
Comparison between Cardiac Output and Pulmonary Vascular Pressure Measured by Indirect Fick and Thermodilution Methods
 ,
,
Abstract
:1. Introduction
2. Methods
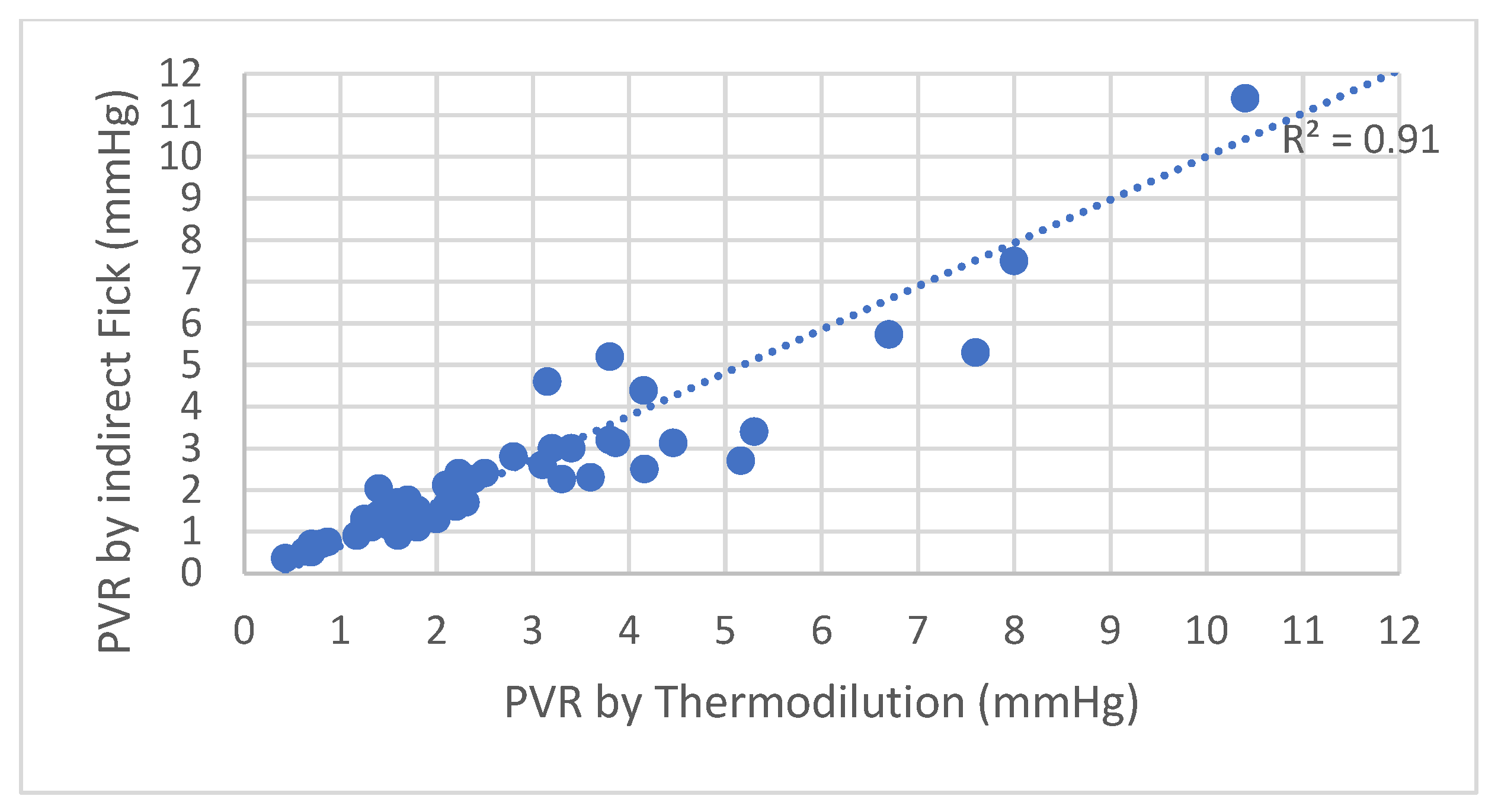
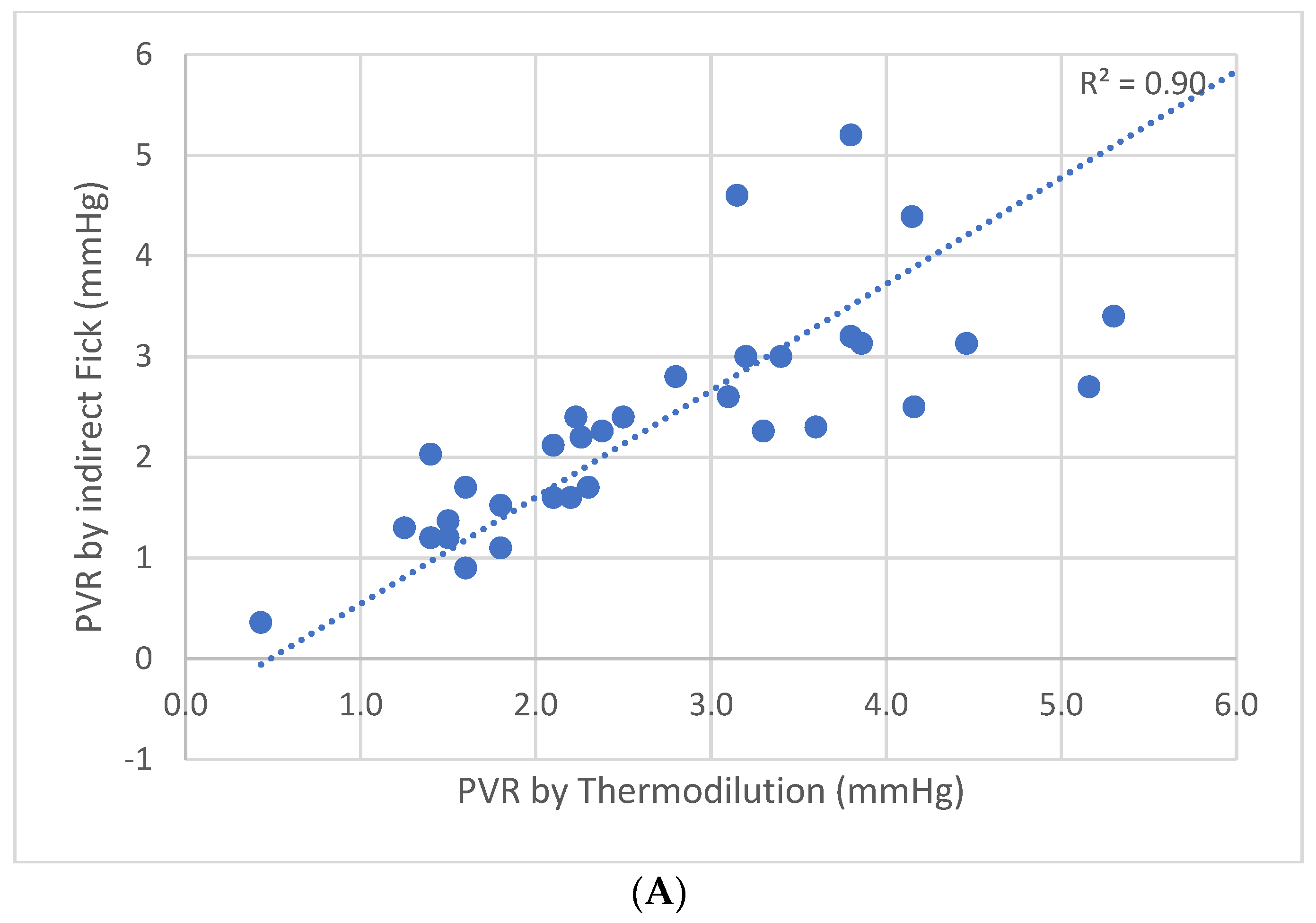
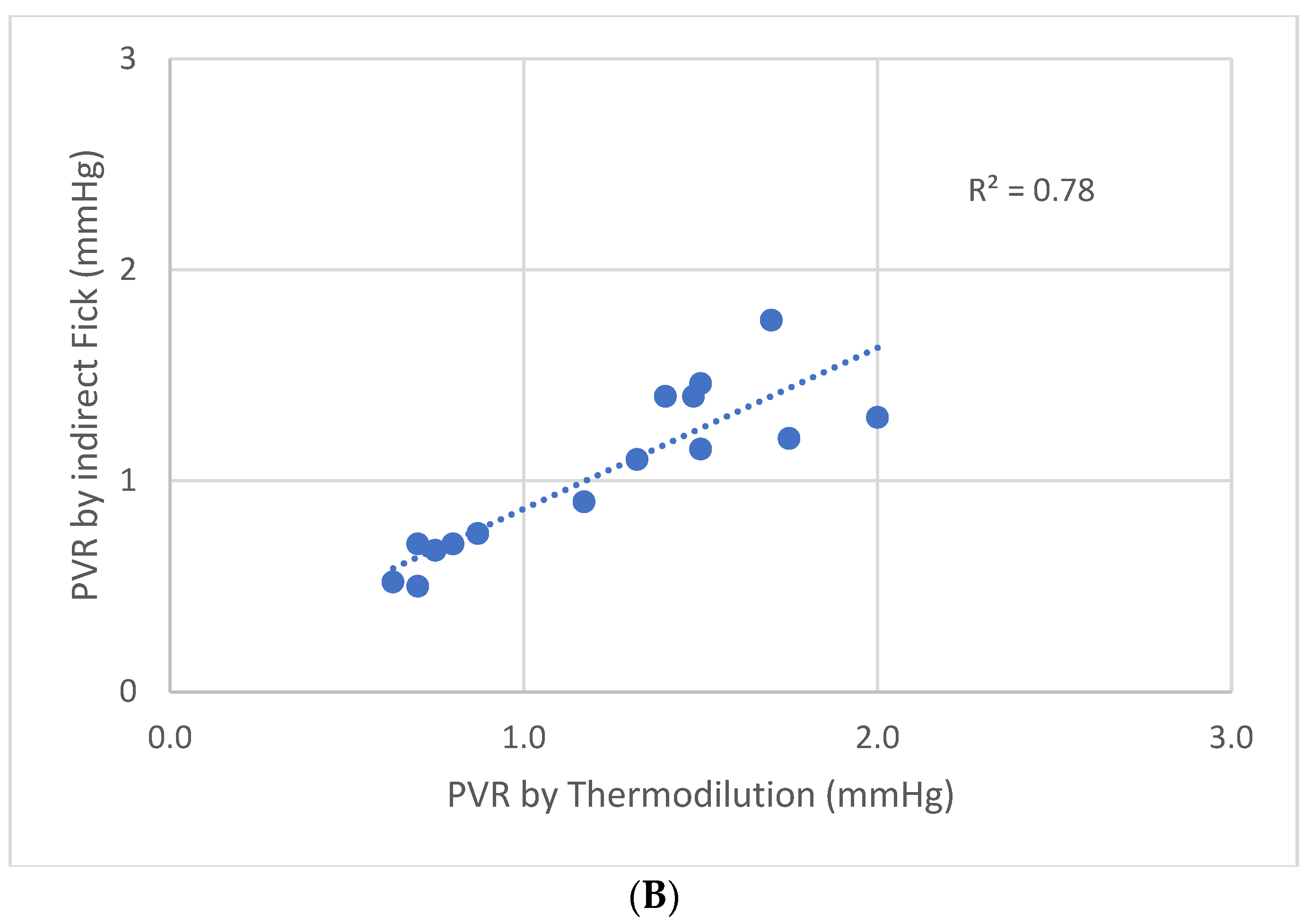
3. Results
4. Discussion
5. Conclusions
- The discrepancy between the thermodilution and indirect Fick methods has been demonstrated before. On the other hand, the results of other studies implied that this discrepancy is not clinically relevant. This study, for the first time, demonstrates that this discrepancy is clinically more relevant when mPAP is over 20 mmHg, but may be left unattended when mPAP is normal, thus confirming that the new cutoff point for mPAP has clear implications also on the discrepancy between the thermodilution and indirect Fick methods.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoeper, M.M.; Maier, R.; Tongers, J.; Niedermeyer, J.; Hohlfeld, J.M.; Hamm, M.; Fabel, H. Determination of Cardiac Output by the Fick Method, Thermodilution, and Acetylene Rebreathing in Pulmonary Hypertension. Am. J. Respir. Crit. Care Med. 1999, 160, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Cigarroa, R.G.; Lange, R.A.; Williams, R.H.; Bedotto, J.B.; Hillis, L. Underestimation of cardiac output by thermodilution in patients with tricuspid regurgitation. Am. J. Med. 