

Positivity and Health Locus of Control: Key Variables to Intervene on Well-Being of Cardiovascular Disease Patients

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
1.1. CVD and Psychological Well-Being and Quality of Life
1.2. CVD and Personality Dispositions: Positivity and Health Locus of Control
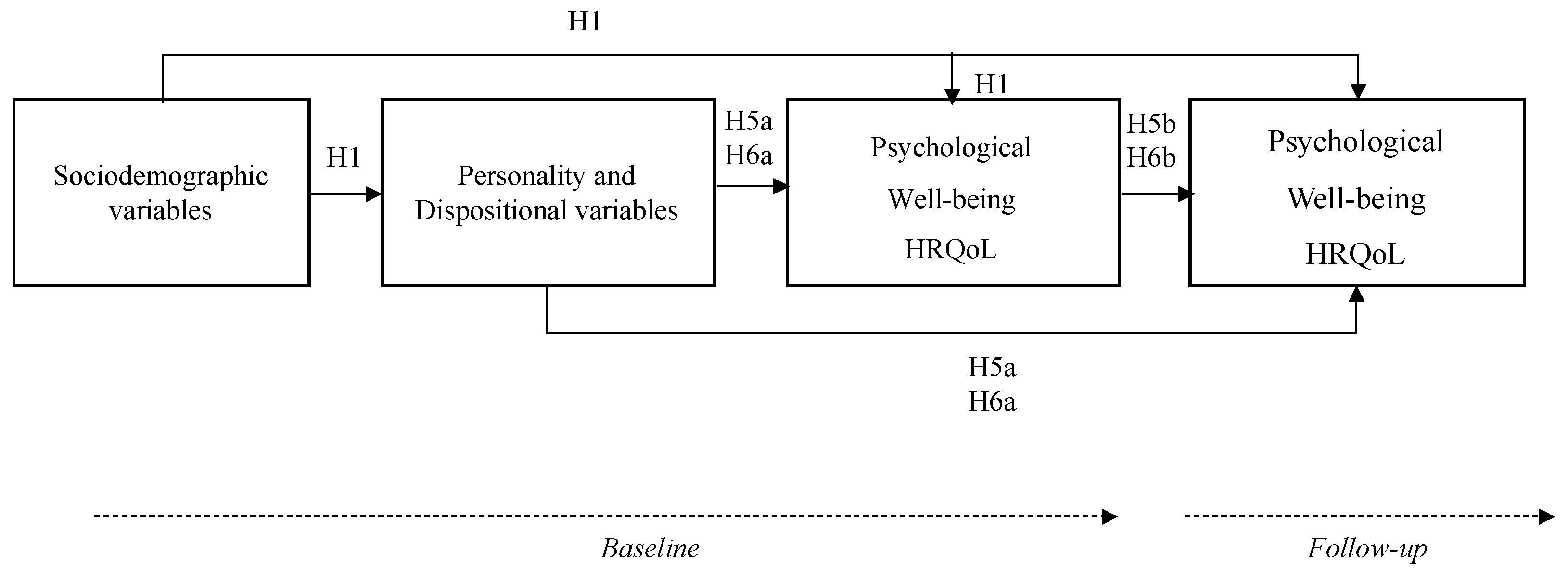
1.3. Aim and Hypotheses
2. Materials and Methods
2.1. Participants and Procedure
2.2. Instruments
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of Participants
3.2. Cross-Sectional Analysis
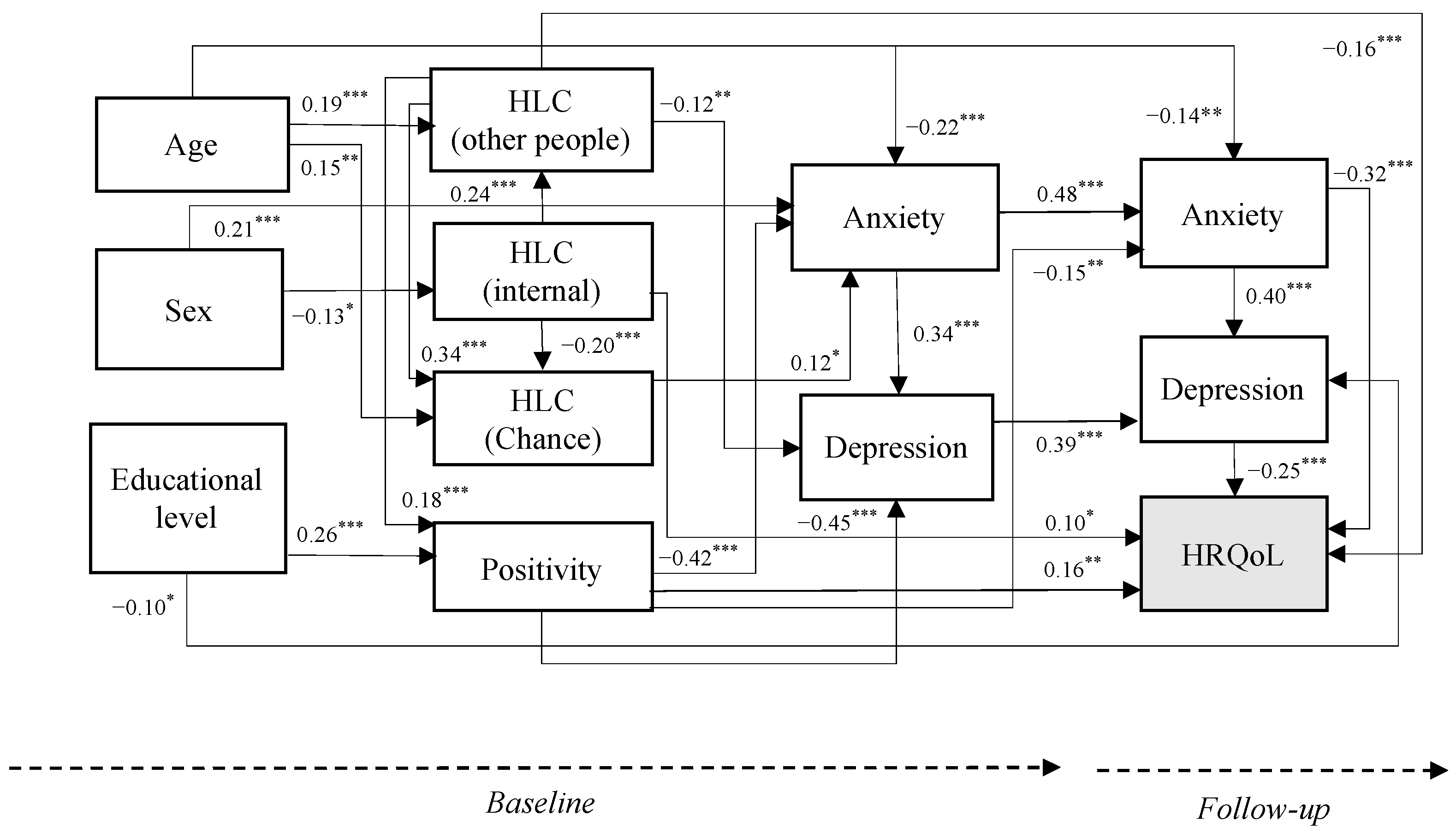
3.3. Longitudinal Analysis
4. Discussion
4.1. Practical Implications
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardiovascular Disease. Available online: https://www.nhs.uk/conditions/cardiovascular-disease/ (accessed on 20 April 2023).
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 31 March 2023).
- Non Communicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 20 April 2023).
- Townsend, N.; Kazakiewicz, D.; Lucy Wright, F.; Timmis, A.; Huculeci, R.; Torbica, A.; Gale, C.P.; Achenbach, S.; Weidinger, F.; Vardas, P. Epidemiology of Cardiovascular Disease in Europe. Nat. Rev. Cardiol. 2022, 19, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Cohen, B.E.; Commodore-Mensah, Y.; Fleury, J.; Huffman, J.C.; Khalid, U.; Labarthe, D.R.; Lavretsky, H.; Michos, E.D.; Spatz, E.S.; et al. Psychological Health, Well-Being, and the Mind-Heart-Body Connection: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e763–e783. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.S.; Andersen, C.M. Minding the Heart: Why Are We Still Not Closer to Treating Depression and Anxiety in Clinical Cardiology Practice? Eur. J. Prev. Cardiol. 2018, 25, 244–246. [Google Scholar] [CrossRef]
- Helmark, C.; Harrison, A.; Pedersen, S.S.; Doherty, P. Systematic Screening for Anxiety and Depression in Cardiac Rehabilitation—Are We There Yet? Int. J. Cardiol. 2022, 352, 65–71. [Google Scholar] [CrossRef]
- Pogosova, N.; Saner, H.; Pedersen, S.S.; Cupples, M.E.; McGee, H.; Höfer, S.; Doyle, F.; Schmid, J.-P.; von Känel, R.; Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation of the European Society of Cardiology. Psychosocial Aspects in Cardiac Rehabilitation: From Theory to Practice. A Position Paper from the Cardiac Rehabilitation Section of the European Association of Cardiovascular Prevention and Rehabilitation of the European Society of Cardiology. Eur. J. Prev. Cardiol. 2015, 22, 1290–1306. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice: Developed by the Task Force for Cardiovascular Disease Prevention in Clinical Practice with Representatives of the European Society of Cardiology and 12 Medical Societies With the Special Contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Kubzansky, L.D.; Huffman, J.C.; Boehm, J.K.; Hernandez, R.; Kim, E.S.; Koga, H.K.; Feig, E.H.; Lloyd-Jones, D.M.; Seligman, M.E.P.; Labarthe, D.R. Positive Psychological Well-Being and Cardiovascular Disease: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1382–1396. [Google Scholar] [CrossRef]
