
Canadian Healthcare Professionals’ Views and Attitudes toward Risk-Stratified Breast Cancer Screening

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials & Methods
2.1. Study Design
2.2. Data Collection Tool
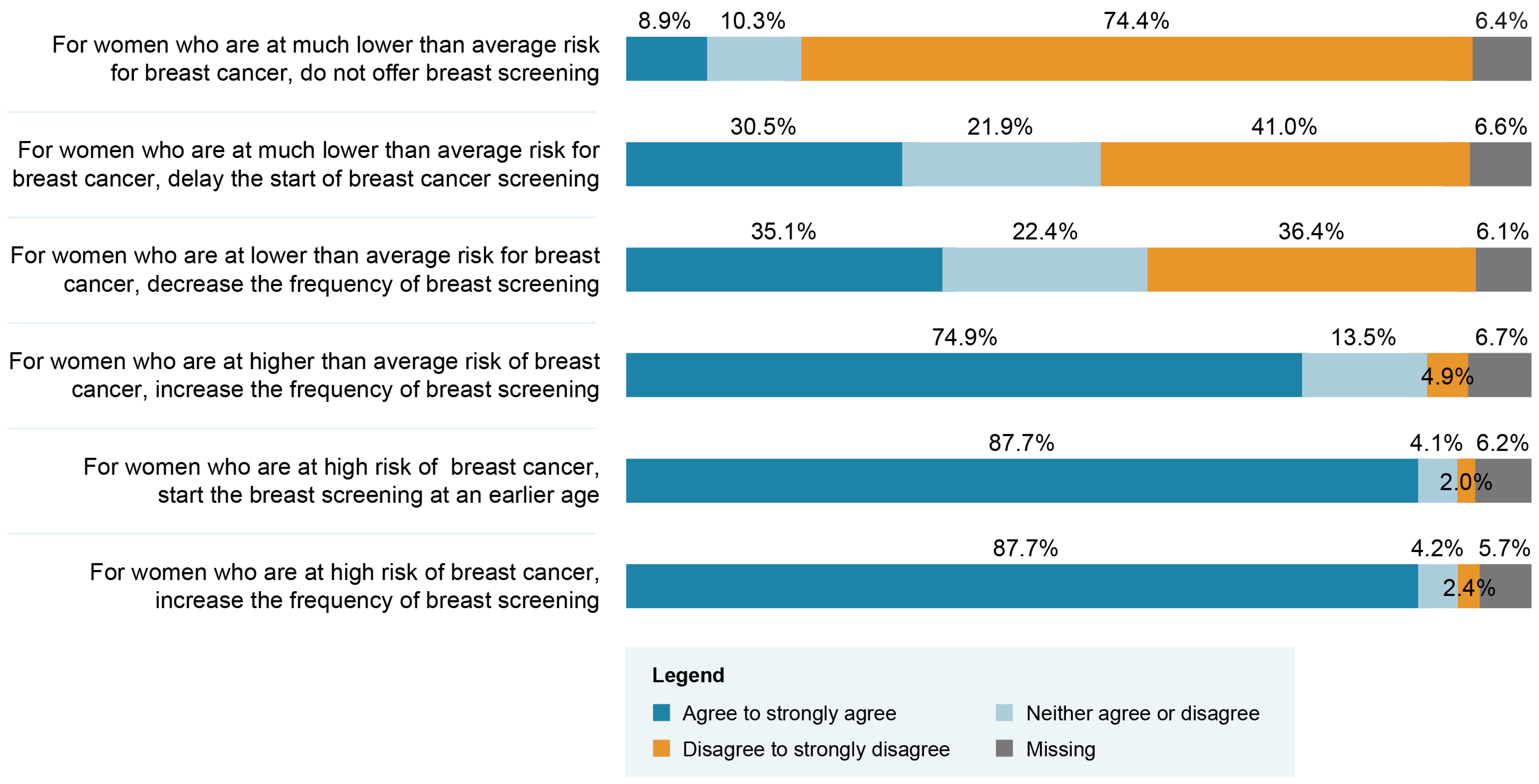
- attitudes toward BC screening recommendations in a context of risk stratification (1 question with 6 statements),
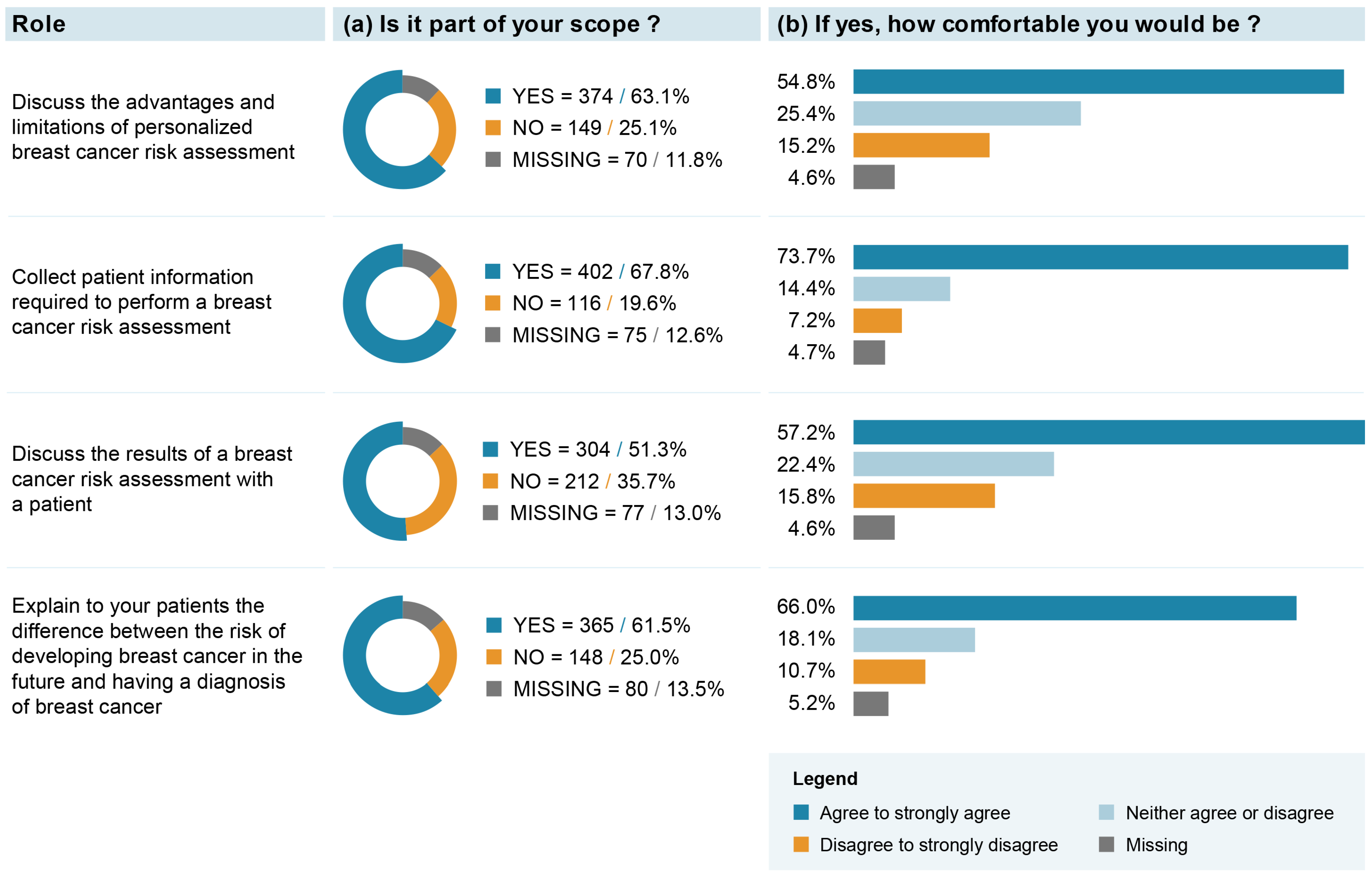
- attitudes toward their role and scope of practice within a risk-stratified BC screening approach (1 question with 5 statements),
- views toward the necessary enhancements to the healthcare system required if such an approach were implemented (1 question),
- views toward the professional group that should play a role if risk-stratified BC screening were implemented (1 question).
