
Personalized Interventional Surgery of the Lumbar Spine: A Perspective on Minimally Invasive and Neuroendoscopic Decompression for Spinal Stenosis
 ,
, 


 , ,
, ,  , ,
, , 
Abstract
:1. Introduction and Method:
Method
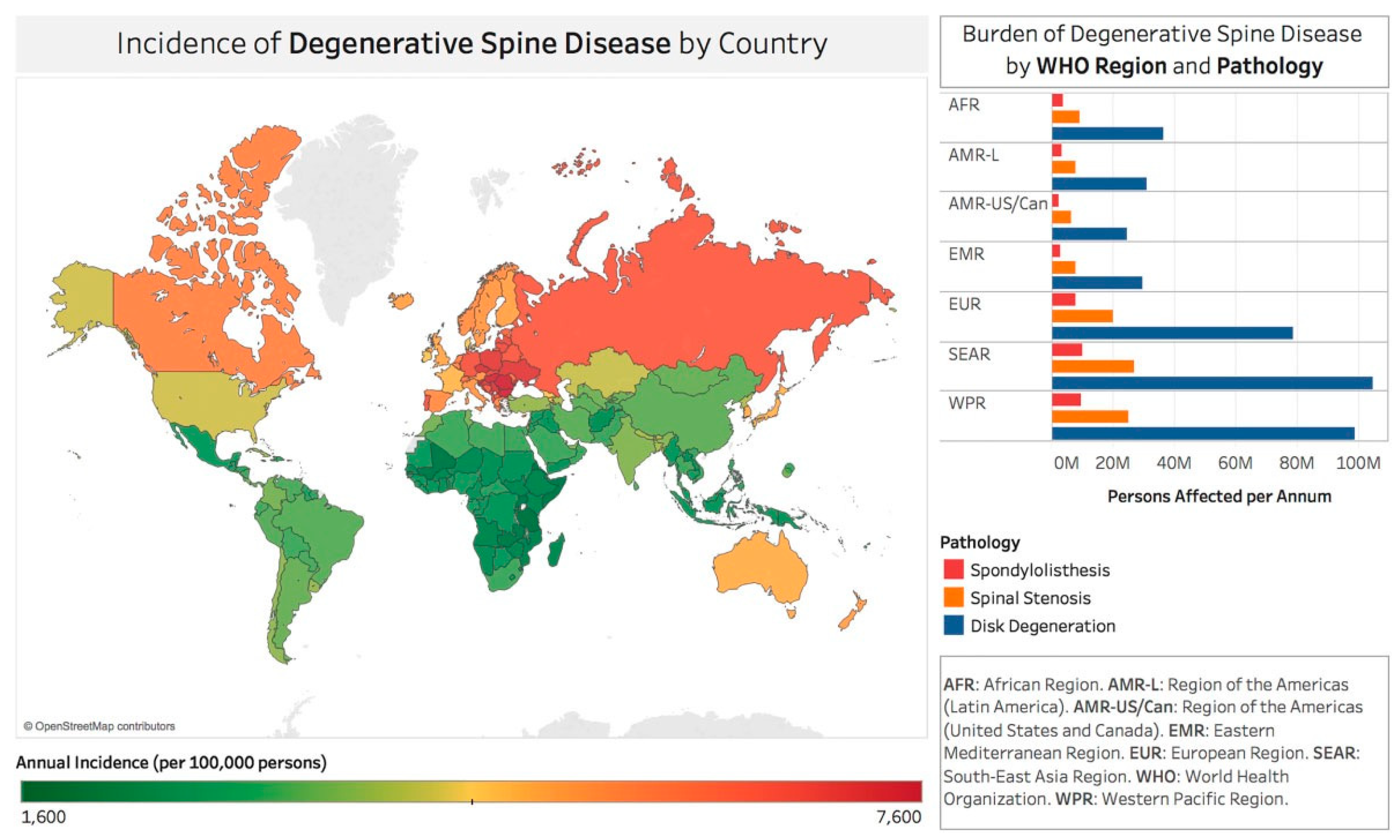
2. Disease Burden
3. Medical Necessity Criteria
4. Timing of Intervention
5. Standards
6. Minimally Invasive Spine Surgery
7. Cost Effectiveness of MIS
8. Pain Generators
9. Direct Visualization
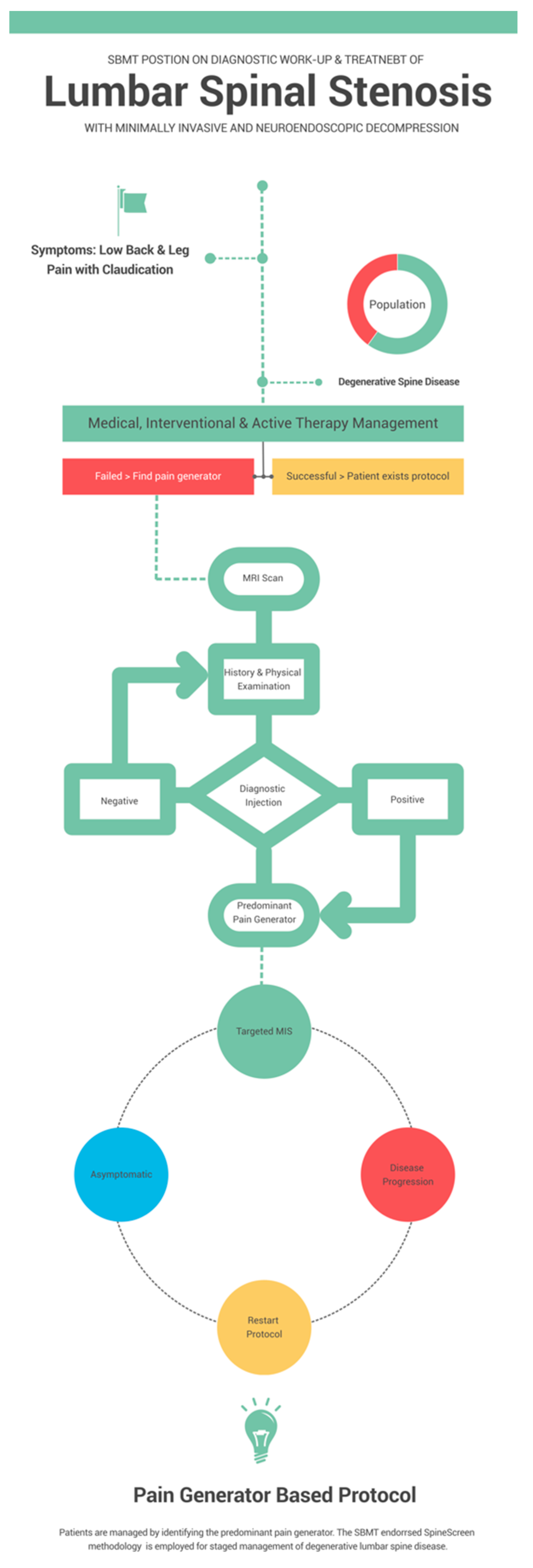
10. Staged Management
11. Surgical Pain Management
12. Discussion
13. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Otani, K.; Kikuchi, S.; Yabuki, S.; Igarashi, T.; Nikaido, T.; Watanabe, K.; Konno, S. Lumbar Spinal Stenosis Has a Negative Impact on Quality of Life Compared with other Comorbidities: An Epidemiological Cross-Sectional Study of 1862 Community-Dwelling Individuals. Sci. World J. 2013, 2013, 590652. [Google Scholar] [CrossRef] [PubMed]
- Kuittinen, P.; Sipola, P.; Leinonen, V.; Saari, T.; Sinikallio, S.; Savolainen, S.; Kröger, H.; Turunen, V.; Airaksinen, O.; Aalto, T. Preoperative MRI Findings Predict Two-Year Postoperative Clinical Outcome in Lumbar Spinal Stenosis. PLoS ONE 2014, 9, e106404. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Zimmerman, Z.E.; Mass, H.; Makhni, M.C. Diagnosis and Management of Lumbar Spinal Stenosis: A Review. JAMA 2022, 327, 1688–1699. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Mirza, S.K.; Martin, B.I.; Kreuter, W.; Goodman, D.C.; Jarvik, J.G. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA 2010, 303, 1259–1265. [Google Scholar] [CrossRef]
- Ziino, C.; Mertz, K.; Hu, S.; Kamal, R. Decompression With or Without Fusion for Lumbar Stenosis: A Cost Minimization Analysis. Spine 2020, 45, 325–332. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Lurie, J.D.; Olson, P.R.; Bronner, K.K.; Fisher, E.S. United States’ trends and regional variations in lumbar spine surgery: 1992–2003. Spine 2006, 31, 2707–2714. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Lurie, J.D.; Tosteson, T.D.; Zhao, W.; Blood, E.A.; Tosteson, A.N.; Birkmeyer, N.; Herkowitz, H.; Longley, M.; Lenke, L.; et al. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J. Bone Jt. Surg. Am. 2009, 91, 1295–1304. [Google Scholar] [CrossRef]
- Fox, M.W.; Onofrio, B.M. Indications for fusion following decompression for lumbar spinal stenosis. Neurosurg. Focus 1997, 3, E4. [Google Scholar] [CrossRef]
- Sigmundsson, F.G.; Joelson, A.; Strömqvist, F. Additional operations after surgery for lumbar disc prolapse : Indications, type of surgery, and long-term follow-up of primary operations performed from 2007 to 2008. Bone Jt. J. 2022, 104-b, 627–632. [Google Scholar] [CrossRef]
- Zhai, S.; Zhao, W.; Bin Zhu, B.; Huang, X.; Liang, C.; Hai, B.; Ding, L.; Zhu, H.; Wang, X.; Wei, F.; et al. The effectiveness of percutaneous endoscopic decompression compared with open decompression and fusion for lumbar spinal stenosis: Protocol for a multicenter, prospective, cohort study. BMC Musculoskelet. Disord. 2022, 23, 1–8. [Google Scholar] [CrossRef]
