
Moderate Aerobic Exercise Reduces the Detrimental Effects of Hypoxia on Cardiac Autonomic Control in Healthy Volunteers

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Cardiac Autonomic Control
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sport. Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Ligibel, J.A.; Bohlke, K.; May, A.M.; Clinton, S.K.; Demark-Wahnefried, W.; Gilchrist, S.C.; Irwin, M.L.; Late, M.; Mansfield, S.; Marshall, T.F.; et al. Exercise, Diet, and Weight Management During Cancer Treatment: ASCO Guideline. J. Clin. Oncol. 2022, 40, 2491–2507. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Li, Y.; Yue, Y.; Yuan, C.; Kang, J.H.; Chavarro, J.E.; Bhupathiraju, S.N.; Roberts, A.L. Adherence to Healthy Lifestyle Prior to Infection and Risk of Post-COVID-19 Condition. JAMA Intern. Med. 2023, 183, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical Inactivity Is Associated with a Higher Risk for Severe COVID-19 Outcomes: A Study in 48 440 Adult Patients. Br. J. Sport. Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef]
- Joyner, M.J.; Green, D.J. Exercise Protects the Cardiovascular System: Effects beyond Traditional Risk Factors. J. Physiol. 2009, 587, 5551–5558. [Google Scholar] [CrossRef]
- White, D.W.; Raven, P.B. Autonomic Neural Control of Heart Rate during Dynamic Exercise: Revisited. J. Physiol. 2014, 592, 2491–2500. [Google Scholar] [CrossRef]
- Hansen, D.; Meeusen, R.; Mullens, A.; Dendale, P. Effect of Acute Endurance and Resistance Exercise on Endocrine Hormones Directly Related to Lipolysis and Skeletal Muscle Protein Synthesis in Adult Individuals with Obesity. Sport. Med. 2012, 42, 415–431. [Google Scholar] [CrossRef]
- Nieman, D.C.; Wentz, L.M. The Compelling Link between Physical Activity and the Body’s Defense System. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef]
- Biolo, G.; Girolamo, F.G.D.; McDonnell, A.; Fiotti, N.; Mearelli, F.; Situlin, R.; Gonelli, A.; Dapas, B.; Giordano, M.; Lainscak, M.; et al. Effects of Hypoxia and Bed Rest on Markers of Cardiometabolic Risk: Compensatory Changes in Circulating Trail and Glutathione Redox Capacity. Front. Physiol. 2018, 9, 1000. [Google Scholar] [CrossRef] [Green Version]
- Grassi, G.; Seravalle, G.; Colombo, M.; Bolla, G.; Cattaneo, B.M.; Cavagnini, F.; Mancia, G. Body Weight Reduction, Sympathetic Nerve Traffic, and Arterial Baroreflex in Obese Normotensive Humans. Circulation 1998, 97, 2037–2042. [Google Scholar] [CrossRef] [Green Version]
- Lucini, D.; De Giacomi, G.; Tosi, F.; Malacarne, M.; Respizzi, S.; Pagani, M. Altered Cardiovascular Autonomic Regulation in Overweight Children Engaged in Regular Physical Activity. Heart 2013, 99, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Yadav, R.L.; Yadav, P.K.; Yadav, L.K.; Agrawal, K.; Sah, S.K.; Islam, M.N. Association between Obesity and Heart Rate Variability Indices: An Intuition toward Cardiac Autonomic Alteration-a Risk of CVD. Diabetes Metab. Syndr. Obes. Targets Ther. 2017, 10, 57–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, S.M.; Eleftheriadou, A.; Alam, U.; Cuthbertson, D.J.; Wilding, J.P.H. Cardiac Autonomic Neuropathy in Obesity, the Metabolic Syndrome and Prediabetes: A Narrative Review. Diabetes Ther. 2019, 10, 1995–2021. [Google Scholar] [CrossRef] [Green Version]