2.3. Statistical Analyses
3. Results
“Am very glad that there is enlightened exploration of routine breast screening practices with risk stratification. I personally have always challenged the recommendations and practices. We also need improved technology to assess breast health as all breast sizes and density are not equal. There are insufficient vertical MRIs available for routine screenings. I eagerly look forward to improved risk assessment and decision making supports”.“Moving from routine to individualized screening is a good idea, but risk assessment cannot be left to family physicians again. Some people do not have family physicians and family physicians already provide primary, secondary and even tertiary care. All specialties offload their follow-ups to family physicians. Adding a risk calculation to family physicians assumes that some will not have this calculation because of lack of time, because of other health problems to discuss or simply because they do not have a family physician. Women who may be at high risk could end up not being screened…”“Shared decision making should be central to this modified program. The risk-based approach is interesting but will need to be the subject of randomized trials to properly assess the risks and benefits. In all cases, the shared decision must be put at the heart of the discussions, which is far from being the case at present”.
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Agency for Cancer Research of the World Health Organization. Current and Future Burden of Breast Cancer: Global Statistics for 2020 and 2040. Available online: https://www.iarc.who.int/news-events/current-and-future-burden-of-breast-cancer-global-statistics-for-2020-and-2040/ (accessed on 30 March 2023).
- Public Health Agency of Canada Breast Cancer. Available online: https://www.canada.ca/en/public-health/services/chronic-diseases/cancer/breast-cancer.html (accessed on 11 April 2023).
- Canadian Task Force on Preventive Health Care Breast Cancer Update. 2018. Available online: https://canadiantaskforce.ca/guidelines/published-guidelines/breast-cancer-update/ (accessed on 11 April 2023).
- Marmot, M.G.; Altman, D.G.; Cameron, D.A.; Dewar, J.A.; Thompson, S.G.; Wilcox, M. The benefits and harms of breast cancer screening: An independent review. Br. J. Cancer 2013, 108, 2205–2240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, J.D.; Nabi, H.H.; Andrulis, I.L.; Antoniou, A.C.; Chiquette, J.; Després, P.; Devilee, P.; Dorval, M.; Droit, A.; Easton, D.F.; et al. Personalized Risk Assessment for Prevention and Early Detection of Breast Cancer: Integration and Implementation (PERSPECTIVE I&I). J. Pers. Med. 2021, 11, 511. [Google Scholar] [CrossRef] [PubMed]
- Esserman, L.J. The WISDOM Study: Breaking the deadlock in the breast cancer screening debate. NPJ Breast Cancer 2017, 3, 34. [Google Scholar] [CrossRef] [PubMed]
- Roux, A.; Cholerton, R.; Sicsic, J.; Moumjid, N.; French, D.P.; Rossi, P.G.; Balleyguier, C.; Guindy, M.; Gilbert, F.J.; Burrion, J.-B.; et al. Study protocol comparing the ethical, psychological and socio-economic impact of personalised breast cancer screening to that of standard screening in the “My Personal Breast Screening” (MyPeBS) randomised clinical trial. BMC Cancer 2022, 22, 507. [Google Scholar] [CrossRef] [PubMed]
- Pashayan, N.; Antoniou, A.C.; Ivanus, U.; Esserman, L.J.; Easton, D.F.; French, D.; Sroczynski, G.; Hall, P.; Cuzick, J.; Evans, D.G.; et al. Personalized early detection and prevention of breast cancer: ENVISION consensus statement. Nat. Rev. Clin. Oncol. 2020, 17, 687–705. [Google Scholar] [CrossRef]