- Bosworth, H.B.; Blalock, D.V.; Hoyle, R.H.; Czajkowski, S.M.; Voils, C.I. The Role of Psychological Science in Efforts to Improve Cardiovascular Medication Adherence. Am. Psychol. 2018, 73, 968–980. [Google Scholar] [CrossRef]
- Pedersen, S.S.; von Känel, R.; Tully, P.J.; Denollet, J. Psychosocial Perspectives in Cardiovascular Disease. Eur. J. Prev. Cardiol. 2017, 24, 108–115. [Google Scholar] [CrossRef]
- Pedersen, S.S.; Doyle, F. Effectiveness of Psychological Intervention as Add-on to Standard Cardiac Rehabilitation: Time to Adopt New Methods or Keep Doing More of the Same? Eur. J. Prev. Cardiol. 2019, 26, 1032–1034. [Google Scholar] [CrossRef] [PubMed]
- Ryff, C.D. Happiness Is Everything, or Is It? Explorations on the Meaning of Psychological Well-Being. J. Personal. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Kobasa, S.C. Stressful Life Events, Personality, and Health: An Inquiry into Hardiness. J. Personal. Soc. Psychol. 1979, 37, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Massé, R.; Poulin, C.; Dassa, C.; Lambert, J.; Bélair, S.; Battaglini, A. The Structure of Mental Health: Higher-Order Confirmatory Factor Analyses of Psychological Distress and Well-Being Measures. Soc. Indic. Res. 1998, 45, 475–504. [Google Scholar] [CrossRef]
- Luque, B.; García, M.d.M.R.; Cuadrado, E.; Gutiérrez, T.; Castillo, R.; Arenas, A.; Tabernero, C. Comparative Study of Positivity and Self-Efficacy for the Regulation of Negative Emotions in Persons with and without Cardiovascular Disease. EC Psychol. Psychiatr 2017, 4, 247–263. [Google Scholar]
- Farhane-Medina, N.Z.; Castillo-Mayén, R.; Luque, B.; Rubio, S.J.; Gutiérrez-Domingo, T.; Cuadrado, E.; Arenas, A.; Tabernero, C. A Brief MHealth-Based Psychological Intervention in Emotion Regulation to Promote Positive Subjective Well-Being in Cardiovascular Disease Patients: A Non-Randomized Controlled Trial. Healthcare 2022, 10, 1640. [Google Scholar] [CrossRef] [PubMed]
- Boehm, J.K.; Soo, J.; Chen, Y.; Zevon, E.S.; Hernandez, R.; Lloyd-Jones, D.; Kubzansky, L.D. Psychological Well-Being’s Link with Cardiovascular Health in Older Adults. Am. J. Prev. Med. 2017, 53, 791–798. [Google Scholar] [CrossRef]
- Ogunmoroti, O.; Osibogun, O.; Spatz, E.S.; Okunrintemi, V.; Mathews, L.; Ndumele, C.E.; Michos, E.D. A Systematic Review of the Bidirectional Relationship between Depressive Symptoms and Cardiovascular Health. Prev. Med. 2022, 154, 106891. [Google Scholar] [CrossRef]
- Gan, Y.; Gong, Y.; Tong, X.; Sun, H.; Cong, Y.; Dong, X.; Wang, Y.; Xu, X.; Yin, X.; Deng, J.; et al. Depression and the Risk of Coronary Heart Disease: A Meta-Analysis of Prospective Cohort Studies. BMC Psychiatry 2014, 14, 371. [Google Scholar] [CrossRef]
- Cohen, B.E.; Edmondson, D.; Kronish, I.M. State of the Art Review: Depression, Stress, Anxiety, and Cardiovascular Disease. Am. J. Hypertens. 2015, 28, 1295–1302. [Google Scholar] [CrossRef]