1989, 86, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Heerdt, P.M.; Pond, C.G.; Blessios, G.A.; Rosenbloom, M. Inaccuracy of cardiac output by thermodilution during acute tricuspid regurgitation. Ann. Thorac. Surg. 1992, 53, 706–708. [Google Scholar] [CrossRef] [PubMed]
- Hodges, M.; Sergeant, S.; Downs, J.B.; Mitchell, L.A. Thermodilution and Fick cardiac index determinations following cardiac surgery. Crit. Care Med. 1975, 3, 182–184. [Google Scholar] [CrossRef] [PubMed]
- Enghoff, E.; Michaëlsson, M.; Pavek, K.; Sjögren, S. A comparison between the thermal dilution method and the direct Fick and the dye dilution methods for cardiac output measurements in man. Acta Soc. Med. Ups. 1970, 75, 157–170. [Google Scholar]
- Kendrick, A.H.; West, J.; Papouchado, M.; Rozkovec, A. Direct Fick cardiac output: Are assumed values of oxygen consumption acceptable? Eur. Heart J. 1988, 9, 337–342. [Google Scholar] [CrossRef]
- Wolf, A.; Pollman, M.J.; Trindade, P.T.; Fowler, M.B.; Alderman, E.L. Use of assumed versus measured oxygen consumption for the determination of cardiac output using the Fick principle. Catheter. Cardiovasc. Diagn. 1998, 43, 372–380. [Google Scholar] [CrossRef]
- Narang, N.; Gore, M.O.; Snell, P.G.; Ayers, C.R.; Lorenzo, S.; Carrick-Ranson, G.; Babb, T.G.; Levine, B.D.; Khera, A.; de Lemos, J.A.; et al. Accuracy of Estimating Resting Oxygen Uptake and Implications for Hemodynamic Assessment. Am. J. Cardiol. 2012, 109, 594–598. [Google Scholar] [CrossRef]
