
Predicting Hospital Ward Admission from the Emergency Department: A Systematic Review

Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
- Population: Patients presenting to the emergency department
- Intervention: prediction models for ward admissions in the hospital from emergency department patients
- Comparison: not applicable
- Outcome: patient admission
2.3. Data Extraction
- Predictive models for hospital readmission.
- Primary population of interest focused on specific conditions (e.g., asthma or bronchiolitis).
- The model predicts whether a patient will be admitted in the future or requires post-triage data.
- Only provided risk factors evaluation and did not build a prediction model.
- Models that do not answer the specific question, i.e.,do not predict ward admission from the emergency department.
- Published in languages other than English and Spanish.
- Full article not available.
2.4. Methodological Quality Assessment
3. Results
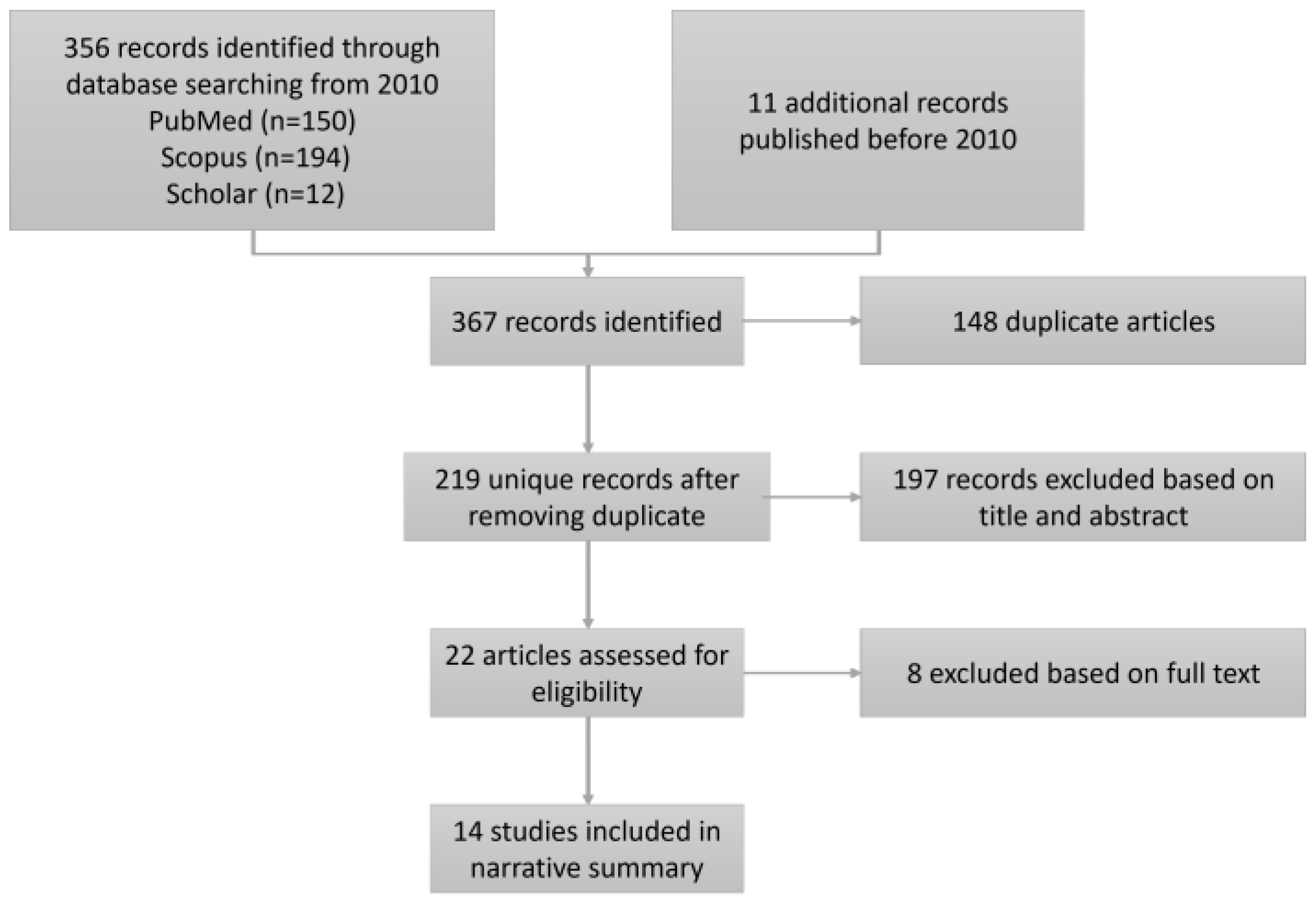
3.1. Study Identification
3.2. Description of Included Studies
3.3. Variables Used to Develop Predictive Models
3.4. Predictiveness of Models
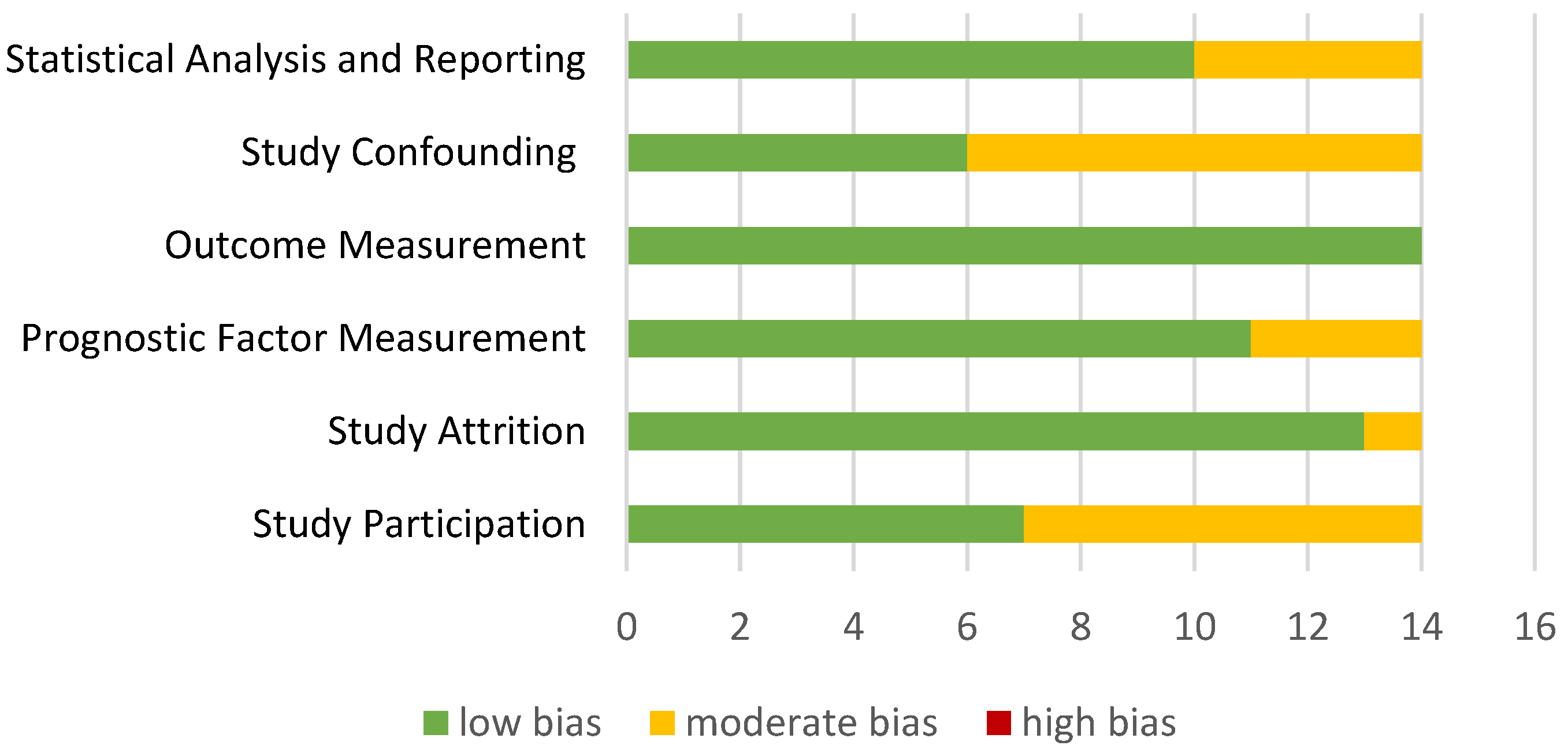
3.5. Methodological Quality Assessment
![Jpm 13 00849 i001]() : means low risk of bias
: means low risk of bias![Jpm 13 00849 i002]() : means moderate risk of bias
: means moderate risk of bias![Jpm 13 00849 i003]() : means high risk of bias
: means high risk of bias


{kind=link}
{kind=link}
| Reference | Study Participation | Study Attrition | Prognostic Factor | Outcome | Study Confounding | Statistical Analysis and Reporting | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|
| Parker et al. [16] |  | |  | | | | |
| Elvira Martínez et al. [17] | | | | | | | |
| De Hond, Anne et al. [18] | | | | | | | |
| Feretzakis, Georgios et al. [19] | | | | | | | |
| Hong, Woo Suk et al. [20] | | | | | | | |
| Graham, B et al. [21] | | | | | | | |
| Cusidó, J et al. [22] | | | | | | | |
| Alexander Zlotnik et al. [23] | | | | | | | |
| A. Brink et al. [24] | | | | | | | |
| Sun, Yan et al. [25] | | | | | | | |
| Feretzakis, Georgios et al. [26] | | | | | | | |
| Lucke, Jacinta A et al. [27] | | | | | | | |
| Allan Cameron et al. [28] | | | | | | | |
| Noel, Guilhem el al. [29] | | | | | | | |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Savioli, G.; Ceresa, I.F.; Gri, N.; Bavestrello Piccini, G.; Longhitano, Y.; Zanza, C.; Piccioni, A.; Esposito, C.; Ricevuti, G.; Bressan, M.A. Emergency Department Overcrowding: Understanding the Factors to Find Corresponding Solutions. J. Pers. Med. 2022, 12, 279. [Google Scholar] [CrossRef] [PubMed]
- Maninchedda, M.; Proia, A.S.; Bianco, L.; Aromatario, M.; Orsi, G.B.; Napoli, C. Main Features and Control Strategies to Reduce Overcrowding in Emergency Departments: A Systematic Review of the Literature. Risk Manag. Healthc. Policy 2023, 16, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Mueller, B.; Kinoshita, T.; Peebles, A.; Graber, M.A.; Lee, S. Artificial intelligence and machine learning in emergency medicine: A narrative review. Acute Med. Surg. 2022, 9, e740. [Google Scholar] [CrossRef] [PubMed]
