

Overweight/Obesity Increases the Risk of Overt Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt in Cirrhotic Patients

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
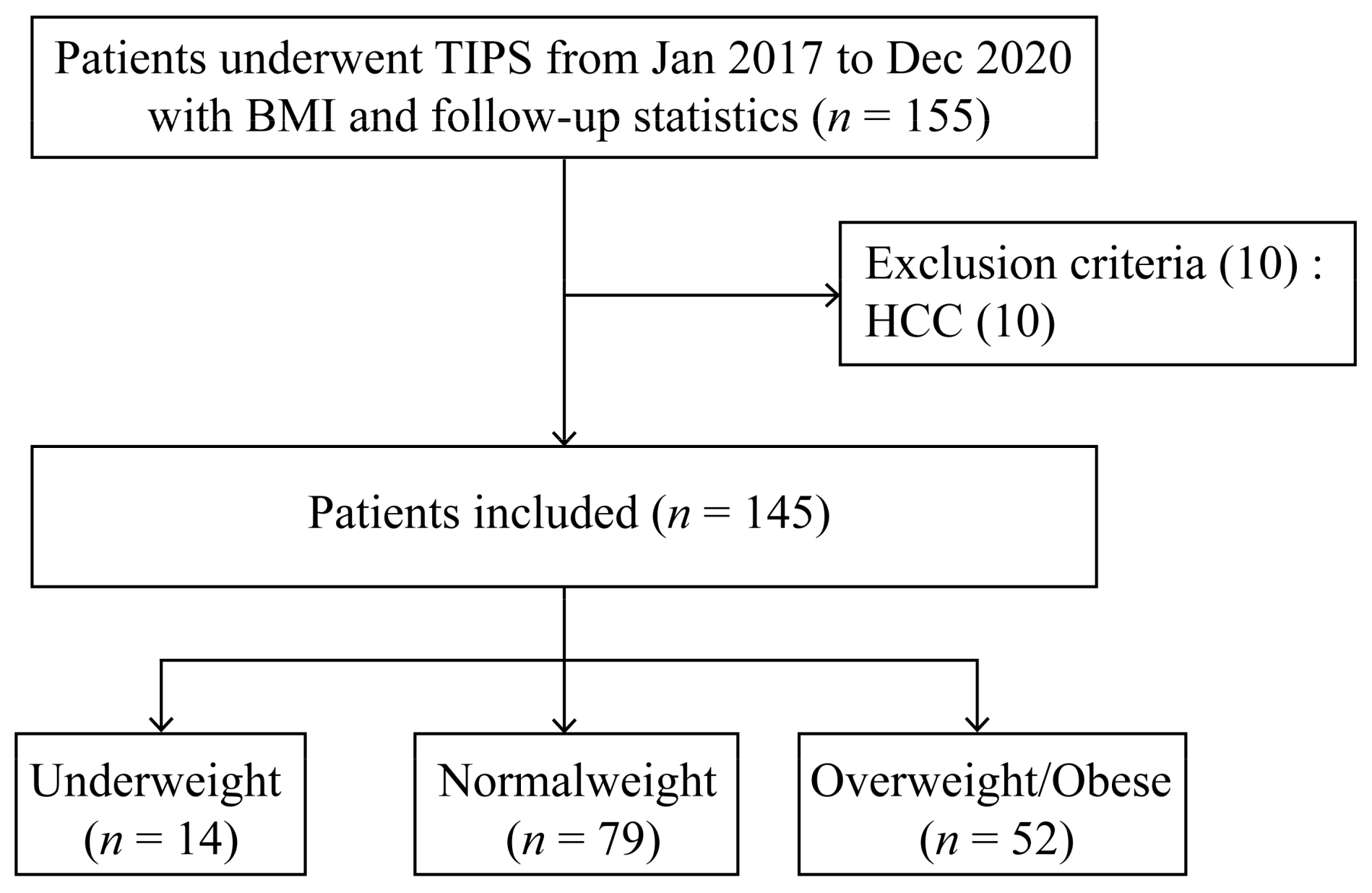
2.1. Patients
2.2. Transjugular Intrahepatic Portosystemic Shunt Procedure
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patients’ Baseline Characteristics
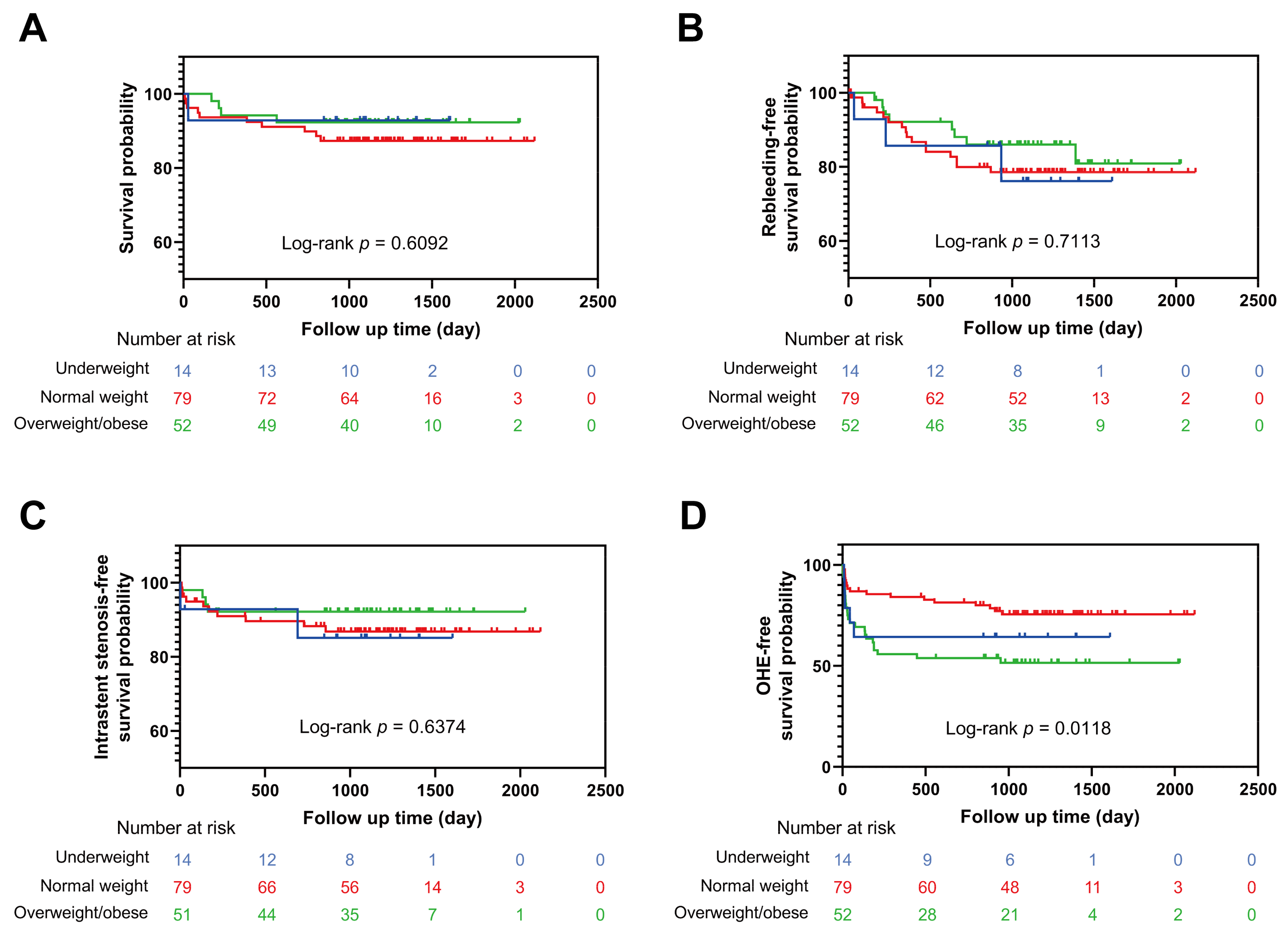
3.2. Hemodynamic Index and Clinical Outcomes
3.3. Relationship between BMI and Post-TIPS OHE
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation; World Health Organization Technical Report Series; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Katzmarzyk, P.T.; Janssen, I.; Ardern, C.I. Physical inactivity, excess adiposity and premature mortality. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2003, 4, 257–290. [Google Scholar] [CrossRef] [PubMed]
- Hourigan, L.F.; Macdonald, G.A.; Purdie, D.; Whitehall, V.H.; Shorthouse, C.; Clouston, A.; Powell, E.E. Fibrosis in chronic hepatitis C correlates significantly with body mass index and steatosis. Hepatology 1999, 29, 1215–1219. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Giral, P.; Charlotte, F.; Bruckert, E.; Thibault, V.; Theodorou, I.; Khalil, L.; Turpin, G.; Opolon, P.; Poynard, T. Liver fibrosis in overweight patients. Gastroenterology 2000, 118, 1117–1123. [Google Scholar] [CrossRef]
- Sanyal, A.J.; Van Natta, M.L.; Clark, J.; Neuschwander-Tetri, B.A.; Diehl, A.; Dasarathy, S.; Loomba, R.; Chalasani, N.; Kowdley, K.; Hameed, B.; et al. Prospective Study of Outcomes in Adults with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2021, 385, 1559–1569. [Google Scholar] [CrossRef]
- Berzigotti, A.; Garcia-Tsao, G.; Bosch, J.; Grace, N.D.; Burroughs, A.K.; Morillas, R.; Escorsell, A.; Garcia-Pagan, J.C.; Patch, D.; Matloff, D.S.; et al. Obesity is an independent risk factor for clinical decompensation in patients with cirrhosis. Hepatology 2011, 54, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, D.; Stanley, A.J.; Hayes, P.C.; Travis, S.; Armstrong, M.J.; Tsochatzis, E.A.; Rowe, I.A.; Roslund, N.; Ireland, H.; Lomax, M.; et al. Transjugular intrahepatic portosystemic stent-shunt in the management of portal hypertension. Gut 2020, 69, 1173–1192. [Google Scholar] [CrossRef]