- Pashayan, N.; Morris, S.; Gilbert, F.J.; Pharoah, P.D.P. Cost-effectiveness and Benefit-to-Harm Ratio of Risk-Stratified Screening for Breast Cancer: A Life-Table Model. JAMA Oncol. 2018, 4, 1504–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Broek, J.J.; Schechter, C.B.; van Ravesteyn, N.T.; Janssens, A.C.J.W.; Wolfson, M.C.; Trentham-Dietz, A.; Simard, J.; Easton, D.F.; Mandelblatt, J.S.; Kraft, P.; et al. Personalizing Breast Cancer Screening Based on Polygenic Risk and Family History. JNCI J. Natl. Cancer Inst. 2021, 113, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Van Ravesteyn, M.N.T.; Miglioretti, D.L.; Stout, N.K.; Lee, D.S.J.; Schechter, C.B.; Buist, D.S.; Huang, H.; Heijnsdijk, E.A.; Trentham-Dietz, A.; Alagoz, O.; et al. Tipping the balance of benefits and harms to favor screening mammography starting at age 40 years: A comparative modeling study of risk. Ann. Intern. Med. 2012, 156, 609–617. [Google Scholar] [CrossRef]
- Trentham-Dietz, A.; Kerlikowske, K.; Stout, N.K.; Miglioretti, D.L.; Schechter, C.B.; Ergun, M.M.A.; Broek, J.J.v.D.; Alagoz, O.; Sprague, B.L.; van Ravesteyn, N.T.; et al. Tailoring Breast Cancer Screening Intervals by Breast Density and Risk for Women Aged 50 Years or Older: Collaborative Modeling of Screening Outcomes. Ann. Intern. Med. 2016, 165, 700–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagnon, J.; Lévesque, E.; Clinical Advisory Committee on Breast Cancer Screening and Prevention; Borduas, F.; Chiquette, J.; Diorio, C.; Duchesne, N.; Dumais, M.; Eloy, L.; Foulkes, W.; et al. Recommendations on breast cancer screening and prevention in the context of implementing risk stratification: Impending changes to current policies. Curr. Oncol. 2016, 23, e615–e625. [Google Scholar] [CrossRef] [Green Version]
- Román, M.; Sala, M.; Domingo, L.; Posso, M.; Louro, J.; Castells, X. Personalized breast cancer screening strategies: A systematic review and quality assessment. PLoS ONE 2019, 14, e0226352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mühlberger, N.; Sroczynski, G.; Gogollari, A.; Jahn, B.; Pashayan, N.; Steyerberg, E.; Widschwendter, M.; Siebert, U. Cost effectiveness of breast cancer screening and prevention: A systematic review with a focus on risk-adapted strategies. Eur. J. Health Econ. 2021, 22, 1311–1344. [Google Scholar] [CrossRef] [PubMed]
- Vilaprinyo, E.; Forné, C.; Carles, M.; Sala, M.; Pla, R.; Castells, X.; Domingo, L.; Rue, M. Cost-effectiveness and harm-benefit analyses of risk-based screening strategies for breast cancer. PLoS ONE 2014, 9, e86858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, S.; Henneman, L.; Dent, T.; Hall, A.; Burton, A.; Pharoah, P.; Pashayan, N.; Burton, H. Do Health Professionals Need Additional Competencies for Stratified Cancer Prevention Based on Genetic Risk Profiling? J. Pers. Med. 2015, 5, 191–212. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Robert, G.; Macfarlane, F.; Bate, P.; Kyriakidou, O. Diffusion of innovations in service organizations: Systematic review and recommendations. Milbank Q 2004, 82, 581–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, D.; Drouin, D.; Lang, A.; Roberge, D.; Ritchie, J.; Plante, A. Interprofessional collaborative practice within cancer teams: Translating evidence into action. A mixed methods study protocol. Implement. Sci. 2010, 5, 53. [Google Scholar] [CrossRef] [Green Version]
