
Quality of Life (QoL) in Patients with Chronic Inflammatory Bowel Diseases: How Much Better with Biological Drugs?

 ,
,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection and Outcome Measures
2.3. Measurements
3. Statistical Analysis
4. Ethical Statement
5. Results
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, Z.; Wang, S.; Li, J. Treatment of Inflammatory Bowel Disease: A Comprehensive Review. Front. Med. 2021, 8, 765474. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, O.H.; Ainsworth, M.A. Tumor necrosis factor inhibitors for inflammatory bowel disease. N. Engl. J. Med. 2013, 369, 754–762. [Google Scholar] [CrossRef] [Green Version]
- Ben-Horin, S.; Kopylov, U.; Chowers, Y. Optimizing anti-TNF treatments in inflammatory bowel disease. Autoimmun. Rev. 2014, 13, 24–30. [Google Scholar] [CrossRef]
- Sekhri, S.; Yarur, A.J. Integrating new and emerging therapies into inflammatory bowel disease clinical practice. Curr. Opin. Gastroenterol. 2022, 38, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Zallot, C.; Peyrin-Biroulet, L. Deep remission in inflammatory bowel disease: Looking beyond symptoms. Curr. Gastroenterol. Rep. 2013, 15, 315. [Google Scholar] [CrossRef]
- Williet, N.; Sandborn, W.J.; Peyrin-Biroulet, L. Patient-reported outcomes as primary end points in clinical trials of inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2014, 12, 1246–1256.e1246. [Google Scholar] [CrossRef]
- Lega, S.; Dubinsky, M.C. What Are the Targets of Inflammatory Bowel Disease Management. Inflamm. Bowel Dis. 2018, 24, 1670–1675. [Google Scholar] [CrossRef]
- Privitera, G.; Pugliese, D.; Lopetuso, L.R.; Scaldaferri, F.; Neri, M.; Guidi, L.; Gasbarrini, A.; Armuzzi, A. Novel trends with biologics in inflammatory bowel disease: Sequential and combined approaches. Therap. Adv. Gastroenterol. 2021, 14, 17562848211006669. [Google Scholar] [CrossRef]
- Buckland, A.; Bodger, K. The cost-utility of high dose oral mesalazine for moderately active ulcerative colitis. Aliment Pharmacol. Ther. 2008, 28, 1287–1296. [Google Scholar] [CrossRef]
- Fengming, Y.; Jianbing, W. Biomarkers of inflammatory bowel disease. Dis. Markers 2014, 2014, 710915. [Google Scholar] [CrossRef] [PubMed]
