
Heart Failure Therapies following Acute Coronary Syndromes with Reduced Ejection Fraction: Data from the ACSIS Survey

 ,
, 
Abstract
:1. Introduction
2. Methods
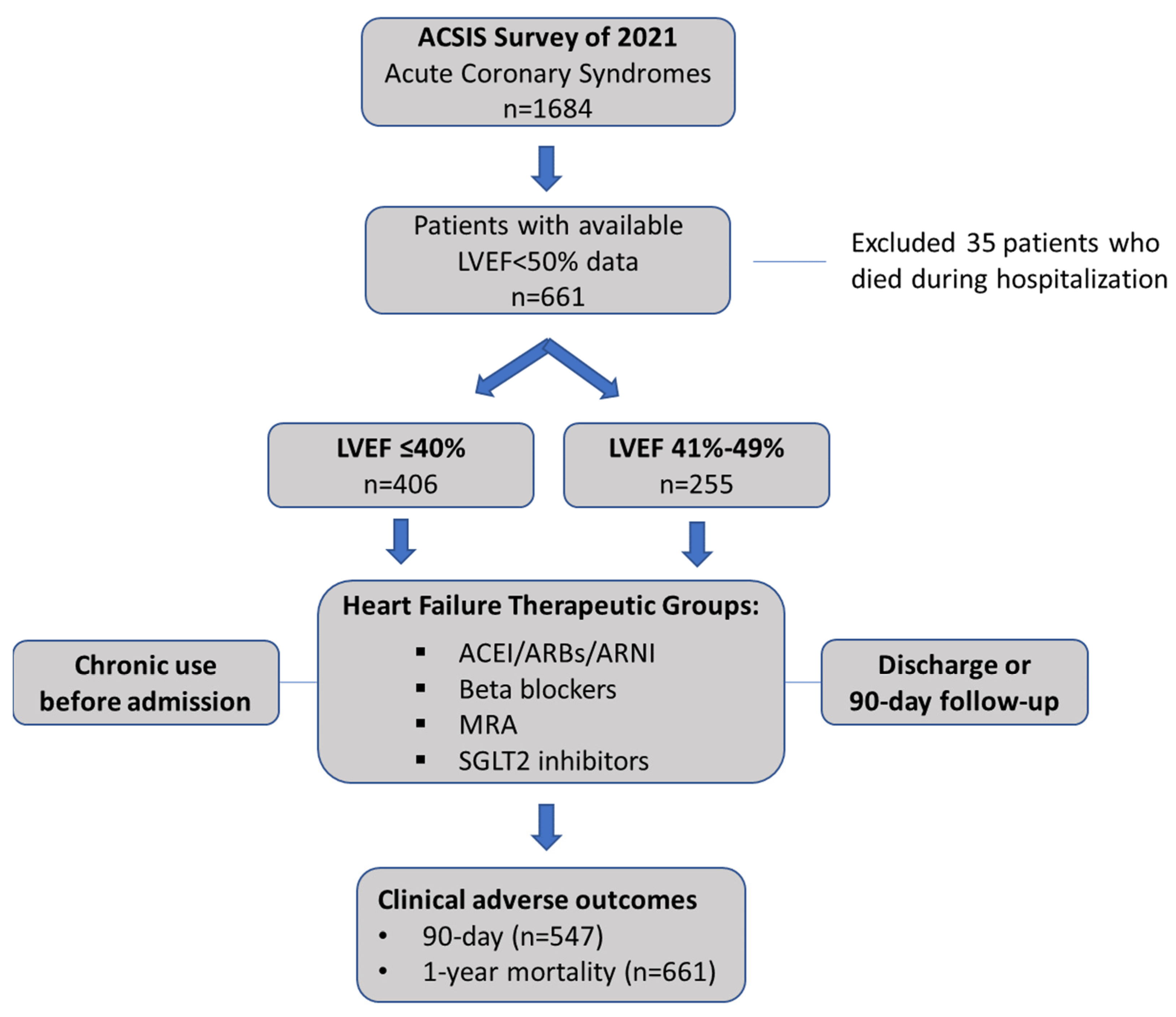
2.1. ACSIS Survey
2.2. Study Population
2.3. Data Analysis
3. Results
3.1. Baseline and In-Hospital Characteristics
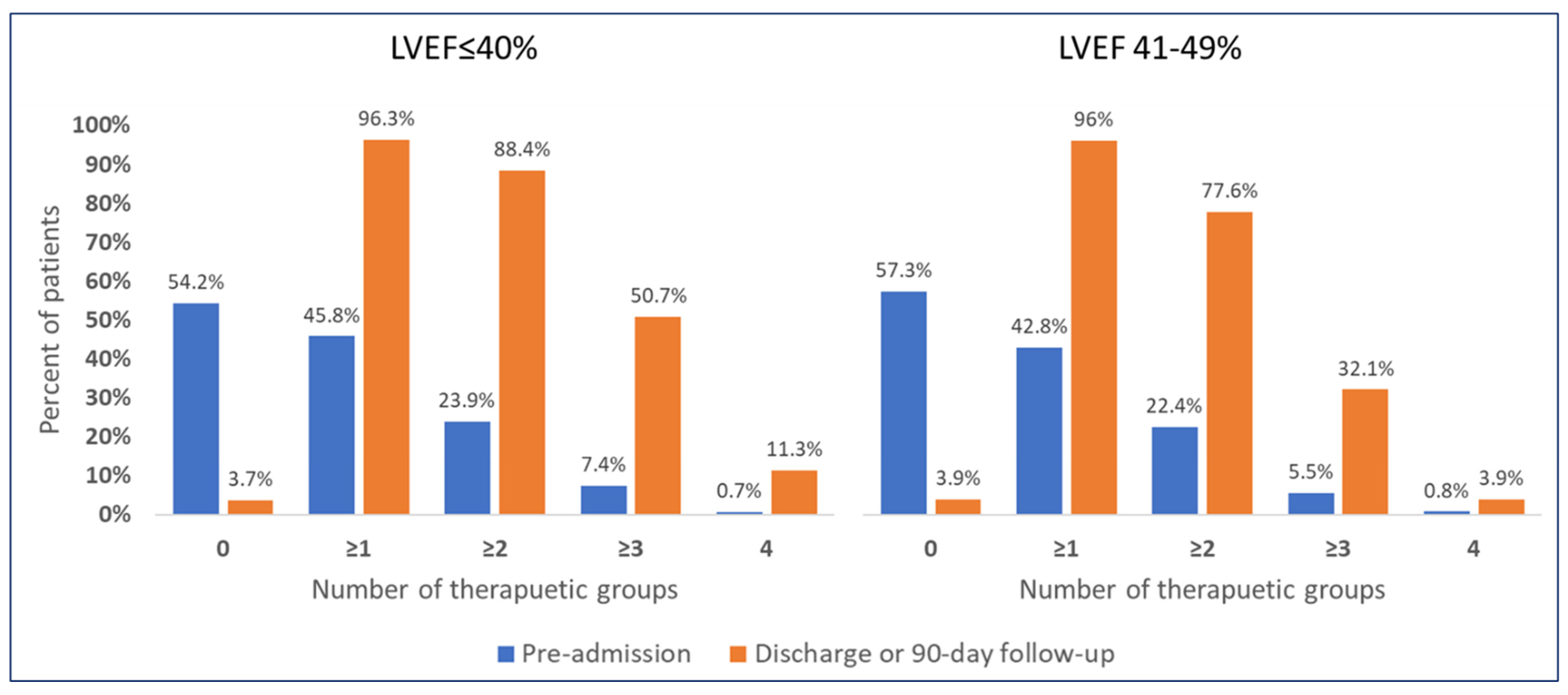
3.2. Drug Therapy for Heart Failure
4. Clinical Outcomes following ACS
5. Discussion
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McMurray, J.J. Clinical practice. Systolic heart failure. N. Engl. J. Med. 2010, 362, 228–238. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Rev. Española Cardiol. Engl. Ed. 2022, 75, 523. [Google Scholar] [CrossRef]
- McMurray, J.J.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. PARADIGM-HF Investigators and Committees. Angioten-sin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef] [Green Version]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. DAPA-HF Trial Committees and Investigators. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Talha, K.M.; Butler, J. Breakthroughs in the treatment of heart failure with mildly reduced and preserved ejection fraction. Clin. Cardiol. 2022, 45 (Suppl. S1), S31–S39. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e895–e1032. [Google Scholar] [CrossRef]
- Hall, T.S.; von Lueder, T.G.; Zannad, F.; Rossignol, P.; Duarte, K.; Chouihed, T.; Solomon, S.D.; Dickstein, K.; Atar, D.; Agewall, S.; et al. High-Risk Myocardial Infarction Database Initiative investigators. Left ventricular ejection fraction and adjudicated, cause-specific hospitalizations after myocardial infarction complicated by heart failure or left ventricular dysfunction. Am. Heart J. 2019, 215, 83–90. [Google Scholar] [CrossRef]