- Laza-Vásquez, C.; Codern-Bové, N.; Cardona-Cardona, A.; Hernández-Leal, M.J.; Pérez-Lacasta, M.J.; Carles-Lavila, M.; Rué, M. Views of health professionals on risk-based breast cancer screening and its implementation in the Spanish National Health System: A qualitative discussion group study. PLoS ONE 2022, 17, e0263788. [Google Scholar] [CrossRef] [PubMed]
- Puzhko, S.; Gagnon, J.; Simard, J.; Knoppers, B.M.; Siedlikowski, S.; Bartlett, G. Health professionals’ perspectives on breast cancer risk stratification: Understanding evaluation of risk versus screening for disease. Public Health Rev. 2019, 40, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, D.P.; Woof, V.G.; Ruane, H.; Evans, D.G.; Ulph, F.; Donnelly, L.S. The feasibility of implementing risk stratification into a national breast cancer screening programme: A focus group study investigating the perspectives of healthcare personnel responsible for delivery. BMC Womens Health 2022, 22, 142. [Google Scholar] [CrossRef] [PubMed]
- Rainey, L.; van der Waal, D.; Donnelly, L.S.; Evans, D.G.; Wengström, Y.; Broeders, M. Women’s decision-making regarding risk-stratified breast cancer screening and prevention from the perspective of international healthcare professionals. PLoS ONE 2018, 13, e0197772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McWilliams, L.; Woof, V.G.; Donnelly, L.S.; Howell, A.; Evans, D.G.; French, D.P. Risk stratified breast cancer screening: UK healthcare policy decision-making stakeholders’ views on a low-risk breast screening pathway. BMC Cancer 2020, 20, 680. [Google Scholar] [CrossRef] [PubMed]
- Keogh, L.A.; Steel, E.; Weideman, P.; Butow, P.; Collins, I.M.; Emery, J.D.; Mann, G.B.; Bickerstaffe, A.; Trainer, A.H.; Hopper, L.J.; et al. Consumer and clinician perspectives on personalising breast cancer prevention information. Breast 2019, 43, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Collins, I.M.; Steel, E.; Mann, G.B.; Emery, J.D.; Bickerstaffe, A.; Trainer, A.; Butow, P.; Pirotta, M.; Antoniou, A.C.; Cuzick, J.; et al. Assessing and managing breast cancer risk: Clinicians’ current practice and future needs. Breast 2014, 23, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Woof, V.G.; McWilliams, L.; Donnelly, L.S.; Howell, A.; Evans, D.G.; Maxwell, A.J.; French, D.P. Introducing a low-risk breast screening pathway into the NHS Breast Screening Programme: Views from healthcare professionals who are delivering risk-stratified screening. Womens Health 2021, 17, 17455065211009746. [Google Scholar] [CrossRef] [PubMed]
- Esquivel-Sada, D.; Levesque, E.; Hagan, J.; Knoppers, B.M.; Simard, J. Envisioning Implementation of a Personalized Approach in Breast Cancer Screening Programs: Stakeholder Perspectives. Healthc. Policy 2019, 15, 39–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laza-Vásquez, C.; Hernández-Leal, M.J.; Carles-Lavila, M.; Pérez-Lacasta, M.J.; Cruz-Esteve, I.; Rué, M.; on behalf of the DECIDO Group. Barriers and Facilitators to the Implementation of a Personalized Breast Cancer Screening Program: Views of Spanish Health Professionals. Int. J. Environ. Res. Public Health 2022, 19, 1406. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, A.; Lapointe, J.; Nabi, H.; Pashayan, N. Risk-Stratified Breast Cancer Screening Incorporating a Polygenic Risk Score: A Survey of UK General Practitioners’ Knowledge and Attitudes. Genes 2023, 14, 732. [Google Scholar] [CrossRef]
- Lapointe, J.; Buron, A.-C.; Mbuya-Bienge, C.; Dorval, M.; Pashayan, N.; Brooks, J.D.; Walker, M.J.; Chiquette, J.; Eloy, L.; Blackmore, K.; et al. Polygenic risk scores and risk-stratified breast cancer screening: Familiarity and perspectives of health care professionals. Genet. Med. 2022, 24, 2380–2388. [Google Scholar] [CrossRef]