- Yeung, A.; Lewandrowski, K.-U. Five-year clinical outcomes with endoscopic transforaminal foraminoplasty for symptomatic degenerative conditions of the lumbar spine: A comparative study of inside-out versus outside-in techniques. J. Spine Surg. 2020, 6, S66–S83. [Google Scholar] [CrossRef]
- Lewandrowski, K.-U.; Ransom, N.A. Five-year clinical outcomes with endoscopic transforaminal outside-in foraminoplasty techniques for symptomatic degenerative conditions of the lumbar spine. J. Spine Surg. 2020, 6, S54–S65. [Google Scholar] [CrossRef] [PubMed]
- Gadjradj, P.S.; Broulikova, H.M.; van Dongen, J.M.; Rubinstein, S.M.; Depauw, P.R.; Vleggeert, C.; Seiger, A.; Peul, W.C.; van Susante, J.L.; van Tulder, M.W.; et al. Cost-effectiveness of full endoscopic versus open discectomy for sciatica. Br. J. Sports Med. 2022, 56, 1018–1025. [Google Scholar] [CrossRef]
- Hasan, S.; Härtl, R.; Hofstetter, C.P. The benefit zone of full-endoscopic spine surgery. J. Spine Surg. 2019, 5, S41–S56. [Google Scholar] [CrossRef] [PubMed]
- Muthu, S.; Ramakrishnan, E.; Chellamuthu, G. Is Endoscopic Discectomy the Next Gold Standard in the Management of Lumbar Disc Disease? Systematic Review and Superiority Analysis. Glob. Spine J. 2020, 11, 1104–1120. [Google Scholar] [CrossRef] [PubMed]
- Perez-Roman, R.J.; Gaztanaga, W.; Lu, V.M.; Wang, M.Y. Endoscopic decompression for the treatment of lumbar spinal stenosis: An updated systematic review and meta-analysis. J. Neurosurgery: Spine 2022, 36, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Shen, J.; Zheng, B.; Huang, Y.; Jin, M.; Morizane, K.; Shao, H.; Chen, X.; Zhang, J. The 100 Most-Cited Publications in Endoscopic Spine Surgery Research. Glob. Spine J. 2020, 11, 587–596. [Google Scholar] [CrossRef]
- Lin, G.-X.; Kotheeranurak, V.; Mahatthanatrakul, A.; Ruetten, S.; Yeung, A.; Lee, S.-H.; Ahn, Y.; Kim, H.-S.; Hofstetter, C.; Lee, J.H.; et al. Worldwide research productivity in the field of full-endoscopic spine surgery: A bibliometric study. Eur. Spine J. 2020, 29, 153–160. [Google Scholar] [CrossRef]
- Lewandrowski, K.-U.; Soriano-Sánchez, J.-A.; Zhang, X.; León, J.F.R.; Solis, S.S.; Ortíz, J.G.R.; Cuéllar, G.O.A.; Silva, M.S.D.L.E.; Hellinger, S.; Dowling, Á.; et al. Surgeon training and clinical implementation of spinal endoscopy in routine practice: Results of a global survey. J. Spine Surg. 2020, 6, S237–S248. [Google Scholar] [CrossRef]
- Lewandrowski, K.-U.; Soriano-Sánchez, J.-A.; Zhang, X.; León, J.F.R.; Solis, S.S.; Ortíz, J.G.R.; Martínez, C.R.; Cuéllar, G.O.A.; Liu, K.; Fu, Q.; et al. Regional variations in acceptance, and utilization of minimally invasive spinal surgery techniques among spine surgeons: Results of a global survey. J. Spine Surg. 2020, 6, S260–S274. [Google Scholar] [CrossRef]
