


Asthma-COPD Overlap in Clinical Practice (ACO_CP 2023): Toward Precision Medicine

Abstract
:1. Introduction
2. Epidemiology
3. Pathogenesis
4. Respiratory Microbiome and ACO during Stable and Exacerbation States
5. Clinical Presentation and Diagnosis
6. Proposed Treatment Guide for ACO
6.1. Non-Pharmacologic Treatment
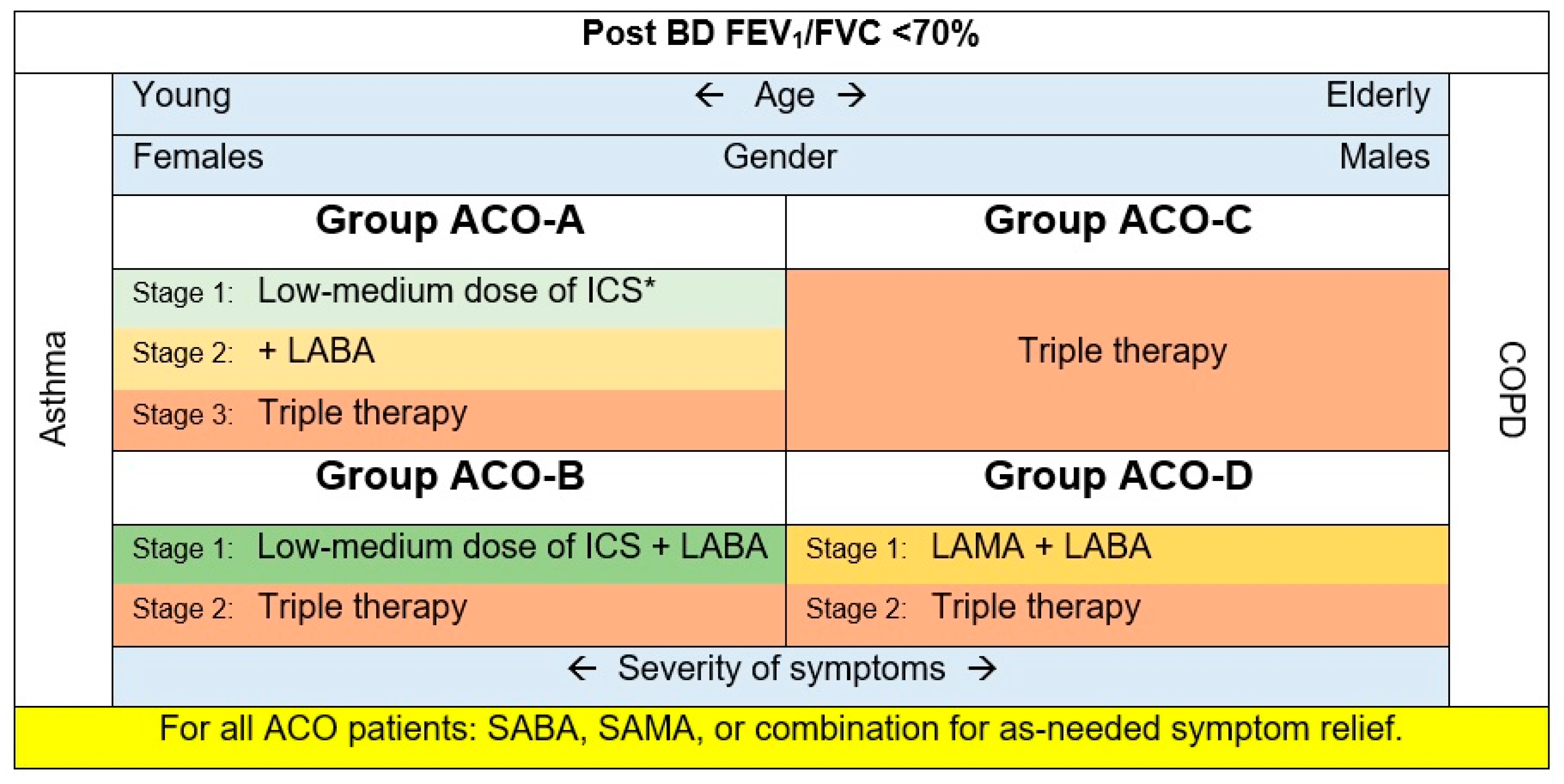
6.2. Pharmacologic Treatment
- Group ACO-A: Asthmatics, non-smokers, most probably females. These patients may exhibit eosinophilic inflammation signs.
- Group ACO-C: COPD accompanied by eosinophilia. Patients in this group tend to be older men with a higher eosinophil count than smokers (>300 cells/µL) and T helper cell type 2–related indicators [49].