- Haussinger, D.; Dhiman, R.K.; Felipo, V.; Gorg, B.; Jalan, R.; Kircheis, G.; Merli, M.; Montagnese, S.; Romero-Gomez, M.; Schnitzler, A.; et al. Hepatic encephalopathy. Nat. Rev. Dis. Prim. 2022, 8, 43. [Google Scholar] [CrossRef]
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef]
- Lauridsen, M.M.; Jepsen, P.; Wernberg, C.W.; Schaffalitzky de Muckadell, O.B.; Bajaj, J.S.; Vilstrup, H. Validation of a Simple Quality-of-Life Score for Identification of Minimal and Prediction of Overt Hepatic Encephalopathy. Hepatol. Commun. 2020, 4, 1353–1361. [Google Scholar] [CrossRef]
- Bustamante, J.; Rimola, A.; Ventura, P.J.; Navasa, M.; Cirera, I.; Reggiardo, V.; Rodés, J. Prognostic significance of hepatic encephalopathy in patients with cirrhosis. J. Hepatol. 1999, 30, 890–895. [Google Scholar] [CrossRef]
- Cordoba, J.; Ventura-Cots, M.; Simón-Talero, M.; Amorós, À.; Pavesi, M.; Vilstrup, H.; Angeli, P.; Domenicali, M.; Ginés, P.; Bernardi, M.; et al. Characteristics, risk factors, and mortality of cirrhotic patients hospitalized for hepatic encephalopathy with and without acute-on-chronic liver failure (ACLF). J. Hepatol. 2014, 60, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Häussinger, D.; Kircheis, G.; Fischer, R.; Schliess, F.; vom Dahl, S. Hepatic encephalopathy in chronic liver disease: A clinical manifestation of astrocyte swelling and low-grade cerebral edema? J. Hepatol. 2000, 32, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Ott, P.; Larsen, F.S. Blood-brain barrier permeability to ammonia in liver failure: A critical reappraisal. Neurochem. Int. 2004, 44, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Frieg, B.; Görg, B.; Gohlke, H.; Häussinger, D. Glutamine synthetase as a central element in hepatic glutamine and ammonia metabolism: Novel aspects. Biol. Chem. 2021, 402, 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- Coltart, I.; Tranah, T.H.; Shawcross, D.L. Inflammation and hepatic encephalopathy. Arch. Biochem. Biophys. 2013, 536, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Shawcross, D.L.; Davies, N.A.; Williams, R.; Jalan, R. Systemic inflammatory response exacerbates the neuropsychological effects of induced hyperammonemia in cirrhosis. J. Hepatol. 