
A Review of the Role of Artificial Intelligence in Healthcare

 , ,
, ,  ,
,
Abstract
:1. Introduction
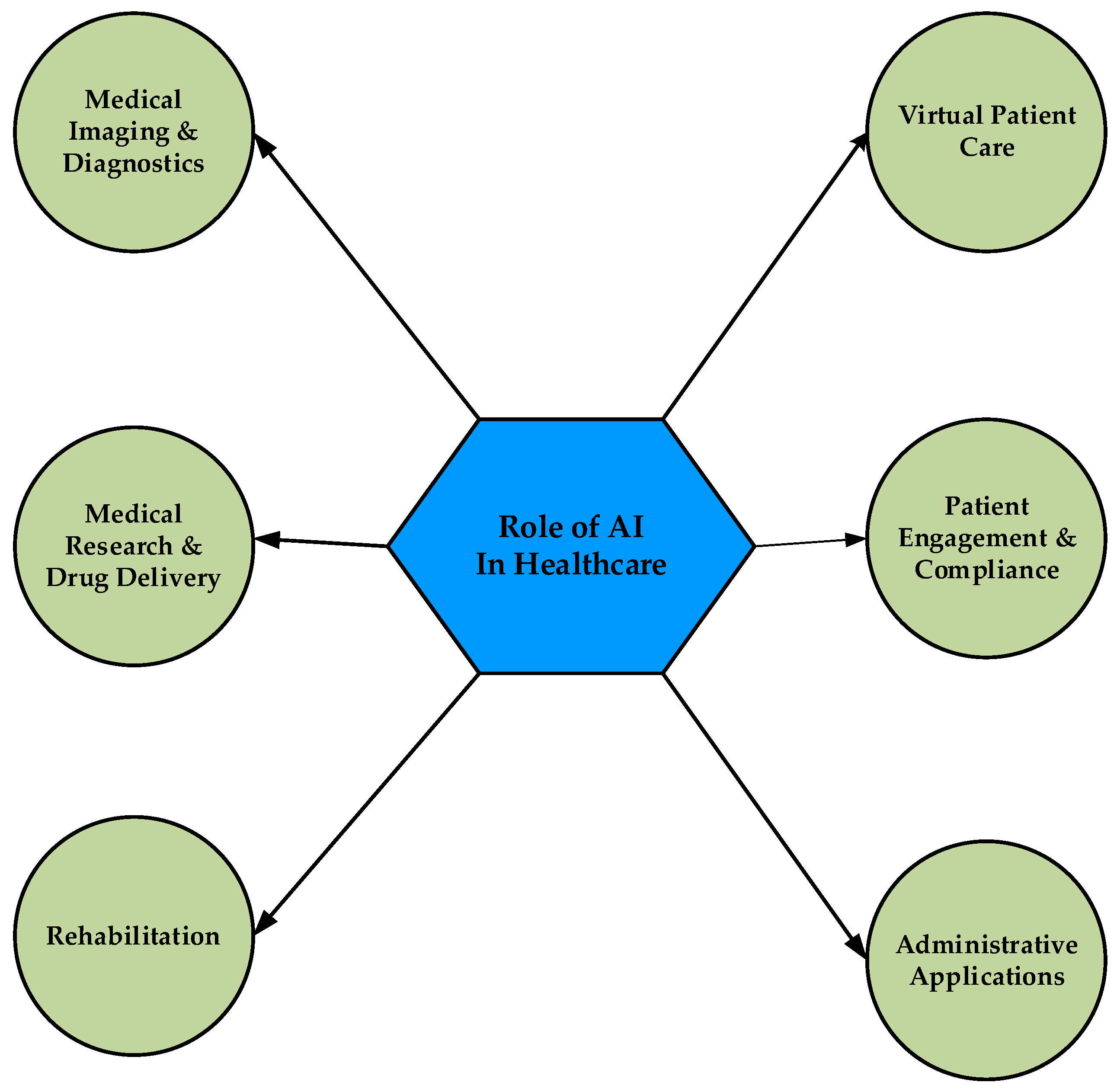
2. Role of AI in Healthcare
2.1. Medical Imaging and Diagnostic Services
2.2. Virtual Patient Care
2.3. Medical Research and Drug Discovery
2.4. Patient Engagement and Compliance
2.5. Rehabilitation
2.6. Administrative Applications
3. Challenges Faced by AI Utilization in Healthcare
3.1. Ethical and Social Challenges
3.2. Governance Challenges
3.3. Technical Challenges
4. Disadvantages of AI in Healthcare
5. Conclusions
Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Snowdon, A. Digital Health: A Framework for Healthcare Transformation. 2020. Available online: https://www.gs1ca.org/documents/digital_health-affht.pdf (accessed on 23 January 2023).
- Williams, O.D. COVID-19 and Private Health: Market and Governance Failure. Development 2020, 63, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Tabriz, A.A.; Nouri, E.; Vu, H.T.; Nghiem, V.T.; Bettilyon, B.; Gholamhoseyni, P.; Kiapour, N. What should accountable care organizations learn from the failure of health maintenance organizations? A theory based systematic review of the literature. Soc. Determ. Health 2017, 3, 222–247. [Google Scholar] [CrossRef]
- Rand Review. Chronic Conditions in America: Price and Prevalence. 2017. Available online: https://www.rand.org/blog/rand-review/2017/07/chronic-conditions-in-america-price-and-prevalence.html (accessed on 11 July 2021).
- World Health Organization. Naming the Coronavirus Disease (COVID-19) and the Virus that Causes It. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(COVID-2019)-and-the-virus-that-causes-it (accessed on 6 July 2021).
- Butcher, C.J.T.; Hussain, W. Digital Healthcare: The Future, RCP Journals. Royal College of Physicians. 2022. Available online: https://www.rcpjournals.org/content/futurehosp/9/2/113 (accessed on 16 January 2023).