- Ravindra, V.M.; Senglaub, S.S.; Rattani, A.; Dewan, M.C.; Härtl, R.; Bisson, E.; Park, K.B.; Shrime, M.G. Degenerative Lumbar Spine Disease: Estimating Global Incidence and Worldwide Volume. Glob. Spine J. 2018, 8, 784–794. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, T.; Jacklyn, G.; Orchard, J.; Passmore, E.; Vos, T.; Freedman, G.; Lim, S.; Punnett, L. The global burden of occupationally related low back pain: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 975–981. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Bain, C.; Williams, G.; Smith, E.; Vos, T.; Barendregt, J.; et al. The global burden of low back pain: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. GBD 2019 Diseases and Injuries Collaborators. Lancet 2020, 396, 1204–1222. [CrossRef]
- Manchikanti, L.; Abdi, S.; Atluri, S.; Benyamin, R.M.; Boswell, M.V.; Buenaventura, R.M.; A Bryce, D.; A Burks, P.; Caraway, D.L.; Calodney, A.K.; et al. An update of comprehensive evidence-based guidelines for interventional techniques in chronic spinal pain. Part II: Guidance and recommendations. Pain Physician 2013, 16. [Google Scholar]
- Choudhri, T.F.; Mummaneni, P.V.; Dhall, S.S.; Eck, J.C.; Groff, M.W.; Ghogawala, Z.; Watters, W.C.; Dailey, A.T.; Resnick, D.K.; Sharan, A.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 4: Radiographic assessment of fusion status. J. Neurosurgery: Spine 2014, 21, 23–30. [Google Scholar] [CrossRef]
- Dailey, A.T.; Ghogawala, Z.; Choudhri, T.F.; Watters, W.C., 3rd; Resnick, D.K.; Sharan, A.; Eck, J.C.; Mummaneni, P.V.; Wang, J.C.; Groff, M.W.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 14: Brace therapy as an adjunct to or substitute for lumbar fusion. J. Neurosurg. Spine 2014, 21, 91–101. [Google Scholar] [CrossRef]
- Eck, J.C.; Sharan, A.; Ghogawala, Z.; Resnick, D.K.; Watters, W.C., 3rd; Mummaneni, P.V.; Dailey, A.T.; Choudhri, T.F.; Groff, M.W.; Wang, J.C.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 7: Lumbar fusion for intractable low-back pain without stenosis or spondylolisthesis. J. Neurosurg. Spine 2014, 21, 42–47. [Google Scholar] [CrossRef]
- Ghogawala, Z.; Resnick, D.K.; Watters, W.C., 3rd; Mummaneni, P.V.; Dailey, A.T.; Choudhri, T.F.; Eck, J.C.; Sharan, A.; Groff, M.W.; Wang, J.C.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 2: Assessment of functional outcome following lumbar fusion. J. Neurosurg. Spine 2014, 21, 7–13. [Google Scholar] [CrossRef]
- Groff, M.W. Introduction: Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. J. Neurosurgery: Spine 2014, 21, 1. [Google Scholar] [CrossRef]
- Kaiser, M.G.; Eck, J.C.; Groff, M.W.; Ghogawala, Z.; Watters, W.C., 3rd; Dailey, A.T.; Resnick, D.K.; Choudhri, T.F.; Sharan, A.; Wang, J.C.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 17: Bone growth stimulators as an adjunct for lumbar fusion. J. Neurosurg. Spine 2014, 21, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Kreiner, D.S.; Baisden, J.; Gilbert, T.; Shaffer, W.O.; Summers, J.T. Re: Diagnostic tests the NASS stenosis guidelines. Spine J. 2014, 14, 201–202. [Google Scholar] [CrossRef] [PubMed]