2004, 40, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Rose, C.F.; Amodio, P.; Bajaj, J.S.; Dhiman, R.K.; Montagnese, S.; Taylor-Robinson, S.D.; Vilstrup, H.; Jalan, R. Hepatic encephalopathy: Novel insights into classification, pathophysiology and therapy. J. Hepatol. 2020, 73, 1526–1547. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Zhang, F.; Xiao, J.; Wang, Y.; He, Q.; Zhu, H.; Leng, X.; Zou, X.; Zhang, M.; Zhuge, Y. Diabetes mellitus increases the risk of hepatic encephalopathy after a transjugular intrahepatic portosystemic shunt in cirrhotic patients. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1264–1269. [Google Scholar] [CrossRef]
- Bhanji, R.A.; Moctezuma-Velazquez, C.; Duarte-Rojo, A.; Ebadi, M.; Ghosh, S.; Rose, C.; Montano-Loza, A.J. Myosteatosis and sarcopenia are associated with hepatic encephalopathy in patients with cirrhosis. Hepatol. Int. 2018, 12, 377–386. [Google Scholar] [CrossRef]
- Nardelli, S.; Lattanzi, B.; Merli, M.; Farcomeni, A.; Gioia, S.; Ridola, L.; Riggio, O. Muscle Alterations Are Associated with Minimal and Overt Hepatic Encephalopathy in Patients with Liver Cirrhosis. Hepatology 2019, 70, 1704–1713. [Google Scholar] [CrossRef]
- Barazzoni, R.; Bischoff, S.; Boirie, Y.; Busetto, L.; Cederholm, T.; Dicker, D.; Toplak, H.; Van Gossum, A.; Yumuk, V.; Vettor, R. Sarcopenic Obesity: Time to Meet the Challenge. Obes. Facts 2018, 11, 294–305. [Google Scholar] [CrossRef]
- Choi, K.M. Sarcopenia and sarcopenic obesity. Korean J. Intern. Med. 2016, 31, 1054–1060. [Google Scholar] [CrossRef]
- Gregor, M.F.; Hotamisligil, G.S. Inflammatory mechanisms in obesity. Annu. Rev. Immunol. 2011, 29, 415–445. [Google Scholar] [CrossRef] [PubMed]
- Gioia, S.; Ridola, L.; Cristofaro, L.; Merli, M.; Faccioli, J.; Riggio, O.; Nardelli, S. The improvement in body composition including subcutaneous and visceral fat reduces ammonia and hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. Liver Int. Off. J. Int. Assoc. Study Liver 2021, 41, 2965–2973. [Google Scholar] [CrossRef] [PubMed]
- Barb, D.; Repetto, E.M.; Stokes, M.E.; Shankar, S.S.; Cusi, K. Type 2 diabetes mellitus increases the risk of hepatic fibrosis in individuals with obesity and nonalcoholic fatty liver disease. Obesity 2021, 29, 1950–1960. [Google Scholar] [CrossRef]