- Santana, M.D.R.; Kliszczewicz, B.; Vanderlei, F.M.; Monteiro, L.R.L.; Martiniano, E.C.; De Moraes, Y.M.; Mangueira, L.B.; Alcantara, G.C.; Da Silva, J.R.A.; Benjamim, C.J.R.; et al. Autonomic Responses Induced by Aerobic Submaximal Exercise in Obese and Overweight Adolescents. Cardiol. Young 2019, 29, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Gil, S.; Peçanha, T.; Dantas, W.S.; Murai, I.H.; Merege-Filho, C.A.A.; de Sá-Pinto, A.L.; Pereira, R.M.R.; de Cleva, R.; Santo, M.A.; Rezende, D.A.N.; et al. Exercise Enhances the Effect of Bariatric Surgery in Markers of Cardiac Autonomic Function. Obes. Surg. 2021, 31, 1381–1386. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. Defining and Setting National Goals for Cardiovascular Health Promotion and Disease Reduction: The American Heart Association’s Strategic Impact Goal through 2020 and Beyond. Circulation 2010, 121, 586–613. [Google Scholar] [CrossRef] [Green Version]
- Spring, B.; Ockene, J.K.; Gidding, S.S.; Mozaffarian, D.; Moore, S.; Rosal, M.C.; Brown, M.D.; Vafiadis, D.K.; Cohen, D.L.; Burke, L.E.; et al. Better Population Health through Behavior Change in Adults: A Call to Action. Circulation 2013, 128, 2169–2176. [Google Scholar] [CrossRef]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on Sports Cardiology and Exercise in Patients with Cardiovascular Disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise Standards for Testing and Training: A Scientific Statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef]
- Lucini, D.; Pagani, M. Exercise Prescription to Foster Health and Well-Being: A Behavioral Approach to Transform Barriers into Opportunities. Int. J. Environ. Res. Public Health 2021, 18, 968. [Google Scholar] [CrossRef] [PubMed]
- Tietjens, J.R.; Claman, D.; Kezirian, E.J.; de Marco, T.; Mirzayan, A.; Sadroonri, B.; Goldberg, A.N.; Long, C.; Gerstenfeld, E.P.; Yeghiazarians, Y. Obstructive Sleep Apnea in Cardiovascular Disease: A Review of the Literature and Proposed Multidisciplinary Clinical Management Strategy. J. Am. Heart Assoc. 2019, 8, e010440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charvat, J.M.; Leonard, D.; Barlow, C.E.; DeFina, L.F.; Willis, B.L.; Lee, S.M.C.; Stenger, M.B.; Mercaldo, S.F.; Van Baalen, M. Long-Term Cardiovascular Risk in Astronauts: Comparing NASA Mission Astronauts With a Healthy Cohort From the Cooper Center Longitudinal Study. Mayo Clin. Proc. 2022, 97, 1237–1246. [Google Scholar] [CrossRef]
- Ferretti, G.; Iellamo, F.; Pizzinelli, P.; Kenfack, M.A.; Lador, F.; Lucini, D.; Porta, A.; Narkiewicz, K.; Pagani, M. Prolonged Head down Bed Rest-Induced Inactivity Impairs Tonic Autonomic Regulation While Sparing Oscillatory Cardiovascular Rhythms in Healthy Humans. J. Hypertens. 2009, 27, 551–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mhatre, S.D.; Iyer, J.; Puukila, S.; Paul, A.M.; Tahimic, C.G.T.; Rubinstein, L.; Lowe, M.; Alwood, J.S.; Sowa, M.B.; Bhattacharya, S.; et al. Neuro-Consequences of the Spaceflight Environment. Neurosci. Biobehav. Rev. 2022, 132, 908–935. [Google Scholar] [CrossRef]