- Briganti, G.; Le Moine, O. Artificial Intelligence in Medicine: Today and Tomorrow. Front. Med. 2020, 7, 27. [Google Scholar] [CrossRef]
- Brabrand, M.; Folkestad, L.; Clausen, N.G.; Knudsen, T.; Hallas, J. Risk scoring systems for adults admitted to the emergency department: A systematic review. Scand. J. Trauma Resusc. Emerg. Med. 2010, 18, 8. [Google Scholar] [CrossRef]
- Wallace, E.; Hinchey, T.; Dimitrov, B.D.; Bennett, K.; Fahey, T.; Smith, S.M. A Systematic Review of the Probability of Repeated Admission Score in Community-Dwelling Adults. J. Am. Geriatr. Soc. 2013, 61, 357–364. [Google Scholar] [CrossRef]
- Wallace, E.; Stuart, E.; Vaughan, N.; Bennett, K.; Fahey, T.; Smith, S.M. Risk Prediction Models to Predict Emergency Hospital Admission in Community-dwelling Adults. Med. Care 2014, 52, 751–765. [Google Scholar] [CrossRef]
- Jiang, S.; Liu, Q.; Ding, B. A systematic review of the modelling of patient arrivals in emergency departments. Quant. Imaging Med. Surg. 2023, 13, 1957–1971. [Google Scholar] [CrossRef]
- Monahan, A.C.; Feldman, S.S. Models predicting hospital admission of adult patients utilizing prehospital data: Systematic review using PROBAST and CHARMS. JMIR Med. Inform. 2021, 9, e30022. [Google Scholar] [CrossRef]
- Silva, E.; Pereira, M.F.; Vieira, J.T.; Ferreira-Coimbra, J.; Henriques, M.; Rodrigues, N.F. Predicting hospital emergency department visits accurately: A systematic review. Int. J. Health Plann. Manag. 2023, 1–14. [Google Scholar] [CrossRef]
- Brink, A.; Alsma, J.; van Attekum, L.A.; Bramer, W.M.; Zietse, R.; Lingsma, H.; Schuit, S.C. Predicting inhospital admission at the emergency department: A systematic review. Emerg. Med. J. 2022, 39, 191–198. [Google Scholar] [CrossRef]
- Sánchez-Salmerón, R.; Gómez-Urquiza, J.L.; Albendín-García, L.; Correa-Rodríguez, M.; Martos-Cabrera, M.B.; Velando-Soriano, A.; Suleiman-Martos, N. Machine learning methods applied to triage in emergency services: A systematic review. Int. Emerg. Nurs. 2022, 60, 101109. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. Available online: https://www.acpjournals.org/doi/10.7326/0003-4819-151-4-200908180-00135 (accessed on 14 April 2023). [CrossRef] [PubMed]
- Santos, C.M.d.C.; Pimenta, C.A.d.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing Bias in Studies of Prognostic Factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef]
- Parker, C.A.; Liu, N.; Wu, S.X.; Shen, Y.; Lam, S.S.W.; Ong, M.E.H. Predicting hospital admission at the emergency department triage: A novel prediction model. Am. J. Emerg. Med. 2019, 37, 1498–1504. [Google Scholar] [CrossRef]
- Martínez, C.M.E.; Fernández, C.; Del Castillo, J.G.; Armengol, J.J.G.; Villarroel, P.; Sánchez, F.J.M. Prediction model for in-hospital admission in patients arriving in the emergency department. An. Sist. Sanit. Navar. 2012, 35, 207–217. [Google Scholar] [CrossRef]