- Siriwardhana, Y.; Gür, G.; Ylianttila, M.; Liyanage, M. The role of 5G for digital healthcare against COVID-19 pandemic: Opportunities and challenges. ICT Express 2020, 7, 244–252. [Google Scholar] [CrossRef]
- Shakeel, T.; Habib, S.; Boulila, W.; Koubaa, A.; Javed, A.R.; Rizwan, M.; Gadekallu, T.R.; Sufiyan, M. A survey on COVID-19 impact in the healthcare domain: Worldwide market implementation, applications, security and privacy issues, challenges and future prospects. Complex Intell. Syst. 2022, 9, 1027–1058. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Lee, D. Opportunities and challenges for contactless healthcare services in the post-COVID-19 Era. Technol. Forecast. Soc. Chang. 2021, 167, 120712. [Google Scholar] [CrossRef]
- Carroll, W.M. Digital health and new technologies. In Nursing and Informatics for the 21st Century Embracing a Digital World, 3rd ed.; Productivity Press: New York, NY, USA, 2022; pp. 29–48. [Google Scholar]
- Mistry, C.; Thakker, U.; Gupta, R.; Obaidat, M.S.; Tanwar, S.; Kumar, N.; Rodrigues, J.J.P.C. MedBlock: An AI-enabled and blockchain-driven medical healthcare system for COVID-19. In Proceedings of the IEEE International Conference Communication, Montreal, QC, Canada, 14–23 June 2021; pp. 1–6. [Google Scholar] [CrossRef]
- Ng, R.; Tan, K.B. Implementing an Individual-Centric Discharge Process across Singapore Public Hospitals. Int. J. Environ. Res. Public Health 2021, 18, 8700. [Google Scholar] [CrossRef]
- Bajwa, J.; Munir, U.; Nori, A.; Williams, B. Artificial intelligence in healthcare: Transforming the practice of medicine. Future Healthcare J. 2021, 8, e188–e194. [Google Scholar] [CrossRef]
- Tagliaferri, S.D.; Angelova, M.; Zhao, X.; Owen, P.J.; Miller, C.T.; Wilkin, T.; Belavy, D.L. Artificial intelligence to improve back pain outcomes and lessons learnt from clinical classification approaches: Three systematic reviews. npj Digit. Med. 2020, 3, 1–16. [Google Scholar] [CrossRef]
- Tran, B.X.; Vu, G.T.; Ha, G.H.; Vuong, Q.-H.; Ho, M.-T.; Vuong, T.-T.; La, V.-P.; Ho, M.-T.; Nghiem, K.-C.P.; Nguyen, H.L.T.; et al. Global Evolution of Research in Artificial Intelligence in Health and Medicine: A Bibliometric Study. J. Clin. Med. 2019, 8, 360. [Google Scholar] [CrossRef] [Green Version]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial intelligence in healthcare: Past, present and future. Stroke Vasc. Neurol. 2017, 2, 230–243. [Google Scholar] [CrossRef] [Green Version]
- Javaid, M.; Haleem, A.; Singh, R.P.; Suman, R.; Rab, S. Significance of machine learning in healthcare: Features, pillars and applications. Int. J. Intell. Networks 2022, 3, 58–73. [Google Scholar] [CrossRef]
- Coursera. What Is Machine Learning in Health Care? Applications and Opportunities. 2022. Available online: https://www.coursera.org/articles/machine-learning-in-health-care (accessed on 30 March 2023).
- Hashimy, L.; Treiblmaier, H.; Jain, G. Distributed ledger technology as a catalyst for open innovation adoption among small and medium-sized enterprises. J. High Technol. Manag. Res. 2021, 32, 100405. [Google Scholar] [CrossRef]
- Stampa, K. How Distributed Ledger Technology Will Transform Health Data. Healthcare. 2020. Available online: https://healthcare-digital.com/technology-and-ai/how-distributed-ledger-technology-will-transform-health-data (accessed on 30 March 2023).
- Alruwaili, F.F. Artificial intelligence and multi agent based distributed ledger system for better privacy and security of electronic healthcare records. PeerJ Comput. Sci. 2020, 6, e323. [Google Scholar] [CrossRef] [PubMed]
- Sadiku, M.N.O.; Zhou, Y.; Musa, S.M. Natural Language Processing. Int. J. Adv. Sci. Res. Eng. 2018, 4, 68–70. [Google Scholar] [CrossRef]
- Iroju, O.G.; Olaleke, J.O. A Systematic Review of Natural Language Processing in Healthcare. Int. J. Inf. Technol. Comput. Sci. 2015, 7, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Trunfio, M.; Rossi, S. Advances in Metaverse Investigation: Streams of Research and Future Agenda. Virtual Worlds 2022, 1, 103–129. [Google Scholar] [CrossRef]
- Park, S.-M.; Kim, Y.-G. A metaverse: Taxonomy, components, applications, and open challenges. IEEE Access 2022, 10, 4209–4251. [Google Scholar] [CrossRef]
- Petrigna, L.; Musumeci, G. The Metaverse: A New Challenge for the Healthcare System: A Scoping Review. J. Funct. Morphol. Kinesiol. 2022, 7, 63. [Google Scholar] [CrossRef] [PubMed]
- Thomason, J. MetaHealth-How will the Metaverse Change Health Care? J. Metaverse 2021, 1, 13–16. Available online: https://dergipark.org.tr/en/download/article-file/2167692 (accessed on 31 December 2022).
- Hassani, H.; Silva, E.S. The Role of ChatGPT in Data Science: How AI-Assisted Conversational Interfaces Are Revolutionizing the Field. Big Data and Cogn. Comput. 2023, 7, 62. [Google Scholar] [CrossRef]
- Sallam, M. ChatGPT Utility in Healthcare Education, Research, and Practice: Systematic Review on the Promising Perspectives and Valid Concerns. Healthcare 2023, 11, 887. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Sanders, L.; Li, K.; Chow, J.C.L. Chatbot for Health Care and Oncology Applications Using Artificial Intelligence and Machine Learning: Systematic Review. JMIR Cancer 2021, 7, e27850. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.; Wang, Y.; Liu, X.; Qiu, X. A survey of transformers. AI Open 2022, 3, 111–132. [Google Scholar] [CrossRef]
- Li, Y.; Rao, S.; Solares, J.R.A.; Hassaine, A.; Ramakrishnan, R.; Canoy, D.; Zhu, Y.; Rahimi, K.; Salimi-Khorshidi, G. BEHRT: Transformer for Electronic Health Records. Sci. Rep. 2020, 10, 7155. [Google Scholar] [CrossRef] [PubMed]
- Shome, D.; Kar, T.; Mohanty, S.N.; Tiwari, P.; Muhammad, K.; AlTameem, A.; Zhang, Y.; Saudagar, A.K.J. COVID-Transformer: Interpretable COVID-19 Detection Using Vision Transformer for Healthcare. Int. J. Environ. Res. Public Health 2021, 18, 11086. [Google Scholar] [CrossRef]
- He, K.; Gan, C.; Li, Z.; Rekik, I.; Yin, Z.; Ji, W.; Gao, Y.; Wang, Q.; Zhang, J.; Shen, D. Transformers in medical image analysis. Intell. Med. 2023, 3, 59–78. [Google Scholar] [CrossRef]
- Li, Y.; Mamouei, M.; Salimi-Khorshidi, G.; Rao, S.; Hassaine, A.; Canoy, D.; Lukasiewicz, T.; Rahimi, K. Hi-BEHRT: Hierarchical Transformer-Based Model for Accurate Prediction of Clinical Events Using Multimodal Longitudinal Electronic Health Records. IEEE J. Biomed. Health Inform. 2023, 27, 1106–1117. Available online: https://ieeexplore.ieee.org/stamp/stamp.jsp?arnumber=9964038 (accessed on 10 May 2023). [CrossRef]
- Shamshad, F.; Khan, S.; Zamir, S.W.; Khan, M.H.; Hayat, M.; Khan, F.S.; Fu, H. Transformers in medical imaging: A survey. Med. Image Anal. 2023, 102802. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration (US-FDA). What Is Digital Health. 2020. Available online: https://www.fda.gov/medical-devices/digital-health-center-excellence/what-digital-health (accessed on 11 July 2021).