- Group ACO-D: COPD with a substantial BD response (FEV1 ≥ 15% and ≥400 mL), as defined by previous publications [14,48,49]. These patients have numerous characteristics of COPD with eosinophilia phenotype, as they are usually older males with comparable baseline lung function [49,54]. Their blood eosinophil level is typically <300 cells/µL.
7. Biologic Agents
7.1. Anti-IgE Therapy
7.2. Anti-IL-5/IL-5 Receptor Alpha (IL-5Ra) Therapies
7.3. IL-4 Receptor Alpha (IL-4Ra) and IL-13 Therapies
8. Future Directions
9. Conclusions and Clinical Care Points
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woodruff, P.G.; van den Berge, M.; Boucher, R.C.; Brightling, C.; Burchard, E.G.; Christenson, S.A.; Han, M.K.; Holtzman, M.J.; Kraft, M.; Lynch, D.A.; et al. American Thoracic Society/National Heart, Lung, and Blood Institute Asthma-Chronic Obstructive Pulmonary Disease Overlap Workshop Report. Am. J. Respir. Crit. Care Med. 2017, 196, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Reddel, H.K.; Bacharier, L.B.; Bateman, E.D.; Brightling, C.E.; Brusselle, G.G.; Buhl, R.; Cruz, A.A.; Duijts, L.; Drazen, J.M.; FitzGerald, J.M.; et al. Global Initiative for Asthma Strategy 2021: Executive summary and rationale for key changes. Eur. Respirat. J. 2022, 59, 17–35. [Google Scholar] [CrossRef] [PubMed]
- GOLD. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2022. Available online: https://goldcopd.org/wp-content/uploads/2021/12/GOLD-REPORT-2022-v1.1-22Nov2021_WMV.pdf (accessed on 1 January 2022).
- GINA. Global Initiative for Asthma (GINA): Strategy for Asthma Management and Prevention. Available online: https://ginasthma.org/reports/ (accessed on 1 October 2022).
- Rhee, C.K. Phenotype of asthma-chronic obstructive pulmonary disease overlap syndrome. Korean J. Int. Med. 2015, 30, 443–449. [Google Scholar] [CrossRef]
- Fujino, N.; Sugiura, H. Aco (Asthma–copd overlap) is independent from copd, a case in favor: A systematic review. Diagnostics 2021, 11, 859. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.M.; Sin, D.D. Asthma-COPD overlap syndrome: Pathogenesis, clinical features, and therapeutic targets. BMJ 2017, 358, j3772. [Google Scholar] [CrossRef]
- Barrecheguren, M.; Esquinas, C.; Miravitlles, M. The asthma–chronic obstructive pulmo-nary disease overlap syndrome (ACOS): Opportunities and challenges. Curr. Opin. Pulm. Med. 2015, 21, 74–79. [Google Scholar] [CrossRef]
- Cosio, B.G.; Soriano, J.B.; López-Campos, J.L.; Calle-Rubio, M.; Soler-Cataluna, J.J.; de-Torres, J.P.; Marín, J.M.; Martínez-Gonzalez, C.; de Lucas, P.; Mir, I.; et al. Defining the Asthma-COPD Overlap Syndrome in a COPD Cohort. Chest 2016, 149, 45–52. [Google Scholar] [CrossRef]
- Sin, D.D.; Miravitlles, M.; Mannino, D.M.; Soriano, J.B.; Price, D.; Celli, B.R.; Leung, J.M.; Nakano, Y.; Park, H.Y.; Wark, P.A.; et al. What is asthma-COPD overlap syndrome? Towards a consensus definition from a round table discussion. Eur. Respir. J. 2016, 48, 664–673. [Google Scholar] [CrossRef]
- Cataldo, D.; Corhay, J.L.; Derom, E.; Louis, R.; Marchand, E.; Michils, A.; Ninane, V.; Peché, R.; Pilette, C.; Vincken, W.; et al. A Belgian survey on the diagnosis of asthma-COPD overlap syndrome. Int. J. Chron. Obstruct. Pulmon Dis. 2017, 12, 601–613. [Google Scholar] [CrossRef]
- Koblizek, V.; Chlumsky, J.; Zindr, V.; Neumannova, K.; Zatloukal, J.; Zak, J.; Sedlak, V.; Kocianova, J.; Zatloukal, J.; Hejduk, K.; et al. Chronic Obstructive Pulmonary Disease: Official diagnosis and treatment guidelines of the Czech Pneumological and Phthisiological Society; a novel phenotypic approach to COPD with patient-oriented care. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2013, 157, 189–201. [Google Scholar] [CrossRef]