- Cioffi, M.; Rosa, A.D.; Serao, R.; Picone, I.; Vietri, M.T. Laboratory markers in ulcerative colitis: Current insights and future advances. World J. Gastrointest. Pathophysiol. 2015, 6, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Holdam, A.S.; Bager, P.; Dahlerup, J.F. Biological therapy increases the health-related quality of life in patients with inflammatory bowel disease in a clinical setting. Scand. J. Gastroenterol. 2016, 51, 706–711. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, validation and norming. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef]
- Webster, K.; Cella, D.; Yost, K. The Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System: Properties, applications, and interpretation. Health Qual. Life Outcomes 2003, 1, 79. [Google Scholar] [CrossRef] [Green Version]
- Tinsley, A.; Macklin, E.A.; Korzenik, J.R.; Sands, B.E. Validation of the functional assessment of chronic illness therapy-fatigue (FACIT-F) in patients with inflammatory bowel disease. Aliment Pharmacol. Ther. 2011, 34, 1328–1336. [Google Scholar] [CrossRef]
- Reilly, M.C.; Zbrozek, A.S.; Dukes, E.M. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics 1993, 4, 353–365. [Google Scholar] [CrossRef]
- Knowles, S.R.; Graff, L.A.; Wilding, H.; Hewitt, C.; Keefer, L.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses-Part I. Inflamm. Bowel Dis. 2018, 24, 742–751. [Google Scholar] [CrossRef]
- Byron, C.; Cornally, N.; Burton, A.; Savage, E. Challenges of living with and managing inflammatory bowel disease: A meta-synthesis of patients’ experiences. J. Clin. Nurs. 2020, 29, 305–319. [Google Scholar] [CrossRef]
- Martino, G.; Caputo, A.; Schwarz, P.; Bellone, F.; Fries, W.; Quattropani, M.C.; Vicario, C.M. Alexithymia and Inflammatory Bowel Disease: A Systematic Review. Front. Psychol. 2020, 11, 1763. [Google Scholar] [CrossRef] [PubMed]
- Sajadinejad, M.S.; Asgari, K.; Molavi, H.; Kalantari, M.; Adibi, P. Psychological issues in inflammatory bowel disease: An overview. Gastroenterol. Res. Pract. 2012, 2012, 106502. [Google Scholar] [CrossRef] [PubMed]
- Burisch, J.; Weimers, P.; Pedersen, N.; Cukovic-Cavka, S.; Vucelic, B.; Kaimakliotis, I.; Duricova, D.; Bortlik, M.; Shonová, O.; Vind, I.; et al. Health-related quality of life improves during one year of medical and surgical treatment in a European population-based inception cohort of patients with inflammatory bowel disease--an ECCO-EpiCom study. J. Crohns Colitis 2014, 8, 1030–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aladraj, H.; Abdulla, M.; Guraya, S.Y.; Guraya, S.S. Health-Related Quality of Life of Patients Treated with Biological Agents and New Small-Molecule Drugs for Moderate to Severe Crohn’s Disease: A Systematic Review. J. Clin. Med. 2022, 11, 3743. [Google Scholar] [CrossRef]