- Anstee, Q.M.; Lawitz, E.J.; Alkhouri, N.; Wong, V.W.-S.; Romero-Gomez, M.; Okanoue, T.; Trauner, M.; Kersey, K.; Li, G.; Han, L.; et al. Noninvasive Tests Accurately Identify Advanced Fibrosis due to NASH: Baseline Data from the STELLAR Trials. Hepatology 2019, 70, 1521–1530. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Stepanova, M.; Rafiq, N.; Henry, L.; Loomba, R.; Makhlouf, H.; Goodman, Z. Nonalcoholic steatofibrosis independently predicts mortality in nonalcoholic fatty liver disease. Hepatol. Commun. 2017, 1, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, R.R.; Corriere, M.; Ferrucci, L. Age-related and disease-related muscle loss: The effect of diabetes, obesity, and other diseases. Lancet Diabetes Endocrinol. 2014, 2, 819–829. [Google Scholar] [CrossRef]
- Adler, M.; Schaffner, F. Fatty liver hepatitis and cirrhosis in obese patients. Am. J. Med. 1979, 67, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Kanoski, S.E.; Davidson, T.L. Different patterns of memory impairments accompany short- and longer-term maintenance on a high-energy diet. J. Exp. Psychol. Anim. Behav. Process. 2010, 36, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Hadjihambi, A.; Konstantinou, C.; Klohs, J.; Monsorno, K.; Le Guennec, A.; Donnelly, C.; Cox, I.J.; Kusumbe, A.; Hosford, P.S.; Soffientini, U.; et al. Partial MCT1 invalidation protects against diet-induced non-alcoholic fatty liver disease and the associated brain dysfunction. J. Hepatol. 2023, 78, 180–190. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.N.; Weiss, N.S.; Kowdley, K.V.; Dominitz, J.A. Is obesity a risk factor for cirrhosis-related death or hospitalization? A population-based cohort study. Gastroenterology 2003, 125, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Hagström, H.; Stål, P.; Hultcrantz, R.; Hemmingsson, T.; Andreasson, A. Overweight in late adolescence predicts development of severe liver disease later in life: A 39 years follow-up study. J. Hepatol. 2016, 65, 363–368. [Google Scholar] [CrossRef]
- Stender, S.; Kozlitina, J.; Nordestgaard, B.G.; Tybjærg-Hansen, A.; Hobbs, H.H.; Cohen, J.C. Adiposity amplifies the genetic risk of fatty liver disease conferred by multiple loci. Nat. Genet. 2017, 49, 842–847. [Google Scholar] [CrossRef]