- Soler-Cataluña, J.J.; Cosío, B.; Izquierdo, J.L.; López-Campos, J.L.; Marín, J.M.; Agüero, R.; Baloira, A.; Carrizo, S.; Esteban, C.; Galdiz, J.B.; et al. Consensus document on the overlap phenotype COPD-asthma in COPD. Arch. Bronconeumol. 2012, 48, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Miravitlles, M.; Alvarez-Gutierrez, F.J.; Calle, M.; Casanova, C.; Cosio, B.G.; López-Viña, A.; Pérez de Llano, L.; Quirce, S.; Roman-Rodríguez, M.; Soler-Cataluña, J.J.; et al. Algorithm for identification of asthma-COPD overlap: Consensus between the Spanish COPD and asthma guidelines. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef] [PubMed]
- Alshabanat, A.; Zafari, Z.; Albanyan, O.; Dairi, M.; FitzGerald, J.M. Asthma and COPD Overlap Syndrome (ACOS): A Systematic Review and Meta Analysis. PLoS ONE 2015, 10, e0136065. [Google Scholar] [CrossRef] [PubMed]
- van Boven, J.F.; Román-Rodríguez, M.; Palmer, J.F.; Toledo-Pons, N.; Cosío, B.G.; Soriano, J.B. Comorbidome, Pattern, and Impact of Asthma-COPD Overlap Syndrome in Real Life. Chest 2016, 149, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, J.; Zhao, H.; Hardin, M.; Hersh, C.P.; Crapo, J.; Kim, V.; Criner, G.J. Analysis of Asthma-Chronic Obstructive Pulmonary Disease Overlap Syndrome Defined on the Basis of Bronchodilator Response and Degree of Emphysema. Ann. Am. Thorac. Soc. 2016, 13, 1483–1489. [Google Scholar] [CrossRef]
- Kumbhare, S.; Pleasants, R.; Ohar, J.A.; Strange, C. Characteristics and Prevalence of Asthma/Chronic Obstructive Pulmonary Disease Overlap in the United States. Ann. Am. Thorac. Soc. 2016, 13, 803–810. [Google Scholar] [CrossRef]
- Dodd, K.E.; Wood, J.; Mazurek, J.M. Mortality Among Persons with Both Asthma and Chronic Obstructive Pulmonary Disease Aged ≥25 Years, by Industry and Occupation—United States, 1999–2016. MMWR Morb. Mort. Wkly Rep. 2020, 69, 670–679. [Google Scholar] [CrossRef]
- Çolak, Y.; Nordestgaard, B.G.; Lange, P.; Vestbo, J.; Afzal, S. Prognosis of Patients with Chronic Obstructive Pulmonary Disease Not Eligible for Major Clinical Trials. Am. J. Respir. Crit. Care Med. 2022, 206, 271–280. [Google Scholar] [CrossRef]
- Vaz Fragoso, C.A.; Murphy, T.E.; Agogo, G.O.; Allore, H.G.; McAvay, G.J. Asthma-COPD overlap syndrome in the US: A prospective population-based analysis of patient-reported outcomes and health care utilization. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 517–527. [Google Scholar] [CrossRef]
- Charokopos, A.; Braman, S.S.; Brown, S.A.W.; Mhango, G.; de-Torres, J.P.; Zulueta, J.J.; Sharma, S.; Holguin, F.; Sigel, K.M.; Powell, C.A.; et al. Lung Cancer Risk among Patients with Asthma-Chronic Obstructive Pulmonary Disease Overlap. Ann. Am. Thorac. Soc. 2021, 18, 1894–1900. [Google Scholar] [CrossRef]
- Orie, N.G. Correlations of emphysema and asthmatic constitution. Acta Allergol. 1961, 16, 407–409. [Google Scholar] [CrossRef] [PubMed]
- Orie, N. The host factor in bronchitis. In Proceedings of the Bronchitis an International Symposium, Groningen, The Netherlands, 9–11 June 1961. [Google Scholar]
- Barnes, P.J. Against the Dutch hypothesis: Asthma and chronic obstructive pulmonary disease are distinct diseases. Am. J. Respir. Crit. Care Med. 2006, 174, 240–243, discussion 243–244. [Google Scholar] [CrossRef] [PubMed]
- Siew, L.Q.C.; Wu, S.Y.; Ying, S.; Corrigan, C.J. Cigarette smoking increases bronchial mucosal IL-17A expression in asthmatics, which acts in concert with environmental aeroallergens to engender neutrophilic inflammation. Clin. Exp. Allerg. 2017, 47, 740–750. [Google Scholar] [CrossRef] [PubMed]
- Itabashi, S.; Fukushima, T.; Aikawa, T.; Yanai, M.; Sekizawa, K.; Sasaki, H.; Takishima, T. Allergic sensitization in elderly patients with chronic obstructive pulmonary disease. Respiration 1990, 57, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Ray, A.; Camiolo, M.; Fitzpatrick, A.; Gauthier, M.; Wenzel, S.E. Are we meeting the promise of endotypes and precision medicine in asthma? Physiol. Rev. 2020, 100, 983–1017. [Google Scholar] [CrossRef] [PubMed]