- Harrington, J.; Petrie, M.C.; Anker, S.D.; Bhatt, D.L.; Jones, W.S.; Udell, J.A.; Hernandez, A.F.; Butler, J. Evaluating the Application of Chronic Heart Failure Therapies and Developing Treatments in Individuals with Recent Myocardial Infarction: A Review. JAMA Cardiol. 2022, 7, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Pfeffer, M.A.; Claggett, B.; Lewis, E.F.; Granger, C.B.; Køber, L.; Maggioni, A.P.; Mann, D.L.; McMurray, J.J.; Rouleau, J.-L.; Solomon, S.D.; et al. Angiotensin Receptor–Neprilysin Inhibition in Acute Myocardial Infarction. N. Engl. J. Med. 2021, 385, 1845–1855. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. EMPACT-MI: A Study to Test Whether Empagliflozin Can Lower the Risk of Heart Failure and Death in People Who Had a Heart Attack (Myocardial Infarction). Available online: https://clinicaltrials.gov/ct2/show/NCT04509674 (accessed on 1 October 2022).
- ClinicalTrials.gov. Dapagliflozin Effects on Cardiovascular Events in Patients with an Acute Heart Attack. Available online: https://clinicaltrials.gov/ct2/show/NCT04564742 (accessed on 1 October 2022).
- Desta, L.; Jernberg, T.; Spaak, J.; Hofman-Bang, C.; Persson, H. Risk and predictors of readmission for heart failure following a myocardial infarction between 2004 and 2013: A Swedish nationwide observational study. Int. J. Cardiol. 2017, 248, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Bhagat, A.A.; Greene, S.J.; Vaduganathan, M.; Fonarow, G.C.; Butler, J. Initiation, Continuation, Switching, and Withdrawal of Heart Failure Medical Therapies During Hospitalization. JACC Heart Fail. 2019, 7, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Bahit, M.C.; Kochar, A.; Granger, C.B. Post-Myocardial Infarction Heart Failure. JACC Heart Fail. 2018, 6, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Kochar, A.; Doll, J.A.; Liang, L.; Curran, J.; Peterson, E.D. Temporal Trends in Post Myocardial Infarction Heart Failure and Outcomes Among Older Adults. J. Card. Fail. 2022, 28, 531–539. [Google Scholar] [CrossRef]
- Frantz, S.; Hundertmark, M.J.; Schulz-Menger, J.; Bengel, F.M.; Bauersachs, J. Left ventricular re-modelling post-myocardial infarction: Pathophysiology, imaging, and novel therapies. Eur Heart J. 2022, 43, 2549–2561. [Google Scholar] [CrossRef]