- Kreiner, D.S.; Hwang, S.W.; Easa, J.E.; Resnick, D.K.; Baisden, J.L.; Bess, S.; Cho, C.H.; DePalma, M.J.; Dougherty, P.; Fernand, R.; et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014, 14, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Dhall, S.S.; Eck, J.C.; Groff, M.W.; Ghogawala, Z.; Watters, W.C., 3rd; Dailey, A.T.; Resnick, D.K.; Choudhri, T.F.; Sharan, A.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 11: Interbody techniques for lumbar fusion. J. Neurosurg. Spine 2014, 21, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Resnick, D.K.; Watters, W.C.; 3rd Mummaneni, P.V.; Dailey, A.T.; Choudhri, T.F.; Eck, J.C.; Sharan, A.; Groff, M.W.; Wang, J.C.; Ghogawala, Z.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 10: Lumbar fusion for stenosis without spondylolisthesis. J. Neurosurg. Spine 2014, 21, 62–66. [Google Scholar] [CrossRef]
- Resnick, D.K.; Watters, W.C., 3rd; Sharan, A.; Mummaneni, P.V.; Dailey, A.T.; Wang, J.C.; Choudhri, T.F.; Eck, J.; Ghogawala, Z.; Groff, M.W.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 9: Lumbar fusion for stenosis with spondylolisthesis. J. Neurosurg. Spine 2014, 21, 54–61. [Google Scholar] [CrossRef]
- Sharan, A.; Groff, M.W.; Dailey, A.T.; Ghogawala, Z.; Resnick, D.K.; Watters, W.C., 3rd; Mummaneni, P.V.; Choudhri, T.F.; Eck, J.C.; Wang, J.C.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 15: Electrophysiological monitoring and lumbar fusion. J. Neurosurg. Spine 2014, 21, 102–105. [Google Scholar] [CrossRef]
- Wang, J.C.; Dailey, A.T.; Mummaneni, P.V.; Ghogawala, Z.; Resnick, D.K.; Watters, W.C., 3rd; Groff, M.W.; Choudhri, T.F.; Eck, J.C.; Sharan, A.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 8: Lumbar fusion for disc herniation and radiculopathy. J. Neurosurg. Spine 2014, 21, 48–53. [Google Scholar] [CrossRef]
- Watters, W.C., 3rd; Resnick, D.K.; Eck, J.C.; Ghogawala, Z.; Mummaneni, P.V.; Dailey, A.T.; Choudhri, T.F.; Sharan, A.; Groff, M.W.; Wang, J.C.; et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 13: Injection therapies, low-back pain, and lumbar fusion. J. Neurosurg. Spine 2014, 21, 79–90. [Google Scholar] [CrossRef]
- Matz, P.G.; Meagher, R.; Lamer, T.; Tontz, W.L.; Annaswamy, T.M.; Cassidy, R.C.; Cho, C.H.; Dougherty, P.; Easa, J.E.; Enix, D.E.; et al. Guideline summary review: An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 2015, 16, 439–448. [Google Scholar] [CrossRef]
- Treatment Guideline for Lumbar Spine Surgery. Washington State Department of Labor & Industries Surgical Guideline for Lumbar Spine–September 2021. Available online: https://www.lni.wa.gov/patient-care/advisory-committees/_docs/LumbarSpineSurgeryGuidelineSeptember2021FinalUpdate.pdf (accessed on 7 July 2022).