- Yang, Y.; Siau, K.; Xie, W.; Sun, Y. Smart Health. J. Organ. End User Comput. 2022, 34, 1–14. [Google Scholar] [CrossRef]
- Kumar, K.; Loebinger, M.R.; Ghafur, S. The role of wirelessly observed therapy in improving treatment adherence. Futur. Healthcare J. 2022, 9, 179–182. [Google Scholar] [CrossRef]
- Kumar, A.; Gadag, S.; Nayak, U.Y. The Beginning of a New Era: Artificial Intelligence in Healthcare. Adv. Pharm. Bull. 2020, 11, 414–425. [Google Scholar] [CrossRef]
- Wallace, P. Learning Healthcare System. The Learning Healthcare Project. 2015. Available online: http://www.learninghealthcareproject.org/section/evidence/25/66/dr-paul-wallace-interview (accessed on 10 July 2022).
- Orth, M.; Averina, M.; Chatzipanagiotou, S.; Faure, G.; Haushofer, A.; Kusec, V.; Machado, A.; A Misbah, S.; Oosterhuis, W.; Pulkki, K.; et al. Opinion: Redefining the role of the physician in laboratory medicine in the context of emerging technologies, personalised medicine and patient autonomy (‘4P medicine’). J. Clin. Pathol. 2017, 72, 191–197. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Strategy on Digital Health 2020–2025. 2021, pp. 7–13. Available online: https://www.who.int/docs/defaultsource/documents/gs4dhdaa2a9f352b0445bafbc79ca799dce4d.pdf (accessed on 10 December 2022).
- Briganti, G.; Le Moine, O. Artificial Intelligence in Medicine: Today and Tomorrow. Front. Med. 2020, 7, 27. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Perer, A.; Wang, F. Data driven analytics for personalized healthcare. In Healthcare Information Management Systems; Weaver, C.B.M., Ed.; Springer: Berlin/Heidelberg, Germany, 2016; pp. 529–554. [Google Scholar]
- Dash, S.; Shakyawar, S.K.; Sharma, M.; Kaushik, S. Big data in healthcare: Management, analysis and future prospects. J. Big Data 2019, 6, 54. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Ma, R.; Sun, S.; Li, Y.; Wang, Y.; Yan, Z. Optimizing the Electronic Health Records Through Big Data Analytics: A Knowledge-Based View. IEEE Access 2019, 7, 136223–136231. [Google Scholar] [CrossRef]
- Rawat, S. How Is Big Data Analytics Using AI? 2021. Available online: https://www.analyticssteps.com/blogs/how-big-data-analytics-using-ai (accessed on 11 January 2023).
- Ghosh, P. AI Early Diagnosis Could Save Heart and Cancer Patients. Science Correspondent. BBC News. 2018. Available online: https://www.bbc.com/news/health-42357257 (accessed on 11 July 2021).
- Wang, D.; Khosla, A.; Gargeya, R.; Irshad, H.; Beck, A.H. Deep learning for identifying metastatic breast cancer. arXiv 2016, arXiv:1606.05718. [Google Scholar]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; Ding, D.; Bagul, A.; Langlotz, C.; Shpanskaya, K.; et al. Chexnet: Radiologist-level pneumonia detection on chest x-rays with deep learning. arXiv 2017, arXiv:1711.05225. [Google Scholar]
- Bedi, G.; Carrillo, F.; Cecchi, G.A.; Slezak, D.F.; Sigman, M.; Mota, N.B.; Ribeiro, S.; Javitt, D.C.; Copelli, M.; Corcoran, C.M. Automated analysis of free speech predicts psychosis onset in high-risk youths. NPJ Schitzophrenia 2015, 1, 15030. [Google Scholar] [CrossRef] [Green Version]
- IBM Research. IBM 5 in 5: With AI, Our Words Will Be a Window into Our Mental Health. 2017. Available online: https://www.ibm.com/blogs/research/2017/1/ibm-5-in-5-our-words-will-be-the-windows-to-our-mental-health/ (accessed on 25 December 2022).
- Chou, C.-Y.; Hsu, D.-Y.; Chou, C.-H. Predicting the Onset of Diabetes with Machine Learning Methods. J. Pers. Med. 2023, 13, 406. [Google Scholar] [CrossRef]
- Gudigar, A.; Raghavendra, U.; Nayak, S.; Ooi, C.P.; Chan, W.Y.; Gangavarapu, M.R.; Dharmik, C.; Samanth, J.; Kadri, N.A.; Hasikin, K.; et al. Role of Artificial Intelligence in COVID-19 Detection. Sensors 2021, 21, 8045. [Google Scholar] [CrossRef] [PubMed]
- Khanna, V.V.; Chadaga, K.; Sampathila, N.; Prabhu, S.; Chadaga, R.; Umakanth, S. Diagnosing COVID-19 using artificial intelligence: A comprehensive review. Netw. Model Anal Health Inf. Bioinforma 2022, 11, 25. [Google Scholar] [CrossRef]
- Costa, G.S.S.; Paiva, A.C.; Junior, G.B.; Ferreira, M.M. COVID-19 automatic diagnosis with ct images using the novel transformer architecture. In Proceedings of the 21st Brazilian Symposium on Computing Applied to Health, Rio de Janeiro, Brazil, 15–18 June 2021; pp. 293–301. [Google Scholar]
- van Tulder, G.; Tong, Y.; EMarchiori, E. Multi-view analysis of unregistered medical images using cross-view transformers. In Proceedings of the Medical Image Computing and Computer Assisted Intervention–MICCAI 2021: 24th International Conference, Part III 24, Strasbourg, France, 27 September–1 October 2021; Springer Nature: Basel, Switzerland, 2021; pp. 104–113. [Google Scholar]
- Krishnan, K.S.; Krishnan, K.S. Vision transformer based COVID-19 detection using chest x-rays. In Proceedings of the 2021 6th International Conference on Signal Processing, Computing and Control (ISPCC), Solan, India, 7–9 October 2021; pp. 644–648. [Google Scholar] [CrossRef]
- Wang, S.-H.; Wu, X.; Zhang, Y.-D.; Tang, C.; Zhang, X. Diagnosis of COVID-19 by Wavelet Renyi Entropy and Three-Segment Biogeography-Based Optimization. Int. J. Comput. Intell. Syst. 2020, 13, 1332–1344. [Google Scholar] [CrossRef]
- Gheflati, B.; Rivaz, H. Vision transformer for classification of breast ultrasound images. arXiv 2021, arXiv:211014731. [Google Scholar] [CrossRef]
- Wolterink, J.M.; Mukhopadhyay, A.; Leiner, T.; Vogl, T.J.; Bucher, A.M.; Išgum, I. Generative Adversarial Networks: A Primer for Radiologists. RadioGraphics 2021, 41, 840–857. [Google Scholar] [CrossRef]
- Chuquicusma, M.J.M.; Hussein, S.; Burt, J.; Bagci, U. How to fool radiologists with generative adversarial networks? A visual turing test for lung cancer diagnosis. In Proceedings of the IEEE 15th International Symposium on Biomedical Imaging, Washington, DC, USA, 4–7 April 2018; pp. 240–244. [Google Scholar]
- Arora, A.; Arora, A. Generative adversarial networks and synthetic patient data: Current challenges and future perspectives. Futur. Healthcare J. 2022, 9, 190–193. [Google Scholar] [CrossRef]
- Will ChatGPT transform healthcare? Nat. Med. 2023, 29, 505–506. [CrossRef]
- Kuehn, B.M. More Than One-Third of US Individuals Use the Internet to Self-diagnose. JAMA 2013, 309, 756–757. [Google Scholar] [CrossRef]
- Wang, G.; Badal, A.; Jia, X.; Maltz, J.S.; Mueller, K.; Myers, K.J.; Niu, C.; Vannier, M.; Yan, P.; Yu, Z.; et al. Development of metaverse for intelligent healthcare. Nat. Mach. Intell. 2022, 4, 922–929. [Google Scholar] [CrossRef]
- Nuffield Council on Bioethics. Artificial Intelligence (AI) in Healthcare and Research. Nuffield Council on Bioethics. 2018. Available online: https://www.nuffieldbioethics.org/assets/pdfs/Artificial-Intelligence-AI-in-healthcare-and-research.pdf (accessed on 11 December 2022).