- Romeo, S.; Sentinelli, F.; Dash, S.; Yeo, G.S.H.; Savage, D.B.; Leonetti, F.; Capoccia, D.; Incani, M.; Maglio, C.; Iacovino, M.; et al. Morbid obesity exposes the association between PNPLA3 I148M (rs738409) and indices of hepatic injury in individuals of European descent. Int. J. Obes. 2010, 34, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Giudice, E.M.d.; Grandone, A.; Cirillo, G.; Santoro, N.; Amato, A.; Brienza, C.; Savarese, P.; Marzuillo, P.; Perrone, L. The association of PNPLA3 variants with liver enzymes in childhood obesity is driven by the interaction with abdominal fat. PLoS ONE 2011, 6, e27933. [Google Scholar] [CrossRef]
- Emdin, C.A.; Haas, M.; Ajmera, V.; Simon, T.G.; Homburger, J.; Neben, C.; Jiang, L.; Wei, W.-Q.; Feng, Q.; Zhou, A.; et al. Association of Genetic Variation with Cirrhosis: A Multi-Trait Genome-Wide Association and Gene-Environment Interaction Study. Gastroenterology 2021, 160, 1620–1633. [Google Scholar] [CrossRef]
- Johnston, H.E.; Takefala, T.G.; Kelly, J.T.; Keating, S.E.; Coombes, J.S.; Macdonald, G.A.; Hickman, I.J.; Mayr, H.L. The Effect of Diet and Exercise Interventions on Body Composition in Liver Cirrhosis: A Systematic Review. Nutrients 2022, 14, 3365. [Google Scholar] [CrossRef]
- Hernández-Conde, M.; Llop, E.; Gómez-Pimpollo, L.; Fernández Carrillo, C.; Rodríguez, L.; Van Den Brule, E.; Perelló, C.; López-Gómez, M.; Abad, J.; Martínez-Porras, J.L.; et al. Adding Branched-Chain Amino Acids to an Enhanced Standard-of-Care Treatment Improves Muscle Mass of Cirrhotic Patients with Sarcopenia: A Placebo-Controlled Trial. Am. J. Gastroenterol. 2021, 116, 2241–2249. [Google Scholar] [CrossRef] [PubMed]
- Estrada, J.A.; Contreras, I. Nutritional Modulation of Immune and Central Nervous System Homeostasis: The Role of Diet in Development of Neuroinflammation and Neurological Disease. Nutrients 2019, 11, 1076. [Google Scholar] [CrossRef] [PubMed]
- Berzigotti, A.; Albillos, A.; Villanueva, C.; Genescá, J.; Ardevol, A.; Augustín, S.; Calleja, J.L.; Bañares, R.; García-Pagán, J.C.; Mesonero, F.; et al. Effects of an intensive lifestyle intervention program on portal hypertension in patients with cirrhosis and obesity: The SportDiet study. Hepatology 2017, 65, 1293–1305. [Google Scholar] [CrossRef]