- Malliani, A.; Pagani, M.; Lombardi, F.; Cerutti, S. Cardiovascular Neural Regulation Explored in the Frequency Domain. Circulation 1991, 84, 482–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siebenmann, C.; Rasmussen, P.; Sørensen, H.; Bonne, T.C.; Zaar, M.; Aachmann-Andersen, N.J.; Nordsborg, N.B.; Secher, N.H.; Lundby, C. Hypoxia Increases Exercise Heart Rate despite Combined Inhibition of β-Adrenergic and Muscarinic Receptors. Am. J. Physiol.–Hearth Circ. Physiol. 2015, 308, H1540–H1546. [Google Scholar] [CrossRef] [Green Version]
- Fisher, J.P.; Flück, D.; Hilty, M.P.; Lundby, C. Carotid Chemoreceptor Control of Muscle Sympathetic Nerve Activity in Hypobaric Hypoxia. Exp. Physiol. 2018, 103, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Kontos, H.A.; Mauck, H.P.; Richardson, D.W.; Patterson, J.L. Mechanism of Circulatory Responses To Systemic Hypoxia in the Anesthetized Dog. Am. J. Physiol. 1965, 209, 397–403. [Google Scholar] [CrossRef]
- Kato, H.; Menon, A.S.; Slutsky, A.S. Mechanisms Mediating the Heart Rate Response to Hypoxemia. Circulation 1988, 77, 407–414. [Google Scholar] [CrossRef] [Green Version]
- Siebenmann, C.; Ryrsø, C.K.; Oberholzer, L.; Fisher, J.P.; Hilsted, L.M.; Rasmussen, P.; Secher, N.H.; Lundby, C. Hypoxia-Induced Vagal Withdrawal Is Independent of the Hypoxic Ventilatory Response in Men. J. Appl. Physiol. 2019, 126, 124–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debevec, T.; McDonnell, A.C.; Macdonald, I.A.; Eiken, O.; Mekjavic, I.B. Whole Body and Regional Body Composition Changes Following 10-Day Hypoxic Confinement and Unloading-Inactivity. Appl. Physiol. Nutr. Metab. 2014, 39, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Badilini, F.; Pagani, M.; Porta, A. HeartScope: A Software Tool Addressing Autonomic Nervous System Regulation. Comput. Cardiol. 2005, 32, 259–262. [Google Scholar] [CrossRef]
- Lucini, D.; Solaro, N.; Pagani, M. Autonomic Differentiation Map: A Novel Statistical Tool for Interpretation of Heart Rate Variability. Front. Physiol. 2018, 9, 401. [Google Scholar] [CrossRef] [Green Version]
- Lucini, D.; Pagani, M.; Mela, G.S.; Malliani, A. Sympathetic Restraint of Baroreflex Control of Heart Period in Normotensive and Hypertensive Subjects. Clin. Sci. 1994, 86, 547–556. [Google Scholar] [CrossRef]
- Iellamo, F.; Di Rienzo, M.; Lucini, D.; Legramante, J.M.; Pizzinelli, P.; Castiglioni, P.; Pigozzi, F.; Pagani, M.; Parati, G. Muscle Metaboreflex Contribution to Cardiovascular Regulation during Dynamic Exercise in Microgravity: Insights from Mission STS-107 of the Space Shuttle Columbia. J. Physiol. 2006, 572, 829–838. [Google Scholar] [CrossRef] [Green Version]
- Korhonen, I.; Lucini, D.; Porta, A.; Milani, O.; Baselli, G.; Pagani, M. Assessment of Arterial and Cardiopulmonary Baroreflex Gains from Simultaneous Recordings of Spontaneous Cardiovascular and Respiratory Variability (Multiple Letters). J. Hypertens. 2001, 19, 351–352. [Google Scholar] [CrossRef]
