
Anti-VEGF Treatment of Diabetic Macular Edema in Denmark: Incidence, Burden of Therapy, and Forecasting Analyses



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Clinical Pathway of Patients with Diabetic Macular Edema
2.3. Treatment Commencement, Regimen, and Discontinuation
2.4. Data Analysis and Statistics
3. Results
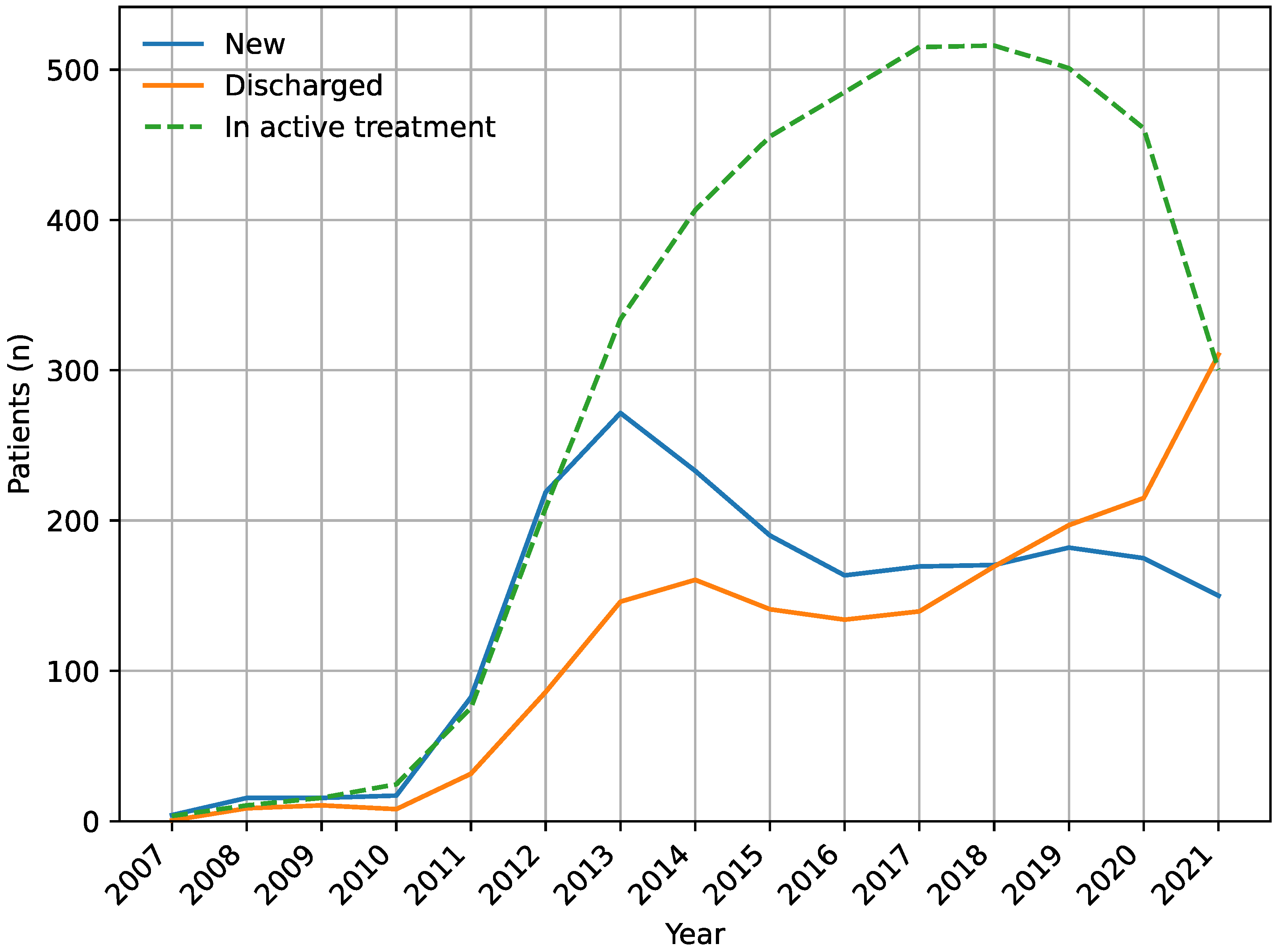
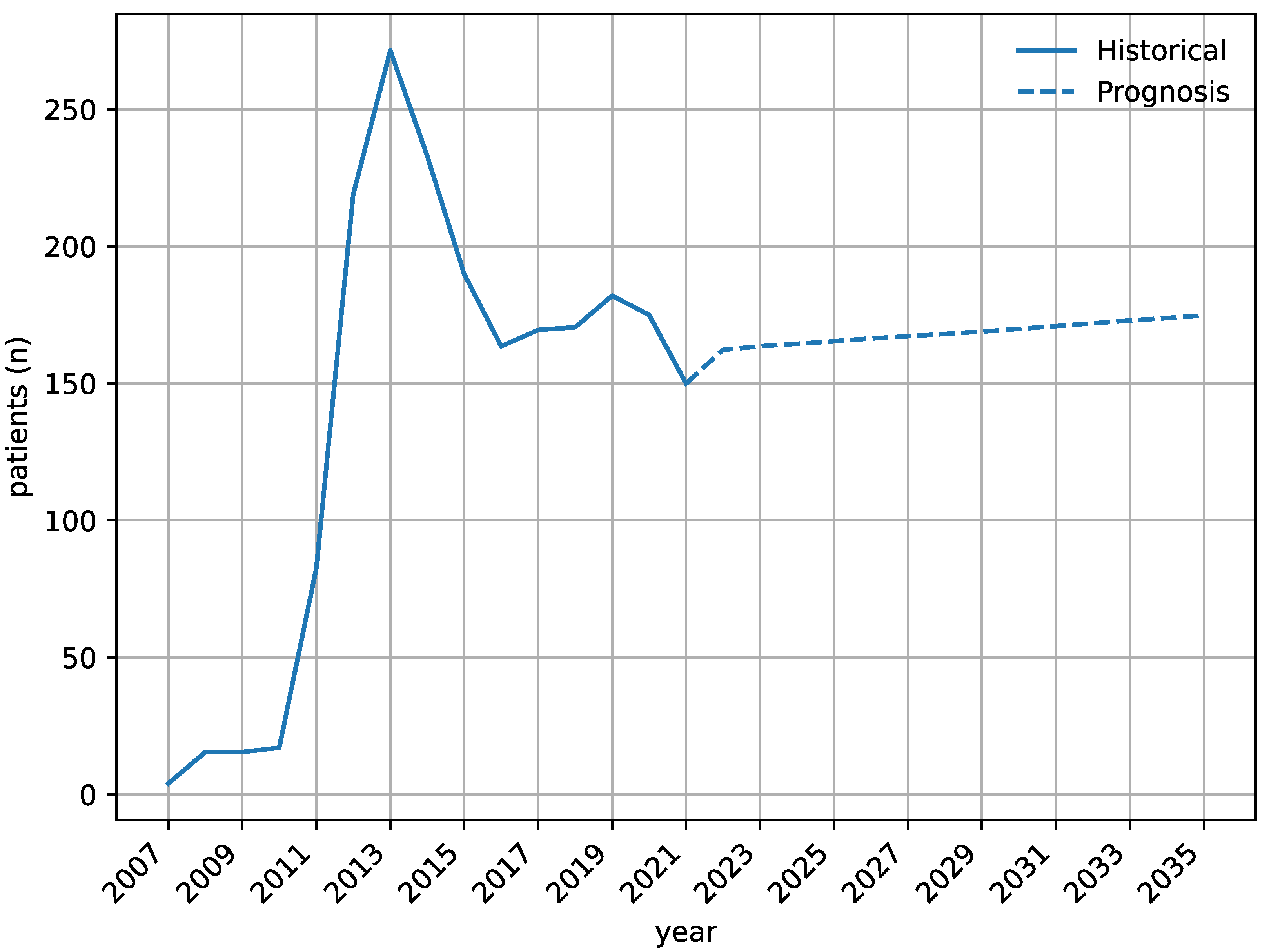
3.1. Number of Patients and Temporal Trends
3.2. Population Incidence of Patients with Diabetic Macular Edema Commenced in Anti-VEGF Therapy
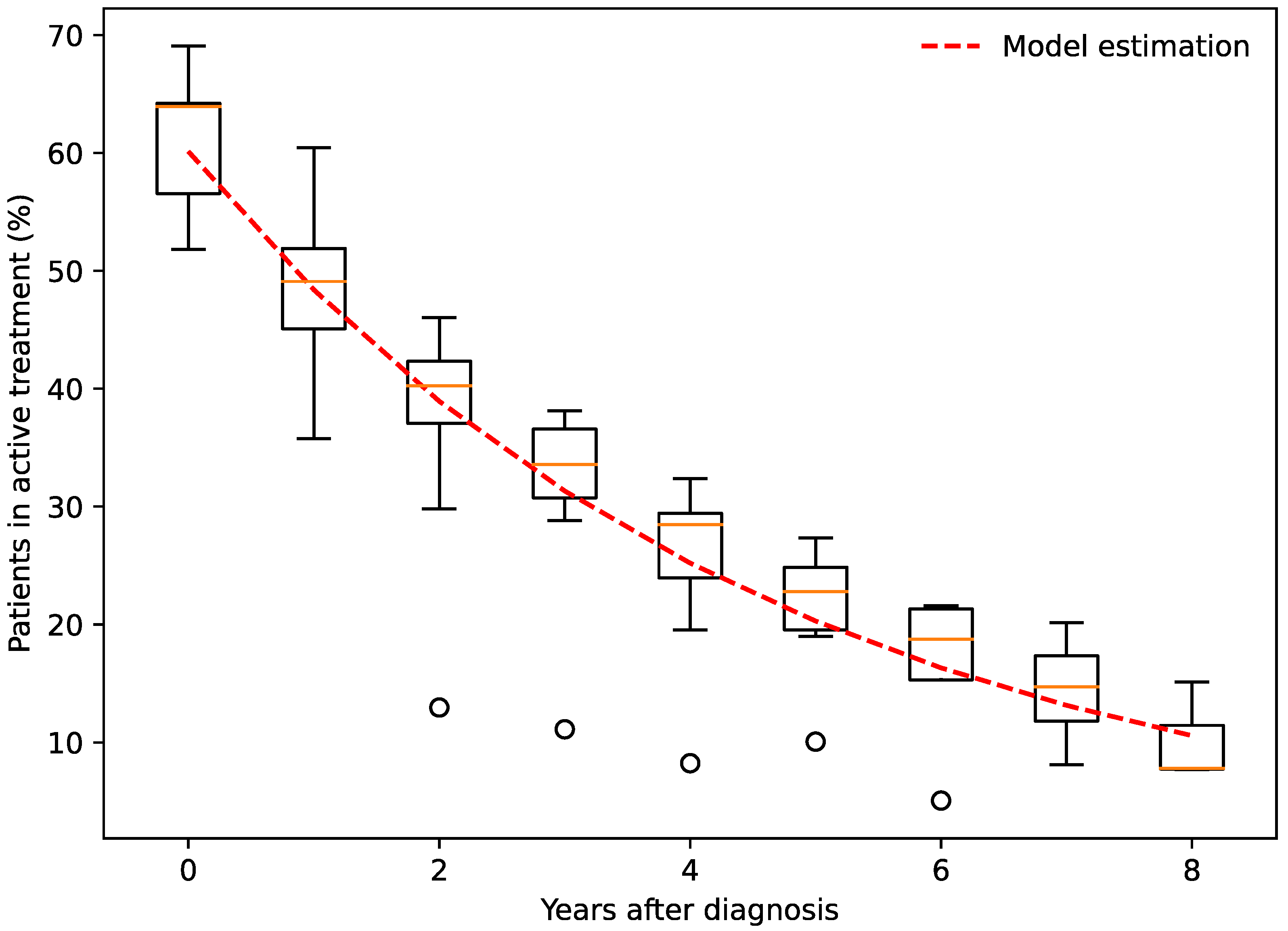
3.3. Proportion in Active Anti-VEGF Treatment over Time
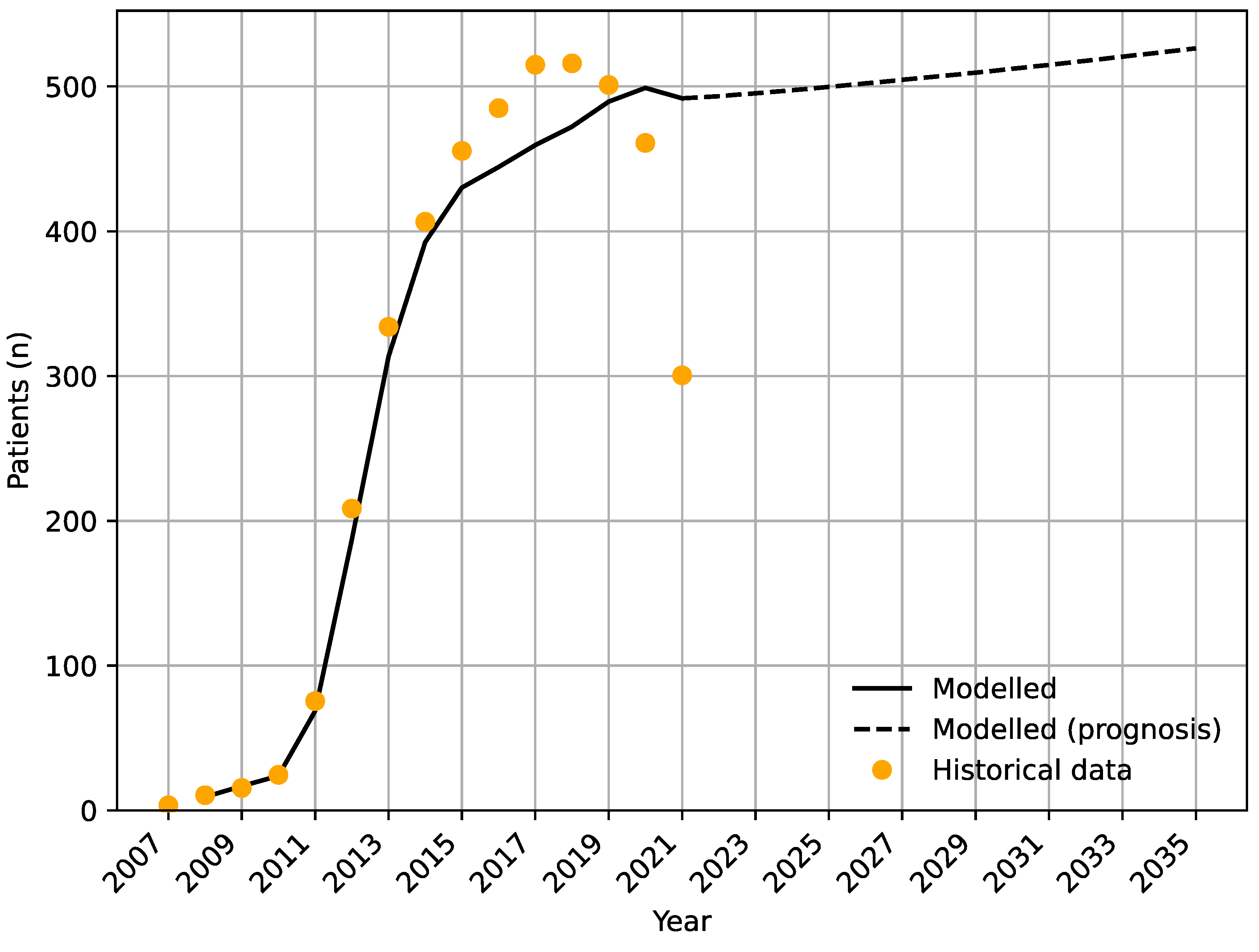
3.4. Modelling the Future Number of Patients with Diabetic Macular Edema in Anti-VEGF Treatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, A.; Lin, X.; Xu, J.; Shan, Y.; Pan, X.; Ye, J.; Shan, P.F. Global burden and gender disparity of vision loss associated with diabetes retinopathy. Acta Ophthalmol. 2021, 99, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Romero-Aroca, P.; Baget-Bernaldiz, M.; Pareja-Rios, A.; Lopez-Galvez, M.; Navarro-Gil, R.; Verges, R. Diabetic Macular Edema Pathophysiology: Vasogenic