- De Hond, A.; Raven, W.; Schinkelshoek, L.; Gaakeer, M.; Ter Avest, E.; Sir, O.; Lameijer, H.; Hessels, R.A.; Reijnen, R.; De Jonge, E.; et al. Machine learning for developing a prediction model of hospital admission of emergency department patients: Hype or hope? Int. J. Med. Inform. 2021, 152, 104496. [Google Scholar] [CrossRef]
- Feretzakis, G.; Karlis, G.; Loupelis, E.; Kalles, D.; Chatzikyriakou, R.; Trakas, N.; Karakou, E.; Sakagianni, A.; Tzelves, L.; Petropoulou, S.; et al. Using Machine Learning Techniques to Predict Hospital Admission at the Emergency Department. J. Crit. Care Med. 2022, 8, 107–116. [Google Scholar] [CrossRef]
- Hong, W.S.; Haimovich, A.D.; Taylor, R.A. Predicting hospital admission at emergency department triage using machine learning. PLoS ONE 2018, 13, e0201016. [Google Scholar] [CrossRef]
- Graham, B.; Bond, R.; Quinn, M.; Mulvenna, M. Using Data Mining to Predict Hospital Admissions From the Emergency Department. IEEE Access 2018, 6, 10458–10469. [Google Scholar] [CrossRef]
- Cusidó, J.; Comalrena, J.; Alavi, H.; Llunas, L. Predicting Hospital Admissions to Reduce Crowding in the Emergency Departments. Appl. Sci. 2022, 12, 10764. [Google Scholar] [CrossRef]
- Zlotnik, A.; Alfaro, M.C.; Pérez, M.C.P.; Gallardo-Antolín, A.; Martínez, J.M.M. Building a Decision Support System for Inpatient Admission Prediction With the Manchester Triage System and Administrative Check-in Variables. CIN Comput. Inform. Nurs. 2016, 34, 224. [Google Scholar] [CrossRef] [PubMed]
- Brink, A.; Alsma, J.; Brink, H.S.; De Gelder, J.; Lucke, J.A.; Mooijaart, S.P.; Zietse, R.; Schuit, S.C.E.; Lingsma, H.F. Prediction admission in the older population in the Emergency Department: The CLEARED tool. Neth. J. Med. 2020, 78, 357–367. [Google Scholar]
- Sun, Y.; Heng, B.H.; Tay, S.Y.; Seow, E. Predicting hospital admissions at emergency department triage using routine administrative data. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2011, 18, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Feretzakis, G.; Sakagianni, A.; Loupelis, E.; Karlis, G.; Kalles, D.; Tzelves, L.; Chatzikyriakou, R.; Trakas, N.; Petropoulou, S.; Tika, A.; et al. Predicting Hospital Admission for Emergency Department Patients: A Machine Learning Approach. Stud. Health Technol. Inform. 2022, 289, 297–300. [Google Scholar] [CrossRef]
- Lucke, J.A.; de Gelder, J.; Clarijs, F.; Heringhaus, C.; de Craen, A.J.M.; Fogteloo, A.J.; Blauw, G.J.; de Groot, B.; Mooijaart, S.P. Early prediction of hospital admission for emergency department patients: A comparison between patients younger or older than 70 years. Emerg. Med. J. 2017, 35, 18–27. [Google Scholar] [CrossRef]
- Cameron, A.; Rodgers, K.; Ireland, A.; Jamdar, R.; McKay, G.A. A simple tool to predict admission at the time of triage. Emerg. Med. J. 2015, 32, 174–179. [Google Scholar] [CrossRef]
