

Robot-Assisted Radical Cystectomy with Modified Vesica Ileale Padovana (VIP) Neobladder Configuration Using a Hybrid Approach: Initial Experience
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
2.2. The Hybrid Approach for the NB Reconstruction
2.3. Creation of a Wallace Plate
2.4. Mobilization of the Ileum
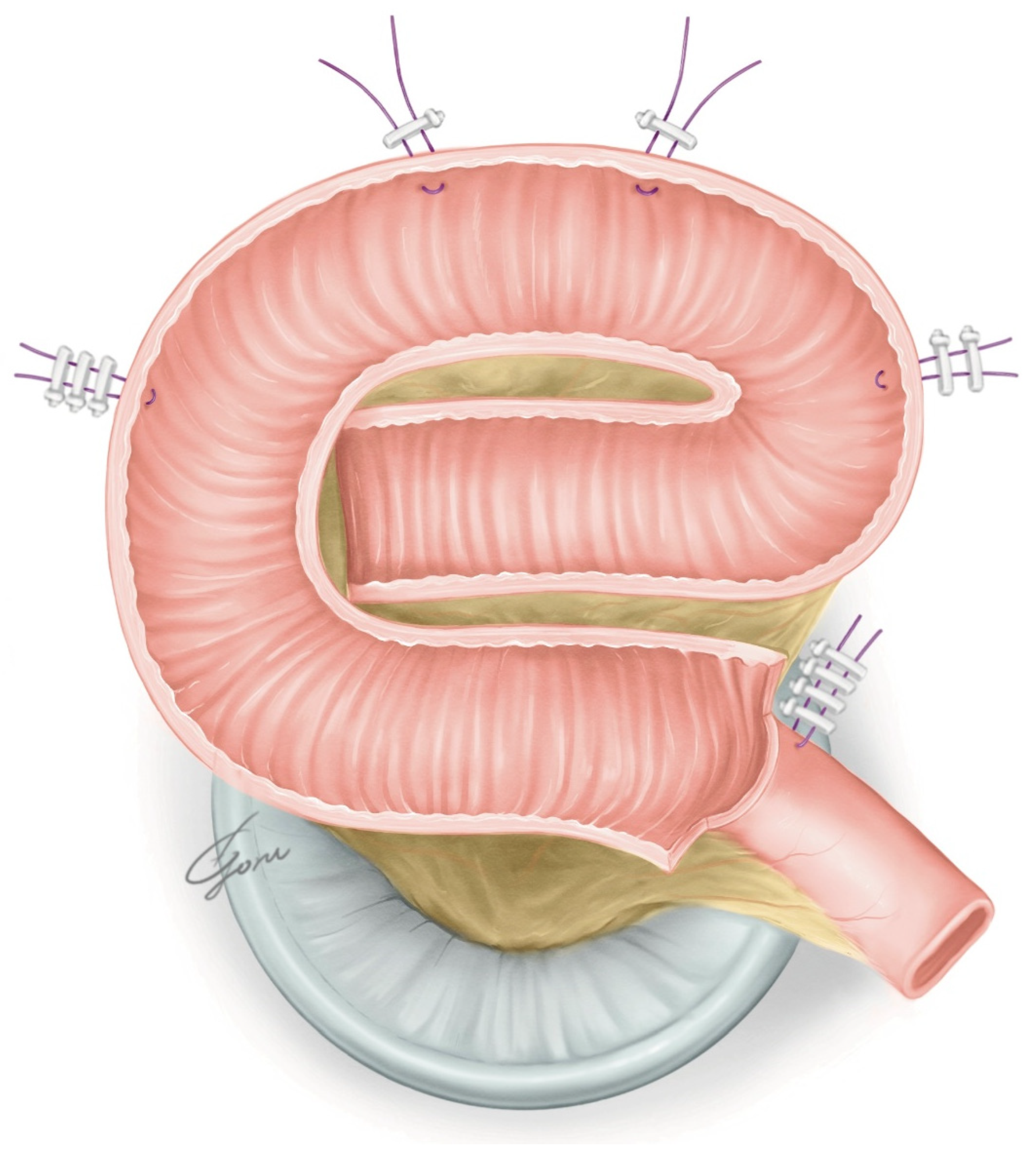
2.5. Extracorporeal Manipulation and Creation of the Posterior Plate
2.6. The Urethra–Ileal Anastomosis and Anterior Wall Closure
2.7. The Ureteric Afferent Limb Anastomosis
2.8. Postoperative Care
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ali, A.S.; Hayes, M.C.; Birch, B.; Dudderidge, T.; Somani, B.K. Health related quality of life (HRQoL) after cystectomy: Comparison between orthotopic neobladder and ileal conduit diversion. Eur. J. Surg. Oncol. 2015, 41, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Cerruto, M.A.; D’Elia, C.; Siracusano, S.; Gedeshi, X.; Mariotto, A.; Iafrate, M.; Niero, M.; Lonardi, C.; Bassi, P.; Belgrano, E.; et al. Systematic review and meta-analysis of non RCT’s on health related quality of life after radical cystectomy using validated questionnaires: Better results with orthotopic neobladder versus ileal conduit. Eur. J. Surg. Oncol. 2016, 42, 343–360. [Google Scholar] [CrossRef]
- Pyrha, L.N.; Raper, F.P. Some uses of an isolated loop of ileum in genito-urinary surgery. Br. J. Surg. 1955, 42, 337–357. [Google Scholar] [CrossRef]
- Colding-Jørgensen, M.; Poulsen, A.L.; Steven, K. Mechanical characteristics of tubular and detubularised bowel for bladder substitution: Theory, urodynamics and clinical results. Br. J. Urol. 1993, 72, 586–593. [Google Scholar] [CrossRef]
- Studer, U.E.; Turner, W.H. The ileal orthotopic bladder. Urology 1995, 45, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Hautmann, R.E. Orthotopic neobladder. In Textbook of Bladder Cancer; Lerner, S.P., Schoenberg, M.P., Sternberg, C.N., Eds.; Taylor & Francis: London, UK, 2006; pp. 581–593. [Google Scholar]
- Hussein, A.A.; May, P.R.; Jing, Z.; Ahmed, Y.E.; Wijburg, C.J.; Canda, A.E.; Dasgupta, P.; Shamim Khan, M.; Menon, M.; Peabody, J.O.; et al. Outcomes of Intracorporeal Urinary Diversion after Robot-Assisted Radical Cystectomy: Results from the International Robotic Cystectomy Consortium. J. Urol. 2018, 199, 1302–1311. [Google Scholar] [CrossRef]
- Pagano, F.; Artibani, W.; Ligato, P.; Piazza, R.; Garbeglio, A.; Passerini, G. Vescica ileale padovana: A technique for total bladder replacement. Eur. Urol. 1990, 17, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Masumori, N.; Fukuta, F. Development of combined method for construction of continent urinary diversion: Studer neobladder. Int. J. Urol. 2019, 26, 1158–1160. [Google Scholar] [CrossRef]