- House of Lords. AI in the UK: Ready, Willing and Able? House of Lords Select Committee on Artificial Intelligence: Report of Session 2017–2019. Authority of the House of Lords. 2018. Available online: https://publications.parliament.uk/pa/ld201719/ldselect/ldai/100/100.pdf (accessed on 16 December 2022).
- Secinaro, S.; Calandra, D.; Secinaro, A.; Muthurangu, V.; Biancone, P. The role of artificial intelligence in healthcare: A structured literature review. BMC Med. Inform. Decis. Mak. 2021, 21, 1–23. [Google Scholar] [CrossRef]
- Oren, O.; Gersh, B.J.; Bhatt, D.L. Artificial intelligence in medical imaging: Switching from radiographic pathological data to clinically meaningful endpoints. Lancet Digit. Health 2020, 2, e486–e488. [Google Scholar] [CrossRef] [PubMed]
- Baig, M.M.; GholamHosseini, H.; Moqeem, A.A.; Mirza, F.; Lindén, M. A Systematic Review of Wearable Patient Monitoring Systems–Current Challenges and Opportunities for Clinical Adoption. J. Med. Syst. 2017, 41, 115. [Google Scholar] [CrossRef]
- Kim, J.; Campbell, A.S.; Wang, J. Wearable non-invasive epidermal glucose sensors: A review. Talanta 2018, 177, 163–170. [Google Scholar] [CrossRef]
- Andrea, M.; Mario, R.P.; Emanuele, F.; Sauro, L.; Filippo, P.; Sara, C.; Lorenzo, S.; Annalisa, C.; Luca, R.; Riccardo, B.; et al. A smart sensing architecture for domestic monitoring: Methodological approach and experimental validation. Sensors 2018, 18, 1–22. [Google Scholar]
- Patel, D.; Tarakji, K.G. Smartwatch diagnosis of atrial fibrillation in patient with embolic stroke of unknown source: A case report. Cardiovasc. Digit. Health J. 2021, 2, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Sükei, E.; Norbury, A.; Perez-Rodriguez, M.M.; Olmos, P.M.; Artés, A. Predicting Emotional States Using Behavioral Markers Derived From Passively Sensed Data: Data-Driven Machine Learning Approach. JMIR mHealth uHealth 2021, 9, e24465. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, A.; Su, H.-W.; Heneghan, C. Assessment of physiological signs associated with COVID-19 measured using wearable devices. NPJ Digit. Med. 2020, 3, 1–8. [Google Scholar] [CrossRef]
- Bogu, G.; Snyder, M. Deep learning-based detection of COVID-19 using wearables data. Deep Learning-Based Detection of COVID-19 Using Wearables Data. MedRxiv 2021. [Google Scholar] [CrossRef]
- Tschopp, J.; L’Huillier, A.G.; Mombelli, M.; Mueller, N.J.; Khanna, N.; Garzoni, C.; Meloni, D.; Papadimitriou-Olivgeris, M.; Neofytos, D.; Hirsch, H.H.; et al. First experience of SARS-CoV-2 infections in solid organ transplant recipients in the Swiss Transplant Cohort Study. Am. J. Transplant. 2020, 20, 2876–2886. [Google Scholar] [CrossRef]
- Yu, M.; Tang, A.; Brown, K.; Bouchakri, R.; St-Onge, P.; Wu, S.; Reeder, J.; Mullie, L.; Chassé, M. Integrating artificial intelligence in bedside care for COVID-19 and future pandemics. BMJ 2021, 375, e068197. [Google Scholar] [CrossRef]
- Garavand, A.; Aslani, N. Metaverse phenomenon and its impact on health: A scoping review. Inform. Med. Unlocked 2022, 32, 101029. [Google Scholar] [CrossRef]
- Ganapathy, K. Telemedicine and Neurological Practice in the COVID-19 Era. Neurol. India 2020, 68, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Lukas, H.; Xu, C.; Yu, Y.; Gao, W. Emerging telemedicine tools for remote COVID-19 diagnosis, monitoring, and management. ACS Nano 2020, 14, 16180–16193. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Zhang, R. Exploring Research Trends of Emerging Technologies in Health Metaverse: A Bibliometric Analysis; Elsevier: Amsterdam, The Netherlands, 2022. [Google Scholar] [CrossRef]
- Gadekallu, T.R.; Huynh-The, T.; Wang, W.; Yenduri, G.; Ranaweera, P.; Pham, Q.-V.; da Costa, D.B.; Liyange, M. Blockchain for the metaverse: A review. arXiv 2022, arXiv:2203.09738. [Google Scholar]
- Chengoden, R.; Victor, N.; Huynh-The, T.; Yenduri, G.; Jhaveri, R.H.; Alazab, M.; Bhattacharya, S.; Hegde, P.; Maddikunta, P.K.R.; Gadekallu, T.R. Metaverse for Healthcare: A Survey on Potential Applications, Challenges and Future Directions. IEEE Access 2023, 11, 12765–12795. [Google Scholar] [CrossRef]
- Futurside. Remote Patient Monitoring Devices, Technology, and Its Future. 2022. Available online: https://futurside.com/how-wearable-medical-device-is-reshaping-remote-patient-monitoring-rpm/ (accessed on 11 January 2023).