- Agache, I.; Akdis, C.A. Precision medicine and phenotypes, endotypes, genotypes, regiotypes, and theratypes of allergic diseases. J. Clin. Investig. 2019, 129, 1493–1503. [Google Scholar] [CrossRef]
- Alsayed, A.R.; Talib, W.; Al-Dulaimi, A.; Daoud, S.; Al Maqbali, M. The first detection of Pneumocystis jirovecii in asthmatic patients post-COVID-19 in Jordan. Bosn. J. Basic Med. Sci. 2022, 22, 784–790. [Google Scholar] [CrossRef]
- Alsayed, A.R.; Al-Dulaimi, A.; Alkhatib, M.; Al Maqbali, M.; Al-Najjar, M.A.A.; Al-Rshaidat, M.M.D. A comprehensive clinical guide for Pneumocystis jirovecii pneumonia: A missing therapeutic target in HIV-uninfected patients. Expert Rev. Respir. Med. 2022, 16, 1167–1190. [Google Scholar] [CrossRef]
- Alsayed, A.R.; Abed, A.; Khader, H.A.; Al-Shdifat, L.M.H.; Hasoun, L.; Al-Rshaidat, M.M.D.; Alkhatib, M.; Zihlif, M. Molecular Accounting and Profiling of Human Respiratory Microbial Communities: Toward Precision Medicine by Targeting the Respiratory Microbiome for Disease Diagnosis and Treatment. Int. J. Mol. Sci. 2023, 24, 4086. [Google Scholar] [CrossRef]
- Al-Dulaimi, A.; Alsayed, A.R.; Maqbali, M.A.; Zihlif, M. Investigating the human rhinovirus co-infection in patients with asthma exacerbations and COVID-19. Pharm. Pract. (Granada) 2022, 20, 2665. [Google Scholar] [CrossRef]
- Alsayed, A.R.; Abed, A.; Jarrar, Y.B.; Alshammari, F.; Alshammari, B.; Basheti, I.A.; Zihlif, M. Alteration of the Respiratory Microbiome in Hospitalized Patients with Asthma–COPD Overlap during and after an Exacerbation. J. Clin. Med. 2023, 12, 2118. [Google Scholar] [CrossRef]
- Sethi, S.; Evans, N.; Grant, B.J.B.; Murphy, T.F. New strains of bacteria and exacerbations of chronic obstructive pulmonary disease. N. Engl. J. Med. 2002, 347, 465–471. [Google Scholar] [CrossRef]
- Murphy, T.F.; Brauer, A.L.; Eschberger, K.; Lobbins, P.; Grove, L.; Cai, X.; Sethi, S. Pseudomonas aeruginosa in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2008, 177, 853–860. [Google Scholar] [CrossRef]
- Sze, M.A.; Dimitriu, P.A.; Hayashi, S.; Elliott, W.M.; McDonough, J.E.; Gosselink, J.V.; Cooper, J.; Sin, D.D.; Mohn, W.W.; Hogg, J.C. The lung tissue microbiome in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2012, 185, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Erb-Downward, J.R.; Thompson, D.L.; Han, M.K.; Freeman, C.M.; McCloskey, L.; Schmidt, L.A.; Young, V.B.; Toews, G.B.; Curtis, J.L.; Sundaram, B. Analysis of the lung microbiome in the “healthy” smoker and in COPD. PLoS ONE 2011, 6, e16384. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, A.; Al-Doori, A.; Al-Dulaimi, A.; Alnaseri, A.; Abuhashish, J.; Aliasin, K.; Alfayoumi, I. Influences of bovine colostrum on nasal swab microbiome and viral upper respiratory tract infections—A case report. Respir. Med. Case Rep. 2020, 31, 101189. [Google Scholar] [CrossRef]
- Adrish, M.; Anand, M.P.; Hanania, N.A. Phenotypes of Asthma-Chronic Obstructive Pulmonary Disease Overlap. Immunol. Allerg. Clin. N. Am. 2022, 42, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.S.; Weiss, S.T.; Bleecker, E.R.; Yancey, S.W.; Dorinsky, P.M. The Salmeterol Multicenter Asthma Research Trial: A comparison of usual pharmacotherapy for asthma or usual pharmacotherapy plus salmeterol. Chest 2006, 129, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Ishiura, Y.; Fujimura, M.; Shiba, Y.; Ohkura, N.; Hara, J.; Kasahara, K. A comparison of the efficacy of once-daily fluticasone furoate/vilanterole with twice-daily fluticasone propionate/salmeterol in asthma-COPD overlap syndrome. Pulm. Pharmacol. Ther. 2015, 35, 28–33. [Google Scholar] [CrossRef] [PubMed]
- GINA. Global Strategy for Asthma Management and Prevention. 2022. Available online: https://ginasthma.org (accessed on 1 July 2022).