versus Inflammatory. J. Diabetes Res. 2016, 2016, 2156273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, M.S.; Rasmussen, M.; Grauslund, J.; Subhi, Y.; Cehofski, L.J. Proteomic analysis of vitreous humour of eyes with diabetic macular oedema: A systematic review. Acta Ophthalmol. 2022, 100, e1043–e1051. [Google Scholar] [CrossRef]
- Boyer, D.S.; Hopkins, J.J.; Sorof, J.; Ehrlich, J.S. Anti-vascular endothelial growth factor therapy for diabetic macular edema. Ther. Adv. Endocrinol. Metab. 2013, 4, 151–169. [Google Scholar] [CrossRef]
- ETDRS research group. Photocoagulation for diabetic macular edema. ETDRS report number 1. Arch Ophthalmol. 1985, 103, 1796–1806. [Google Scholar]
- Nguyen, Q.D.; Shah, S.M.; Heier, J.S.; Do, D.V.; Lim, J.; Boyer, D.; Abraham, P.; Campochiaro, P.A.; READ-2 Study Group. Primary End Point (Six Months) Results of the Ranibizumab for Edema of the mAcula in diabetes (READ-2) study. Ophthalmology 2009, 116, 2175–2181. [Google Scholar] [CrossRef]
- Massin, P.; Bandello, F.; Garweg, J.G.; Hansen, L.L.; Harding, S.P.; Larsen, M.; Mitchell, P.; Sharp, D.; Wolf-Schnurrbusch, U.E.; Gekkieva, M.; et al. Safety and efficacy of ranibizumab in diabetic macular edema (RESOLVE Study): A 12-month, randomized, controlled, double-masked, multicenter phase II study. Diabetes Care 2010, 33, 2399–2405. [Google Scholar] [CrossRef] [Green Version]