- Iwamoto, H.; Morizane, S.; Yamamoto, A.; Shimizu, R.; Nishikawa, R.; Yamaguchi, N.; Hikita, K.; Honda, M.; Takenaka, A. Utility of the HYBRID Method Incorporating the Advantages of Both Extracorporeal and Intracorporeal Urinary Diversion in Robotic-Assisted Radical Cystectomy. Yonago Acta Med. 2022, 65, 288–295. [Google Scholar] [CrossRef]
- Dalimov, Z.; Iqbal, U.; Jing, Z.; Wiklund, P.; Kaouk, J.; Kim, E.; Wijburg, C.; Wagner, A.A.; Roupret, M.; Dasgupta, P.; et al. Intracorporeal Versus Extracorporeal Neobladder After Robot-assisted Radical Cystectomy: Results From the International Robotic Cystectomy Consortium. Urology 2022, 159, 127–132. [Google Scholar] [CrossRef]
- Otaola-Arca, H.; Seetharam Bhat, K.R.; Patel, V.R.; Moschovas, M.C.; Orvieto, M. Totally intracorporeal robot-assisted urinary diversion for bladder cancer (part 2). Review and detailed characterization of the existing intracorporeal orthotopic ileal neobladder. Asian J. Urol. 2021, 8, 63–80. [Google Scholar] [CrossRef]
- Jonsson, M.N.; Adding, L.C.; Hosseini, A.; Schumacher, M.C.; Volz, D.; Nilsson, A.; Carlsson, S.; Wiklund, N.P. Robot-assisted radical cystectomy with intracorporeal urinary diversion in patients with transitional cell carcinoma of the bladder. Eur. Urol. 2011, 60, 1066–1073. [Google Scholar] [CrossRef]
- Benamran, D.; Phé, V.; Drouin, S.J.; Perrot, O.; Grégoris, A.; Parra, J.; Vaessen, C.; Seisen, T.; Rouprêt, M. Functional outcomes obtained with intracorporeal neobladder after robotic radical cystectomy for cancer: A narrative review. J. Robot. Surg. 2020, 14, 813–820. [Google Scholar] [CrossRef]
- Guru, K. Intracorporeal orthotopic neobladder: Est modus in rebus. Eur. Urol. Open Sci. 2021, 35, 16–17. [Google Scholar] [CrossRef]
- Lavallée, E.; Wiklund, P. The Studer Neobladder: An established and reproducible technique for intracorporeal urinary diversion. Eur. Urol. Open Sci. 2021, 35, 18–20. [Google Scholar] [CrossRef]
- Goh, A.C.; Gill, I.S.; Lee, D.J.; de Castro Abreu, A.L.; Fairey, A.S.; Leslie, S.; Berger, A.K.; Daneshmand, S.; Sotelo, R.; Gill, K.S.; et al. Robotic intracorporeal orthotopic ileal neobladder: Replicating open surgical principles. Eur. Urol. 2012, 62, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Chopra, S.; de Castro Abreu, A.L.; Berger, A.K.; Sehgal, S.; Gill, I.; Aron, M.; Desai, M.M. Evolution of robot-assisted orthotopic ileal neobladder formation: A step-by-step update to the University of Southern California (USC) technique. BJU Int. 2017, 119, 185–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hautmann, R.E.; Herr, H.W.; Pruthi, R.S.; Aron, M. Robotic radical cystectomy—Is the diversion the Achilles’ heel? J. Urol. 2014, 192, 1601–1603. [Google Scholar] [CrossRef]