- Lewandrowski, K.-U. Retrospective analysis of accuracy and positive predictive value of preoperative lumbar MRI grading after successful outcome following outpatient endoscopic decompression for lumbar foraminal and lateral recess stenosis. Clin. Neurol. Neurosurg. 2019, 179, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Weber, H. Lumbar disc herniation. A controlled, prospective study with ten years of observation. Spine 1983, 8, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Atlas, S.J.; Keller, R.B.; Wu, Y.A.; Deyo, R.A.; Singer, D.E. Long-Term Outcomes of Surgical and Nonsurgical Management of Lumbar Spinal Stenosis: 8 to 10 Year Results from the Maine Lumbar Spine Study. Spine 2005, 30, 936–943. [Google Scholar] [CrossRef]
- Atlas, S.J.; Keller, R.B.; Chang, Y.; Deyo, R.A.; Singer, D.E. Surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: Five-year outcomes from the Maine Lumbar Spine Study. Spine 2001, 26, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Atlas, S.J.; Keller, R.B.; Robson, D.; Deyo, R.A.; Singer, D.E. Surgical and nonsurgical management of lumbar spinal stenosis: Four-year outcomes from the maine lumbar spine study. Spine 2000, 25, 556–562. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Lurie, J.D.; Tosteson, T.D.; Skinner, J.S.; Hanscom, B.; Tosteson, A.N.; Herkowitz, H.H.; Fischgrund, J.; Cammisa, F.P.; Albert, T.; et al. Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006, 296, 2451–2459. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Lurie, J.D.; Tosteson, T.D.; Hanscom, B.; Tosteson, A.N.; Blood, E.A.; Birkmeyer, N.J.; Hilibrand, A.S.; Herkowitz, H.; Cammisa, F.P.; et al. Surgical versus Nonsurgical Treatment for Lumbar Degenerative Spondylolisthesis. New Engl. J. Med. 2007, 356, 2257–2270. [Google Scholar] [CrossRef]
- Tosteson, A.N.; Lurie, J.D.; Tosteson, T.D.; Skinner, J.S.; Herkowitz, H.; Albert, T.; Boden, S.D.; Bridwell, K.; Longley, M.; Andersson, G.B.; et al. Surgical treatment of spinal stenosis with and without degenerative spondylolisthesis: Cost-effectiveness after 2 years. Ann. Intern. Med. 2008, 149, 845–853. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Lurie, J.D.; Tosteson, T.D.; Tosteson, A.N.; Blood, E.A.; Abdu, W.A.; Herkowitz, H.H.; Hilibrand, A.; Albert, T.; Fischgrund, J. Surgical versus nonoperative treatment for lumbar disc herniation: Four-year results for the Spine Patient Outcomes Research Trial (SPORT). Spine 2008, 33, 2789–2800. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Tosteson, T.D.; Lurie, J.D.; Tosteson, A.N.; Blood, E.; Hanscom, B.; Herkowitz, H.; Cammisa, F.; Albert, T.; Boden, S.D.; et al. Surgical versus Nonsurgical Therapy for Lumbar Spinal Stenosis. New Engl. J. Med. 2008, 358, 794–810. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Tosteson, T.D.; Lurie, J.D.; Tosteson, A.; Blood, E.; Herkowitz, H.; Cammisa, F.; Albert, T.; Boden, S.D.; Hilibrand, A.; et al. Surgical Versus Nonoperative Treatment for Lumbar Spinal Stenosis Four-Year Results of the Spine Patient Outcomes Research Trial. Spine 2010, 35, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- Shvartzman, L.; Weingarten, E.; Sherry, H.; Levin, S.; Persaud, A. Cost-Effectiveness Analysis of Extended Conservative Therapy Versus Surgical Intervention in the Management of Herniated Lumbar Intervertebral Disc. Spine 1992, 17, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Hout, W.B.V.D.; Peul, W.C.; Koes, B.; Brand, R.; Kievit, J.; Thomeer, R.T.W.M.; for the Leiden-The Hague Spine Intervention Prognostic Study Group. Prolonged conservative care versus early surgery in patients with sciatica from lumbar disc herniation: Cost utility analysis alongside a randomised controlled trial. BMJ 2008, 336, 1351–1354. [Google Scholar] [CrossRef] [PubMed]