- Golovics, P.A.; Gonczi, L.; Reinglas, J.; Verdon, C.; Pundir, S.; Afif, W.; Wild, G.; Bitton, A.; Bessissow, T.; Lakatos, P.L. Patient-Reported Outcome and Clinical Scores Are Equally Accurate in Predicting Mucosal Healing in Ulcerative Colitis: A Prospective Study. Dig Dis. Sci. 2022, 67, 3089–3095. [Google Scholar] [CrossRef]
- Tribbick, D.; Salzberg, M.; Connell, W.; Macrae, F.; Kamm, M.; Bates, G.; Cunningham, G.; Austin, D.; Knowles, S. Differences Across Illness Perceptions in Inflammatory Bowel Disease and Their Relationships to Psychological Distress and Quality of Life. Gastroenterol. Nurs. 2017, 40, 291–299. [Google Scholar] [CrossRef]
- Fardet, L.; Kassar, A.; Cabane, J.; Flahault, A. Corticosteroid-induced adverse events in adults: Frequency, screening and prevention. Drug Saf. 2007, 30, 861–881. [Google Scholar] [CrossRef]
- Schacke, H.; Docke, W.D.; Asadullah, K. Mechanisms involved in the side effects of glucocorticoids. Pharmacol. Ther. 2002, 96, 23–43. [Google Scholar] [CrossRef]
- Klein, J.F. Adverse psychiatric effects of systemic glucocorticoid therapy. Am. Fam. Physician 1992, 46, 1469–1474. [Google Scholar]
- Sullivan, P.W.; Ghushchyan, V.H.; Globe, G.; Sucher, B. Health-related quality of life associated with systemic corticosteroids. Qual. Life Res. 2017, 26, 1037–1058. [Google Scholar] [CrossRef]
- Herrera-deGuise, C.; Casellas, F.; Robles, V.; Navarro, E.; Borruel, N. Predictive value of early restoration of quality of life in Crohn’s disease patients receiving antitumor necrosis factor agents. J. Gastroenterol. Hepatol. 2015, 30, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Patel, H.; Colombel, J.F.; Rubin, D.T.; James, A.; Mody, R.; Lasch, K. Effects of vedolizumab on health-related quality of life in patients with ulcerative colitis: Results from the randomised GEMINI 1 trial. Aliment Pharmacol. Ther. 2017, 45, 264–275. [Google Scholar] [CrossRef] [PubMed]
- Vermeire, S.; D’Haens, G.; Baert, F.; Danese, S.; Kobayashi, T.; Loftus, E.V.; Bhatia, S.; Agboton, C.; Rosario, M.; Chen, C.; et al. Efficacy and Safety of Subcutaneous Vedolizumab in Patients With Moderately to Severely Active Crohn’s Disease: Results From the VISIBLE 2 Randomised Trial. J. Crohns Colitis 2022, 16, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Paschos, P.; Katsoula, A.; Salanti, G.; Giouleme, O.; Athanasiadou, E.; Tsapas, A. Systematic review with network meta-analysis: The impact of medical interventions for moderate-to-severe ulcerative colitis on health-related quality of life. Aliment Pharmacol. Ther. 2018, 48, 1174–1185. [Google Scholar] [CrossRef]