- Tyritzis, S.I.; Hosseini, A.; Jonsson, M.; Adding, C.; Nilsson, A.; Wiklund, N.P. Robot-assisted intracorporeal formation of the ileal neobladder. J. Endourol. 2012, 26, 1570–1575. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.W.; Sooriakumaran, P.; Sanchez-Salas, R.; Ahonen, R.; Nyberg, T.; Wiklund, N.P.; Hosseini, A. Robot-assisted radical cystectomy with intracorporeal neobladder diversion: The Karolinska experience. Indian J. Urol. 2014, 30, 307–313. [Google Scholar] [PubMed]
- Schwentner, C.; Sim, A.; Balbay, M.D.; Todenhöfer, T.; Aufderklamm, S.; Halalsheh, O.; Mischinger, J.; Böttge, J.; Rausch, S.; Bier, S.; et al. Robot-assisted radical cystectomy and intracorporeal neobladder formation: On the way to a standardized procedure. World J. Surg. Oncol. 2015, 13, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canda, A.E.; Atmaca, A.F.; Altinova, S.; Akbulut, Z.; Balbay, M.D. Robot-assisted nerve-sparing radical cystectomy with bilateral extended pelvic lymph node dissection (PLND) and intracorporeal urinary diversion for bladder cancer: Initial experience in 27 cases. BJU Int. 2012, 110, 434–444. [Google Scholar] [CrossRef]
- Akbulut, Z.; Canda, A.E.; Ozcan, M.F.; Atmaca, A.F.; Ozdemir, A.T.; Balbay, M.D. Robot-assisted laparoscopic nerve-sparing radical cystoprostatectomy with bilateral extended lymph node dissection and intracorporeal Studer pouch construction: Outcomes of first 12 cases. J. Endourol. 2011, 25, 1469–1479. [Google Scholar] [CrossRef] [PubMed]
- Pruthi, R.S.; Nix, J.; McRackan, D.; Hickerson, A.; Nielsen, M.E.; Raynor, M.; Wallen, E.M. Robotic-assisted laparoscopic intracorporeal urinary diversion. Eur. Urol. 2010, 57, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Sim, A.; Todenhöfer, T.; Mischinger, J.; Halalsheh, O.; Fahmy, O.; Boettge, J.; Rausch, S.; Bier, S.; Aufderklamm, S.; Liatsikos, E.; et al. Y pouch neobladder-a simplified method of intracorporeal neobladder after robotic cystectomy. J. Endourol. 2015, 29, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Asimakopoulos, A.D.; Campagna, A.; Gakis, G.; Corona Montes, V.E.; Piechaud, T.; Hoepffner, J.L.; Mugnier, C.; Gaston, R. Nerve Sparing, Robot-Assisted Radical Cystectomy with Intracorporeal Bladder Substitution in the Male. J. Urol. 2016, 196, 1549–1557. [Google Scholar] [CrossRef] [PubMed]
- Koie, T.; Ohyama, C.; Yoneyama, T.; Nagasaka, H.; Yamamoto, H.; Imai, A.; Hatakeyama, S.; Hashimoto, Y. Robotic cross-folded U-configuration intracorporeal ileal neobladder for muscle-invasive bladder cancer: Initial experience and functional outcomes. Int. J. Med. Robot. 2018, 14, e1955. [Google Scholar] [CrossRef] [Green Version]