- Aichmair, A.; LSOS Study Group; Burgstaller, J.M.; Schwenkglenks, M.; Steurer, J.; Porchet, F.; Brunner, F.; Farshad, M. Cost-effectiveness of conservative versus surgical treatment strategies of lumbar spinal stenosis in the Swiss setting: Analysis of the prospective multicenter Lumbar Stenosis Outcome Study (LSOS). Eur. Spine J. 2016, 26, 501–509. [Google Scholar] [CrossRef]
- Selva-Sevilla, C.; Ferrara, P.; Gerónimo-Pardo, M. Cost-utility Analysis for Recurrent Lumbar Disc Herniation: Conservative Treatment Versus Discectomy Versus Discectomy With Fusion. Clin. Spine Surg. 2019, 32, E228–E234. [Google Scholar] [CrossRef]
- Lewandrowski, K.-U.; Abraham, I.; León, J.F.R.; Telfeian, A.E.; Lorio, M.P.; Hellinger, S.; Knight, M.; De Carvalho, P.S.T.; Ramos, M.R.F.; Dowling, Á.; et al. A Proposed Personalized Spine Care Protocol (SpineScreen) to Treat Visualized Pain Generators: An Illustrative Study Comparing Clinical Outcomes and Postoperative Reoperations between Targeted Endoscopic Lumbar Decompression Surgery, Minimally Invasive TLIF and Open Laminectomy. J. Pers. Med. 2022, 12, 1065. [Google Scholar] [CrossRef]
- Yeung, A.; Roberts, A.; Zhu, L.; Qi, L.; Zhang, J.; Lewandrowski, K.-U. Treatment of Soft Tissue and Bony Spinal Stenosis by a Visualized Endoscopic Transforaminal Technique Under Local Anesthesia. Neurospine 2019, 16, 52–62. [Google Scholar] [CrossRef]
- Khalil, J.G.; Smuck, M.; Koreckij, T.; Keel, J.; Beall, D.; Goodman, B.; Kalapos, P.; Nguyen, D.; Garfin, S. A prospective, randomized, multicenter study of intraosseous basivertebral nerve ablation for the treatment of chronic low back pain. Spine J. 2019, 19, 1620–1632. [Google Scholar] [CrossRef]
- Määttä, J.H.; Wadge, S.; MacGregor, A.; Karppinen, J.; Williams, F.M. ISSLS Prize Winner: Vertebral Endplate (Modic) Change is an Independent Risk Factor for Episodes of Severe and Disabling Low Back Pain. Spine 2015, 40, 1187–1193. [Google Scholar] [CrossRef]
- Mayer, H.M. Discogenic low back pain and degenerative lumbar spinal stenosis—How appropriate is surgical treatment? Der Schmerz 2001, 15, 484–491. [Google Scholar] [CrossRef]
- Nguyen, C.; Poiraudeau, S.; Rannou, F. From Modic 1 vertebral-endplate subchondral bone signal changes detected by MRI to the concept of ‘active discopathy’. Ann. Rheum. Dis. 2015, 74, 1488–1494. [Google Scholar] [CrossRef] [PubMed]
- Rahme, R.; Moussa, R. The Modic Vertebral Endplate and Marrow Changes: Pathologic Significance and Relation to Low Back Pain and Segmental Instability of the Lumbar Spine. Am. J. Neuroradiol. 2008, 29, 838–842. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.T.; Gore, S. In-vivo Endoscopic Visualization of Patho-anatomy in Symptomatic Degenerative Conditions of the Lumbar Spine II: Intradiscal, Foraminal, and Central Canal Decompression. Surg. Technol. Online 2011, 21. [Google Scholar]
- Bechara, B.P.; Agarwal, V.; Boardman, J.; Perera, S.; Weiner, D.K.; Vo, N.; Kang, J.; Sowa, G.A. Correlation of Pain With Objective Quantification of Magnetic Resonance Images in Older Adults With Chronic Low Back Pain. Spine 2014, 39, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Dowling, Á.; Lewandrowski, K.-U.; da Silva, F.H.P.; Parra, J.A.A.; Portillo, D.M.; Giménez, Y.C.P. Patient selection protocols for endoscopic transforaminal, interlaminar, and translaminar decompression of lumbar spinal stenosis. J. Spine Surg. 2020, 6, S120–S132. [Google Scholar] [CrossRef] [PubMed]
- Lewandrowski, K.-U.; Yeung, A. Lumbar Endoscopic Bony and Soft Tissue Decompression With the Hybridized Inside-Out Approach: A Review And Technical Note. Neurospine 2020, 17, S34–S43. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.; Lewandrowski, K.-U. Early and staged endoscopic management of common pain generators in the spine. J. Spine Surg. 2020, 6, S1–S5. [Google Scholar] [CrossRef] [PubMed]
- Menendez, J.Y.; Omar, N.B.; Chagoya, G.; Tabibian, B.E.; Elsayed, G.A.; Walters, B.C.; Guthrie, B.L.; Hadley, M.N. Patient Satisfaction in Spine Surgery: A Systematic Review of the Literature. Asian Spine J. 2019, 13, 1047–1057. [Google Scholar] [CrossRef]