- Minderhoud, I.M.; Samsom, M.; Oldenburg, B. Crohn’s disease, fatigue, and infliximab: Is there a role for cytokines in the pathogenesis of fatigue? World J. Gastroenterol. 2007, 13, 2089–2093. [Google Scholar] [CrossRef]
- Bellone, F.; Sardella, A.; Muscianisi, M.; Basile, G. Fatigue, sarcopenia, and frailty in older adults with Inflammatory Bowel Disease. Minerva Gastroenterol. 2021; Online ahead of print. [Google Scholar] [CrossRef]
- Vogelaar, L.; van’t Spijker, A.; van Tilburg, A.J.; Kuipers, E.J.; Timman, R.; van der Woude, C.J. Determinants of fatigue in Crohn’s disease patients. Eur. J. Gastroenterol. Hepatol. 2013, 25, 246–251. [Google Scholar] [CrossRef]
- Peruzzolo, T.L.; Pinto, J.V.; Roza, T.H.; Shintani, A.O.; Anzolin, A.P.; Gnielka, V.; Kohmann, A.M.; Marin, A.S.; Lorenzon, V.R.; Brunoni, A.R.; et al. Inflammatory and oxidative stress markers in post-traumatic stress disorder: A systematic review and meta-analysis. Mol. Psychiatry 2022, 27, 3150–3163. [Google Scholar] [CrossRef]
- Zhang, C.L.; Gao, M.Q.; Jiang, X.C.; Pan, X.; Zhang, X.Y.; Li, Y.; Shen, Q.; Chen, Y.; Pang, B. Research progress and value of albumin-related inflammatory markers in the prognosis of non-small cell lung cancer: A review of clinical evidence. Ann. Med. 2023, 55, 1294–1307. [Google Scholar] [CrossRef]
- Elbadawy, H.M.; Khattab, A.; El-Agamy, D.S.; Eltahir, H.M.; Alhaddad, A.; Aljohani, F.D.; Almuzaini, T.M.; Abouzied, M.M.; Aldhafiri, A. IL-6 at the center of cytokine storm: Circulating inflammation mediators as biomarkers in hospitalized COVID-19 patients. J. Clin. Lab Anal. 2023, 37, e24881. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T0 | T1 | T2 | p | |
|---|---|---|---|---|
| Number | 50 | 50 | 50 | |
| Sex (m/f) | 26/24 | 26/24 | 26/24 | |
| Disease (CD/UC) | 26/24 | 26/24 | 26/24 | |
| Age at diagnosis | 28 (12–44) | |||
| Age at time of start of biological treatment | 48 (33–63) | |||
| No surgery/surgery | 38/12 | 38/12 | 38/12 | |
| Vedolizumab/Infliximab | 22/28 | 22/28 | 22/28 | |
| Median and IQR | ||||
| Red blood cells (103/mm3) | 4550 (4202.5–5087.5) | 4585 (4167.5–5030) | 4533 (4187.5–5020) | ns |
| Hemoglobin (g%) | 12.4 (10.6–13.7) | 12.3 (11.2–13.6) | 12.65 (11.3–13.9) | ns |
| HCT % | 38.6 (33.7–41) | 37.6 (33.9–41.7) | 38.2 (34.7–41.7) | ns |
| MCV fl | 83 (76–89.8) | 83.05 (77.9–90.5) | 83.2 (76.9–87.9) | ns |