- Thrush, D.N. Spirometric versus Fick-derived oxygen consumption: Which method is better? Crit. Care Med. 1996, 24, 91–95. [Google Scholar] [CrossRef]
- Fares, W.H.; Blanchard, S.K.; Stouffer, G.A.; Chang, P.P.; Rosamond, W.D.; Ford, H.J.; Aris, R.M. Thermodilution and Fick cardiac outputs differ: Impact on pulmonary hypertension evaluation. Can. Respir. J. 2012, 19, 261–266. [Google Scholar] [CrossRef]
- Opotowsky, A.R.; Hess, E.; Maron, B.A.; Brittain, E.L.; Baron, A.E.; Maddox, T.M.; Alshawabkeh, L.I.; Wertheim, B.M.; Xu, M.; Assad, T.R. Thermodilution vs Estimated Fick Cardiac Output Measurement in Clinical Practice: An Analysis of Mortality From the Veterans Affairs Clinical Assessment, Reporting, and Tracking (VA CART) Program and Vanderbilt University. JAMA Cardiol. 2017, 2, 1090–1099. [Google Scholar] [CrossRef] [PubMed]
- Grafton, G.; Cascino, T.M.; Perry, D.; Ashur, C.; Koelling, T.M. Resting Oxygen Consumption and Heart Failure: Importance of Measurement for Determination of Cardiac Output With the Use of the Fick Principle. J. Card. Fail. 2019, 26, 664–672. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacz, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. ESC/ERS Guidelines for diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2023, 61, 1–879. [Google Scholar]