- Tan, W.S.; Sridhar, A.; Goldstraw, M.; Zacharakis, E.; Nathan, S.; Hines, J.; Cathcart, P.; Briggs, T.; Kelly, J.D. Robot-assisted intracorporeal pyramid neobladder. BJU Int. 2015, 116, 771–779. [Google Scholar] [CrossRef]
- Butt, Z.A.; Forbes, E.; Zorn, J.; Martin, B. Robotic radical cystectomy with intracorporeal neobladder: Initial experience and outcomes. Can. Urol. Assoc. J. 2015, 9, E156–E159. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Zheng, J.; He, P.; Zhang, J.; Wang, C.; Zheng, J.; Li, X.; Lang, L.; Zhou, Z.; Chen, Z. Refinement surgical technique, and perioperative and functional outcomes in patients with robotic intracorporeal Hautmann orthotopic neobladder. Urology 2020, 138, 45–51. [Google Scholar] [CrossRef]
- Whelan, P.; Tan, W.P.; Papagiannopoulos, D.; Omotosho, P.; Deane, L. Robotic assisted laparoscopic radical cystectomy with stentless intracorporeal modified Ves.Pa neobladder: Early experience. J. Robot. Surg. 2017, 11, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Dal Moro, F.; Zattoni, F. Ves.Pa.-designing a novel robotic intracorporeal orthotopic ileal neobladder. Urology 2016, 91, 99–103. [Google Scholar] [CrossRef]
- Simone, G.; Papalia, R.; Misuraca, L.; Tuderti, G.; Minisola, F.; Ferriero, M.; Vallat, G.; Guaglianone, S.; Gallucci, M. Robotic intracorporeal Padua ileal bladder: Surgical technique, perioperative, oncologic and functional outcomes. Eur. Urol. 2018, 73, 934–940. [Google Scholar] [CrossRef]
- Pyun, J.H.; Kim, H.K.; Cho, S.; Kang, S.G.; Cheon, J.; Lee, J.G.; Kim, J.J.; Kang, S.H. Robot-assisted radical cystectomy with total intracorporeal urinary diversion: Comparative analysis with extracorporeal urinary diversion. J. Laparoendosc. Adv. Surg. Tech. 2016, 26, 349–355. [Google Scholar] [CrossRef]
- Kang, S.G.; Ko, Y.H.; Jang, H.A.; Kim, J.; Kim, S.H.; Cheon, J.; Kang, S.H. Initial experience of robot-assisted radical cystectomy with total intracorporeal urinary diversion: Comparison with extracorporeal method. Laparoendosc. Adv. Surg. Tech. 2012, 22, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Christoph, F.; Herrmann, F.; Werthemann, P.; Janik, T.; Schostak, M.; Klopf, C.; Weikert, S. Ureteroenteric strictures: A single center experience comparing Bricker versus Wallace ureteroileal anastomosis in patients after urinary diversion for bladder cancer. BMC Urol. 2019, 19, 100. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.G.; Guru, K.; Wiklund, P.; Catto, J.; Yuh, B.; Novara, G.; Murphy, D.G.; Al-Tartir, T.; Collins, J.W.; Zhumkhawala, A.; et al. Robot-assisted radical cystectomy and urinary diversion: Technical recommendations from the Pasadena Consensus Panel. Eur. Urol. 2015, 67, 423–431. [Google Scholar] [CrossRef]
- Yanagisawa, T.; Miki, J.; Enei, Y.; Obayashi, K.; Kimura, T.; Egawa, S. Novel “double-pulling” technique for neobladder-urethral anastomosis in laparoscopic radical cystectomy. Int. J. Urol. 2020, 27, 822–823. [Google Scholar] [CrossRef]