- Michaelides, M.; Kaines, A.; Hamilton, R.D.; Fraser-Bell, S.; Rajendram, R.; Quhill, F.; Boos, C.J.; Xing, W.; Egan, C.; Peto, T.; et al. A prospective randomized trial of intravitreal bevacizumab or laser therapy in the management of diabetic macular edema (BOLT study) 12-month data: Report 2. Ophthalmology 2010, 117, 1078–1086. [Google Scholar] [CrossRef]
- Nguyen, Q.D.; Brown, D.M.; Marcus, D.M.; Boyer, D.S.; Patel, S.; Feiner, L.; Gibson, A.; Sy, J.; Rundle, A.C.; Hopkins, J.J.; et al. Ranibizumab for diabetic macular edema: Results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology 2012, 119, 789–801. [Google Scholar] [CrossRef]
- Sedeh, F.B.; Scott, D.A.R.; Subhi, Y.; Sørensen, T.L. Prevalence of neovascular age-related macular degeneration and geographic atrophy in Denmark. Dan. Med. J. 2017, 64, A5422. [Google Scholar] [PubMed]
- Potapenko, I.; la Cour, M. Modelling and prognostication of growth in the number of patients treated for neovascular age-related macular degeneration. Acta Ophthalmol. 2021, 99, e1348–e1353. [Google Scholar] [CrossRef] [PubMed]