- Ishiura, Y.; Fujimura, M.; Ohkura, N.; Hara, J.; Kasahara, K.; Ishii, N.; Tamaki, T.; Shimizu, T.; Nomura, S. Effect of triple therapy in patients with asthma-COPD overlap. Int. J. Clin. Pharmacol. Ther. 2019, 57, 384–392. [Google Scholar] [CrossRef]
- Joo, H.; Han, D.; Lee, J.H.; Rhee, C.K. Heterogeneity of asthma–COPD overlap syndrome. Int. J. Chron. Obstruct. Pulm. Dis. 2017, 12, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Pérez-de-Llano, L.; Cosio, B.G. Asthma-COPD overlap is not a homogeneous disorder: Further supporting data. Respir. Res. 2017, 18, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Boulet, L.-P.; Boulay, M.-È.; Dérival, J.-L.; Milot, J.; Lepage, J.; Bilodeau, L.; Maltais, F. Asthma-COPD overlap phenotypes and smoking: Comparative features of asthma in smoking or non-smoking patients with an incomplete reversibility of airway obstruction. COPD J. Chron. Obstruct. Pulm. Dis. 2018, 15, 130–138. [Google Scholar] [CrossRef]
- Plaza, V.; Álvarez, F.; Calle, M.; Casanova, C.; Cosío, B.G.; López-Viña, A.; de Llano, L.P.; Quirce, S.; Román-Rodríguez, M.; Soler-Cataluña, J.J. Consensus on the asthma–COPD overlap (ACO) between the Spanish COPD guidelines (GesEPOC) and the Spanish guidelines on the management of asthma (GEMA). Arch. Bronconeumol. 2017, 53, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Toledo-Pons, N.; Van Boven, J.F.M.; Román-Rodríguez, M.; Pérez, N.; Felices, J.L.V.; Soriano, J.B.; Cosío, B.G. ACO: Time to move from the description of different phenotypes to the treatable traits. PLoS ONE 2019, 14, 0210915. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, S.; Barnes, N.; Brusselle, G.; Compton, C.; Criner, G.J.; Dransfield, M.T.; Halpin, D.M.G.; Han, M.K.; Hartley, B.; Lange, P.; et al. Blood eosinophils and treatment response with triple and dual combination therapy in chronic obstructive pulmonary disease: Analysis of the IMPACT trial. Lancet Respir. Med. 2019, 7, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Bafadhel, M.; Peterson, S.; De Blas, M.A.; Calverley, P.M.; Rennard, S.I.; Richter, K.; Fagerås, M. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: A post-hoc analysis of three randomised trials. Lancet Respir. Med. 2018, 6, 117–126. [Google Scholar] [CrossRef]
- GOLD. The Global Initiative for Chronic Obstructive Lung Disease (GOLD). Available online: https://goldcopd.org/2023-gold-report-2/ (accessed on 1 January 2023).
- Venkatesan, P. GOLD COPD report: 2023 update. Lancet Respir. Med. 2023, 11, 18. [Google Scholar] [CrossRef]
- Oh, J.Y.; Lee, Y.S.; Min, K.H.; Hur, G.Y.; Lee, S.Y.; Kang, K.H.; Rhee, C.K.; Park, S.J.; Khan, A.; Na, J.; et al. Increased urinary l-histidine in patients with asthma-COPD overlap: A pilot study. Int. J. COPD 2018, 13, 1809–1818. [Google Scholar] [CrossRef]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; Schatz, M.; Li, J.T.; Marcus, P.; Murray, J.J.; Pendergraft, T.B. Development of the Asthma Control Test: A survey for assessing asthma control. J. Allergy Clin. Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef]
- Hanania, N.A.; Chipps, B.E.; Griffin, N.M.; Yoo, B.; Iqbal, A.; Casale, T.B. Omalizumab effectiveness in asthma-COPD overlap: Post hoc analysis of PROSPERO. J. Allerg. Clin. Immunol. 2019, 143, 1629–1633.e1622. [Google Scholar] [CrossRef]
- de Llano, L.P.; Rivas, D.D.; Malanda, N.M.; Moral, V.P.; Blanco, J.A.G.; Muñoz-Esquerre, M.; García-Moguel, I.; Campos, R.M.D.; Martínez-Moragón, E.; Mena, A.H.; et al. The Response to Biologics is Better in Patients with Severe Asthma Than in Patients with Asthma–COPD Overlap Syndrome. J. Asthma Allerg. 2022, 15, 363–369. [Google Scholar] [CrossRef]
- Donovan, T.; Crossingham, I.; Milan, S.J.; Wang, R.; Bradley, P. Anti-IL5 therapies for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2019, 2019, 14651858. [Google Scholar] [CrossRef]