| MCH pg | 27.36 (24.7–30.3) | 27.9 (24.1–30.1) | 27.7 (25.2–29.6) | ns |
| White blood cells (103/mm3) | 9445 (6550–11400) | 7505 (5900–9591) | 7265 (6050–9755) | <0.001 |
| Platelets (103/mm3) | 299.5 (231.5–438) | 274.3 (231.1–380.5) | 269.5 (222.8–381.2) | ns |
| C-reactive protein (mg/dL) | 4.57 (1.42–15) | 3.05 (0.42–8.65) | 3.35 (1–10.2) | <0.001 |
| Erythrocyte sedimentation rate (mm) | 20 (11.3–42.3) | 15 (8–40) | 16 (7.75–40) | ns |
| Total protein (g/dL) | 6.97 (6.7–7.3) | 7.1 (6.8–7.4) | 7.1 (6.7–7.5) | ns |
| Alpha1 globulins % | 4.85 (3.3–5.52) | 4.3 (3–5.3) | 3.87 (2.8–5) | <0.001 |
| Alpha2 globulins % | 12.2 (10.2–13.3) | 11.2 (9.1–12.5) | 11.1 (9.6–12.2) | <0.001 |
| Median (min–max) | ||||
| Disease activity score(s) | ||||
| SES-CD | 18 (7–30) | |||
| Rutgeerts | 4 (2–4) | |||
| Mayo | 2 (1–3) | |||
| CD (HBI) | 3 (1–7) | 0 (0–8) | 0 (0–7) | =0.002 |
| UC (pMS) | 4 (1–9) | 2 (0–7) | 0 (0–8) | <0.001 |
| Friedman’s Test | Wilcoxon’s Test | |||
|---|---|---|---|---|
| p-Value | p-Value | |||
| T0–T1–T2 | T0–T1 | T1–T2 | T0–T2 | |
| White blood cells | p < 0.001 | 0.003 | 0.754 | 0.002 |
| C-reactive protein | p < 0.001 | 0.047 | 0.539 | 0.046 |
| Alpha1 globulins | p < 0.01 | 0.217 | 0.201 | 0.008 |
| Alpha2 globulins | p < 0.001 | 0.001 | 0.566 | 0.002 |
| T0-T1 | T1-T2 | T0-T2 | ||||
|---|---|---|---|---|---|---|
| Wilcoxon’s Test—SF-36 | ||||||
| Δ% | p-value | Δ% | p-value | Δ% | p-value | |
| 1. Physical role and functioning | 27.2 | p < 0.001 | 3.21 | p = 0.182 | 30.4 | p < 0.001 |
| 2. Role and physical health | 100.9 | p < 0.001 | 21.2 | p = 0.036 | 122.1 | p < 0.001 |
| 3. Mental health | 69.5 | p < 0.005 | 14.8 | p = 0.377 | 84.4 | p < 0.001 |
| 4. Vitality | 35.3 | p < 0.001 | 3.56 | p = 0.091 | 38.9 | p < 0.001 |
| 5. Emotional role | 29.5 | p < 0.001 | 6.81 | p = 0.006 | 36.3 | p < 0.001 |
| 6. Social functioning | 33.9 | p < 0.001 | 6.59 | p = 0.006 | 40.5 | p < 0.001 |
| 7. Body pain | 51.3 | p < 0.001 | −2.06 | p = 0.577 | 49.3 | p < 0.001 |
| 8. General health | 51.8 | p < 0.001 | −0.61 | p = 0.703 | 51.2 | p < 0.001 |
| Wilcoxon’s Test—FACIT:GH | ||||||
| Δ% | p-value | Δ% | p-value | Δ% | p-value | |
| 1. Physical well-being | 25.7 | p < 0.001 | 4.25 | p < 0.001 | 31.1 | p = 0.000 |
| 2. Social/family well-being | −2.31 | p = 0.411 | 2.37 | p = 0.916 | 0 | p = 0.419 |
| 3. Emotional well-being | 22.6 | p < 0.001 | 1.64 | p = 0.233 | 24.56 | p < 0.001 |
| 4. Functional well-being | 18.2 | p < 0.001 | 4.78 | p = 0.216 | 23.84 | p < 0.001 |