- Batelaan, N.M.; Seldenrijk, A.; Bot, M.; van Balkom, A.J.L.M.; Penninx, B.W.J.H. Anxiety and New Onset of Cardiovascular Disease: Critical Review and Meta-Analysis. Br. J. Psychiatry 2016, 208, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Rawashdeh, S.I.; Ibdah, R.; Kheirallah, K.A.; Al-Kasasbeh, A.; Raffee, L.A.; Alrabadi, N.; Albustami, I.S.; Haddad, R.; Ibdah, R.M.; Al-Mistarehi, A.-H. Prevalence Estimates, Severity, and Risk Factors of Depressive Symptoms among Coronary Artery Disease Patients after Ten Days of Percutaneous Coronary Intervention. Clin. Pract. Epidemiol. Ment. Health 2021, 17, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Gathright, E.C.; Goldstein, C.M.; Josephson, R.A.; Hughes, J.W. Depression Increases the Risk of Mortality in Patients with Heart Failure: A Meta-Analysis. J. Psychosom. Res. 2017, 94, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Allabadi, H.; Probst-Hensch, N.; Alkaiyat, A.; Haj-Yahia, S.; Schindler, C.; Kwiatkowski, M.; Zemp, E. Mediators of Gender Effects on Depression among Cardiovascular Disease Patients in Palestine. BMC Psychiatry 2019, 19, 284. [Google Scholar] [CrossRef]
- Serpytis, P.; Navickas, P.; Lukaviciute, L.; Navickas, A.; Aranauskas, R.; Serpytis, R.; Deksnyte, A.; Glaveckaite, S.; Petrulioniene, Z.; Samalavicius, R. Gender-Based Differences in Anxiety and Depression Following Acute Myocardial Infarction. Arq. Bras. Cardiol. 2018, 111, 676–683. [Google Scholar] [CrossRef]
- Conley, S.; Feder, S.; Redeker, N.S. The Relationship between Pain, Fatigue, Depression and Functional Performance in Stable Heart Failure. Heart Lung 2015, 44, 107–112. [Google Scholar] [CrossRef]
- Ko, H.-Y.; Lee, J.-K.; Shin, J.-Y.; Jo, E. Health-Related Quality of Life and Cardiovascular Disease Risk in Korean Adults. Korean J. Fam. Med. 2015, 36, 349–356. [Google Scholar] [CrossRef]
- Rieckmann, N.; Neumann, K.; Feger, S.; Ibes, P.; Napp, A.; Preuß, D.; Dreger, H.; Feuchtner, G.; Plank, F.; Suchánek, V.; et al. Health-Related Qualify of Life, Angina Type and Coronary Artery Disease in Patients with Stable Chest Pain. Health Qual. Life Outcomes 2020, 18, 140. [Google Scholar] [CrossRef]
- Yin, S.; Njai, R.; Barker, L.; Siegel, P.Z.; Liao, Y. Summarizing Health-Related Quality of Life (HRQOL): Development and Testing of a One-Factor Model. Popul. Health Metr. 2016, 14, 22. [Google Scholar] [CrossRef]
- Al-Noumani, H.; Al Omari, O.; Al-Naamani, Z. Role of Health Literacy, Social Support, Patient-Physician Relationship, and Health-Related Quality of Life in Predicting Medication Adherence in Cardiovascular Diseases in Oman. Patient Prefer. Adherence 2023, 17, 643–652. [Google Scholar] [CrossRef]
- Pinheiro, L.C.; Reshetnyak, E.; Sterling, M.R.; Richman, J.S.; Kern, L.M.; Safford, M.M. Using Health-Related Quality of Life to Predict Cardiovascular Disease Events. Qual. Life Res. 2019, 28, 1465–1475. [Google Scholar] [CrossRef] [PubMed]