- Li, Z.-Z.; Hou, S.-X.; Shang, W.-L.; Song, K.-R.; Wu, W.-W. Evaluation of endoscopic dorsal ramus rhizotomy in managing facetogenic chronic low back pain. Clin. Neurol. Neurosurg. 2014, 126, 11–17. [Google Scholar] [CrossRef]
- Yeung, A.; Gore, S. Endoscopically Guided Foraminal and Dorsal Rhizotomy for Chronic Axial Back Pain Based on Cadaver and Endoscopically Visualized Anatomic Study. Int. J. Spine Surg. 2014, 8, 23. [Google Scholar] [CrossRef]
- Walter, S.G.; Schildberg, F.A.; Rommelspacher, Y. Endoscopic Sacrolumbar Facet Joint Denervation in Osteoarthritic and Degenerated Zygapophyseal Joints. Arthrosc. Tech. 2018, 7, e1275–e1279. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Ding, T.; Wang, D.; Zhao, J.; Yang, H.; Gu, X.; Feng, D.; Zhang, Y.; Liu, H.; Tang, F.; et al. Endoscopic rhizotomy for chronic lumbar zygapophysial joint pain. J. Orthop. Surg. Res. 2020, 15, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tieber, F.; Lewandrowski, K.-U. Technology advancements in spinal endoscopy for staged management of painful spine conditions. J. Spine Surg. 2020, 6, S19–S28. [Google Scholar] [CrossRef] [PubMed]
- Lewandrowski, K.-U. Incidence, Management, and Cost of Complications After Transforaminal Endoscopic Decompression Surgery for Lumbar Foraminal and Lateral Recess Stenosis: A Value Proposition for Outpatient Ambulatory Surgery. Int. J. Spine Surg. 2019, 13, 53–67. [Google Scholar] [CrossRef]
- Selby, D.K. When to Operate and What to Operate Upon. Orthop. Clin. North Am. 1983, 14, 577–588. [Google Scholar] [CrossRef]
- Sengupta, D.K.; Herkowitz, H.N. Lumbar spinal stenosis. Treatment strategies and indications for surgery. Orthop. Clin. N. Am. 2003, 34, 281–295. [Google Scholar] [CrossRef]
- Kurra, S.; Lavelle, W.F.; Silverstein, M.P.; Savage, J.W.; Orr, R.D. Long-term outcomes of transforaminal lumbar interbody fusion in patients with spinal stenosis and degenerative scoliosis. Spine J. 2018, 18, 1014–1021. [Google Scholar] [CrossRef]
- Lewandrowski, K.-U.; Dowling, Á.; de Carvalho, P.S.T.; Calderaro, A.L.; dos Santos, T.S.; Silva, M.S.D.L.E.; León, J.F.R.; Yeung, A. Indication and Contraindication of Endoscopic Transforaminal Lumbar Decompression. World Neurosurg. 2020, 145, 631–642. [Google Scholar] [CrossRef]
- Lohre, R.; Wang, J.C.; Lewandrowski, K.-U.; Goel, D.P. Virtual reality in spinal endoscopy: A paradigm shift in education to support spine surgeons. J. Spine Surg. 2020, 6, S208–S223. [Google Scholar] [CrossRef]
- Pan, M.; Li, Q.; Li, S.; Mao, H.; Meng, B.; Zhou, F.; Yang, H. Percutaneous Endoscopic Lumbar Discectomy: Indications and Complications. Pain Physician 2020, 23, 49–56. [Google Scholar]
- Wagner, R.; Haefner, M. Indications and Contraindications of Full-Endoscopic Interlaminar Lumbar Decompression. World Neurosurg. 2020, 145, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, C.; Wang, J.; Chu, T.-W.; Li, C.-Q.; Zhang, Z.-F.; Zheng, W.-J. Minimally invasive strategies and options for far-lateral lumbar disc herniation. Chin. J. Traumatol. 2008, 11, 259–266. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| A Request May Be Appropriate for | If the Patient Has | AND the Diagnosis Is Supported by These Clinical Findings: | And This Has Been Done | ||
|---|---|---|---|---|---|
| Surgical Procedure | Condition or Diagnosis | Subjective | Objective | Imaging | Non-Operative Care |
| Lumbar Decompression including: Lumbar laminectomy, laminotomy, discectomy, microdiscectomy, foraminotomy, or far lateral decompression | Nerve Root Entrapment due to central/paracentral/foraminal/extra-foraminal herniated nucleus pulposus. | Sensory symptoms in dermatomal distribution including: Radiating pain, burning, numbness, tingling, or paresthesia. | Objective findings must include two or more of the following:
| CT-Myelogram or MRI (within 6 months of requested surgery) must corroborate subjective and objective findings with substantial disc herniation, resulting in one or more of the following on the nerve root:
| At least six weeks of non-operative care from the date of injury, unless substantial or progressive motor weakness is documented. Care may include:
|
| Lumbar Decompression including: Lumbar laminectomy, laminotomy, or discectomy | Central spinal stenosis, moderate or severe | Neurogenic claudication, defined as:
| Bilateral lower extremity pain or weakness with standing and walking. -If unilateral pain is present, hip or vascular pathology should be ruled out by exam. | MRI or CT-Myelogram (within 6 months of requested surgery) confirms subjective and objective findings of moderate or severe central spinal stenosis. In the case of discordant reading between surgeon and radiologist that is unresolvable following review, another independent radiologist review is required. | At least six weeks of non-operative care from the date of injury, unless substantial or progressive motor weakness is documented. Care may include:
|
| Endoscopically Visualized Pain Generator | MRI Negative | MRI Positive | Total: |
|---|---|---|---|
| Hypertrophied Ligamentum Flavum | 7 | 35 | 42 |
| 7.3% | 31.8% | 20.4% | |
| Contained Herniated Disc | 6 | 25 | 31 |
| 6.3% | 22.7% | 15.0% | |
| Hypertrophied Superior Articular Process | 3 | 24 | 27 |
| 3.1% | 21.8% | 13.1% | |
| Inflamed Disc With Toxic Annular Tear | 25 | 0 | 25 |
| 26.0% | 0.0% | 12.1% | |
| Extruded Herniated Disc | 5 | 19 | 24 |
| 5.2% | 17.3% | 11.7% | |
| Delaminated and Fissured Disc Tissue | 17 | 0 | 17 |
| 17.7% | 0.0% | 8.3% | |
| Intra-Annular Granulation Tissue | 9 | 0 | 9 |
| 9.4% | 0.0% | 4.4% | |
| Facet Cyst | 1 | 7 | 8 |
| 1.0% | 6.4% | 3.9% | |
| Hidden Shoulder Osteophyte | 7 | 0 | 7 |
| 7.3% | 0.0% | 3.4% | |
| Inflamed Nerve | 6 | 0 | 6 |
| 6.3% | 0.0% | 2.9% | |
| Tethered and Furcal Nerve Roots | 6 | 0 | 6 |
| 6.3% | 0.0% | 2.9% | |
| Contracted Foraminal Ligaments | 4 | 0 | 4 |
| 4.2% | 0.0% | 1.9% | |
| Total ELD Patients | 96 | 110 | 206 |
| 100.0% | 100.0% | 100.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewandrowski, K.-U.; Yeung, A.; Lorio, M.P.; Yang, H.; Ramírez León, J.F.; Sánchez, J.A.S.; Fiorelli, R.K.A.; Lim, K.T.; Moyano, J.; Dowling, Á.; et al. Personalized Interventional Surgery of the Lumbar Spine: A Perspective on Minimally Invasive and Neuroendoscopic Decompression for Spinal Stenosis. J. Pers. Med. 2023, 13, 710. https://doi.org/10.3390/jpm13050710
Lewandrowski K-U, Yeung A, Lorio MP, Yang H, Ramírez León JF, Sánchez JAS, Fiorelli RKA, Lim KT, Moyano J, Dowling Á, et al. Personalized Interventional Surgery of the Lumbar Spine: A Perspective on Minimally Invasive and Neuroendoscopic Decompression for Spinal Stenosis. Journal of Personalized Medicine. 2023; 13(5):710. https://doi.org/10.3390/jpm13050710
Chicago/Turabian StyleLewandrowski, Kai-Uwe, Anthony Yeung, Morgan P. Lorio, Huilin Yang, Jorge Felipe Ramírez León, José Antonio Soriano Sánchez, Rossano Kepler Alvim Fiorelli, Kang Taek Lim, Jaime Moyano, Álvaro Dowling, and et al. 2023. "Personalized Interventional Surgery of the Lumbar Spine: A Perspective on Minimally Invasive and Neuroendoscopic Decompression for Spinal Stenosis" Journal of Personalized Medicine 13, no. 5: 710. https://doi.org/10.3390/jpm13050710
APA StyleLewandrowski, K. -U., Yeung, A., Lorio, M. P., Yang, H., Ramírez León, J. F., Sánchez, J. A. S., Fiorelli, R. K. A., Lim, K. T., Moyano, J., Dowling, Á., Sea Aramayo, J. M., Park, J. -Y., Kim, H. -S., Zeng, J., Meng, B., Gómez, F. A., Ramirez, C., De Carvalho, P. S. T., Rodriguez Garcia, M., ... on behalf of Teams/Organizations/Institutions. (2023). Personalized Interventional Surgery of the Lumbar Spine: A Perspective on Minimally Invasive and Neuroendoscopic Decompression for Spinal Stenosis. Journal of Personalized Medicine, 13(5), 710. https://doi.org/10.3390/jpm13050710