingal, Nabeel, Seema Mehdi, Krishna Undela, Shahid Ud Din Wani, Mansour Almuqbil, Sultan Alshehri, Faiyaz Shakeel, Mohammad T. Imam, and Santhepete N. Manjula. 2023. "Prevalence of Cognitive Decline in Type 2 Diabetes Mellitus Patients: A Real-World Cross-Sectional Study in Mysuru, India" Journal of Personalized Medicine 13, no. 3: 524. https://doi.org/10.3390/jpm13030524
APA StyleKinattingal, N., Mehdi, S., Undela, K., Wani, S. U. D., Almuqbil, M., Alshehri, S., Shakeel, F., Imam, M. T., & Manjula, S. N. (2023). Prevalence of Cognitive Decline in Type 2 Diabetes Mellitus Patients: A Real-World Cross-Sectional Study in Mysuru, India. Journal of Personalized Medicine, 13(3), 524. https://doi.org/10.3390/jpm13030524