- Phyo, A.Z.Z.; Ryan, J.; Gonzalez-Chica, D.A.; Stocks, N.P.; Reid, C.M.; Tonkin, A.M.; Woods, R.L.; Nelson, M.R.; Murray, A.M.; Gasevic, D.; et al. Health-Related Quality of Life and Incident Cardiovascular Disease Events in Community-Dwelling Older People: A Prospective Cohort Study. Int. J. Cardiol. 2021, 339, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Ryckman, R.M. Theories of Personality, 8th ed.; Wadsworth/Thomson Learning: Belmont, CA, USA, 2004; pp. xxii, 698; ISBN 978-0-534-61983-1. [Google Scholar]
- Caprara, G.V.; Alessandri, G.; Eisenberg, N.; Kupfer, A.; Steca, P.; Caprara, M.G.; Yamaguchi, S.; Fukuzawa, A.; Abela, J. The Positivity Scale. Psychol. Assess. 2012, 24, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.; Mei, S.; Gao, T.; Liang, L.; Li, C.; Hu, Y.; Guo, X.; Meng, C.; Lv, J.; Yuan, T.; et al. Self-Esteem as a Mediator between Life Satisfaction and Depression among Cardiovascular Disease Patients. Clin. Nurs. Res. 2022, 31, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Amonoo, H.L.; Celano, C.M.; Sadlonova, M.; Huffman, J.C. Is Optimism a Protective Factor for Cardiovascular Disease? Curr. Cardiol. Rep. 2021, 23, 158. [Google Scholar] [CrossRef]
- Boehm, J.K.; Kubzansky, L.D. The Heart’s Content: The Association between Positive Psychological Well-Being and Cardiovascular Health. Psychol. Bull. 2012, 138, 655–691. [Google Scholar] [CrossRef]
- DuBois, C.M.; Lopez, O.V.; Beale, E.E.; Healy, B.C.; Boehm, J.K.; Huffman, J.C. Relationships between Positive Psychological Constructs and Health Outcomes in Patients with Cardiovascular Disease: A Systematic Review. Int. J. Cardiol. 2015, 195, 265–280. [Google Scholar] [CrossRef]
- Araújo-Soares, V.; Hankonen, N.; Presseau, J.; Rodrigues, A.; Sniehotta, F.F. Developing Behavior Change Interventions for Self-Management in Chronic Illness. Eur. Psychol. 2019, 24, 7–25. [Google Scholar] [CrossRef]
- Wallston, B.S.; Wallston, K.A.; Kaplan, G.D.; Maides, S.A. Development and Validation of the Health Locus of Control (HLC) Scale. J. Consult. Clin. Psychol. 1976, 44, 580–585. [Google Scholar] [CrossRef]
- Waller, K.V.; Bates, R.C. Health Locus of Control and Self-Efficacy Beliefs in a Healthy Elderly Sample. Am. J. Health Promot. 1992, 6, 302–309. [Google Scholar] [CrossRef]
- Pharr, J.; Enejoh, V.; Mavegam, B.O.; Olutola, A.; Karick, H.; Ezeanolue, E.E. Relationship between Health Locus of Control and Risky Sexual Behaviors among Nigerian Adolescents. J. AIDS Clin. Res. 2015, 6, 471. [Google Scholar] [CrossRef] [PubMed]