- Shaik, T.; Tao, X.; Higgins, N.; Li, L.; Gururajan, R.; Zhou, X.; Acharya, U.R. Remote patient monitoring using artificial intelligence: Current state, applications, and challenges. WIREs Data Min. Knowl. Discov. 2023, 13, 1485. [Google Scholar] [CrossRef]
- Bouabida, K.; Malas, K.; Talbot, A.; Desrosiers, M.; Lavoie, F.; Lebouché, B.; Taguemout, M.; Rafie, E.; Lessard, D.; Pomey, M.-P. Remote Patient Monitoring Program for COVID-19 Patients Following Hospital Discharge: A Cross-Sectional Study. Front. Digit. Health 2021, 3, 153. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A.; Singh, R.P. ChatGPT for healthcare services: An emerging stage for an innovative perspective. BenchCouncil Trans. Benchmarks Stand. Eval. 2023, 3, 100105. [Google Scholar] [CrossRef]
- Academy of Royal Medical Colleges. Artificial Intelligence in Healthcare. 2019. Available online: https://www.aomrc.org.uk/wpcontent/uploads/2019/01/Artificial_intelligence_in_healthcare_0119.pdf (accessed on 11 January 2023).
- O’mara-Eves, A.; Thomas, J.; McNaught, J.; Miwa, M.; Ananiadou, S. Using text mining for study identification in systematic reviews: A systematic review of current approaches. Syst. Rev. 2015, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Weissler, E.H.; Naumann, T.; Andersson, T.; Ranganath, R.; Elemento, O.; Luo, Y.; Freitag, D.F.; Benoit, J.; Hughes, M.C.; Khan, F.; et al. The role of machine learning in clinical research: Transforming the future of evidence generation. Trials 2021, 22, 1–15. [Google Scholar] [CrossRef]
- Suh, I.; McKinney, T.; Siu, K.-C. Current Perspective of Metaverse Application in Medical Education, Research and Patient Care. Virtual Worlds 2023, 2, 115–128. [Google Scholar] [CrossRef]
- Khan, R.A.; Jawaid, M.; Khan, A.R.; Sajjad, M. ChatGPT-Reshaping medical education and clinical management. Pak. J. Med. Sci. 2023, 39, 7653. [Google Scholar] [CrossRef] [PubMed]
- Buvailo, A. Artificial Intelligence in Drug Discovery and Biotech: 2022 Recap and Key Trends. 2022. Available online: https://www.biopharmatrend.com/post/615-pharmaceutical-artificial-intelligence-key-developments-in-2022/ (accessed on 31 January 2023).
- Son, W.S. Drug Discovery Enhanced by Artificial Intelligence. Biomed. J. Sci. Tech. Res. 2018, 12, 8936–8938. [Google Scholar] [CrossRef]
- Williams, K.; Bilsland, E.; Sparkes, A.; Aubrey, W.; Young, M.; Soldatova, L.N.; De Grave, K.; Ramon, J.; de Clare, M.; Sirawaraporn, W.; et al. Cheaper faster drug development validated by the repositioning of drugs against neglected tropical diseases. J. R. Soc. Interface 2015, 12, 20141289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, K.-K.; Pichika, M.R. Artificial intelligence in drug development: Present status and future prospects. Drug Discov. Today 2019, 24, 773–780. [Google Scholar] [CrossRef]
- Sellwood, M.A. Artificial intelligence in drug discovery. Fut. Sci. 2018, 10, 2025–2028. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.-J. ChatGPT and other artificial intelligence applications speed up scientific writing. J. Chin. Med. Assoc. 2023, 86, 351–353. [Google Scholar] [CrossRef]
- Taecharungroj, V. “What Can ChatGPT Do?” Analyzing Early Reactions to the Innovative AI Chatbot on Twitter. Big Data Cogn. Comput. 2023, 7, 35. [Google Scholar] [CrossRef]
- Paul, D.; Sanap, G.; Shenoy, S.; Kalyane, D.; Kalia, K.; Tekade, R.K. Artificial intelligence in drug discovery and development. Drug Discov. Today 2020, 26, 80–93. [Google Scholar] [CrossRef]
- Álvarez-Machancoses, O.; Fernández-Martínez, J.L. Using artificial intelligence methods to speed up drug discovery. Expert Opin. Drug Discov. 2019, 14, 769–777. [Google Scholar] [CrossRef]
- Dana, D.; Gadhiya, S.V.; St. Surin, L.G.; Li, D.; Naaz, F.; Ali, Q.; Paka, L.; Yamin, M.A.; Narayan, M.; Goldberg, I.D.; et al. Deep Learning in Drug Discovery and Medicine; Scratching the Surface. Molecules 2018, 23, 2384. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Virmani, T.; Pathak, V.; Sharma, A.; Pathak, K.; Kumar, G.; Pathak, D. Artificial Intelligence-Based Data-Driven Strategy to Accelerate Research, Development, and Clinical Trials of COVID Vaccine. Biomed Res Int. 2022, 2022, 7205241. [Google Scholar] [CrossRef] [PubMed]
- Bagabir, S.A.; Ibrahim, N.K.; Ateeq, R.H. COVID-19 and Artificial Intelligence: Genome sequencing, drug development and vaccine discovery. J. Infect. Public Health 2022, 15, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Davenport, T.; Kalakota, R. The potential for artificial intelligence in healthcare. Future Healthcare J. 2019, 6, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Davenport, T.H.; Hongsermeier, T.; Mc Cord, K.A. Using AI to Improve Electronic Health Records. Harvard Business Review. 2018. Available online: https://hbr.org/2018/12/using-ai-to-improve-electronic-health-records (accessed on 28 December 2022).
- Volpp, K.; Mohta, S. Improved Engagement Leads to Better Outcomes, But Better Tools Are Needed. Insights Report. NEJM Catalyst. 2016. Available online: https://catalyst.nejm.org/patient-engagementreport-improved-engagement-leads-better-outcomes-better-toolsneeded (accessed on 15 January 2023).
- Hukunda, B.; Rau, A.; Upadhyay, P. Reimaging Healthcare Opportunities with Artificial Intelligence. Infosys Navigate Your Next. 2018. Available online: https://www.infosys.com/industries/healthcare/featuresopinions/Documents/reimagining-healthcare-opportunities.pdf (accessed on 10 January 2023).