- Hautmann, R.E.; Abol-Enein, H.; Davidsson, T.; Gudjonsson, S.; Hautmann, S.H.; Holm, H.V.; Lee, C.T.; Liedberg, F.; Madersbacher, S.M.; Mansson, W.; et al. International consultation on urologic disease-European Association of Urology Consultation on bladder cancer 2012. ICUD-EAU International Consultation on Bladder Cancer 2012: Urinary diversion. Eur. Urol. 2013, 63, 67–80. [Google Scholar] [CrossRef]
- Cacciamani, G.E.; Rajarubendra, N.; Artibani, W.; Gill, I.S. Robotic intracorporeal urinary diversion: State of the art. Curr. Opin. Urol. 2019, 29, 293–300. [Google Scholar] [CrossRef]
- Goldberg, H.; Baniel, J.; Mano, R.; Gillon, G.; Kedar, D.; Yossepowitch, O. Low-dose oral desmopressin for treatment of nocturia and nocturnal enuresis in patients after radical cystectomy and orthotopic urinary diversion. BJU Int. 2014, 114, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Satkunasivam, R.; Santomauro, M.; Chopra, S.; Plotner, E.; Cai, J.; Miranda, G.; Salibian, S.; Aron, M.; Ginsberg, D.; Daneshmand, S.; et al. Robotic intracorporeal orthotopic neobladder: Urodymnamic outcomes, urinary function, and health-related Quality of life. Euro. Urol. 2016, 69, 247–253. [Google Scholar] [CrossRef]
- Di Maida, F.; Grosso, A.A.; Tasso, G.; Gemma, L.; Lambertini, L.; Nardoni, S.; Mari, A.; Tuccio, A.; Vittori, G.; Masieri, L.; et al. Robot assisted radical cystectomy with Florence Robotic Intracorporeal neobladder (FloRIN): Functional ando urodynamic features compared with a contemporary series of open Vescica Ileale Padovana (VIP). Eur. J. Surg. Oncol. 2022, 48, 1854–1861. [Google Scholar] [CrossRef]
- Cheng, Q.; Gu, L.; Chen, W.; Zhao, X.; Ma, X.; Chang, X.; Ai, Q.; Li, H. Nerve-spring technique could achieve a functional trifecta outcome of robotic intracorporeal studer’s orthotopic neobladder in the male. Bladder 2022, 9, e50. [Google Scholar] [CrossRef]
- Furrer, M.A.; Kiss, B.; Studer, U.E.; Wuethrich, P.Y.; Gahl, B.; Seiler, R.; Roth, B.; Bosshard, P.; Thomas, B.C.; Burkhard, F.C.; et al. Seminal Vesical Sparing Cystectomy for Bladder Cancer is Feasible with Good Functional Results without Impairing Oncological Outcomes: A Longitudinal Long-Term Propensity-Matched Single Center Study. J. Urol. 2021, 205, 1629–1640. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Yang, J.; Gao, M.; Liu, H.; Li, J.; Hu, J.; Zhang, Y.; Zhong, G.; Li, K.; Dong, W.; et al. Pelvic reconstruction and lateral prostate capsule sparing techniques improve early continence of robot-assisted radical cystectomy with orthotopic ileal neobladder. Int. Urol. Nephrol. 2022, 54, 1537–1543. [Google Scholar] [CrossRef]