- Wallston, K.A.; Wallston, B.S.; DeVellis, R. Development of the Multidimensional Health Locus of Control (MHLC) Scales. Health Educ. Monogr. 1978, 6, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Berglund, E.; Lytsy, P.; Westerling, R. The Influence of Locus of Control on Self-Rated Health in Context of Chronic Disease: A Structural Equation Modeling Approach in a Cross Sectional Study. BMC Public Health 2014, 14, 492. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Lista, J.; Perez-Martinez, P.; Garcia-Rios, A.; Alcala-Diaz, J.F.; Perez-Caballero, A.I.; Gomez-Delgado, F.; Fuentes, F.; Quintana-Navarro, G.; Lopez-Segura, F.; Ortiz-Morales, A.M.; et al. CORonary Diet Intervention with Olive Oil and Cardiovascular PREVention Study (the CORDIOPREV Study): Rationale, Methods, and Baseline Characteristics: A Clinical Trial Comparing the Efficacy of a Mediterranean Diet Rich in Olive Oil versus a Low-Fat Diet on Cardiovascular Disease in Coronary Patients. Am. Heart J. 2016, 177, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Lista, J.; Alcala-Diaz, J.F.; Torres-Peña, J.D.; Quintana-Navarro, G.M.; Fuentes, F.; Garcia-Rios, A.; Ortiz-Morales, A.M.; Gonzalez-Requero, A.I.; Perez-Caballero, A.I.; Yubero-Serrano, E.M.; et al. Long-Term Secondary Prevention of Cardiovascular Disease with a Mediterranean Diet and a Low-Fat Diet (CORDIOPREV): A Randomised Controlled Trial. Lancet 2022, 399, 1876–1885. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Terol, M.C.; López-Roig, S.; Rodríguez-Marín, J.; Martín-Aragón, M.; Pastor, M.A.; Reig, M.T. Propiedades Psicométricas de La Escala Hospitalaria de Ansiedad y Depresión (HAD) En Población Española. [Hospital Anxiety and Depression Scale (HAD): Psychometric Properties in Spanish Population.]. Ansiedad Estrés 2007, 13, 163–176. [Google Scholar]
- Ware, J.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of Scales and Preliminary Tests of Reliability and Validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef]
- Failde, I.; Medina, P.; Ramirez, C.; Arana, R. Construct and Criterion Validity of the SF-12 Health Questionnaire in Patients with Acute Myocardial Infarction and Unstable Angina. J. Eval. Clin. Pract. 2010, 16, 569–573. [Google Scholar] [CrossRef]
- Vilagut, G.; Valderas, J.M.; Ferrer, M.; Garin, O.; López-García, E.; Alonso, J. [Interpretation of SF-36 and SF-12 questionnaires in Spain: Physical and mental components]. Med. Clin. 2008, 130, 726–735. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Alessandri, G.; Caprara, G.V.; Tisak, J. The Unique Contribution of Positive Orientation to Optimal Functioning: Further Explorations. Eur. Psychol. 2012, 17, 44–54. [Google Scholar] [CrossRef]
- Sahoo, S.; Padhy, S.K.; Padhee, B.; Singla, N.; Sarkar, S. Role of Personality in Cardiovascular Diseases: An Issue That Needs to Be Focused Too! Indian Heart J. 2018, 70 (Suppl. 3), S471–S477. [Google Scholar] [CrossRef]
- Steca, P.; Monzani, D.; Pierobon, A.; Avvenuti, G.; Greco, A.; Giardini, A. Measuring Dispositional Optimism in Patients with Chronic Heart Failure and Their Healthcare Providers: The Validity of the Life Orientation Test-Revised. Patient Prefer. Adherence 2017, 11, 1497–1503. [Google Scholar] [CrossRef] [PubMed]
- Caprara, G.V.; Eisenberg, N.; Alessandri, G. Positivity: The Dispositional Basis of Happiness. J. Happiness Stud. 2017, 18, 353–371. [Google Scholar] [CrossRef]