- Conover, W.J. The Rank Transformation-an Easy and Intuitive Way to Connect Many Nonparametric Methods to Their Parametric Counterparts for Seamless Teaching Introductory Statistics Courses. Wiley Interdiscip. Rev. Comput. Stat. 2012, 4, 432–438. [Google Scholar] [CrossRef]
- Hoff, P.; Belavý, D.L.; Huscher, D.; Lang, A.; Hahne, M.; Kuhlmey, A.K.; Maschmeyer, P.; Armbrecht, G.; Fitzner, R.; Perschel, F.H.; et al. Effects of 60-Day Bed Rest with and without Exercise on Cellular and Humoral Immunological Parameters. Cell. Mol. Immunol. 2015, 12, 483–492. [Google Scholar] [CrossRef] [Green Version]
- Jacob, P.; Bonnefoy, J.; Ghislin, S.; Frippiat, J.P. Long-Duration Head-down Tilt Bed Rest Confirms the Relevance of the Neutrophil to Lymphocyte Ratio and Suggests Coupling It with the Platelet to Lymphocyte Ratio to Monitor the Immune Health of Astronauts. Front. Immunol. 2022, 13, 952928. [Google Scholar] [CrossRef]
- Belavý, D.L.; Seibel, M.J.; Roth, H.J.; Armbrecht, G.; Rittweger, J.; Felsenberg, D. The Effects of Bed-Rest and Countermeasure Exercise on the Endocrine System in Male Adults: Evidence for Immobilization-Induced Reduction in Sex Hormone-Binding Globulin Levels. J. Endocrinol. Investig. 2012, 35, 54–62. [Google Scholar] [CrossRef]
- Rudwill, F.; O’Gorman, D.; Lefai, E.; Chery, I.; Zahariev, A.; Normand, S.; Pagano, A.F.; Chopard, A.; Damiot, A.; Laurens, C.; et al. Metabolic Inflexibility Is an Early Marker of Bed-Rest-Induced Glucose Intolerance Even When Fat Mass Is Stable. J. Clin. Endocrinol. Metab. 2018, 103, 1910–1920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbic, F.; Heusser, K.; Minonzio, M.; Shiffer, D.; Cairo, B.; Tank, J.; Jordan, J.; Diedrich, A.; Gauger, P.; Zamuner, R.A.; et al. Effects of Prolonged Head-Down Bed Rest on Cardiac and Vascular Baroreceptor Modulation and Orthostatic Tolerance in Healthy Individuals. Front. Physiol. 2019, 10, 1061. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, K.I.; Zhang, R.; Perhonen, M.A.; Zuckerman, J.H.; Levine, B.D. Reduced Baroreflex Control of Heart Period after Bed Rest Is Normalized by Acute Plasma Volume Restoration. Am. J. Physiol. 2004, 287, R1256–R1262. [Google Scholar] [CrossRef] [Green Version]
- Iwasaki, K.I.; Shiozawa, T.; Kamiya, A.; Michikami, D.; Hirayanagi, K.; Yajima, K.; Iwase, S.; Mano, T. Hypergravity Exercise against Bed Rest Induced Changes in Cardiac Autonomic Control. Eur. J. Appl. Physiol. 2005, 94, 285–291. [Google Scholar] [CrossRef]
- Konda, N.N.; Karri, R.S.; Winnard, A.; Nasser, M.; Evetts, S.; Boudreau, E.; Caplan, N.; Gradwell, D.; Velho, R.M. A Comparison of Exercise Interventions from Bed Rest Studies for the Prevention of Musculoskeletal Loss. NPJ Microgravity 2019, 5, 12. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.W.; Jung, W.S.; Kim, J.W.; Nam, S.S.; Park, H.Y. Aerobic Continuous and Interval Training under Hypoxia Enhances Endurance Exercise Performance with Hemodynamic and Autonomic Nervous System Function in Amateur Male Swimmers. Int. J. Environ. Res. Public Health 2021, 18, 3944. [Google Scholar] [CrossRef]