- Swan, H.J.C.; Ganz, W.; Forrester, J.; Marcus, H.; Diamond, G.; Chonette, D. Catheterization of the Heart in Man with Use of a Flow-Directed Balloon-Tipped Catheter. N. Engl. J. Med. 1970, 283, 447–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadota, L.T. Theory and application of thermodilution cardiac output measurement: A review. Heart Lung 1985, 14, 605–616. [Google Scholar]
- Fick, A. Uber die Messung des Blutquantums in Den Herzventrikeln. Sitz. Der Physmed. Ges. Zu Wurzbg. 1870, 1, 16–17. [Google Scholar]
- Stewart, G.N. Researches on the circulation time and on the influences, which affect it. The output of the heart. J. Physiol. 1897, 22, 159–183. [Google Scholar] [CrossRef]
- Ganz, W.; Donoso, R.; Marcus, H.S.; Forrester, J.S.; Swan, H.J. A new technique for measurement of cardiac output by thermodilution in man. Am. J. Cardiol. 1971, 27, 392–396. [Google Scholar] [CrossRef]
- Dehmer, G.J.; Firth, B.G.; Hillis, L.D. Oxygen consumption in adult patients during cardiac catheterization. Clin. Cardiol. 1982, 5, 436–440. [Google Scholar] [CrossRef]
- Bergstra, A.; Van Dijk, R.B.; Hillege, H.L.; Lie, K.I.; Mook, G.A. Assumed oxygen consumption based on calculation from dye dilution cardiac output: An improved formula. Eur. Hear. J. 1995, 16, 698–703. [Google Scholar] [CrossRef]