- Bozkurt, B.; Coats, A.J.S.; Tsutsui, H.; Abdelhamid, C.M.; Adamopoulos, S.; Albert, N.; Anker, S.D.; Atherton, J.; Böhm, M.; Butler, J.; et al. Universal definition and classification of heart failure: A report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur. J. Heart Fail. 2021, 23, 352–380. [Google Scholar]
- Von Lewinski, D.; Kolesnik, E.; Tripolt, N.J.; Pferschy, P.N.; Benedikt, M.; Wallner, M.; Alber, H.; Berger, R.; Lichtenauer, M.; Saely, C.H.; et al. Empagliflozin in acute myocardial infarction: The EMMY trial. Eur. Heart J. 2022, 43, 4421–4432. [Google Scholar] [CrossRef]
- Cvijic, M.; Rib, Y.; Danojevic, S.; Radulescu, C.I.; Nazghaidze, N.; Vardas, P. Heart failure with mildly reduced ejection fraction: From diagnosis to treatment. Gaps and dilemmas in current clinical practice. Heart Fail. Rev. 2022. epub ahead of print. [Google Scholar] [CrossRef]
- Lam, C.S.; Solomon, S.D. The middle child in heart failure: Heart failure with mid-range ejection fraction (40–50%). Eur. J. Heart Fail. 2014, 16, 1049–1055. [Google Scholar] [CrossRef]
- Pfeffer, M.A.; Claggett, B.; Lewis, E.F.; Granger, C.B.; Kober, L.; Maggioni, A.P.; Mann, D.L.; McMurray, J.J.V.; Rouleau, J.-L.; Solomon, S.D.; et al. Impact of sacubitril/valsartan versus ramipril on total heart failure events in the PARADISE-MI Trial. Circulation 2022, 145, 87–89. [Google Scholar] [CrossRef]
- Luo, N.; Fonarow, G.C.; Lippmann, S.J.; Mi, X.; Heidenreich, P.A.; Yancy, C.W.; Greiner, M.A.; Hammill, B.G.; Hardy, N.C.; Turner, S.J.; et al. Early Adoption of Sacubitril/Valsartan for Patients with Heart Failure with Reduced Ejection Fraction: Insights from Get with the Guidelines-Heart Failure (GWTG-HF). JACC Heart Fail. 2017, 5, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Pierce, J.B.; Li, Z.; Greiner, M.; Lippmann, S.J.; Hardy, N.C.; Shen, X.; Stampehl, M.; Mentz, R.J.; Allen, L.A.; Peterson, P.N.; et al. Adoption of Sacubitril/Valsartan Among Patients with Heart Failure with Mildly Reduced or Preserved Ejection Fraction: The Get with the Guidelines—Heart Failure Registry. Circ. Heart Fail. 2022, 16, e010176. [Google Scholar] [CrossRef]