- Fornasiero, A.; Skafidas, S.; Stella, F.; Zignoli, A.; Savoldelli, A.; Rakobowchuk, M.; Pellegrini, B.; Schena, F.; Mourot, L. Cardiac Autonomic and Physiological Responses to Moderate- intensity Exercise in Hypoxia. Int. J. Sport. Med. 2019, 40, 886–896. [Google Scholar] [CrossRef]
- Lee-Iannotti, J.K.; Parish, J.M. Exercise as a Treatment for Sleep Apnea. J. Clin. Sleep Med. 2020, 16, 1005–1006. [Google Scholar] [CrossRef]
- Desplan, M.; Mercier, J.; Sabaté, M.; Ninot, G.; Prefaut, C.; Dauvilliers, Y. A Comprehensive Rehabilitation Program Improves Disease Severity in Patients with Obstructive Sleep Apnea Syndrome: A Pilot Randomized Controlled Study. Sleep Med. 2014, 15, 906–912. [Google Scholar] [CrossRef]
- Kline, C.E.; Ewing, G.B.; Burch, J.B.; Blair, S.N.; Durstine, J.L.; Davis, J.M.; Youngstedt, S.D. Exercise Training Improves Selected Aspects of Daytime Functioning in Adults with Obstructive Sleep Apnea. J. Clin. Sleep Med. 2012, 8, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Kline, C.E.; Crowley, E.P.; Ewing, G.B.; Burch, J.B.; Blair, S.N.; Durstine, J.L.; Davis, J.M.; Youngstedt, S.D. The Effect of Exercise Training on Obstructive Sleep Apnea and Sleep Quality: A Randomized Controlled Trial. Sleep 2011, 34, 1631–1640. [Google Scholar] [CrossRef] [PubMed]
- Sengul, Y.S.; Ozalevli, S.; Oztura, I.; Itil, O.; Baklan, B. The Effect of Exercise on Obstructive Sleep Apnea: A Randomized and Controlled Trial. Sleep Breath. 2011, 15, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Bollens, B.; Reychler, G. Efficacy of Exercise as a Treatment for Obstructive Sleep Apnea Syndrome: A Systematic Review. Complement. Ther. Med. 2018, 41, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.P.; Veale, D.; Pépin, J.L.; Lévy, P.A. Obstructive Sleep Apnoea and the Autonomic Nervous System. Sleep Med. Rev. 1998, 2, 69–92. [Google Scholar] [CrossRef]
- Dissanayake, H.U.; Bin, Y.S.; Ucak, S.; de Chazal, P.; Sutherland, K.; Cistulli, P.A. Association between Autonomic Function and Obstructive Sleep Apnea: A Systematic Review. Sleep Med. Rev. 2021, 57, 101470. [Google Scholar] [CrossRef]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic Dysfunction in ‘Long COVID’: Rationale, Physiology and Management Strategies. Clin. Med. J. R. Coll. Physicians Lond. 2021, 21, E63–E67. [Google Scholar] [CrossRef]
- Bärtsch, P.; Gibbs, J.S.R. Effect of Altitude on the Heart and the Lungs. Circulation 2007, 116, 2191–2202. [Google Scholar] [CrossRef] [Green Version]
- Parati, G.; Agostoni, P.; Basnyat, B.; Bilo, G.; Brugger, H.; Coca, A.; Festi, L.; Giardini, G.; Lironcurti, A.; Luks, A.M.; et al. Clinical Recommendations for High Altitude Exposure of Individuals with Pre-Existing Cardiovascular Conditions: A Joint Statement by the European Society of Cardiology, the Council on Hypertension of the European Society of Cardiology, the European Societ. Eur. Heart J. 2018, 39, 1546–1554. [Google Scholar] [CrossRef]
- American College of Cardiology. Exercise and Elevation. Available online: https://www.acc.org/latest-in-cardiology/articles/2021/03/15/13/39/exercise-and-elevation (accessed on 16 February 2023).