- Koitsalu, M.; Sprangers, M.A.; Eklund, M.; Czene, K.; Hall, P.; Gronberg, H.; Brandberg, Y. Public interest in and acceptability of the prospect of risk-stratified screening for breast and prostate cancer. Acta Oncol. 2016, 55, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Shieh, Y.; Eklund, M.; Madlensky, L.; Sawyer, S.D.; Thompson, C.K.; Stover Fiscalini, A.; Ziv, E.; Van’t Veer, L.J.; Esserman, L.J.; Tice, J.A. Breast Cancer Screening in the Precision Medicine Era: Risk-Based Screening in a Population-Based Trial. J. Natl. Cancer Inst. 2017, 109, djw290. [Google Scholar] [CrossRef] [Green Version]
- Altmann, T.K. Attitude: A Concept Analysis. Nurs. Forum 2008, 43, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Merriam-Webster Point of View. Available online: https://www.merriam-webster.com/dictionary/point%20of%20view (accessed on 17 February 2023).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enders, C.K. Applied Missing Data Analysis; The Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Meisel, S.F.; Pashayan, N.; Rahman, B.; Side, L.; Fraser, L.; Gessler, S.; Lanceley, A.; Wardle, J. Adjusting the frequency of mammography screening on the basis of genetic risk: Attitudes among women in the UK. Breast 2015, 24, 237–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bienge, C.M.; Pashayan, N.; Brooks, J.D.; Dorval, M.; Chiquette, J.; Eloy, L.; Turgeon, A.; Lambert-Côté, L.; Paquette, J.-S.; Lévesque, E.; et al. Women’s Views on Multifactorial Breast Cancer Risk Assessment and Risk-Stratified Screening: A Population-Based Survey from Four Provinces in Canada. J. Pers. Med. 2021, 11, 95. [Google Scholar] [CrossRef]
- Ghanouni, A.; Sanderson, S.C.; Pashayan, N.; Renzi, C.; von Wagner, C.; Waller, J. Attitudes towards risk-stratified breast cancer screening among women in England: A cross-sectional survey. J. Med. Screen. 2020, 27, 138–145. [Google Scholar] [CrossRef] [Green Version]
- Sankatsing, V.D.V.; van Ravesteyn, N.T.; Heijnsdijk, E.A.M.; Broeders, M.J.M.; de Koning, H.J. Risk stratification in breast cancer screening: Cost-effectiveness and harm-benefit ratios for low-risk and high-risk women. Int. J. Cancer 2020, 147, 3059–3067. [Google Scholar] [CrossRef]
- Statistics Canada Canada’s Population Estimates, Third Quarter 2022. Available online: https://www150.statcan.gc.ca/n1/daily-quotidien/221221/dq221221f-eng.htm?HPA=1&indid=4098-1&indgeo=0 (accessed on 6 February 2023).
- Bégin, M. Medicare: Canada’s Right to Health; Optimum Publishing Internation, Inc.: Toronto, ON, Canada, 1988. [Google Scholar]
- Government of Canada Health care in Canada: Access Our Universal Health Care System. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/services/new-immigrants/new-life-canada/health-care/universal-system.html (accessed on 6 February 2023).
- Statistics Canada Health Fact Sheets: Primary Health Care Providers. 2019. Available online: https://www150.statcan.gc.ca/n1/pub/82-625-x/2020001/article/00004-eng.htm (accessed on 6 February 2023).
- Blood, K.A.; McCullum, M.; Wilson, C.; Cheifetz, R.E. Hereditary breast cancer in British Columbia: Outcomes from BC Cancer’s High-Risk Clinic. BCMJ 2018, 60, 40–46. [Google Scholar]
- Cancer Care Ontario Breast Cancer Screening for Women at High Risk. Available online: https://www.cancercareontario.ca/en/guidelines-advice/cancer-continuum/screening/breast-cancer-high-risk-women (accessed on 25 March 2023).