- Noel, G.; Bonte, N.; Persico, N.; Bar, C.; Luigi, S.; Roch, A.; Michelet, P.; Gentile, S.; Viudesa, G. Real-time estimation of inpatient beds required in emergency departments. Eur. J. Emerg. Med. 2019, 26, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Díaz, J.; Alberdi, J.C.; Pajares, M.S.; López, C.; López, R.; Lage, M.B.; Otero, A. A model for forecasting emergency hospital admissions: Effect of environmental variables. J. Environ. Health 2001, 64, 9–15. [Google Scholar]


| PICO Element | Keyword Terms |
|---|---|
| P Population | emergency patient, emergency patients |
| I Intervention(s) | predictive models, predict, predictive, predictable, prediction, predictions, Model, models, admission, hospital admission, predictive model emergency admission, Hospital admission predictive models, Hospital admission predictive model, predictive hospital admission |
| C Comparison(s) | - |
| O Outcome(s) | Hospital admission, emergency admission, Improve triage, QoL, emergency rooms management |
| Search String | Search Date | Results | |
|---|---|---|---|
| PubMed | ((admission [Title]) OR admissions [Title])) AND (emergency [Title]) AND ((predict [Title]) OR (predicting [Title]) OR (prediction [Title]) OR (triage [Title]) OR (model [Title])) NOT (COVID-19) | 16 January 2023 | 150 articles |
| Scopus | TITLE ((“admission” OR “admissions”) AND “emergency” AND (“predict” OR “predicting” OR “prediction” OR “triage “OR “model”)) AND NOT “COVID-19” AND PUBYEAR > 2009 AND PUBYEAR < 2023 AND (LIMIT-TO (PUBSTAGE,”final”)) AND (LIMIT-TO (SRCTYPE,”j”)) AND (LIMIT-TO (LANGUAGE,”English”) OR LIMIT-TO (LANGUAGE,”Spanish”)) | 16 January 2023 | 194 articles |
| Google scholar | allintitle: admission emergency hospital “machine learning” | 16 January 2023 | 12 articles |
| Others | - | 16 January 2023 | 11 articles |
| Autor | Title | Country Year | Purpose | Number of Data | Inclusion Criteria | Type of Data | Algorithm | Results |
|---|---|---|---|---|---|---|---|---|
| Parker, Clare Allison et al. [16] | Predicting hospital admission at the emergency department triage: A novel prediction model | USA – 2019 | create a model capable of predicting the hospital admission of a patient at the time of triage | 1,232,016 patients, 38.7% admitted | Emergency patients | Age group, race, zip code, day of week, time of day, triage category, mode of arrival and febrile status | Logistic regression | AUC validation: 0.825 [95% IC 0.824–0.827] |
| Elvira Martínez, C. M. et al. [17] | Prediction model for in-hospital admission in patients arriving in the emergency department | Spain – 2012 | Hospital admission prediction model for hospital bed determination | 2476 patients, of which 114 (4.6%) were admitted | Adult patients who were stable on arrival at the ED | Age, sex, triage level, initial disposition, first diagnosis, diagnostic test and medication | Logistic regression | AUC: 0.85 [95% IC 0.81–0.88; p < 0.001] Sensitivity: 76% Specificity: 82% |