- La Farge, C.G.; Miettinen, O.S. The estimation of oxygen consumption. Cardiovasc. Res. 1970, 4, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Smithies, M.; Bihari, D.J. Delivery dependent oxygen consumption: Asking the wrong questions and not getting any answers. Crit. Care Med. 1993, 21, 1622–1626. [Google Scholar] [CrossRef] [PubMed]
- Fakler, U.; Pauli, C.; Hennig, M.; Sebening, W.; Hess, J. Assumed oxygen consumption frequently results in large errors in the determination of cardiac output. J. Thorac. Cardiovasc. Surg. 2005, 130, 272–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narang, N.; Thibodeau, J.; Levine, B.D.; Gore, M.O.; Ayers, C.R.; Lange, R.A.; Cigarroa, J.E.; Turer, A.T.; De Lemos, J.A.; McGuire, D.K. Inaccuracy of Estimated Resting Oxygen Uptake in the Clinical Setting. Circulation 2014, 129, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Chase, P.J.; Davis, P.G.; Wideman, L.; Starnes, J.W.; Schulz, M.R.; Bensimhon, D.R. Comparison of Estimations Versus Measured Oxygen Consumption at Rest in Patients With Heart Failure and Reduced Ejection Fraction Who Underwent Right-Sided Heart Catheterization. Am. J. Cardiol. 2015, 116, 1724–1730. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Higginbotham, M.B.; Cobb, F.R. Exercise training in patients with severe left ventricular dysfunction. Hemodynamic and metabolic effects. Circulation 1988, 78, 506–515. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Poole, D.C.; Musch, T.I. Effect of heart failure on muscle capillary geometry: Implications for O2 exchange. Med. Sci. Sport. Exerc. 1998, 30, 1230–1237. [Google Scholar] [CrossRef]
- Springer, J.; Springer, J.I.; Anker, S.D. Muscle wasting and sarcopenia in heart failure and beyond: Update 2017. ESC Heart Fail 2017, 4, 492–498. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Guazzi, M.; Boriani, G.; Cicoira, M.; Corra, U.; Dalla Libera, L.; Working Group ‘Exercise Physiology, Sport Cardiology and Cardiac Rehabilitation’of the Italian Society of Cardiology (Italian Federation of Cardiology). Exercise intolerance in chronic heart failure: Mechanisms and therapies. Part I. Eur. J. Prev. Cardiol. 2010, 17, 643–648. [Google Scholar] [CrossRef]
- Hambrecht, R.; Niebauer, J.; Fiehn, E.; Kälberer, B.; Offner, B.; Hauer, K.; Riede, U.; Schlierf, G.; Kübler, W.; Schuler, G. Physical training in patients with stable chronic heart failure: Effects on cardiorespiratory fitness and ultrastructural abnormalities of leg muscles. J. Am. Coll. Cardiol. 1995, 25, 1239–1249. [Google Scholar] [CrossRef] [Green Version]




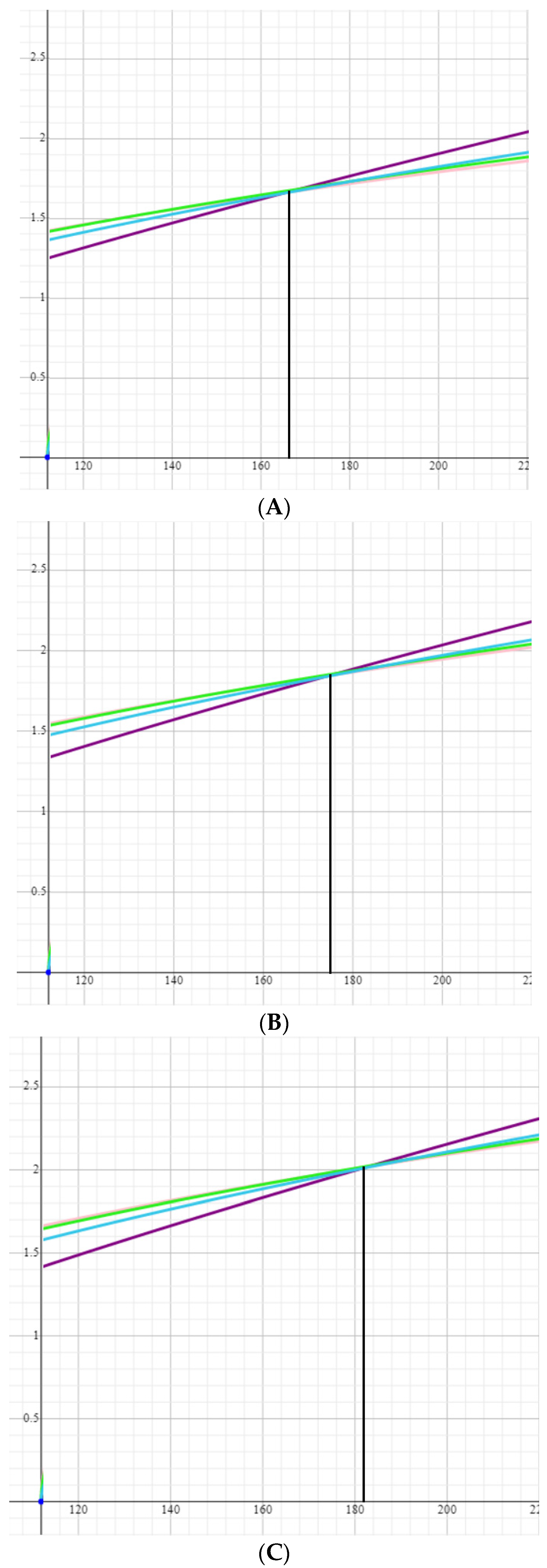
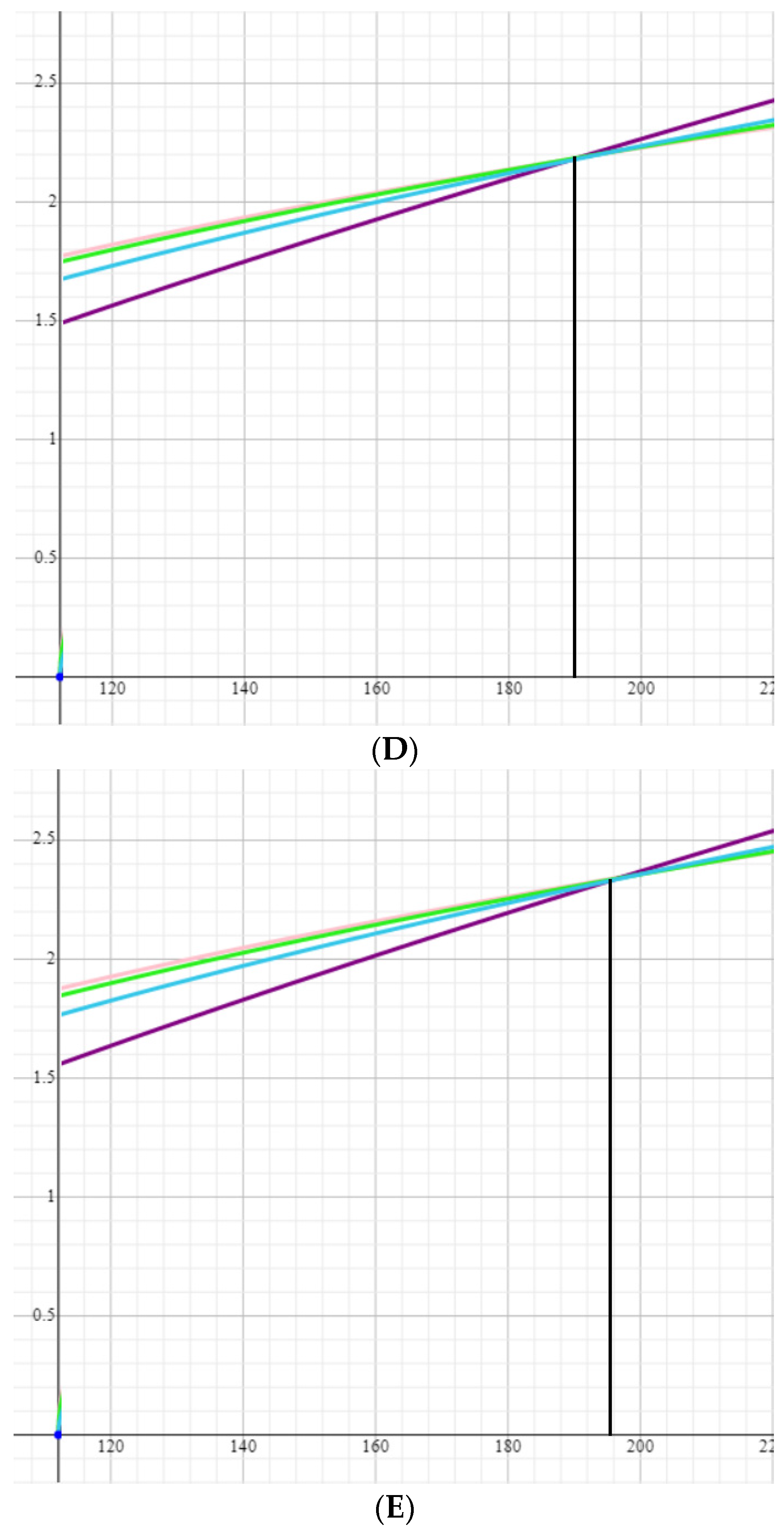
 —Gehan and George formula,
—Gehan and George formula,  —Haycock formula,
—Haycock formula,  —Mosteller formula,
—Mosteller formula,  —Dubois formula.