- Castro, M.; Corren, J.; Pavord, I.D.; Maspero, J.; Wenzel, S.; Rabe, K.F.; Busse, W.W.; Ford, L.; Sher, L.; FitzGerald, J.M.; et al. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. N. Engl. J. Med. 2018, 378, 2486–2496. [Google Scholar] [CrossRef] [PubMed]
- Busse, W.; Corren, J.; Lanier, B.Q.; McAlary, M.; Fowler-Taylor, A.; Cioppa, G.D.; van As, A.; Gupta, N. Omalizumab, anti-IgE recombinant humanized monoclonal antibody, for the treatment of severe allergic asthma. J. Allerg. Clin. Immunol. 2001, 108, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Lemanske, R.F., Jr.; Nayak, A.; McAlary, M.; Everhard, F.; Fowler-Taylor, A.; Gupta, N. Omalizumab improves asthma-related quality of life in children with allergic asthma. Pediatrics 2002, 110, e55. [Google Scholar] [CrossRef]
- Maltby, S.; Gibson, P.G.; Powell, H.; McDonald, V.M. Omalizumab Treatment Response in a Population with Severe Allergic Asthma and Overlapping COPD. Chest 2017, 151, 78–89. [Google Scholar] [CrossRef]
- Yalcin, A.D.; Celik, B.; Yalcin, A.N. Omalizumab (anti-IgE) therapy in the asthma-COPD overlap syndrome (ACOS) and its effects on circulating cytokine levels. Immunopharmacol. Immunotoxicol. 2016, 38, 253–256. [Google Scholar] [CrossRef]
- Tat, T.S.; Cilli, A. Omalizumab treatment in asthma-COPD overlap syndrome. J. Asthm. 2016, 53, 1048–1050. [Google Scholar] [CrossRef]
- Kupryś-Lipińska, I.; Pałczyński, C.; Molinska, J.; Kuna, P. Omalizumab therapy in a patient with severe asthma and co-existing chronic obstructive pulmonary disease. Postepy Dermatol. Alergol. 2019, 36, 239–241. [Google Scholar] [CrossRef]
- Castro, M.; Wenzel, S.E.; Bleecker, E.R.; Pizzichini, E.; Kuna, P.; Busse, W.W.; Gossage, D.L.; Ward, C.K.; Wu, Y.; Wang, B.; et al. Benralizumab, an anti-interleukin 5 receptor α monoclonal antibody, versus placebo for uncontrolled eosinophilic asthma: A phase 2b randomised dose-ranging study. Lancet Respir. Med. 2014, 2, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Bel, E.H.; Wenzel, S.E.; Thompson, P.J.; Prazma, C.M.; Keene, O.N.; Yancey, S.W.; Ortega, H.G.; Pavord, I.D. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N. Engl. J. Med. 2014, 371, 1189–1197. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.; Zangrilli, J.; Wechsler, M.E.; Bateman, E.D.; Brusselle, G.G.; Bardin, P.; Murphy, K.; Maspero, J.F.; O’Brien, C.; Korn, S. Reslizumab for inadequately controlled asthma with elevated blood eosinophil counts: Results from two multicentre, parallel, double-blind, randomised, placebo-controlled, phase 3 trials. Lancet Respir. Med. 2015, 3, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Rabe, K.F.; Nair, P.; Brusselle, G.; Maspero, J.F.; Castro, M.; Sher, L.; Zhu, H.; Hamilton, J.D.; Swanson, B.N.; Khan, A.; et al. Efficacy and Safety of Dupilumab in Glucocorticoid-Dependent Severe Asthma. N. Engl. J. Med. 2018, 378, 2475–2485. [Google Scholar] [CrossRef] [PubMed]
- Corren, J.; Ambrose, C.S.; Sałapa, K.; Roseti, S.L.; Griffiths, J.M.; Parnes, J.R.; Colice, G. Efficacy of Tezepelumab in Patients with Severe, Uncontrolled Asthma and Perennial Allergy. J. Allerg. Clin. Immunol. Pract. 2021, 9, 4334–4342.e4336. [Google Scholar] [CrossRef]
- Corren, J.; Chen, S.; Callan, L.; Gil, E.G. The effect of tezepelumab on hospitalizations and emergency department visits in patients with severe asthma. Ann. Allerg. Asthm. Immunol. 2020, 125, 211–214. [Google Scholar] [CrossRef]
- Brightling, C.E.; Bleecker, E.R.; Panettieri, R.A., Jr.; Bafadhel, M.; She, D.; Ward, C.K.; Xu, X.; Birrell, C.; van der Merwe, R. Benralizumab for chronic obstructive pulmonary disease and sputum eosinophilia: A randomised, double-blind, placebo-controlled, phase 2a study. Lancet Respir. Med. 2014, 2, 891–901. [Google Scholar] [CrossRef]
- Pavord, I.D.; Chanez, P.; Criner, G.J.; Kerstjens, H.A.M.; Korn, S.; Lugogo, N.; Martinot, J.B.; Sagara, H.; Albers, F.C.; Bradford, E.S.; et al. Mepolizumab for Eosinophilic Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2017, 377, 1613–1629. [Google Scholar] [CrossRef]