- Catto, J.W.F.; Khetrapal, P.; Ricciardi, F.; Ambler, G.; Williams, N.R.; Al-Hammouri, T.; Khan, M.S.; Thurairaja, R.; Nair, R.; Feber, A.; et al. iROC Study Team. Effect of Robot-Assisted Radical Cystectomy With Intracorporeal Urinary Diversion vs. Open Radical Cystectomy on 90-Day Morbidity and Mortality Among Patients With Bladder Cancer: A Randomized Clinical Trial. JAMA 2022, 327, 2092–2103. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.; Khan, S.A.; Hayn, M.H.; Agarwal, P.K.; Badani, K.K.; Balbay, M.D.; Castle, E.P.; Dasgupta, P.; Ghavamian, R.; Guru, K.A.; et al. Analysis of intracorporeal compared with extracorporeal urinary diversion after robot-assisted radical cystectomy: Results from the International Robotic Cystectomy Consortium. Eur. Urol. 2014, 65, 340–347. [Google Scholar] [CrossRef]
- Anceschi, U.; Brassetti, A.; Tuderti, G.; Ferriero, M.C.; Costantini, M.; Bove, A.M.; Calabrò, F.; Carlini, P.; Vari, S.; Mastroianni, R.; et al. Impact of Clinical Response to Neoadjuvant Chemotherapy in the Era of Robot Assisted Radical Cystectomy: Results of a Single-Center Experience. J. Clin. Med. 2020, 24, 2736. [Google Scholar] [CrossRef]
- Prata, F.; Anceschi, U.; Taffon, C.; Rossi, S.M.; Verri, M.; Iannuzzi, A.; Ragusa, A.; Esperto, F.; Prata, S.M.; Crescenzi, A.; et al. Real-Time Urethral and Ureteral Assessment during Radical Cystectomy Using Ex-Vivo Optical Imaging: A Novel Technique for the Evaluation of Fresh Unfixed Surgical Margins. Curr. Oncol. 2023, 30, 3421–3431. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Gender, n (%) | |
| Male | 10 (100) |
| Female | 0 (0) |
| Median age, year (range) | 66 (60–70) |
| Clinical T stage, n (%) | |
| CIS | 1 (10.0) |
| Ta | 0 (0) |
| T1 | 1 (10.0) |
| T2 | 5 (50.0) |
| ≥T3 | 3 (30.0) |
| Neoadjuvant chemotherapy use, n (%) | 9 (90.0) |
| RC histology, n (%) | |
| pT0 | 2 (20.0) |
| CIS | 1 (10.0) |
| pTa | 0 (0) |
| pT1 | 2 (20.0) |
| pT2 | 2 (20.0) |
| ≥pT3 | 3 (30.0) |
| Complications | Incidence, n (%) |
|---|---|
| Short-term complications | |
| Surgical | |
| Neobladder leakage | 1 (10) |
| Gastrointestinal | |
| Ileus | 1 (10) |
| Diarrhea/vomiting | 2 (20) |
| Vitamin B12 deficiency | 1 (10) |
| Infection | |
| Urinary tract infection | 1 (10) |
| Long-term complications | |
| Daytime incontinence | 1 (10) |
| Nighttime incontinence | 2 (20) |
| Readmission due to complications | 0 (0) |
| Grade of Clavien system complications | |
| Minor (Grade I–II) | 9 |
| Major (≧Grade III) | 0 |