—Gehan and George formula, —Haycock formula, —Mosteller formula, —Dubois formula.
—Dubois formula.
—Gehan and George formula, —Haycock formula, —Mosteller formula, —Dubois formula.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AGE (YEARS) | 69.5 ± 12.5 |
| MALE GENDER | 13 (24%) |
| NYHA FUNCTIONAL CLASS | |
| I | 2 (3.8%) |
| II | 27 (51.9%) |
| III | 18 (34.6%) |
| IV | 5 (9.6%) |
| COMORBIDITIES | |
| HYPERTENSION | 28 (51%) |
| DIABETES MELLITUS | 13 (24%) |
| DYSLIPIDEMIA | 35 (64%) |
| OBESITY | 14 (25%) |
| SMOKING | 4 (7%) |
| OBSTRUCTIVE CORONARY ARTERY DISEASE | 10 (18%) |
| PERIPHERAL ARTERY DISEASE INVOLVING CAROTID ARTERY | 1 (2%) |
| PERIPHERAL ARTERY DISEASE INVOLVING OTHER ARTERIES | 1 (2%) |
| S.P. MYOCARDIAL INFARCTION | 4 (7%) |
| ATRIAL FIBRILLATION OR FLUTTER | 18 (33%) |
| S.P. PCI | 34 (62%) |
| S.P. CABG | 2 (4%) |
| CEREBROVASCULAR DISEASE | 5 (9%) |
| S.P. PERIPHERAL EMBOLUS | 3 (5%) |
| THYROID DISEASE | 9 (16%) |
| CHRONIC OBSTRUCTIVE PULMONARY DISEASE | 5 (9%) |
| SIGNIFICANT REGURGITATING VALVULAR HEART DISEASE | 9 (17%) |
| OBSTRUCTIVE SLEEP APNEA | 6 (11%) |
| CHRONIC RENAL DISEASE | 32 (60%) |
| GFR > 90 | 20 (36%) |
| GFR 60–90 | 15 (27%) |
| GFR 30–90 | 18 (33%) |
| GFR < 30 | 2 (4%) |
| CONGENITAL HEART DISEASE | 1 (2%) |
| AUTOIMMUNE DISEASE | 5 (9%) |
| VENOUS THROMBOEMBOLIC DISEASE | 7 (13%) |
| CIRRHOSIS | 2 (4%) |
| S.P. MALIGNANCY | 3 (5%) |
| TREATMENT | |
| ACEI OR ARB | 23 (42%) |
| BETA-BLOCKERS | 25 (45%) |
| MINERALOCORTICOID RECEPTOR ANTAGONISTS | 6 (11%) |
| DIURETICS | 22 (40%) |
| CALCIUM CHANNEL BLOCKERS | 12 (22%) |
| LIPID-LOWERING DRUGS | 29 (53%) |
| ANTIAGGREGANTS | 26 (47%) |
| ANTICOAGULANTS | 20 (36%) |
| HYPOGLYCEMICS | 10 (18%) |
| SPECIFIC TREATMENT AGAINST PULMONARY HYPERTENSION | 8 (15%) |
| PHOSPHODIESTERASE-5 INHIBITORS | 4 (50%) |
| PROSTAGLANDIN AND PROSTACYCLIN ANALOGS | 2 (25%) |
| ENDOTHELIN RECEPTOR ANTAGONISTS | 2 (25%) |
| ECHOCARDIOGRAPHIC PARAMETERS | |
| LEFT VENTRICULAR EJECTION FRACTION (EF, %) | |
| EF ≥ 50 | 51 (93%) |
| EF 40–50 | 2 (3.5%) |
| EF < 40 | 2 (3.5%) |
| MEAN THICKNESS (MM) | 10.7 ± 1.6 |
| LEFT VENTRICULAR MASS INDEXED (GR/M2) | 79.3 ± 37.1 |
| DIASTOLIC DYSFUNCTION GRADE | |
| IMPAIRED RELAXATION | 24 (52%) |
| PSEUDONORMAL FILLING PATTERN | 11 (24%) |
| RESTRICTIVE FILLING PATTERN | 7 (15%) |
| INCONCLUSIVE | 4 (9%) |
| Mean Pulmonary Arterial Pressure (mmHg) | |
|---|---|
| ≥25 | 26 (47%) |
| <25 | 29 (53%) |
| >20 | 40 (73%) |
| ≤20 | 15 (27%) |
| Mean PCWP (mmHg) | |
| ≥15 | 24 (44%) |
| <15 | 31 (56%) |
| LVEDP (mmHg) | |
| ≥15 | 22 (46%) |
| <15 | 26 (54%) |
| RVEDP (mmHg) | |