- Jepsen, P.; Watson, H.; Andersen, P.K.; Vilstrup, H. Diabetes as a risk factor for hepatic encephalopathy in cirrhosis patients. J. Hepatol. 2015, 63, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Gil-Gómez, A.; Ampuero, J.; Rojas, Á.; Gallego-Durán, R.; Muñoz-Hernández, R.; Rico, M.C.; Millán, R.; García-Lozano, R.; Francés, R.; Soriano, G.; et al. Development and Validation of a Clinical-Genetic Risk Score to Predict Hepatic Encephalopathy in Patients with Liver Cirrhosis. Am. J. Gastroenterol. 2021, 116, 1238–1247. [Google Scholar] [CrossRef] [PubMed]
- Gairing, S.J.; Schleicher, E.M.; Labenz, C. Diabetes mellitus—Risk factor and potential future target for hepatic encephalopathy in patients with liver cirrhosis? Metab. Brain Dis. 2022, 1–10. [Google Scholar] [CrossRef]
- Louissaint, J.; Deutsch-Link, S.; Tapper, E.B. Changing Epidemiology of Cirrhosis and Hepatic Encephalopathy. Clin. Gastroenterol. Hepatol. 2022, 20, S1–S8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total (n = 145) | Underweight (n = 14) | Normal Weight (n = 79) | Overweight/Obese (n = 52) | p Value |
|---|---|---|---|---|---|
| Age (years) | 58 (50–66) | 52.5 (47.5–58) | 58 (51–66) | 60.5 (49.5–66.8) | 0.468 |
| Gender (male) | 92 (63.4%) | 10 (71.4%) | 46 (58.2%) | 36 (69.2%) | 0.357 |
| BMI (kg/m2) | 21.95 (20.05–24.04) | 17.75 (17.20–18.08) | 21.09 (19.84–21.97) | 24.98 (23.88–26.49) | <0.001 |
| Etiology (virus/others) | 73/72 | 10/4 | 38/41 | 25/27 | 0.252 |
| Ascites * (no/light/medium/heavy) | 10/35/32/67 | 0/1/2/10 | 5/18/20/36 | 5/16/10/21 | 0.342 |
| Diabetes | 25 (17.2%) | 2 (14.3%) | 11 (13.9%) | 12 (23.1%) | 0.413 |
| Hypertension | 13 (9.0%) | 1 (7.1%) | 7 (8.9%) | 5 (9.6%) | >0.999 |
| Pre-TIPS OHE | 1 (0.7%) | 0 (0%) | 0 (0%) | 1 (1.9%) | 0.455 |
| Spleen | 121 (83.4%) | 11 (78.6%) | 66 (83.5%) | 44 (84.6%) | 0.864 |
| Portal thrombosis | 53 (36.6%) | 4 (28.6%) | 29 (36.7%) | 20 (38.5%) | 0.792 |
| PT (s) | 14.1 (13.0–15.1) | 14.5 (14.1–15.6) | 14.2 (12.7–15.1) | 13.8 (13.0–15.0) | 0.386 |
| INR | 1.24 (1.14–1.34) | 1.28 (1.23–1.38) | 1.24 (1.11–1.33) | 1.22 (1.14–1.34) | 0.295 |
| Fib (g/L) | 1.7 (1.4–2.2) | 1.5 (1.2–1.7) | 1.8 (1.5–2.3) | 1.7 (1.5–2.3) | 0.190 |
| ALT (U/L) | 18.80 (13.65–26.50) | 16.75 (10.90–26.80) | 19.9 (13.8–34.3) | 18.5 (13.3–24.9) | 0.352 |
| AST (U/L) | 25.0 (20.2–35.1) | 21.4 (16.3–38.5) | 24.9 (20.5–37.0) | 27.2 (21.1–31.4) | 0.339 |