- Tromp, J.; Ouwerkerk, W.; Teng, T.-H.K.; Cleland, J.G.F.; Bamadhaj, S.; Angermann, C.E.; Dahlstrom, U.; Tay, W.T.; Dickstein, K.; Ertl, G.; et al. Global disparities in prescription of guideline-recommended drugs for heart failure with reduced ejection fraction. Eur. Heart J. 2022, 43, 2224–2234. [Google Scholar] [CrossRef] [PubMed]
- Curtis, L.H.; Mi, X.; Qualls, L.G.; Check, D.K.; Hammill, B.G.; Hammill, S.C.; Heidenreich, P.A.; Masoudi, F.A.; Setoguchi, S.; Hernandez, A.F.; et al. Transitional adherence and persistence in the use of aldosterone antagonist therapy in patients with heart failure. Am. Heart J. 2013, 165, 979–986.e1. [Google Scholar] [CrossRef]
- Mebazza, A.; Davison, B.; Chioncel, O.; Cohen-Solal, A.; Diaz, R.; Filippatos, G.; Metra, M.; Ponikowski, P.; Sliwa, K.; Voors, A.A.; et al. Safety, tolerability, and efficacy of up-titration of guide-line-directed medical therapies for acute heart failure (STRONG-HF): A multinational, open-label, randomised, trial. Lancet 2022, 400, 1938–1952. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.; Straus, S.E.; Farkouh, M.E.; Austin, P.C.; Taljaard, M.; Chong, A.; Fahim, C.; Poon, S.; Cram, P.; Smith, S.; et al. Trial of an Intervention to Improve Acute Heart Failure Outcomes. N. Engl. J. Med. 2023, 388, 22–32. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | LVEF ≤ 40% | LVEF 41–49% | p-Value |
|---|---|---|---|---|
| n = 661 | n = 406 | n = 255 | ||
| Age, years (mean (SD)) | 63.97 (11.99) | 64.50 (12.07) | 63.12 (11.83) | 0.150 |
| Gender (male) | 542 (82.0) | 319 (78.6) | 223 (87.5) | 0.005 |
| BMI (kg/m2) (median [IQR]) | 26.9 [24.5, 29.8] | 26.8 [24.4, 29.7] | 27.2 [24.5, 30.3] | 0.260 |
| Hypertension | 403 (61.0) | 252 (62.1) | 151 (59.2) | 0.516 |
| Dyslipidemia | 439 (66.5) | 269 (66.3) | 170 (66.9) | 0.926 |
| Diabetes mellitus | 287 (43.4) | 181 (44.6) | 106 (41.6) | 0.496 |
| Current smokers | 312 (47.2) | 189 (46.6) | 123 (48.2) | 0.732 |
| Past smokers | 116 (17.5) | 72 (17.7) | 44 (17.3) | 0.958 |