- Anderson, D. Artificial Intelligence and Applications in PM&R. Am. J. Phys. Med. Rehabil. 2019, 98, e128–e129. [Google Scholar] [CrossRef]
- Luxton, D.D.; Riek, L.D. Artificial intelligence and robotics in rehabilitation. In Handbook of Rehabilitation Psychology; Brenner, L.A., Reid-Arndt, S.A., Elliott, T.R., Frank, R.G., Caplan, B., Eds.; American Psychological Association: Washington, DC, USA, 2019; pp. 507–520. [Google Scholar] [CrossRef]
- Goldzweig, C.L.; Orshansky, G.; Paige, N.M.; Towfigh, A.A.; Haggstrom, D.A.; Miake-Lye, I.; Beroes, J.M.; Shekelle, P.G. Electronic Patient Portals: Evidence on Health Outcomes, Satisfaction, Efficiency, and Attitudes. Ann. Intern. Med. 2013, 159, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Sinsky, C.A.; Willard-Grace, R.; Schutzbank, A.M.; Margolius, D.; Bodenheimer, T. In Search of Joy in Practice: A Report of 23 High-Functioning Primary Care Practices. Ann. Fam. Med. 2013, 11, 272–278. [Google Scholar] [CrossRef] [Green Version]
- Sinsky, C.; Colligan, L.; Li, L.; Prgomet, M.; Reynolds, M.S.; Goeders, M.L.; Westbrook, J.; Tutty, M.; Blike, G. Allocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 Specialties. Ann. Intern. Med. 2016, 165, 753–760. [Google Scholar] [CrossRef]
- Lin, S.; Khoo, J.; Schillinger, E. Next big thing: Integrating medical scribes into academic medical centres. BMJ Simul. Technol. Enhanc. Learn. 2016, 2, 27–29. [Google Scholar] [CrossRef]
- Choi, C.; Schwarting, W.; DelPreto, J.; Rus, D. Learning Object Grasping for Soft Robot Hands. IEEE Robot. Autom. Lett. 2018, 3, 2370–2377. [Google Scholar] [CrossRef]
- Aggarwal, R.; Ganvir, S.S. Artificial intelligence in physiotherapy. Physiother. J. Indian Assoc. Physiother. 2021, 15, 55. [Google Scholar] [CrossRef]
- Frackiewicz, M. ChatGPT and the Future of Rehabilitation Therapy: An AI-Driven Approach. TS2 Space. 2023. Available online: https://ts2.space/en/chatgpt-and-the-future-of-rehabilitation-therapy-an-ai-driven-approach/ (accessed on 10 May 2023).
- Sharma, A.; Lin, I.W.; Miner, A.S.; Atkins, D.C.; Althoff, T. Human–AI collaboration enables more empathic conversations in text-based peer-to-peer mental health support. Nat. Mach. Intell. 2023, 5, 46–57. [Google Scholar] [CrossRef]
- Chung, E.J.; Lee, B.-H. The effects of flipped learning on learning motivation and attitudes in a class of college physical therapy students. J. Probl. Learn. 2018, 5, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Nadarzynski, T.; Miles, O.; Cowie, A.; Ridge, D. Acceptability of artificial intelligence (AI)-led chatbot services in healthcare: A mixed-methods study. Digit. Health 2019, 5, 2055207619871808. [Google Scholar] [CrossRef]
- Moon, I.; An, Y.; Min, S.; Park, C. Therapeutic Effects of Metaverse Rehabilitation for Cerebral Palsy: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 1578. [Google Scholar] [CrossRef]
- Kidziński, Ł.; Delp, S.; Schwartz, M. Automatic real-time gait event detection in children using deep neural networks. PLoS ONE 2019, 14, e0211466. [Google Scholar] [CrossRef] [Green Version]
- Lambercy, O.; Lehner, R.; Chua, K.; Wee, S.K.; Rajeswaran, D.K.; Kuah, C.W.K.; Ang, W.T.; Liang, P.; Campolo, D.; Hussain, A.; et al. Neurorehabilitation From a Distance: Can Intelligent Technology Support Decentralized Access to Quality Therapy? Front. Robot. 2021, 8, 612415. [Google Scholar] [CrossRef]
- Neibling, B.A.; Jackson, S.M.; Hayward, K.S.; Barker, R.N. Perseverance with technology-facilitated home-based upper limb practice after stroke: A systematic mixed studies review. J. Neuroeng. Rehabil. 2021, 18, 1–26. [Google Scholar] [CrossRef]
- Chidambaram, S.; Maheswaran, Y.; Patel, K.; Sounderajah, V.; Hashimoto, D.A.; Seastedt, K.P.; McGregor, A.H.; Markar, S.R.; Darzi, A. Using Artificial Intelligence-Enhanced Sensing and Wearable Technology in Sports Medicine and Performance Optimisation. Sensors 2022, 22, 6920. [Google Scholar] [CrossRef]
- Gichoya, J.W.; McCoy, L.G.; Celi, L.A.; Ghassemi, M. Equity in essence: A call for operationalising fairness in machine learning for healthcare. BMJ Health Care Inform. 2021, 28, e100289. [Google Scholar] [CrossRef]
- Soliño-Fernandez, D.; Ding, A.; Bayro-Kaiser, E.; Ding, E.L. Willingness to adopt wearable devices with behavioral and economic incentives by health insurance wellness programs: Results of a US cross-sectional survey with multiple consumer health vignettes. BMC Public Health 2019, 19, 1649. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Li, H.; Luo, Y. An empirical study of wearable technology acceptance in healthcare. Ind. Manag. Data Syst. 2015, 115, 1704–1723. [Google Scholar] [CrossRef]
- Tran, V.-T.; Riveros, C.; Ravaud, P. Patients’ views of wearable devices and AI in healthcare: Findings from the ComPaRe e-cohort. NPJ Digit. Med. 2019, 2, 53. [Google Scholar] [CrossRef] [Green Version]
- Wani, S.U.D.; Khan, N.A.; Thakur, G.; Gautam, S.P.; Ali, M.; Alam, P.; Alshehri, S.; Ghoneim, M.M.; Shakeel, F. Utilization of Artificial Intelligence in Disease Prevention: Diagnosis, Treatment, and Implications for the Healthcare Workforce. Healthcare 2022, 10, 608. [Google Scholar] [CrossRef]
- Berg, S. Nudge Theory Explored to Boost Medication Adherence. Chicago: American Medical Association. 2018. Available online: www.ama-assn.org/delivering-care/patient-support-advocacy/nudge-theory-exploredboost-medication-adherence (accessed on 1 January 2023).
- Commins, J. Nurses Say Distractions Cut Bedside Time by 25%. HealthLeaders. 2010. Available online: www.healthleadersmedia.com/nursing/nurses-say-distractions-cut-bedside-time-25 (accessed on 5 January 2023).
- Utermohlen, K. Four Robotic Process Automation (RPA) Applications in the Healthcare Industry. Medium. 2018. Available online: https://medium.com/@karl.utermohlen/4-robotic-process-automation-rpa-applications-inthe-healthcare-industry-4d449b24b613 (accessed on 29 December 2022).