- Kau, A.L.; Korenblat, P.E. Anti-interleukin 4 and 13 for asthma treatment in the era of endotypes. Curr. Opin. Allerg. Clin. Immunol. 2014, 14, 570–575. [Google Scholar] [CrossRef]
- Hanania, N.A.; Korenblat, P.; Chapman, K.R.; Bateman, E.D.; Kopecky, P.; Paggiaro, P.; Yokoyama, A.; Olsson, J.; Gray, S.; Holweg, C.T.; et al. Efficacy and safety of lebrikizumab in patients with uncontrolled asthma (LAVOLTA I and LAVOLTA II): Replicate, phase 3, randomised, double-blind, placebo-controlled trials. Lancet Respir. Med. 2016, 4, 781–796. [Google Scholar] [CrossRef]
- Panettieri, R.A., Jr.; Sjöbring, U.; Péterffy, A.; Wessman, P.; Bowen, K.; Piper, E.; Colice, G.; Brightling, C.E. Tralokinumab for severe, uncontrolled asthma (STRATOS 1 and STRATOS 2): Two randomised, double-blind, placebo-controlled, phase 3 clinical trials. Lancet Respir. Med. 2018, 6, 511–525. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| More Likely Asthma If: | More Likely COPD If: |
|---|---|
| Prior diagnosis of asthma | Previous diagnosis of COPD, (chronic bronchitis or emphysema) |
| Onset age < 20 years | Onset age > 40 years |
| Variation in respiratory symptoms within short periods | Persistence respiratory symptoms |
| Worsening of symptoms at night or early morning | Daily symptoms and exertional dyspnea |
| Symptoms triggered by exposure to allergens, dust, exercise, or emotions/laughter | Chronic cough and sputum precede onset of dyspnea, unrelated to triggers |
| Family history of asthma, atopy, or eczema | Heavy exposure to a risk factor (such as smoking and biomass fuel) |
| Documented airflow limitation variability (spirometry or peak flow meter) | Documented persistent airflow limitation (post-BD FEV1/FVC < 70%) |
| Normal lung function between symptoms | Abnormal lung function between symptoms |
| No worsening of symptoms over time (symptoms vary either seasonally or from year to year) | Symptoms slowly worsening and progressive over time (years) |
| May improve spontaneously or have an immediate response to BDs or ICS over weeks | Rapid-acting BD provides limited relief |
| Normal chest radiograph | Severe hyperinflation on chest radiograph |
| No. | Reference | Major Criteria | Minor Criteria |
|---|---|---|---|
| 1. | [13] |
|
|
| Required points | 2 | - | |
| OR | 1 | 2 | |
| 2. | [12] |
|
|
| Required points | 2 | - | |
| OR | 1 | 2 | |
| 3. | [9] |
|
|
| Required points | 1 | - | |
| OR | - | 2 | |
| 4. | [10] |
|
|
| Required points | 3 | 1 | |
| ACO in a COPD patient: | |||
| 5. | [11] |
|
|
| ACO in an asthma patient: | |||
|
| ||
| Required points | 2 | 1 | |
| 6. | [14] |
|
|
| Required points | 3 | 1 | |
| Field | Criteria | Comments |
|---|---|---|
| Demographic data | Age ≥ 40 years. | |
| Medical history | A documented asthmatic history before the age of 40. | |
| Prior symptoms of asthma or allergic rhinitis. | ||
| History of atopy and/or allergies. | ||
| ≥10-pack-year of tobacco smoking or equivalent air pollution. | ||
| Symptoms | The frequency, intensity, and duration of respiratory symptoms. | Respiratory symptoms (e.g., dyspnea including exertional dyspnea, cough, sputum) are persistent, but variability in symptoms may be prominent. |
| Exercise limitation. | ||
| Spirometry | Post-BD FEV1/FVC < 70% or LLN and BD increase in FEV1 > 12% and 400 mL. | The assessment of ACO must involve spirometry before and after BD. These tests confirm airflow limitation (obstruction) and evaluate its reversibility. The airflow limitation is not completely reversible, however there has been historical variance. ACO patients usually have a BD response, defined as a post-BD rise in FEV1 or FVC of more than 10% of the predicted value; however, asthma patients usually have an increase in FEV1 or FVC of more than 15% of their predicted value. Post-BD FEV1 and FEV1/FVC are poor in ACO patients. Normal post-BD values suggest asthma. |