| 5. Additional concerns (FACIT-FS) | 30.9 | p < 0.001 | 1.15 | p = 0.180 | 32.4 | p < 0.001 |
| 6. FACIT-G | 15.3 | p < 0.001 | 3.93 | p < 0.001 | 19.8 | p < 0.001 |
| 7. FACIT-GH (FACIT-G + FACIT-FS) | 20.4 | p < 0.001 | 2.94 | p = 0.015 | 23.9 | p < 0.001 |
| Wilcoxon’s Test—WPAI:GH | ||||||
| Δ% | p-value | Δ% | p-value | Δ% | p-value | |
| 2. Work time missed (health) | −50.9 | p < 0.05 | −15.4 | p = 0.285 | −58.4 | p < 0.05 |
| 3. Work time missed (other) | −21.6 | p = 0.655 | 5.47 | p = 0.317 | −17.3 | p = 0.285 |
| 4. Effective worked hours | −11.6 | p < 0.007 | 5.94 | p = 0.027 | −6.36 | p < 0.001 |
| 5. Impairment at work | −40.1 | p < 0.008 | −11.3 | p = 0.043 | −46.9 | p < 0.001 |
| 6. Regular activity impairment | −37.7 | p < 0.000 | −8.8 | p = 0.088 | −43.2 | p < 0.001 |
| Spearman’s Test | ||||||||
|---|---|---|---|---|---|---|---|---|
| SF-36 | ||||||||
| ΔWBC | ΔNeu | ΔLimph | ΔCRP | Δalpha1 | ΔHb | ΔMCV | ΔMCH | |
| 1. ΔPhysical functioning | rs 0.301 p = 0.038 | |||||||
| 2. ΔPhysical health | rs 0.418 p = 0.004 | rs 0.555 p = 0.002 | rs −0.496 p = 0.014 | rs 0.583 p = 0.003 | ||||
| 3. ΔMental health | ||||||||
| 4. ΔVitality | ||||||||
| 5. ΔEmotional role | rs 0.315 p = 0.026 | rs −0.311 p = 0.028 | rs −0.248 p < 0.05 | rs −0.349 p < 0.01 | ||||
| 6. ΔSocial functioning | ||||||||
| 7. ΔBody pain | ||||||||
| 8. ΔGeneral health | rs −0.254 p < 0.05 | rs −0.266 p < 0.05 | ||||||
| FACIT-F | ||||||||
| ΔWBC | ΔNeu | ΔLimph | ΔCRP | Δalpha1 | ΔHb | ΔMCV | ΔMCH | |
| 1. ΔPhysical well-being | rs 0.370 p = 0.008 | rs −0.348 p < 0.01 | ||||||
| 2. ΔSocial/family well-being | ||||||||
| 3. ΔEmotional well-being | ||||||||
| 4. ΔFunctional well-being | ||||||||
| 5. ΔAdditional concerns (FACIT-FS) | ||||||||
| 6. ΔFACIT-G | rs 0.303 p = 0.032 | rs −0.344 p = 0.014 | ||||||
| 7. ΔFACIT-GH | rs −0.369 p = 0.008 | |||||||
| WPAI:GH | ||||||||
| ΔWBC | ΔNeu | ΔLimph | ΔCRP | Δalpha1 | ΔHb | ΔMCV | ΔMCH | |
| 2. ΔWork time missed (health) | rs 0.634 p < 0.001 | rs 0.857 p < 0.001 | ||||||
| 3. ΔWork time missed (other) | rs −0.515 p = 0.002 | rs 0.488 p = 0.003 | ||||||
| 4. ΔEffective worked hours | rs −0.437 p = 0.003 | |||||||
| 5. ΔImpairment at work | rs −0.496 p = 0.002 | |||||||
| 6. ΔRegular activity impairment | ||||||||
| Serum Parameters | Spearman’s Test | |
|---|---|---|
| Alpha1 globulins | WBC | rs −0.379, p = 0.007 |
| Alpha1 globulins | ESR | rs 0.458, p = 0.001 |
| Alpha1 | Alpha2 globulins | rs 0.501, p = 0.000 |
| ESR | CRP | rs 0.305, p = 0.031 |