| TB (μmol/L) | 15.5 (10.9–22.8) | 15.2 (8.4–21.5) | 15.2 (10.3–21.9) | 16.2 (11.7–23.7) | 0.698 |
| ALB (g/L) | 34.20 (31.50–37.05) | 33.20 (30.25–37.15) | 34.30 (31.60–36.90) | 33.95 (31.25–37.38) | 0.885 |
| Cr (μmol/L) | 59 (50–71) | 65 (53–78) | 60 (48–71) | 58 (51–65) | 0.408 |
| WBC (*10^9/L) | 2.50 (1.80–4.30) | 1.95 (1.48–3.75) | 2.45 (1.68–4.33) | 2.70 (2.00–4.60) | 0.228 |
| PLT (*10^9/L) | 65.0 (40.5–112.0) | 46.0 (39.8–66.8) | 63.0 (40.0–102.0) | 76.5 (41.0–124.0) | 0.185 |
| MELD score | 9 (8–11) | 10 (9–12) | 9 (8–11) | 10 (8–11) | 0.527 |
| CTP score | 7 (6–8) | 7 (6–8) | 7 (6–7) | 7 (6–8) | 0.490 |
| CTP class (A/B/C) | 56/88/1 | 5/9/0 | 27/52/0 | 24/27/1 | 0.333 |
| Patients received 8 mm stents | 109 (75.2%) | 12 (85.7%) | 56 (70.9%) | 41 (78.8%) | 0.370 |
| Duration of follow-up (day) | 1224 (1044–1443) | 1099 (923–1404) | 1230 (1051–1443) | 1200 (1034–1470) | 0.597 |
| Total (n = 145) | Underweight (n = 14) | Normal Weight (n = 79) | Overweight/Obese (n = 52) | p Value | |
|---|---|---|---|---|---|
| Hemodynamic index | |||||
| Pre-TIPS PPG (mmHg) | 22 (20–27) | 25 (22–27) | 24 (20–28) | 20 (18–25) | 0.005 |
| Post-TIPS PPG (mmHg) | 9 (6–12) | 10 (6–12) | 9 (5–12) | 8 (6–11) | 0.780 |
| Final PPG ≤ 12 mmHg | 116 (80%) | 11 (79%) | 62 (78%) | 43 (83%) | 0.832 |
| Percentage of PPG drop (%) | 60 (46–75) | 61 (55–77) | 61 (50–75) | 57 (45–73) | 0.548 |
| PPG drop ≥ 50% baseline | 104 (72%) | 11 (79%) | 60 (76%) | 33 (63%) | 0.250 |
| Good response to TIPS * | 121 (83%) | 12 (86%) | 65 (82%) | 44 (85%) | 0.913 |
| Pre-TIPS NH3 (μmol/L) | 25.50 (12.50–40.00) | 9.00 (9.00–49.50) | 25.00 (14.00–39.50) | 29.50 (16.25–40.50) | 0.483 |
| Post-TIPS NH3 (μmol/L) | 33.00 (22.00–49.00) | 32.50 (10.50–55.00) | 32.00 (18.75–49.25) | 38.00 (25.00–49.00) | 0.537 |
| Outcomes | |||||
| Variceal rebleeding | 27 (19%) | 3 (21%) | 16 (20%) | 8 (15%) | 0.752 |
| Intrastent stenosis | 17 (12%) | 2 (14%) | 10 (13%) | 5 (10%) | 0.827 |
| OHE | 50 (34%) | 5 (36%) | 20 (25%) | 25 (48%) | 0.027 |
| Death | 15 (10%) | 1 (7%) | 10 (13%) | 4 (8%) | 0.605 |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Age | 1.040 (1.006–1.075) | 0.020 | 1.041 (1.004–1.080) | 0.030 |
| Male | 2.070 (0.976–4.390) | 0.058 | 1.859 (0.797–4.337) | 0.151 |
| BMI | ||||
| Normal weight | ||||