- Mercer, D.A.; Ditto, B.; Lavoie, K.L.; Campbell, T.; Arsenault, A.; Bacon, S.L. Health Locus of Control Is Associated With Physical Activity and Other Health Behaviors in Cardiac Patients. J. Cardiopulm. Rehabil. Prev. 2018, 38, 394–399. [Google Scholar] [CrossRef]
- Lindström, M.; Rosvall, M. Health Locus of Control and Mortality: A Population-Based Prospective Cohort Study. Public Health 2020, 185, 209–211. [Google Scholar] [CrossRef]
- Milte, C.M.; Luszcz, M.A.; Ratcliffe, J.; Masters, S.; Crotty, M. Influence of Health Locus of Control on Recovery of Function in Recently Hospitalized Frail Older Adults. Geriatr. Gerontol. Int. 2015, 15, 341–349. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.S.; Slindee, L.; Kraemer, S.; Yeh, C.S. The Impact of Internal Locus of Control on Healthcare Utilization, Expenditures, and Health Status across Older Adult Income Levels. Geriatr. Nurs. 2020, 41, 274–281. [Google Scholar] [CrossRef]
- Moradi, Y.; Shara, S.A.A.; Namadi, F.; Mollazadeh, F. The Relationship between Health Locus of Control and Self-Efficacy in Patients with Heart Failure. Nurs. Midwifery Stud. 2022, 11, 31. [Google Scholar] [CrossRef]
- Williams, J.S.; Lynch, C.P.; Voronca, D.; Egede, L.E. Health Locus of Control and Cardiovascular Risk Factors in Veterans with Type 2 Diabetes. Endocrine 2016, 51, 83–90. [Google Scholar] [CrossRef]
- Rizza, F.; Gison, A.; Bonassi, S.; Dall’Armi, V.; Tonto, F.; Giaquinto, S. “Locus of Control”, Health-Related Quality of Life, Emotional Distress and Disability in Parkinson’s Disease. J. Health Psychol. 2017, 22, 844–852. [Google Scholar] [CrossRef] [PubMed]
- Banik, A.; Schwarzer, R.; Knoll, N.; Czekierda, K.; Luszczynska, A. Self-Efficacy and Quality of Life among People with Cardiovascular Diseases: A Meta-Analysis. Rehabil. Psychol. 2018, 63, 295–312. [Google Scholar] [CrossRef] [PubMed]
- Pakaya, R.E.; Syam, Y.; Syahrul, S. Correlation of Self-Efficacy and Self-Care of Patients Undergoing Hemodialysis with Their Quality of Life. Enfermería Clínica 2021, 31, S797–S801. [Google Scholar] [CrossRef]
- Nguyen, T.T.N.; Liang, S.-Y.; Liu, C.-Y.; Chien, C.-H. Self-Care Self-Efficacy and Depression Associated with Quality of Life among Patients Undergoing Hemodialysis in Vietnam. PLoS ONE 2022, 17, e0270100. [Google Scholar] [CrossRef]
- Wang, R.; Zhou, C.; Wu, Y.; Sun, M.; Yang, L.; Ye, X.; Zhang, M. Patient Empowerment and Self-Management Behaviour of Chronic Disease Patients: A Moderated Mediation Model of Self-Efficacy and Health Locus of Control. J. Adv. Nurs. 2022, 78, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Grisolía, J.M.; Longo, A.; Hutchinson, G.; Kee, F. Applying Health Locus of Control and Latent Class Modelling to Food and Physical Activity Choices Affecting CVD Risk. Soc. Sci. Med. 2015, 132, 1–10. [Google Scholar] [CrossRef]