| Chronic renal failure | 64 (9.7) | 44 (10.8) | 20 (7.8) | 0.258 |
| Chronic Obstructive Pulmonary Disease | 43 (6.5) | 32 (7.9) | 11 (4.3) | 0.098 |
| Any malignancy | 36 (5.5) | 21 (5.2) | 15 (6.0) | 0.800 |
| Peripheral Vascular Disease | 58 (8.8) | 38 (9.4) | 20 (7.9) | 0.607 |
| Prior Cerebrovascular Accident/Transient Ischemic Attack | 60 (9.1) | 43 (10.6) | 17 (6.7) | 0.116 |
| History of Congestive Heart Failure | 80 (12.1) | 62 (15.3) | 18 (7.1) | 0.002 |
| Prior Myocardial Infarction | 236 (35.8) | 154 (37.9) | 82 (32.4) | 0.176 |
| Prior Coronary Artery Bypass Graft | 43 (6.5) | 27 (6.7) | 16 (6.3) | 0.977 |
| Prior Percutaneous Coronary Intervention | 230 (34.8) | 149 (36.7) | 81 (31.9) | 0.239 |
| Chronic Use before Admission | Initiated during Hospitalization | Therapy at Discharge or at 90-Day Follow-Up | |
|---|---|---|---|
| EF ≤ 40% (n = 406) | |||
| ACEI (%) | 82 (20.2%) | 208 (51.2%) | 260 (64%) |
| ARB (%) | 53 (13.1%) | 60 (14.8%) | 103 (25.4%) |
| ARNI (%) | 3 (0.7%) | 4 (1%) | 16 (3.9%) |
| MRA (%) | 24 (5.9%) | 143 (35.2%) | 174 (42.9%) |
| Beta Blockers (%) | 120 (29.6%) | 270 (66.5%) | 370 (91.1%) |
| SGLT2I (%) | 35 (8.6%) | 34 (8.4%) | 103 (25.4%) |
| Diuretics (%) | 28 (6.9%) | 105 (25.9%) | 132 (32.5%) |
| No. of HF therapeutic groups (median [IQR]) | 0 [0, 1] | 2 [1, 3] | 3 [2, 3] |
| EF 41–49% (n = 255) | |||
| ACEI (%) | 47 (18.4%) | 134 (52.5%) | 164 (64.3%) |
| ARB (%) | 39 (15.3%) | 26 (10.2%) | 55 (21.6%) |
| ARNI (%) | 0 | 0 | 1 (0.4%) |
| MRA (%) | 4 (1.6%) | 26 (10.2%) | 31 (12.2%) |
| Beta Blockers (%) | 64 (25.1%) | 166 (65.1%) | 221 (86.7%) |
| SGLT2I (%) | 28 (11%) | 26 (10.2%) | 68 (26.7%) |
| Diuretics (%) | 14 (5.5%) | 26 (10.2%) | 41 (16.1%) |
| No. of HF therapeutic groups (median [IQR]) | 0 [0, 1] | 2 [1, 2] | 2 [2, 3] |
| Overall | LVEF ≤ 40% | LVEF 41–49% | p-Value | |
|---|---|---|---|---|
| Patients with Available 90-Day Follow-Up | ||||
| n | 547 | 328 | 219 | |
| Rehospitalizations—ACS (cardiac, unscheduled) * (%) | 12 (2.2) | 9 (2.7) | 3 (1.4) | 0.437 |