- Subhi, Y.; Sørensen, T.L. Neovascular Age-Related Macular Degeneration in the Very Old (≥90 Years): Epidemiology, Adherence to Treatment, and Comparison of Efficacy. J. Ophthalmol. 2017, 2017, 7194927. [Google Scholar] [CrossRef] [PubMed]
- Gharehbagh, S.S.; Subhi, Y.; Sørensen, T.L. Efficacy of aflibercept for polypoidal choroidal vasculopathy in Caucasians. Acta Ophthalmol. 2018, 96, e94–e95. [Google Scholar] [CrossRef] [Green Version]
- Petri, A.S.; Boysen, K.; Cehofski, L.J.; van Dijk, E.H.C.; Dysli, C.; Fuchs, J.; Mastropasqua, R.; Subhi, Y. Intravitreal Injections with Vascular Endothelial Growth Factor Inhibitors: A Practical Approach. Ophthalmol. Ther. 2020, 9, 191–203. [Google Scholar] [CrossRef] [Green Version]
- Fu, D.J.; Keenan, T.D.; Faes, L.; Lim, E.; Wagner, S.K.; Moraes, G.; Huemer, J.; Kern, C.; Patel, P.J.; Balaskas, K.; et al. Insights from Survival Analyses During 12 Years of Anti-Vascular Endothelial Growth Factor Therapy for Neovascular Age-Related Macular Degeneration. JAMA Ophthalmol. 2021, 139, 57–67. [Google Scholar] [CrossRef]