- Caprara, G.V.; Castellani, V.; Alessandri, G.; Mazzuca, F.; La Torre, M.; Barbaranelli, C.; Colaiaco, F.; Gerbino, M.; Pasquali, V.; D’Amelio, R.; et al. Being Positive despite Illness: The Contribution of Positivity to the Quality of Life of Cancer Patients. Psychol. Health 2016, 31, 524–534. [Google Scholar] [CrossRef]
- Tabernero, C.; Caprara, G.V.; Gutiérrez-Domingo, T.; Cuadrado, E.; Castillo-Mayén, R.; Arenas, A.; Rubio, S.; Luque, B. Positivity and Self-Efficacy Beliefs Explaining Health-Related Quality of Life in Cardiovascular Patients. Psicothema 2021, 33, 433–441. [Google Scholar] [CrossRef]
- Xu, H.-Y.; Yu, Y.-J.; Zhang, Q.-H.; Hu, H.-Y.; Li, M. Tailored Interventions to Improve Medication Adherence for Cardiovascular Diseases. Front. Pharmacol. 2020, 11, 510339. [Google Scholar] [CrossRef]
- Cruz-Ramos, N.A.; Alor-Hernández, G.; Colombo-Mendoza, L.O.; Sánchez-Cervantes, J.L.; Rodríguez-Mazahua, L.; Guarneros-Nolasco, L.R. MHealth Apps for Self-Management of Cardiovascular Diseases: A Scoping Review. Healthcare 2022, 10, 322. [Google Scholar] [CrossRef] [PubMed]
- Gignac, G.E.; Szodorai, E.T. Effect Size Guidelines for Individual Differences Researchers. Personal. Individ. Differ. 2016, 102, 74–78. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sociodemographic Characteristics | Frequencies | (%) |
|---|---|---|
| Sex | ||
| Male | 508 | 85.7 |
| Female | 85 | 14.3 |
| Age, Mean (SD) = 64.75 (9.07) | ||
| Employment status | ||
| Unemployed | 29 | 4.9 |
| Part-time worker | 17 | 2.9 |
| Full-time worker | 119 | 20.1 |
| Retired | 398 | 67.1 |
| Housework | 30 | 5.1 |
| Partner | ||
| Yes/With | 527 | 88.9 |
| No/Without | 66 | 11.1 |
| Educational level | ||
| Very low | 1 | 0.2 |
| Low | 18 | 3.0 |
| Middle | 332 | 56.0 |
| High | 226 | 38.1 |
| Very high | 16 | 2.7 |
| Economic level | ||
| Very low | 8 | 1.3 |
| Low | 90 | 15.2 |
| Middle | 460 | 77.6 |
| High | 35 | 5.9 |
| (a) | Baseline (n = 593) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| 1. Other people HLC | 1 | |||||||||
| 2. Internal HLC | 0.26 ** | 1 | ||||||||
| 3. Chance HLC | 0.30 ** | −0.02 | 1 | |||||||
| 4. Positivity | 0.20 ** | 0.13 ** | 0.07 | 1 | ||||||
| 5. HADS | −0.17 ** | −0.20 ** | −0.05 | −0.55 ** | 1 | |||||
| 6. Anxiety | −0.09 | −0.15 ** | −0.02 | −0.44 ** | 0.91 ** | 1 | ||||
| 7. Depression | −0.22 ** | −0.22 ** | −0.10 * | −0.55 ** | 0.86 ** | 0.58 ** | 1 | |||
| 8. SF-12 | −0.02 | 0.16 ** | −0.02 | 0.46 ** | −0.63 ** | −0.54 ** | −0.59 ** | 1 | ||
| 9. SF-12 (MCS) | 0.05 | 0.14 ** | 0.01 | 0.51 ** | −0.73 ** | −0.65 ** | −0.65 ** | −0.88 * | 1 | |
| 10. SF-12 (PCS) | −0.03 | 0.15 ** | −0.06 | 0.34 ** | −0.43 ** | −0.38 ** | −0.44 ** | −0.91 ** | 0.61 ** | 1 |
| (b) | Follow-up (n = 323) | |||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| 1. Other people HLC | 1 | |||||||||
| 2. Internal HLC | 0.25 ** | 1 | ||||||||
| 3. Chance HLC | 0.39 ** | 0.05 | 1 | |||||||
| 4. Positivity | 0.29 ** | 0.15 ** | 0.10 | 1 | ||||||
| 5. HADS | −0.29 ** | −0.25 ** | −0.11 | −0.48 ** | 1 | |||||