| Underweight | 1.639 (0.491–5.469) | 0.422 | 1.749 (0.485–6.301) | 0.393 |
| Overweight/obese | 2.731 (1.298–5.746) | 0.008 | 2.754 (1.236–6.140) | 0.013 |
| Etiology (virus) | 1.414 (0.710–2.815) | 0.324 | ||
| Diabetes | 1.992 (0.831–4.773) | 0.122 | ||
| Hypertension | 1.208 (0.374–3.908) | 0.752 | ||
| Spleen | 1.063 (0.421–2.688) | 0.897 | ||
| Portal thrombosis | 0.964 (0.473–1.966) | 0.920 | ||
| PT (s) | 0.902 (0.726–1.120) | 0.350 | ||
| INR | 0.291 (0.030–2.796) | 0.285 | ||
| Fib (g/L) | 1.331 (0.739–2.398) | 0.341 | ||
| TB (μmmol/L) | 1.001 (0.972–1.032) | 0.922 | ||
| ALB (g/L) | 0.993 (0.912–1.082) | 0.878 | ||
| Cr (μmol/L) | 1.016 (1.001–1.031) | 0.033 | 1.014 (0.998–1.029) | 0.079 |
| WBC (*10^9/L) | 1.100 (0.947–1.277) | 0.213 | ||
| PLT (*10^9/L) | 1.001 (0.997–1.005) | 0.777 | ||
| MELD score | 1.075 (0.944–1.224) | 0.277 | ||
| CTP score | 1.090 (0.810–1.466) | 0.570 | ||
| Ascites | ||||
| No | ||||
| Light | 2.667 (0.492–14.461) | 0.256 | ||
| Medium | 2.095 (0.378–11.615) | 0.397 | ||
| Heavy | 2.091 (0.410–10.666) | 0.375 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, L.; Yin, X.; Cheng, Y.; Wang, X.; Zhang, M.; Zou, X.; Wang, L.; Zhuge, Y.; Zhang, F. Overweight/Obesity Increases the Risk of Overt Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt in Cirrhotic Patients. J. Pers. Med. 2023, 13, 682. https://doi.org/10.3390/jpm13040682
Gu L, Yin X, Cheng Y, Wang X, Zhang M, Zou X, Wang L, Zhuge Y, Zhang F. Overweight/Obesity Increases the Risk of Overt Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt in Cirrhotic Patients. Journal of Personalized Medicine. 2023; 13(4):682. https://doi.org/10.3390/jpm13040682
Chicago/Turabian StyleGu, Lihong, Xiaochun Yin, Yang Cheng, Xixuan Wang, Ming Zhang, Xiaoping Zou, Lei Wang, Yuzheng Zhuge, and Feng Zhang. 2023. "Overweight/Obesity Increases the Risk of Overt Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt in Cirrhotic Patients" Journal of Personalized Medicine 13, no. 4: 682. https://doi.org/10.3390/jpm13040682
APA StyleGu, L., Yin, X., Cheng, Y., Wang, X., Zhang, M., Zou, X., Wang, L., Zhuge, Y., & Zhang, F. (2023). Overweight/Obesity Increases the Risk of Overt Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt in Cirrhotic Patients. Journal of Personalized Medicine, 13(4), 682. https://doi.org/10.3390/jpm13040682