- Diabetic Retinopathy Clinical Research Network; Wells, J.A.; Glassman, A.R.; Ayala, A.R.; Jampol, L.M.; Aiello, L.P.; Antoszyk, A.N.; Arnold-Bush, B.; Baker, C.W.; Bressler, N.M.; et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N. Engl. J. Med. 2015, 372, 1193–1203. [Google Scholar] [CrossRef] [Green Version]
- Glassman, A.R.; Wells, J.A., 3rd; Josic, K.; Maguire, M.G.; Antoszyk, A.N.; Baker, C.; Beaulieu, W.T.; Elman, M.J.; Jampol, L.M.; Sun, J.K. Five-Year Outcomes after Initial Aflibercept, Bevacizumab, or Ranibizumab Treatment for Diabetic Macular Edema (Protocol T Extension Study). Ophthalmology 2020, 127, 1201–1210. [Google Scholar] [CrossRef]
- Van Aken, E.; Favreau, M.; Ramboer, E.; Denhaerynck, K.; MacDonald, K.; Abraham, I.; Brié, H. Real-World Outcomes in Patients with Diabetic Macular Edema Treated Long Term with Ranibizumab (VISION Study). Clin. Ophthalmol. 2020, 14, 4173–4185. [Google Scholar] [CrossRef]
- Zirpel, J.J.; Pfister, I.B.; Gerhardt, C.; Garweg, J.G. Long-term outcomes of intravitreal therapy for symptomatic diabetic macular oedema in a real-world setting in Switzerland. Graefes Arch Clin. Exp. Ophthalmol. 2021, 259, 3569–3578. [Google Scholar] [CrossRef]