| De Hond, Anne; Raven, Wouter et al. [18] | Machine learning for developing a prediction model of hospital admission of emergency department patients: Hype or hope? | Netherlands – 2021 | Early identification of emergency department patients in need of hospitalization | 172,104 patients, of whom 66,782 (39%) were hospitalized | Emergency patients | An increasing number of data available at triage, ∼30 min (including vital signs) and ∼2 h (including laboratory tests) | Gradient- powered decision tree modelling | AUC: 0.84 (0.77–0.88) at triage, 0.86 (0.82–0.89) at ∼30 min and 0.86 (0.74–0.93) after ∼2 h |
| Feretzakis, Georgios; Karlis, George; Loupelis, Evangelos et al. [19] | Using Machine Learning Techniques to Predict Hospital Admission at the Emergency Department | Greece – 2022 | Develop an algorithm using ML techniques to aid clinical decision making in the emergency department | 3204 patients, of which 1175 were admitted to the emergency room (36.7%) | Emergency patients | Laboratory data, age, sex, triage disposition to the emergency department and ambulance utilization | Random forest | AUC: 0.789 |
| Hong, Woo Suk; Haimovich, Adrian Daniel; Taylor at al. [20] | Predicting hospital admission at emergency department triage using machine learning | USA – 2018 | Predict hospital admission at the time of emergency department triage | 560,486 patients, 29.7% were admitted | Emergency patients | Three databases: 1—triage data; 2—medical history data; 3—triage and medical history data. | Gradient boosting (XGBoost) | AUC: 0.92 [IC 95% 0.92–0.93] |
| Graham, B.; Bond, R.; Quinn, M.; Mulvenna, M. [21] | Using Data Mining to Predict Hospital Admissions from the Emergency Department | U.K. – 2018 | Use of data mining using machine learning techniques to predict admissions to the emergency department | 120,600 patients | Emergency patients | Age, mode of arrival, triage, care group, previous admission, … | Gradient boosting machine (GBM) | AUC: 0.859 Accuracy: 80.31% |
| Cusidó, J.; Comalrena, J.; Alavi, H.; Llunas, L. [22] | Predicting Hospital Admissions to Reduce Crowding in the Emergency Departments | Spain – 2022 | Assisting in many areas of hospital administration | 3,189,204 patients, 11.02% of which ended in admission | Emergency patients | Identification, cumulative visits, age, days of age, gender, CCS (Clinical Classification System), CCS frequency, classification (triage) | Gradient boosting machine (GBM) | AUC: 0.8938 [IC 95% de 0.8929–0.8948] Accuracy: 0.9113 |
| Alexander Zlotnik, Miguel Cuchí Alfaro et al. [23] | Building a Decision Support System for Inpatient Admission Prediction with the Manchester Triage System and Administrative Check-in Variables | Spain – 2016 | Give nurses the ability to allocate resources in advance using predictive modelling | 255,668 patients | Emergency patients | Nine routinely collected variables routinely available right at the end of the triage process | Artificial neural network model | AUC: 0.8575 [IC 95 % 0.8540–0.8610] |