- Hainsworth, R.; Drinkhill, M.J.; Rivera-Chira, M. The Autonomic Nervous System at High Altitude. Clin. Auton. Res. 2007, 17, 13–19. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | Units | Definition |
|---|---|---|
| HR | beat/min | Heart rate |
| RR Mean | msec | Average of RR interval from tachogram |
| RR V | msec2 | RR variance (total power) from tachogram (proxy of vagal drive) |
| RR LFa | msec2 | Absolute power (a) of low-frequency (LF) component of RR variability (V) |
| RR HFa | msec2 | Absolute power (a) of high-frequency (HF) component of RRV |
| RR LFnu | nu | Normalized power (nu) of low-frequency (LF) component of RRV |
| RR HFnu | nu | Normalized power (nu) of high-frequency (HF) component of RRV |
| RR LF/HF | - | Ratio between absolute values of LF and HF |
| RR LFHz | Hz | Center frequency of RR LF |
| RR HFHz | Hz | Center frequency of RR HF, providing a measure of respiratory rate |
| Resp | Hz | Center frequency of respiration (piezoelectric sensor) spectra |
| SAP Mean | mmHg | Average of systogram (i.e., systolic arterial pressure variability by Finometer) |
| SAP V | mmHg2 | Systolic arterial pressure variance from systogram |
| SAP LFa | mmHg2 | Absolute power of LF component of systogram (proxy of vascular sympathetic drive) |
| SAP HFa | mmHg2 | Absolute power of HF component of systogram |
| Alpha Index M | msec/mmHg | Frequency-domain (proxy) measure of cardiac baroreflex gain (proxy of vagal drive) |
| BRS | msec/mmHg | Time-domain measure of cardiac baroreflex slope (proxy of vagal drive) |
| A.XAR | msec/mmHg | Bivariate causal index of RR–SAP relationship |
| A.XXAR | msec/mmHg | Causal index from trivariate model of RR–SAP (avoiding respiration bias) relationship (proxy of arterial baroreflex) |