- Arevalo, J.F.; Lasave, A.F.; Wu, L.; Acon, D.; Farah, M.E.; Gallego-Pinazo, R.; Alezzandrini, A.A.; Fortuna, V.; Quiroz-Mercado, H.; Salcedo-Villanueva, G.; et al. Intravitreal bevacizumab for diabetic macular oedema: 5-year results of the Pan-American Collaborative Retina Study group. Br. J. Ophthalmol. 2016, 100, 1605–1610. [Google Scholar] [CrossRef]
- Rasmussen, A.; Bloch, S.B.; Fuchs, J.; Hansen, L.H.; Larsen, M.; LaCour, M.; Lund-Andersen, H.; Sander, B. A 4-year longitudinal study of 555 patients treated with ranibizumab for neovascular age-related macular degeneration. Ophthalmology 2013, 120, 2630–2636. [Google Scholar] [CrossRef] [PubMed]
- Statistics Denmark: The Population. Available online: https://www.dst.dk/en/Statistik/dokumentation/documentationofstatistics/the-population (accessed on 12 February 2023).
- Statistics Denmark: Population Projections. Available online: https://www.dst.dk/en/Statistik/dokumentation/documentationofstatistics/population-projections (accessed on 12 February 2023).
- Danish Ophthalmological Society: National Guideline for Screening of Diabetic Retinopathy (in Danish). Available online: https://dansk-oftalmologisk-selskab.dk/wp-content/uploads/2021/05/National-retningslinje-for-screening-af-diabetisk-retinopati.pdf (accessed on 12 February 2023).