| MCV | MCH | rs 0.757, p = 0.000 |
| MCV | Hb | rs 0.315, p = 0.026 |
| MCH | Hb | rs 0.477, p= 0.000 |
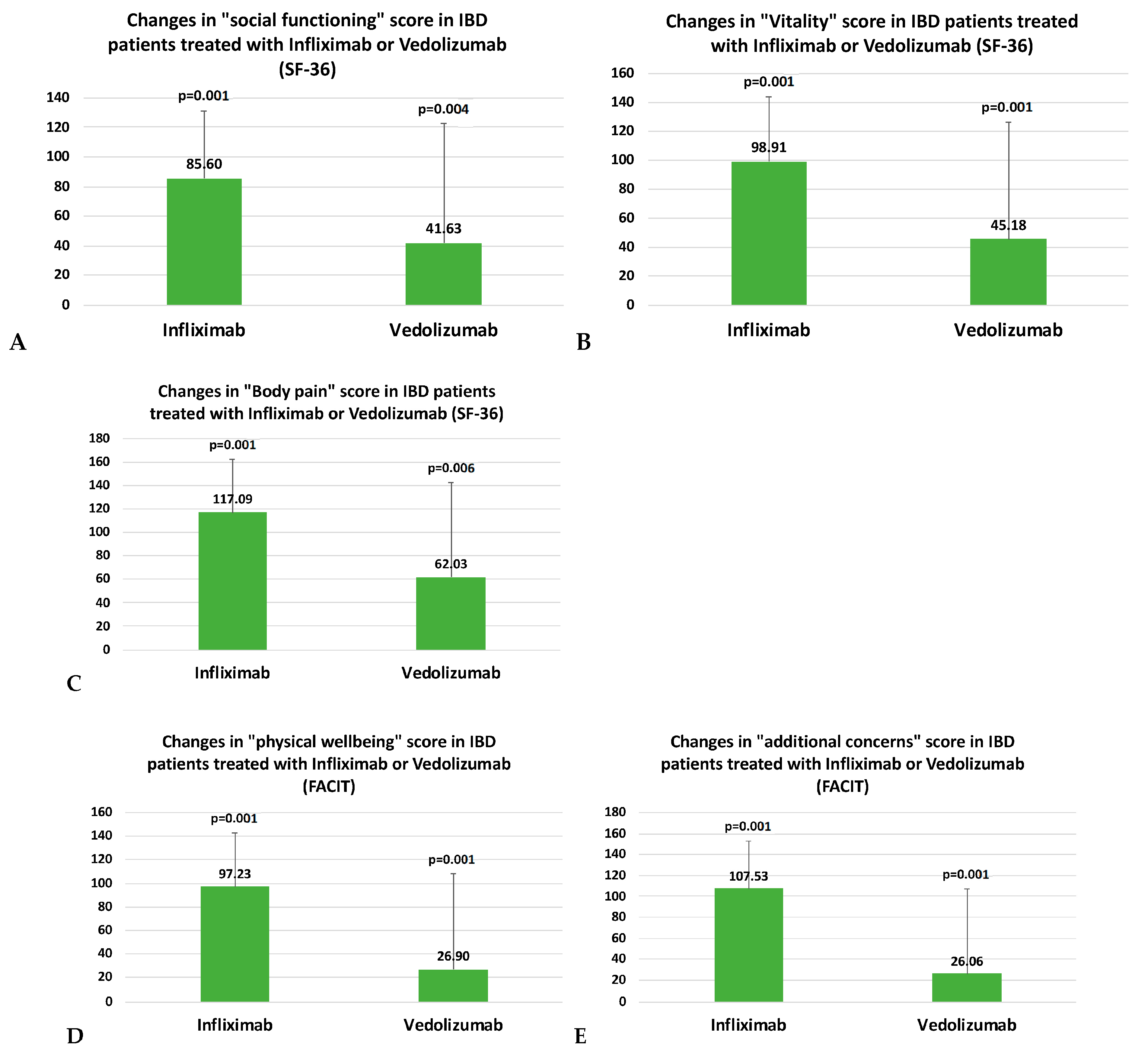
| Infliximab | W | Vedolizumab | W | MW | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SF-36 | T0 | T1 | T2 | Δ1% | Δ2% | p | T0 | T1 | T2 | Δ1% | Δ2% | p | p |
| 4. | 40 (36.2) | 60 (22.5) | 63.6 (25) | 49.7 | 60.8 | 0.000 | 42.5 (18.75) | 55 (22.5) | 50 (15) | 25.8 | 23.1 | 0.001 | 0.001 |
| 6. | 43.75 (40.6) | 68.8 (37.5) | 75 (37.5) | 48.0 | 61.0 | 0.001 | 50 (25) | 50 (37.5) | 52.5 (32.5) | 23.0 | 24.7 | 0.004 | 0.001 |
| 7. | 35 (53.1) | 67.5 (30.6) | 77.5 (45) | 65.8 | 77.2 | 0.000 | 45 (31.8) | 55 (30) | 53.7 (19.4) | 40 | 28.2 | 0.006 | 0.001 |
| FACIT-F | T0 | T1 | T2 | Δ1% | Δ2% | p | T0 | T1 | T2 | Δ1% | Δ2% | p | p |
| 1. | 17.5 (13.5) | 24 (3) | 25 (5) | 37.4 | 45.6 | 0.000 | 20 (9.5) | 23.5 (6) | 24 (5.5) | 17.6 | 21 | 0.000 | 0.001 |
| 5. | 31.5 (21.5) | 42 (10.5) | 43 (10.2) | 43 | 50.7 | 0.000 | 30.5 (16.2) | 38.5 (8.5) | 39 (13.2) | 22.2 | 19.2 | 0.001 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bellone, F.; Morace, C.; Impalà, G.; Viola, A.; Gullo, A.L.; Cinquegrani, M.; Fries, W.; Sardella, A.; Scolaro, M.; Basile, G.; et al. Quality of Life (QoL) in Patients with Chronic Inflammatory Bowel Diseases: How Much Better with Biological Drugs? J. Pers. Med. 2023, 13, 947. https://doi.org/10.3390/jpm13060947
Bellone F, Morace C, Impalà G, Viola A, Gullo AL, Cinquegrani M, Fries W, Sardella A, Scolaro M, Basile G, et al. Quality of Life (QoL) in Patients with Chronic Inflammatory Bowel Diseases: How Much Better with Biological Drugs? Journal of Personalized Medicine. 2023; 13(6):947. https://doi.org/10.3390/jpm13060947
Chicago/Turabian StyleBellone, Federica, Carmela Morace, Giulia Impalà, Anna Viola, Alberto Lo Gullo, Maria Cinquegrani, Walter Fries, Alberto Sardella, Mariangela Scolaro, Giorgio Basile, and et al. 2023. "Quality of Life (QoL) in Patients with Chronic Inflammatory Bowel Diseases: How Much Better with Biological Drugs?" Journal of Personalized Medicine 13, no. 6: 947. https://doi.org/10.3390/jpm13060947
APA StyleBellone, F., Morace, C., Impalà, G., Viola, A., Gullo, A. L., Cinquegrani, M., Fries, W., Sardella, A., Scolaro, M., Basile, G., Squadrito, G., & Mandraffino, G. (2023). Quality of Life (QoL) in Patients with Chronic Inflammatory Bowel Diseases: How Much Better with Biological Drugs? Journal of Personalized Medicine, 13(6), 947. https://doi.org/10.3390/jpm13060947