| A. Brink, J Alsma, H S Brink et al. [24] | Prediction admission in the older population in the Emergency Department: the CLEARED tool | Netherlands – 2020 | Develop and validate a clinical prediction tool for admission to the emergency department | 7606 patients | Emergency patients 70 years of age and older | Vital signs, the category of the Manchester triage system, and the need for laboratory or radiology tests | Logistic regression | AUC: 0.766 [IC 95% 0.759–0.781] |
| Sun, Yan; Heng, Bee Hoon; Tay, Seow Yian; Seow, Eillyne [25] | Predicting Hospital Admissions at Emergency Department Triage Using Routine Administrative Data | Singapore – 2011 | Be able to predict, at the time of triage, the need for hospital admission to the emergency department | 317,581 patients, of which 30.2% were admitted | Emergency patients | Demographics, ED visit or hospital admission in the previous 3 months, mode of arrival, patient acuity category (PAC) of emergency department visit and coexisting chronic diseases (diabetes, hypertension and dyslipidemia) | Logistic regression | AUC: 0.849 [IC 95% 0.847–0.851] |
| Feretzakis, Georgios; Sakagianni, Aikaterini et al. [26] | Predicting Hospital Admission for Emergency Department Patients: A Machine Learning Approach | Greece – 2022 | Establish a machine learning model and evaluate its predictive ability for hospital admission | 3204 patients | Emergency patients | Laboratory data, age, sex, use of ambulance (ambulance), triage disposition to the ED, and ED outcome (admission or discharge). (ambulance), triage disposition to ED | Gaussian NB | AUC: 0.806 |
| Lucke, Jacinta A.; de Gelder, Jelle; et al. [27] | Early prediction of hospital admission for emergency department patients: a comparison between patients younger or older than 70 years | Netherlands – 2018 | Develop models that predict hospital admissions to the emergency department | 10,807 patients | Two models, 1. over 70 2. less than 70 but greater than 18 | Age, sex, triage category, mode of arrival, blood test performed, chief complaint, ED visit, type of specialist, blood sample phlebotomized and vital signs | Multivariate logistic regression | AUC: <70 years: 0.86 [IC 95% 0.85 a 0.87] ≥70 years: 0.77 [IC 95% 0.75 a 0.79] |
| Allan Cameron, Kenneth Rodgers et al. [28] | A simple tool to predict admission at the time of triage | U.K. – 2015 | Create and validate a simple clinical score to estimate the probability of admission at the time of triage | 215,231 patients | Emergency patients | Triage category, age, National Early Warning Score (NEWS), ambulance arrival, referral source and admission within the last year | Mixed-effects multiple logistic model | AUC: 0.8774 [IC 95% 0.8752–0.8796] |
| Noel, Guilhem; Bonte, Nicolásd et al. [29] | Real-time estimation of inpatient beds required in emergency departments | France – 2019 | Develop a real-time automated model to predict admissions after triage | 11,653 patients, were 19.5–24.7% admitted | Emergency patients | Variables available in triage | Logistic regression | AUC: 0.815 [0.0–805.825] |
| Studys | Type of Variable | Variables | |
|---|---|---|---|
| Parker et al. [16] | Demographics | Age group, race | |