- Petrella, R.J.; Blouin, J.; Davies, B.; Barbeau, M. Prevalence, Demographics, and Treatment Characteristics of Visual Impairment due to Diabetic Macular Edema in a Representative Canadian Cohort. J. Ophthalmol. 2012, 2012, 159167. [Google Scholar] [CrossRef] [Green Version]
- Jandorf, S.; Krogh Nielsen, M.; Sørensen, K.; Sørensen, T.L. Low health literacy levels in patients with chronic retinal disease. BMC Ophthalmol. 2019, 19, 174. [Google Scholar] [CrossRef] [Green Version]
- Safai, N.; Carstensen, B.; Vestergaard, H.; Ridderstråle, M. Impact of a multifactorial treatment programme on clinical outcomes and cardiovascular risk estimates: A retrospective cohort study from a specialised diabetes centre in Denmark. BMJ Open 2018, 8, e019214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jørgensen, M.E.; Almdal, T.P.; Carstensen, B. Time trends in mortality rates in type 1 diabetes from 2002 to 2011. Diabetologia 2013, 56, 2401–2404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jørgensen, M.E.; Almdal, T.P.; Faerch, K. Reduced incidence of lower-extremity amputations in a Danish diabetes population from 2000 to 2011. Diabet. Med. 2014, 31, 443–447. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level of DR | Subgroup | Diabetes in Control * | Diabetes Not in Control or No Information |
|---|---|---|---|
| 0: No DR | 24–48 ** months | 12–24 months | |
| 1: Mild NPDR | No DME | 24 months | 12 months |
| DME without CSME | 3–6 months | 3 months | |
| 2: Moderate NPDR | No DME | 12–24 months | 6–12 months |
| DME without CSME | 3–6 months | 3 months | |
| 3: Severe NPDR | No DME | 3–6 months | 3 months |
| DME without CSME | 3 months | 3 months | |
| 4: PDR | New or recurring | Referral to tertiary center | Referral to tertiary center |
| Stable (after treatment) | 6–12 *** months | 3–12 months | |
| CSME | New or recurring | Referral to tertiary center | Referral to tertiary center |
| Stable (after treatment) | 3 *** months | 3 months |
| Age Category | Males | Females |
|---|---|---|
| <40 years | 1.2 | 1.0 |
| 40–44 years | 7.0 | 2.4 |
| 45–49 years | 12.3 | 5.1 |
| 50–54 years | 22.4 | 8.3 |
| 55–59 years | 27.6 | 18.5 |
| 60–64 years | 39.0 | 23.8 |
| 65–69 years | 45.2 | 27.1 |
| 70–74 years | 52.9 | 22.1 |
| 75–79 years | 44.9 | 27.5 |
| 80–84 years | 25.2 | 17.9 |
| 85–89 years | 24.7 | 16.3 |
| ≥90 years | 3.0 | 10.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Subhi, Y.; Potapenko, I.; Hajari, J.N.; la Cour, M. Anti-VEGF Treatment of Diabetic Macular Edema in Denmark: Incidence, Burden of Therapy, and Forecasting Analyses. J. Pers. Med. 2023, 13, 546. https://doi.org/10.3390/jpm13030546
Subhi Y, Potapenko I, Hajari JN, la Cour M. Anti-VEGF Treatment of Diabetic Macular Edema in Denmark: Incidence, Burden of Therapy, and Forecasting Analyses. Journal of Personalized Medicine. 2023; 13(3):546. https://doi.org/10.3390/jpm13030546
Chicago/Turabian StyleSubhi, Yousif, Ivan Potapenko, Javad Nouri Hajari, and Morten la Cour. 2023. "Anti-VEGF Treatment of Diabetic Macular Edema in Denmark: Incidence, Burden of Therapy, and Forecasting Analyses" Journal of Personalized Medicine 13, no. 3: 546. https://doi.org/10.3390/jpm13030546
APA StyleSubhi, Y., Potapenko, I., Hajari, J. N., & la Cour, M. (2023). Anti-VEGF Treatment of Diabetic Macular Edema in Denmark: Incidence, Burden of Therapy, and Forecasting Analyses. Journal of Personalized Medicine, 13(3), 546. https://doi.org/10.3390/jpm13030546