- Corny, J.; Rajkumar, A.; Martin, O.; Dode, X.; Lajonchère, J.-P.; Billuart, O.; Bézie, Y.; Buronfosse, A. A machine learning–based clinical decision support system to identify prescriptions with a high risk of medication error. J. Am. Med. Inform. Assoc. 2020, 27, 1688–1694. [Google Scholar] [CrossRef]
- Ranchon, F.; Chanoine, S.; Lambert-Lacroix, S.; Bosson, J.-L.; Moreau-Gaudry, A.; Bedouch, P. Development of artificial intelligence powered apps and tools for clinical pharmacy services: A systematic review. Int. J. Med. Inform. 2023, 172, 104983. [Google Scholar] [CrossRef]
- Caruana, R.; Lou, Y.; Gehrke, J.; Koch, P.; Sturm, M.; Elhadad, N. Intelligible Models for HealthCare: Predicting Pneumonia Risk and Hospital 30-day Readmission. In Proceedings of the 21th ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, Sydney, Australia, 10 August 2015; ACM Press: Sydney, NSW, Australia, 2015; pp. 1721–1730. [Google Scholar]
- Clement, T.; Kemmerzell, N.; Abdelaal, M.; Amberg, M. XAIR: A Systematic Metareview of Explainable AI (XAI) Aligned to the Software Development Process. Mach. Learn. Knowl. Extr. 2023, 5, 78–108. [Google Scholar] [CrossRef]
- Tiwari, R. Explainable AI (XAI) and its Applications in Building Trust and Understanding in AI Decision Making. International J. Sci. Res. Eng. Manag. 2023, 7, 1–13. [Google Scholar] [CrossRef]
- Alvarez-Melis, D.; Jaakkola, T.S. Towards robust interpretability with self-explaining neural networks. arXiv 2018, arXiv:1806.07538. [Google Scholar] [CrossRef]
- Giuste, F.; Shi, W.; Zhu, Y.; Naren, T.; Isgut, M.; Sha, Y.; Tong, L.; Gupte, M.; Wang, M.D. Explainable Artificial Intelligence Methods in Combating Pandemics: A Systematic Review. IEEE Rev. Biomed. Eng. 2022, 16, 5–21. [Google Scholar] [CrossRef]
- Jadhav, S.; Deng, G.; Zawin, M.; Kaufman, A.E. COVID-view: Diagnosis of COVID-19 using Chest CT. IEEE Trans. Vis. Comput. Graph. 2021, 28, 227–237. [Google Scholar] [CrossRef]
- Dilsizian, S.E.; Siegel, E.L. Artificial Intelligence in Medicine and Cardiac Imaging: Harnessing Big Data and Advanced Computing to Provide Personalized Medical Diagnosis and Treatment. Curr. Cardiol. Rep. 2013, 16, 1–8. [Google Scholar] [CrossRef]
- Sunarti, S.; Rahman, F.F.; Naufal, M.; Risky, M.; Febriyanto, K.; Masnina, R. Artificial intelligence in healthcare: Opportunities and risk for future. Gac. Sanit. 2021, 35, S67–S70. [Google Scholar] [CrossRef]
- Farhud, D.D.; Zokaei, S. Ethical Issues of Artificial Intelligence in Medicine and Healthcare. Iran. J. Public Health 2021, 50, i–v. [Google Scholar] [CrossRef]
- Reddy, S.; Allan, S.; Coghlan, S.; Cooper, P. A governance model for the application of AI in health care. J. Am. Med. Inform. Assoc. 2019, 27, 491–497. [Google Scholar] [CrossRef]
- World Health Organization. Ethics and Governance of Artificial Intelligence for Health: WHO Guidance; World Health Organization: Geneva, Switzerland, 2021; p. 150. Available online: https://www.who.int/publications/i/item/9789240029200 (accessed on 29 December 2022).
- Marwaha, J.S.; Landman, A.B.; Brat, G.A.; Dunn, T.; Gordon, W.J. Deploying digital health tools within large, complex health systems: Key considerations for adoption and implementation. NPJ Digit. Med. 2022, 5, 13. [Google Scholar] [CrossRef]
- Liao, F.; Adelaine, S.; Afshar, M.; Patterson, B.W. Governance of Clinical AI applications to facilitate safe and equitable deployment in a large health system: Key elements and early successes. Front. Digit. Health 2022, 4, 931439. [Google Scholar] [CrossRef]
- Forcier, M.B.; Gallois, H.; Mullan, S.; Joly, Y. Integrating artificial intelligence into health care through data access: Can the GDPR act as a beacon for policymakers? J. Law Biosci. 2019, 6, 317–335. [Google Scholar] [CrossRef]
- Schaake, M. The European Commission’s Artificial Intelligence Act. Standford Univeristy Human-Centered Artificial Intelligence (BHAI), Standford, Canada. 2021. Available online: https://hai.stanford.edu/sites/default/files/2021-06/HAI_Issue-Brief_The-European-Commissions-Artificial-Intelligence-Act.pdf (accessed on 5 May 2023).
- Brown, R. Challenges to Successful AI Implementation in Healthcare. Data Science Central. 2022. Available online: https://www.datasciencecentral.com/challenges-to-successful-ai-implementation-in-healthcare/ (accessed on 30 March 2023).
- Tachkov, K.; Zemplenyi, A.; Kamusheva, M.; Dimitrova, M.; Siirtola, P.; Pontén, J.; Nemeth, B.; Kalo, Z.; Petrova, G. Barriers to Use Artificial Intelligence Methodologies in Health Technology Assessment in Central and East European Countries. Front. Public Health 2022, 10, 921226. [Google Scholar] [CrossRef]
- Marcus, G. Deep learning: A Critical Appraisal. arXiv 2018. Available online: https://arxiv.org/abs/1801.00631 (accessed on 1 May 2019).
- Kelly, C.J.; Karthikesalingam, A.; Suleyman, M.; Corrado, G.; King, D. Key challenges for delivering clinical impact with artificial intelligence. BMC Med. 2019, 17, 195. [Google Scholar] [CrossRef] [Green Version]
- Choudhury, A.; Asan, O. Impact of accountability, training, and human factors on the use of artificial intelligence in healthcare: Exploring the perceptions of healthcare practitioners in the US. Hum. Factors Healcare 2022, 2, 100021. [Google Scholar] [CrossRef]
- Joshi, N. 5 AI Implementation Challenges in Healthcare. 2020. Available online: https://www.allerin.com/blog/5-ai-implementation-challenges-in-healthcare (accessed on 31 March 2023).