| Triage information | Day of week, time of day, triage category | ||
| Others | Zip code, febrile state, mode of arrival | ||
| Elvira Martínez et al. [17] | Demographics | Age, sex | |
| Triage information | Triage level, initial disposition | ||
| Clinical and laboratory findings | First diagnosis, diagnostic test | ||
| Medication | Medication | ||
| De Hond, Anne et al. [18] | Triage information | Data available at triage | |
| Clinical and laboratory findings | Vital signs, laboratory tests | ||
| Feretzakis, Georgios et al. [19] | Clinical and laboratory findings | Serum levels of urea, creatine, lactate dehydrogenase, creatine kinase, protein C-reactive, complete blood count with dialysis, paral acvated thromboplastin time, DDi-mer, Internonal normalized rao | |
| Demographics | Age, sex | ||
| Triage information | Triage disposition to the emergency department | ||
| Others | Ambulance utilization | ||
| Hong, Woo Suk et al. [20] | Clinical and laboratory findings | Clinical history data | |
| Triage information | Data from triage | ||
| Graham, B et al. [21] | Demographics | Age, gender | |
| Clinical and laboratory findings | Care group | ||
| Triage information | Manchester triage category | ||
| Medical history | Previous admission within the last week, month and year | ||
| Others | Mode of arrival to hospital | ||
| Cusidó, J et al. [22] | Demographics | Identification, age, days of age, gender | |
| Medical history | Cumulative visits | ||
| Triage information | Classification (triage), CCS (Clinical Classification System), CCS frequency | ||
| Alexander Zlotnik et al. [23] | Demographics | Age range, sex, insurance status | |
| Triage information | MTS score, MTS chief complaint group | ||
| Medical history | ED visits (preceding 12 month) | ||
| Clinical and laboratory findings | Visit source, visit cause | ||
| Others | Ambulance arrival | ||
| A. Brink et al. [24] | Triage information | Manchester’s triage system category | |
| Clinical and laboratory findings | Body temperature, heart rate, diastolic blood pressure, systolic blood pressure, oxygen saturation, respiratory rate, baseline status, the need for laboratory or radiology testing | ||
| Sun, Yan et al. [25] | Demographics | Age, gender and ethnicity | |
| Triage information | Patient acuity category (PAC) of emergency room visit | ||
| Medical history | ED visit or hospital admission in the previous 3 months | ||
| Others | Mode of arrival, coexisting chronic diseases (diabetes, hypertension and dyslipidemia) | ||
| Feretzakis, Georgios et al. [26] | Demographics | Age, sex | |
| Triage information | ED triage disposition | ||
| Clinical and laboratory findings | Serum levels of Urea (UREA), creatinine (CREA), lactate dehydrogenase (LDH), creatine kinase (CPK), C-reactive protein (CRP), complete blood count with differential, including leukocytes, white blood cells (WBC) and white blood cells (WBC), neutrophil count (NEUT%), lymphocyte count (LYM%), hemoglobin (HGB) and platelets (PLT), activated partial thromboplastin time (aPTT), thrombocyte (aPTT), D-dimer, international normalized ratio (INR) | ||