| 6. Anxiety | −0.19 * | −0.21 * | −0.06 | −0.43 ** | 0.93 ** | 1 | ||||
| 7. Depression | −0.36 ** | −0.27 ** | −0.19 ** | −0.47 ** | 0.86 ** | 0.64 ** | 1 | |||
| 8. SF-12 | 0.10 | 0.15 ** | −0.01 | 0.39 ** | −0.56 ** | −0.53 ** | −0.47 ** | 1 | ||
| 9. SF-12 (MCS) | 0.16 ** | 0.18 ** | −0.02 | 0.44 ** | −0.67 ** | −0.65 ** | −0.54 ** | 0.87 ** | 1 | |
| 10. SF-12 (PCS) | 0.04 | 0.09 | 0.00 | 0.29 ** | −0.38 ** | −0.33 ** | −0.34 ** | 0.91 ** | 0.61 ** | 1 |
| Follow-Up (n = 323) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| 1. Other people HLC | 0.47 ** | 0.24 ** | 0.22 ** | 0.18 ** | −0.17 ** | −0.13 ** | −0.22 ** | −0.06 | 0.05 | −0.14 * |
| 2. Internal HLC | 0.22 ** | 0.44 ** | −0.10 | 0.10 | −0.14 * | −0.09 | −0.16 ** | 0.13 * | 0.16 ** | 0.08 |
| 3. Chance HLC | 0.19 ** | −0.01 | 0.43 ** | 0.04 | −0.03 | 0.01 | −0.06 | −0.09 | −0.08 | −0.08 |
| 4. Positivity | 0.23 ** | 0.17 ** | 0.02 | 0.54 ** | −0.39 ** | −0.35 ** | −0.36 ** | 0.33 ** | 0.36 ** | 0.26 ** |
| 5. HADS | −0.24 ** | −0.16 ** | −0.04 | −0.41 ** | 0.60 ** | 0.58 ** | 0.50 ** | −0.35 ** | −0.44 ** | −0.22 ** |
| 6. Anxiety | −0.14 * | −0.13 * | 0.00 | −0.32 ** | 0.55 ** | 0.58 ** | 0.39 ** | −0.31 ** | −0.41 ** | −0.16 ** |
| 7. Depression | −0.29 ** | −0.19 ** | −0.10 | −0.43 ** | 0.51 ** | 0.41 ** | 0.54 ** | −0.32 ** | −0.37 ** | −0.23 ** |
| 8. SF-12 | 0.12 * | 0.06 | −0.07 | 0.33 ** | −0.45 ** | −0.39 ** | −0.39 ** | −0.60 ** | 0.53 ** | 0.54 ** |
| 9. SF-12 (MCS) | 0.18 ** | 0.09 | −0.02 | 0.36 ** | −0.51 ** | −0.47 ** | −0.44 ** | 0.49 ** | 0.55 ** | 0.36 ** |
| 10. SF-12 (PCS) | 0.04 | 0.00 | −0.11 | 0.23 ** | −0.29 ** | −0.22 ** | −0.27 ** | 0.54 ** | 0.39 ** | 0.57 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luque, B.; Farhane-Medina, N.Z.; Villalba, M.; Castillo-Mayén, R.; Cuadrado, E.; Tabernero, C. Positivity and Health Locus of Control: Key Variables to Intervene on Well-Being of Cardiovascular Disease Patients. J. Pers. Med. 2023, 13, 873. https://doi.org/10.3390/jpm13050873
Luque B, Farhane-Medina NZ, Villalba M, Castillo-Mayén R, Cuadrado E, Tabernero C. Positivity and Health Locus of Control: Key Variables to Intervene on Well-Being of Cardiovascular Disease Patients. Journal of Personalized Medicine. 2023; 13(5):873. https://doi.org/10.3390/jpm13050873
Chicago/Turabian StyleLuque, Bárbara, Naima Z. Farhane-Medina, Marta Villalba, Rosario Castillo-Mayén, Esther Cuadrado, and Carmen Tabernero. 2023. "Positivity and Health Locus of Control: Key Variables to Intervene on Well-Being of Cardiovascular Disease Patients" Journal of Personalized Medicine 13, no. 5: 873. https://doi.org/10.3390/jpm13050873
APA StyleLuque, B., Farhane-Medina, N. Z., Villalba, M., Castillo-Mayén, R., Cuadrado, E., & Tabernero, C. (2023). Positivity and Health Locus of Control: Key Variables to Intervene on Well-Being of Cardiovascular Disease Patients. Journal of Personalized Medicine, 13(5), 873. https://doi.org/10.3390/jpm13050873