- Khan, B.; Fatima, H.; Qureshi, A.; Kumar, S.; Hanan, A.; Hussain, J.; Abdullah, S. Drawbacks of Artificial Intelligence and Their Potential Solutions in the Healthcare Sector. Biomed. Mater. Devices 2023, 1–8. [Google Scholar] [CrossRef]
- Baowaly, M.K.; Lin, C.-C.; Liu, C.-L.; Chen, K.-T. Synthesizing electronic health records using improved generative adversarial networks. J. Am. Med. Inform. Assoc. 2018, 26, 228–241. [Google Scholar] [CrossRef]
- Neill, D.B. Using artifcial intelligence to improve hospital inpatient care. IEEE Intell. Syst. 2013, 28, 92–95. [Google Scholar] [CrossRef]
- Fernandes, M.; Vieira, S.M.; Leite, F.; Palos, C.; Finkelstein, S.; Sousa, J.M. Clinical Decision Support Systems for Triage in the Emergency Department using Intelligent Systems: A Review. Artif. Intell. Med. 2020, 102, 101762. [Google Scholar] [CrossRef]
- Gama, F.; Tyskbo, D.; Nygren, J.; Barlow, J.; Reed, J.; Svedberg, P. Implementation Frameworks for Artificial Intelligence Translation Into Health Care Practice: Scoping Review. J. Med. Internet Res. 2022, 24, e32215. [Google Scholar] [CrossRef]
- Wolff, J.; Pauling, J.; Keck, A.; Baumbach, J. Systematic Review of Economic Impact Studies of Artificial Intelligence in Health Care. J. Med. Internet Res. 2020, 22, e16866. [Google Scholar] [CrossRef]
- Alami, H.; Lehoux, P.; Denis, J.L.; Motulsky, A.; Petitgand, C.; Savoldelli, M.; Rouquet, R.; Gagnon, M.P.; Roy, D.; Fortin, J.P. Organizational readiness for artifcial intelligence in health care: Insights for decision-making and practice. J. Health Organ. Manag. 2021, 35, 106–114. [Google Scholar] [CrossRef]
- Duggal, N. Advantages and Disadvantages of Artificial Intelligence. Simplilearn. 2023. Available online: https://www.simplilearn.com/advantages-and-disadvantages-of-artificial-intelligence-article (accessed on 11 May 2023).


{kind=link}
| Term | Definition |
|---|---|
| Artificial intelligence (AI) | AI denotes the science and engineering of creating intelligent machines using algorithms or rules, which the machine shadows to mimic human cognitive functions, namely, learning and problem solving [13]. AI usually refers to computer technologies that emulate mechanisms supported by human intelligence, namely, adaptation, deep learning, reasoning, engagement, and sensory understanding [14,15]. It aims to mimic human cognitive functions. It brings a paradigm shift in healthcare, driven by the increasing availability of health data and the rapid growth of analytical techniques [16]. |
| Machine learning (ML) | ML is a subtype of AI technology that aims to improve the speed and accuracy of physicians’ work. It also denotes several statistical techniques that allow computers to learn from experience without being explicitly programmed. This learning usually takes the form of variations in how an algorithm works [17]. It is also a tool applied in healthcare to assist healthcare professionals in caring for patients and managing clinical data. It is an application of AI that involves programming computers to mimic how humans think and learn [18]. |
| Distributed Ledger Technology (DLT) | DLT is an innovative and rapidly growing method for recording and sharing data across different data stores (ledgers) [19]. It is secure, immutable, and readily available. It can allow patients to take control of their own data, eventually generating trust in an industry that matters to all of us [20]. DLT integrated with AI describes a novel and advanced method to achieve the intelligent, resilient, and safe handling of electronic health record data [21]. |
| Natural language processing (NLP) | Natural language processing (NLP) denotes the field of study that emphasizes the interactions between human language and computers [22]. NLP techniques can capture unstructured healthcare information, analyze its grammatical structure, determine the meaning of information, and translate information; therefore, it can be easily understood by electronic healthcare systems. These techniques also reduce costs and improve the quality of healthcare [23]. |
| Metaverse | The metaverse represents a 3D space based on virtual and augmented reality, where individuals can utilize their own avatars to play, work, and synchronously interconnect with each other [24]. It delivers an entrancing, communicative, and pleasurable healthcare service experience tailored to achieve patients’ desires. It includes modern technologies such as AI, telepresence, blockchain, virtual reality (VR), augmented reality (AR), and digital twinning. These technologies highly influence healthcare [25]. The metaverse application is exclusively associated with healthcare, establishing a “niche theme” for academics, such as education, research, training, and disease prevention and management. It has become a vibrant technology for strengthening medical students’ competence. Furthermore, patients’ health illnesses can be directly monitored at their homes, and real life can also be connected with the virtual one using digital twins, a diverse technology [26,27]. |
| Chat Generative Pretrained Transformer (ChatGPT) | ChatGPT is an AI-based conversational agent that utilizes natural language processing (NLP) and machine learning algorithms to simulate human-like conversations [28]. Its critical applications in healthcare, including practice, education, and research, could be auspicious if the accompanying valid concerns are proactively inspected and tackled. It functions as a chatbot, a program that can comprehend and create responses using a text-grounded interface [29]. Xu et al. [30] described the application of chatbots in healthcare, comprising patient support; monitoring and administration; and tumor diagnostics, screening, and management. |
| Transformer | Transformer is a critical deep learning model and is broadly used in various areas, namely, computer vision (CV), natural language processing (NLP), and speech processing [31]. The applications of transformers are observed in electronic health records, medical imaging, and COVID-19 detection [32,33,34,35,36]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Kuwaiti, A.; Nazer, K.; Al-Reedy, A.; Al-Shehri, S.; Al-Muhanna, A.; Subbarayalu, A.V.; Al Muhanna, D.; Al-Muhanna, F.A. A Review of the Role of Artificial Intelligence in Healthcare. J. Pers. Med. 2023, 13, 951. https://doi.org/10.3390/jpm13060951
Al Kuwaiti A, Nazer K, Al-Reedy A, Al-Shehri S, Al-Muhanna A, Subbarayalu AV, Al Muhanna D, Al-Muhanna FA. A Review of the Role of Artificial Intelligence in Healthcare. Journal of Personalized Medicine. 2023; 13(6):951. https://doi.org/10.3390/jpm13060951
Chicago/Turabian StyleAl Kuwaiti, Ahmed, Khalid Nazer, Abdullah Al-Reedy, Shaher Al-Shehri, Afnan Al-Muhanna, Arun Vijay Subbarayalu, Dhoha Al Muhanna, and Fahad A. Al-Muhanna. 2023. "A Review of the Role of Artificial Intelligence in Healthcare" Journal of Personalized Medicine 13, no. 6: 951. https://doi.org/10.3390/jpm13060951
APA StyleAl Kuwaiti, A., Nazer, K., Al-Reedy, A., Al-Shehri, S., Al-Muhanna, A., Subbarayalu, A. V., Al Muhanna, D., & Al-Muhanna, F. A. (2023). A Review of the Role of Artificial Intelligence in Healthcare. Journal of Personalized Medicine, 13(6), 951. https://doi.org/10.3390/jpm13060951