| Alpha Index CP | msec/mmHg | Trivariate model derived proxy of cardiopulmonary baroreflex |
| Variables | Ambulatory | Bedrest | Cond | Contrast | ||
|---|---|---|---|---|---|---|
| Normoxia | Hypoxia | Normoxia | Hypoxia | |||
| HR (b/min) | 61.52 ± 6.49 | 62.44 ± 5.92 | 61.62 ± 4.91 | 67.76 ± 7.95 | 0.111 | |
| RR (ms) | 985.24 ± 103.04 | 968.57 ± 89.17 | 979.15 ± 76.26 | 896.25 ± 100.67 | 0.111 | |
| RR V (ms2) | 4248.66 ± 4295.91 | 3406.52 ± 1701.65 | 3203.75 ± 1687.2 | 2468.54 ± 1416.04 | 0.192 | |
| RR LFa (ms2) | 1074.59 ± 987.12 | 1066.7 ± 544.24 | 957.6 ± 788.91 | 622 ± 625.06 | 0.100 | |
| RR HFa (ms2) | 1249.4 ± 1711.39 | 1025.39 ± 1122.01 | 888.24 ± 842.7 | 388.16 ± 313.8 | 0.063 | |
| RR LFnu (nu) | 47.96 ± 13.52 | 55.58 ± 14.59 | 53.48 ± 25.7 | 54.32 ± 17.59 | 0.168 | |
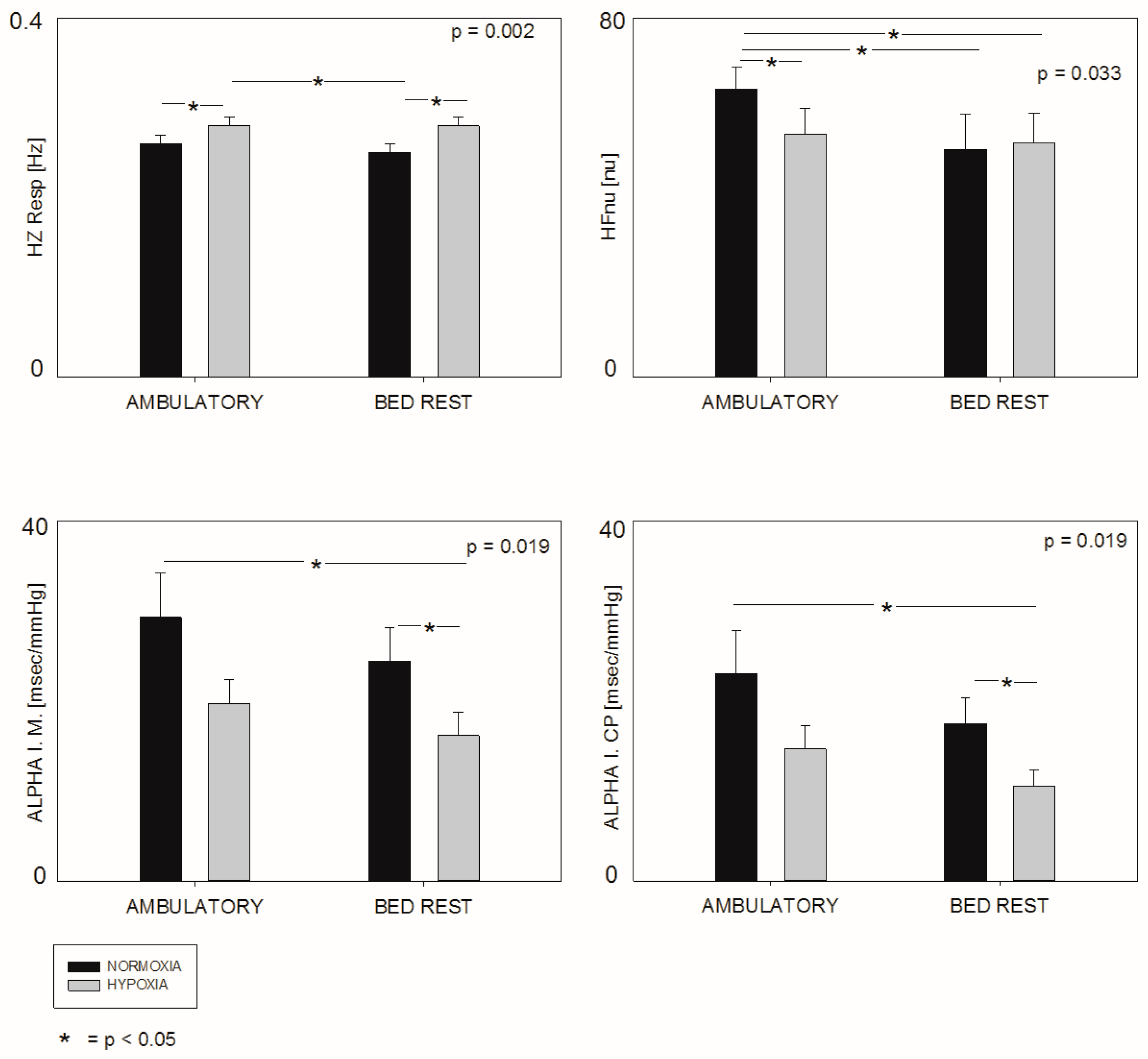
| RR HFnu (nu) | 48.14 ± 12.44 | 40.59 ± 14.63 | 38.04 ± 19.55 | 39.1 ± 16.62 | 0.033 | a b c |
| LF/HF nu (au) | 1.12 ± 0.55 | 1.61 ± 0.74 | 2.24 ± 2.08 | 1.68 ± 0.82 | 0.065 | |
| RR LFHz (Hz) | 0.1 ± 0.03 | 0.09 ± 0.03 | 0.1 ± 0.02 | 0.1 ± 0.03 | 0.957 | |
| RR HFHz (Hz) | 0.26 ± 0.05 | 0.28 ± 0.05 | 0.25 ± 0.06 | 0.27 ± 0.04 | 0.009 | a d |
| RESP (Hz) | 0.26 ± 0.05 | 0.28 ± 0.06 | 0.25 ± 0.06 | 0.28 ± 0.05 | 0.002 | a d f |
| SAP (mmHg) | 117.55 ± 12.35 | 117.24 ± 9.12 | 113.31 ± 17.21 | 121.21 ± 15.2 | 0.471 | |
| SAP V (mmHg2) | 24.48 ± 21.35 | 26.33 ± 17.93 | 23.90 ± 22.77 | 19.83 ± 16.04 | 0.447 | |
| SAP LFa (mmHg2) | 5.50 ± 4.02 | 13.44 ± 12.63 | 6.41 ± 10.45 | 6.93 ± 7.68 | 0.042 | d e |
| SAP HFa (mmHg2) | 1.22 ± 1.45 | 1.56 ± 1.93 | 1.36 ± 1.97 | 1.16 ± 1.01 | 0.053 | |
| Alpha Index M (ms/mmHg) | 29.30 ± 16.62 | 19.73 ± 9.06 | 24.38 ± 12.85 | 16.15 ± 8.63 | 0.019 | c f |