| FEV1 < 80%. | ||
| Persistent partially reversible airflow obstruction (without normalization of obstruction). | While airflow limitation is required for ACO diagnosis, it does not assist distinguish ACO from asthma or COPD. | |
| Laboratory tests | A high level of total serum IgE (>100 international units/mL). | Not routinely obtained. May point a practitioner to asthma or ACO. |
| Elevated peripheral blood eosinophil count (>300 cells/µL). | May point a practitioner to asthma or ACO. | |
| Evidence of allergic disease. | Not routinely obtained. May point a practitioner to asthma or ACO. | |
| Elevated sputum eosinophil counts. | Not routinely obtained. More common in asthma or ACO than COPD. | |
| Alpha-1 antitrypsin deficiency. | Recommended for all patients with fixed-airflow limitation. | |
| Imaging | A chest radiograph is often used to diagnose chronic symptoms or an exacerbation. The chest radiograph may indicate hyperinflation in ACO patients, but it does not distinguish between asthma, COPD, and ACO. | |
| If there is diagnostic uncertainty, high-resolution computed tomography may be helpful. Small airway disease without emphysema may be ACO, although asthma (without COPD) and bronchiolitis obliterans should be evaluated. Severe emphysema is more common in COPD than ACO [8]. |
| Intervention | Comments |
|---|---|
| Smoking cessation | For all ACO patients who smoke. Avoiding exposure to additional sources of smoke and irritating inhalants. |
| Vaccination | |
| Annual influenza vaccine | For all adults. |
| Pneumococcus vaccine | Decreases the rate of exacerbations and community-acquired pneumonia. |
| Allergen avoidance | |
| Inhaler technique | At each appointment, the inhaler technique should be reviewed. |
| Pulmonary rehabilitation | These programs are undeniably beneficial for COPD patients and could be helpful supplementary resources for teaching inhaler techniques and keeping the most active lifestyle possible. |
| Class | Biologic Agents | Evidence | References |
|---|---|---|---|
| Anti-IgE therapy | Omalizumab | Reduces exacerbations and improves symptoms moderately in allergic asthma patients with elevated serum IgE levels and sensitivity to perennial allergens; may be advantageous in ACO. | [56,60,61,62,63,64,65] |
| Anti-IL-5/IL-5 receptor alpha (IL-5Ra) therapies | Benralizumab Mepolizumab Reslizumab | Minimizes asthma exacerbations, improves asthma symptoms and quality of life, and reduces systemic corticosteroid use. | [66,67,68] |
| IL-4 receptor alpha (IL-4Ra) and IL-13 therapies | Dupilumab | Enhances lung function and decreases exacerbations in severe asthma, with patients with higher blood eosinophil levels benefiting the most. However, efficacy in COPD and ACO is not established. | [59,69] |
| Anti-thymic stromal lymphopoietin-IgG2λ | Tezepelumab | Add-on controller treatment of severe asthma in adults and children ≥ 12 years of age. | [70,71] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsayed, A.R.; Abu-Samak, M.S.; Alkhatib, M. Asthma-COPD Overlap in Clinical Practice (ACO_CP 2023): Toward Precision Medicine. J. Pers. Med. 2023, 13, 677. https://doi.org/10.3390/jpm13040677
Alsayed AR, Abu-Samak MS, Alkhatib M. Asthma-COPD Overlap in Clinical Practice (ACO_CP 2023): Toward Precision Medicine. Journal of Personalized Medicine. 2023; 13(4):677. https://doi.org/10.3390/jpm13040677
Chicago/Turabian StyleAlsayed, Ahmad R., Mahmoud S. Abu-Samak, and Mohammad Alkhatib. 2023. "Asthma-COPD Overlap in Clinical Practice (ACO_CP 2023): Toward Precision Medicine" Journal of Personalized Medicine 13, no. 4: 677. https://doi.org/10.3390/jpm13040677
APA StyleAlsayed, A. R., Abu-Samak, M. S., & Alkhatib, M. (2023). Asthma-COPD Overlap in Clinical Practice (ACO_CP 2023): Toward Precision Medicine. Journal of Personalized Medicine, 13(4), 677. https://doi.org/10.3390/jpm13040677