| Rehospitalizations—CHF (%) | 14 (2.6) | 12 (3.7) | 2 (0.9) | 0.085 |
| ACS (UA/NSTEMI/STEMI/ Stent thrombosis) (%) | 19 (3.5) | 14 (4.3) | 5 (2.3) | 0.315 |
| Aborted SCD (%) | 1 (0.2) | 1 (0.3) | 0 (0.0) | 1.000 |
| 90-day any mortality (%) | 2 (0.4) | 1 (0.3) | 1 (0.5) | 1.000 |
| Combined outcome 90-days (CHF, ACS, any death) (%) | 33 (6.0) | 25 (7.6) | 8 (3.7) | 0.084 |
| Referral to rehabilitation (%) | 388 (72.8) | 234 (73.6) | 154 (71.6) | 0.690 |
| Participation in rehabilitation (or scheduled) (%) | 175 (34.1) | 106 (34.2) | 69 (34.0) | 1.000 |
| All patients | ||||
| n | 661 | 406 | 255 | |
| 30-day MACE ** (%) | 52 (7.9) | 34 (8.4) | 18 (7.1) | 0.643 |
| 1-year mortality *** (%) | 21 (3.2) | 17 (4.2) | 4 (1.6) | 0.101 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zafrir, B.; Ovdat, T.; Abu Akel, M.; Bahouth, F.; Orvin, K.; Beigel, R.; Amir, O.; Elbaz-Greener, G. Heart Failure Therapies following Acute Coronary Syndromes with Reduced Ejection Fraction: Data from the ACSIS Survey. J. Pers. Med. 2023, 13, 1015. https://doi.org/10.3390/jpm13061015
Zafrir B, Ovdat T, Abu Akel M, Bahouth F, Orvin K, Beigel R, Amir O, Elbaz-Greener G. Heart Failure Therapies following Acute Coronary Syndromes with Reduced Ejection Fraction: Data from the ACSIS Survey. Journal of Personalized Medicine. 2023; 13(6):1015. https://doi.org/10.3390/jpm13061015
Chicago/Turabian StyleZafrir, Barak, Tal Ovdat, Mahmood Abu Akel, Fadel Bahouth, Katia Orvin, Roy Beigel, Offer Amir, and Gabby Elbaz-Greener. 2023. "Heart Failure Therapies following Acute Coronary Syndromes with Reduced Ejection Fraction: Data from the ACSIS Survey" Journal of Personalized Medicine 13, no. 6: 1015. https://doi.org/10.3390/jpm13061015
APA StyleZafrir, B., Ovdat, T., Abu Akel, M., Bahouth, F., Orvin, K., Beigel, R., Amir, O., & Elbaz-Greener, G. (2023). Heart Failure Therapies following Acute Coronary Syndromes with Reduced Ejection Fraction: Data from the ACSIS Survey. Journal of Personalized Medicine, 13(6), 1015. https://doi.org/10.3390/jpm13061015