| Others | Ambulance use (ambulance) | ||
| Lucke, Jacinta A et al. [27] | <70 years | Demographics | Age, sex |
| Triage information | Triage category, chief complaint | ||
| Clinical and laboratory findings | Blood test performance, all vital signs, phlebotomized blood sample | ||
| Medical history | ED revisit | ||
| Others | Mode of arrival, type of specialist | ||
| ≥70 years | Demographics | Age | |
| Triage information | Triage category, chief complaint | ||
| Clinical and laboratory findings | Performance of blood work, phlebotomized blood sample, all vital signs except heart rate | ||
| Medical history | ED visits | ||
| Others | Mode of arrival | ||
| Allan Cameron et al. [28] | Demographics | Age | |
| Triage information | Triage category, National Early Warning Score (NEWS) | ||
| Medical history | Admission in the last year | ||
| Others | Ambulance arrival, referral source | ||
| Noel, Guilhem et al. [29] | Demographics | Sex, age, age category | |
| Triage information | Triage category, final diagnosis | ||
| Others | Mode of arrival | ||
| Reference | Result: AUC |
|---|---|
| Hong, Woo Suk et al. [20] | 0.92 (95% CI 0.92–0.93) |
| Cusidó, J et al. [22] | 0.8938 (95% CI 0.8929–0.8948) |
| Allan Cameron et al. [28] | 0.8774 (95% CI 0.8752–0.8796) |
| Elvira Martínez et al. [17] | 0.85 (95% CI 0.81–0.88) |
| Sun, Yan et al. [25] | 0.849 (95% CI 0.847–0.851) |
| Graham, B et al. [21] | 0.859 |
| Parker et al. [16] | 0.825 (95% CI 0.824–0.827) |
| Alexander Zlotnik et al. [23] | 0.8575 (95% CI 0.8540–0.8610) |
| De Hond, Anne et al. [18] | 0.86 (0.77–0.88) at triage 0.86 (0.82–0.89) at 30 min 0.86 (0.74–0.93) after approximately 2 h |
| Noel, Guilhem el al. [29] | 0.815 (0.805–0.825) |
| Feretzakis, Georgios et al. [26] | 0.806 |
| Feretzakis, Georgios et al. [19] | 0.789 |
| Lucke, Jacinta A et al. [27] | 0.86 (95% CI 0.85–0.87) for those older than 70 years 0.77 (95% CI 0.75–0.79) for those younger than 70 years |
| A. Brink et al. [24] | 0.766 (95% CI 0.759–0.781) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larburu, N.; Azkue, L.; Kerexeta, J. Predicting Hospital Ward Admission from the Emergency Department: A Systematic Review. J. Pers. Med. 2023, 13, 849. https://doi.org/10.3390/jpm13050849
Larburu N, Azkue L, Kerexeta J. Predicting Hospital Ward Admission from the Emergency Department: A Systematic Review. Journal of Personalized Medicine. 2023; 13(5):849. https://doi.org/10.3390/jpm13050849
Chicago/Turabian StyleLarburu, Nekane, Laiene Azkue, and Jon Kerexeta. 2023. "Predicting Hospital Ward Admission from the Emergency Department: A Systematic Review" Journal of Personalized Medicine 13, no. 5: 849. https://doi.org/10.3390/jpm13050849
APA StyleLarburu, N., Azkue, L., & Kerexeta, J. (2023). Predicting Hospital Ward Admission from the Emergency Department: A Systematic Review. Journal of Personalized Medicine, 13(5), 849. https://doi.org/10.3390/jpm13050849