| ≥10 | 36 (79%) |
| <10 | 16 (31%) |
| Mean right atrial pressure (mmHg) | |
| ≥10 | 15 (29%) |
| <10 | 36 (71%) |
| Mean systemic arterial pressure (mmHg) | |
| ≥110 | 11 (25%) |
| <110 | 43 (75%) |
| Authors, Year | Name | Equation | Cohort Summary |
|---|---|---|---|
| Dehmer, Firth and Hillis, 1970 [19] | Dehmer | VO2 = 125 × BSA * | n = 108, mean age 49 years, 64% male, 9% cardiomyopathy |
| LaFarge and Mettinen, 1970 [21] | LaFarge | VO2 = 138.1 − (11.49 × log age) + 0.378 × HR) × BSA * for menVO2 = 138.1 − (17.04 × log age) + 0.378 × HR) × BSA * for women | n = 879, mean age not provided, range 3–40 years, 59% male, % cardiomyopathy |
| Bergstra, van Dijk, Hillege, Lie and Mook, 1995 [20] | Bergstra | VO2 = 157.3 × BSA * + 10 − (10.5 × log age) + 4.8 for menVO2 = 157.3 × BSA * − (10.5 × log age) + 4.8 for women | n = 250, mean age 34.6 years, 57% male, % cardiomyopathy not provided |
| Name of the Formula | Formula |
|---|---|
| Haycock | BSA (m2) = 0.024265 × Height (cm)0.3964 × Weight (kg)0.5378 |
| DuBois and DuBois | BSA (m2) = 0.20247 × Height (cm)0.725 × Weight (kg)0.0.425 |
| Gehan and George | BSA (m2) = 0.0235 × Height (cm)0.42246 × Weight (kg)0.51456 |
| Mosteller | BSA (m2) = ([Height (cm) × Weight (kg)]/3600)1/2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volodarsky, I.; Kerzhner, K.; Haberman, D.; Cuciuc, V.; Poles, L.; Blatt, A.; Kirzhner, E.; George, J.; Gandelman, G. Comparison between Cardiac Output and Pulmonary Vascular Pressure Measured by Indirect Fick and Thermodilution Methods. J. Pers. Med. 2023, 13, 559. https://doi.org/10.3390/jpm13030559
Volodarsky I, Kerzhner K, Haberman D, Cuciuc V, Poles L, Blatt A, Kirzhner E, George J, Gandelman G. Comparison between Cardiac Output and Pulmonary Vascular Pressure Measured by Indirect Fick and Thermodilution Methods. Journal of Personalized Medicine. 2023; 13(3):559. https://doi.org/10.3390/jpm13030559
Chicago/Turabian StyleVolodarsky, Igor, Katerina Kerzhner, Dan Haberman, Valeri Cuciuc, Lion Poles, Alex Blatt, Elena Kirzhner, Jacob George, and Gera Gandelman. 2023. "Comparison between Cardiac Output and Pulmonary Vascular Pressure Measured by Indirect Fick and Thermodilution Methods" Journal of Personalized Medicine 13, no. 3: 559. https://doi.org/10.3390/jpm13030559
APA StyleVolodarsky, I., Kerzhner, K., Haberman, D., Cuciuc, V., Poles, L., Blatt, A., Kirzhner, E., George, J., & Gandelman, G. (2023). Comparison between Cardiac Output and Pulmonary Vascular Pressure Measured by Indirect Fick and Thermodilution Methods. Journal of Personalized Medicine, 13(3), 559. https://doi.org/10.3390/jpm13030559