| Institution | University of Southern California, USA | Karolinska, Sweden | Ankara, Turkey | North Carolina University, USA | Eberhard-Karls University, Germany | Saint-Augustin, France | Hirosaki University, Japan | London University, UK | Queen Elizabeth II, Canada | Third Military Medical University, China | Rush University, USA | Padova University, Italy | Regina Elena, Italy | Korea University, Korea | Sapporo Medical University, Japan | Juntendo University, Japan |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Goh et al. [17] Chopra et al. [18] | Jonsson et al. [13], Tyritzis et al. [20], Collins et al. [21] | Schwentner et al. [22], canda et al. [23], Akubulut et al. [24] | Pruthi et al. [25] | Sim et al. [26] | Asimakopoulos et al. [27] | Koie et al. [28] | Tan et al. [29] | Butt et al. [30] | Zhou et al. [31] | Whelan et al. [32] | Dal Moro et al. [33] | Simone et al. [34] | Pyun et al. [35] Kang et al. [36] | Masumori et al. [9] | Our series |
| n | 8 | 36 70 86 | 62 23 - | 3 | 73 | 40 | 22 | 20 | 4 | 40 | 2 | - | 45 | - | - | 10 |
| Length of ileum used, cm | 60 | 50 | 50 | N/A | 40 | 40 | 40 | 50 | 65 | 40 | 45 | 45 | 42 | 60 | 55 | 55 |
| Detubularization, cm | 44 | 40 | 40 | N/A | 28 | N/A | 40 | 50 | N/A | 40 | 45 | 40 | 42 | 60 | 40 | 45 |
| Afferent limb, cm | Yes, 11 | Yes,10 | Yes, 10 | No | Yes, 6 × 2 | No | No | No | Yes, N/A | No | No | No | No | No | Yes,15 | Yes,10 |
| Timing of the urethro-ileal anastomosis | After posterior plate reconstruction | Start of the reconstruction (before detuburiztion) | Start of the reconstruction (before detuburiztion) | After pouch completion | Start of the reconstruction (before detuburiztion) | Start of the reconstruction (before detuburiztion) | Start of the reconstruction (after detuburiztion) | After pouch completion | After pouch completion | Start of the reconstruction(before detuburiztion) | Start of the reconstruction (before detuburiztion) | Start of the reconstruction (after detuburiztion) | After posterior plate reconstruction | Start of the reconstruction (before detuburiztion) | After posterior plate reconstruction | After posterior plate reconstruction |
| Method of the urethro-ileal anastomosis | Circumferential | Opening | Opening | Opening | Opening | Opening | Opening | Opening | Opening | Opening | Opening | Opening | Opening | Opening | Circumferential | Circumferential |
| Uretero-enteric anastomosis | Bricker | Wallace | Wallace | Bricker | Bricker | Wallace | Split nipple technique | Bricker | Bricker | Bricker | Bricker | Bricker | Split nipple technique | Bricker | Bricker | Wallace |
| Direction to fold | Bilateral sides to center | Diagonally downward | Diagonally upward | N/A | Single folding, Bilateral sides to center | Top to bottom | Top to bottom | Up down left right to center | Bilateral sides to center | Bilateral sides to center | Top to bottom | Top to bottom | Top to bottom | Single folding, Bilateral sides to center | Diagonally upward | Bilateral sides to center |