| BRS (ms/mmHg) | 28.08 ± 15.83 | 20.26 ± 4.28 | 25.99 ± 13.09 | 17.67 ± 8.48 | 0.089 | |
| A.XAR (ms/mmHg) | 7.56 ± 6.44 | 6.76 ± 3.70 | 8.27 ± 7.53 | 8.02 ± 6.42 | 0.662 | |
| A.XXAR (ms/mmHg) | 7.19 ± 6.48 | 5.05 ± 2.67 | 6.87 ± 7.02 | 5.58 ± 4.16 | 0.765 | |
| Alpha Index CP (ms/mmHg) | 23.00 ± 16.02 | 14.68 ± 8.84 | 17.51 ± 9.24 | 10.57 ± 6.05 | 0.049 | c f |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giovanelli, L.; Malacarne, M.; Pagani, M.; Biolo, G.; Mekjavic, I.B.; Bernardelli, G.; Lucini, D. Moderate Aerobic Exercise Reduces the Detrimental Effects of Hypoxia on Cardiac Autonomic Control in Healthy Volunteers. J. Pers. Med. 2023, 13, 585. https://doi.org/10.3390/jpm13040585
Giovanelli L, Malacarne M, Pagani M, Biolo G, Mekjavic IB, Bernardelli G, Lucini D. Moderate Aerobic Exercise Reduces the Detrimental Effects of Hypoxia on Cardiac Autonomic Control in Healthy Volunteers. Journal of Personalized Medicine. 2023; 13(4):585. https://doi.org/10.3390/jpm13040585
Chicago/Turabian StyleGiovanelli, Luca, Mara Malacarne, Massimo Pagani, Gianni Biolo, Igor B. Mekjavic, Giuseppina Bernardelli, and Daniela Lucini. 2023. "Moderate Aerobic Exercise Reduces the Detrimental Effects of Hypoxia on Cardiac Autonomic Control in Healthy Volunteers" Journal of Personalized Medicine 13, no. 4: 585. https://doi.org/10.3390/jpm13040585
APA StyleGiovanelli, L., Malacarne, M., Pagani, M., Biolo, G., Mekjavic, I. B., Bernardelli, G., & Lucini, D. (2023). Moderate Aerobic Exercise Reduces the Detrimental Effects of Hypoxia on Cardiac Autonomic Control in Healthy Volunteers. Journal of Personalized Medicine, 13(4), 585. https://doi.org/10.3390/jpm13040585