| Ureteral stenting insertion | Percutaneous, internalized | Per urethra/Percutaneous, internalized/Percutaneous externalized | Percutaneous externalized/Per urethra | Per urethra | Percutaneous internalized | Per urethra | Percutaneous internalized | Percutaneous externalized | Percutaneous internalized | N/A | None | None | Percutaneous internalized | Percutaneous internalized | Percutaneous externalized | Percutaneous externalized/Percutaneous internalized |
| Shape | Modified Studer | Modified Studer | Modified Studer | U | Y | Y (similar to Cross-folded U) | Cross-folded U | Pyramid | Hautmann W | Hautmann W | Ves.Pa | Ves.Pa | Modified VIP | Camey | Modified Studer | Modified VIP |
| Operative time, min, (range or SD) | 450 (420–780) | 480 (330–760) 420 (265–760) - | 476 (310–690) 594 - | 318 (258–696) | 442 (280–690) | 315 (172–400) | 430 (349–476) | 150 (120–360) | 523 (75) | 320 (230–500) | 543 | - | 305 (282–345) | 649 | - | 496 (418–615) |
| Estimated blood loss, mL, (range or SD) | 225 (100–700) | 625 (200–2200) 500 (100–2200) - | 385 (200–800) 430 - | 221 (50–400) | 347 (50–800) | 395 (0–700) | 300 (119–450) | 260 (100–500) | 238 (48) | 300 (100–2000) | 225 | - | 210 (50–250) | 148 | - | 524 (110–850) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimizu, F.; Muto, S.; Kitamura, K.; China, T.; Shirakawa, T.; Kimura, T.; Ieda, T.; Nagata, M.; Isotani, S.; Nakagawa, Y.; et al. Robot-Assisted Radical Cystectomy with Modified Vesica Ileale Padovana (VIP) Neobladder Configuration Using a Hybrid Approach: Initial Experience. J. Pers. Med. 2023, 13, 802. https://doi.org/10.3390/jpm13050802
Shimizu F, Muto S, Kitamura K, China T, Shirakawa T, Kimura T, Ieda T, Nagata M, Isotani S, Nakagawa Y, et al. Robot-Assisted Radical Cystectomy with Modified Vesica Ileale Padovana (VIP) Neobladder Configuration Using a Hybrid Approach: Initial Experience. Journal of Personalized Medicine. 2023; 13(5):802. https://doi.org/10.3390/jpm13050802
Chicago/Turabian StyleShimizu, Fumitaka, Satoru Muto, Kosuke Kitamura, Toshiyuki China, Tomoya Shirakawa, Tomoki Kimura, Takeshi Ieda, Masayoshi Nagata, Shuji Isotani, Yuki Nakagawa, and et al. 2023. "Robot-Assisted Radical Cystectomy with Modified Vesica Ileale Padovana (VIP) Neobladder Configuration Using a Hybrid Approach: Initial Experience" Journal of Personalized Medicine 13, no. 5: 802. https://doi.org/10.3390/jpm13050802
APA StyleShimizu, F., Muto, S., Kitamura, K., China, T., Shirakawa, T., Kimura, T., Ieda, T., Nagata, M., Isotani, S., Nakagawa, Y., & Horie, S. (2023). Robot-Assisted Radical Cystectomy with Modified Vesica Ileale Padovana (VIP) Neobladder Configuration Using a Hybrid Approach: Initial Experience. Journal of Personalized Medicine, 13(5), 802. https://doi.org/10.3390/jpm13050802