- Fok, R.W.-Y.; Ong, C.S.B.; Lie, D.; Ishak, D.; Fung, S.M.; Tang, W.E.; Sun, S.; Smith, H.; Ngeow, J.Y.Y. How practice setting affects family physicians’ views on genetic screening: A qualitative study. BMC Fam. Pract. 2021, 22, 141. [Google Scholar] [CrossRef]
- Hagan, J.; Lévesque, E.; Knoppers, B.M. Influence des facteurs organisationnels sur l’implantation d’une approche personnalisée de dépistage du cancer du sein. St. Publique 2016, 28, 353–361. [Google Scholar] [CrossRef]
- Plat, A.W.; Kroon, A.A.; Van Schayck, C.P.; De Leeuw, P.W.; Stoffers, H.E. Obtaining the family history for common, multifactorial diseases by family physicians. A descriptive systematic review. Eur. J. Gen. Pract. 2009, 15, 231–242. [Google Scholar] [CrossRef]
- Selkirk, C.G.; Weissman, S.M.; Anderson, A.; Hulick, P.J. Physicians’ Preparedness for Integration of Genomic and Pharmacogenetic Testing into Practice Within a Major Healthcare System. Genet. Test. Mol. Biomark. 2013, 17, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Chow-White, P.; Ha, D.; Laskin, J. Knowledge, attitudes, and values among physicians working with clinical genomics: A survey of medical oncologists. Hum. Resour. Health 2017, 15, 42. [Google Scholar] [CrossRef] [PubMed]
- Hann, K.E.J.; Fraser, L.; Side, L.; Gessler, S.; Waller, J.; Sanderson, S.C.; Freeman, M.; Jacobs, I.; Lanceley, A. Health care professionals’ attitudes towards population-based genetic testing and risk-stratification for ovarian cancer: A cross-sectional survey. BMC Womens Health 2017, 17, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Gender | |
| Women | 432 (93.5) |
| Men | 30 (6.5) |
| [Missing data/Prefer not to answer] | [131] |
| Profession | |
| Physician | 103 (22.3) |
| Nurse | 323 (69.7) |
| Other (1) | 37 (8.0) |
| [Missing data] | [130] |
| Medical specialty | |
| Family medicine/Primary care | 167 (36.1) |
| Oncology | 59 (12.8) |
| Other (2) | 236 (51.1) |
| [Missing data] | [131] |
| Number of years of practice | |
| <5 years | 58 (12.5) |
| 5–14 years | 135 (29.2) |
| 15–25 years | 113 (24.4) |
| >25 years | 157 (33.9) |
| [Missing data] | [130] |
| Region of practice | |
| Province of Québec | 377 (82.9) |
| Province of Ontario | 46 (10.1) |
| Other Provinces (3) | 32 (7.0) |
| [Missing data] | [138] |
| Practice Setting | |
| Academic Hospital | 133 (28.9) |
| Community Hospital | 98 (21.3) |
| Community health center | 78 (17.0) |
| Family health team/group/network | 75 (16.3) |
| Private clinic | 25 (5.4) |
| Other (4) | 51 (11.1) |
| [Missing data] | [133] |
| Entire Group n (%) | Province of Québec n (%) | Other Canadian Provinces n (%) | p-Value | |
|---|---|---|---|---|
| Primary care physician | 450 (24.7) | 338 (26.3) | 75 (20.4) | 0.02 |
| Nurse practitioner | 425 (23.3) | 318 (24.7) | 67 (18.3) | 0.01 |
| Genetic counsellor | 235 (12.9) | 163 (12.7) | 47 (12.8) | 0.94 |
| Nurse navigator | 231 (12.7) | 162 (12.6) | 49 (13.4) | 0.70 |
| Geneticist | 203 (11.1) | 158 (12.3) | 29 (7.9) | 0.02 |
| Radiologist | 190 (10.4) | 137 (10.6) | 36 (9.8) | 0.64 |
| Other † | 87 (4.8) | 11 (0.9) | 64 (17.4) | <0.01 |
| Entire Group n (%) | Province of Québec n (%) | Other Canadian Provinces n (%) | p-Value | |
|---|---|---|---|---|
| Access to a primary care physician | 229 (15.6) | 187 (16.9) | 25 (11.1) | 0.03 |
| Number of nurse practitioners | 189 (12.9) | 148 (13.4) | 25 (11.1) | 0.35 |
| Access to breast screening (e.g., mammogram, MRI) | 177 (12.0) | 133 (12.0) | 28 (12.4) | 0.87 |
| Time allocated to a patient-physician appointment | 162 (11.0) | 117 (10.6) | 25 (11.1) | 0.82 |
| Access to a nurse or nurse practitioner | 155 (10.6) | 118 (10.7) | 26 (11.6) | 0.70 |
| Medical training | 152 (10.3) | 125 (11.3) | 15 (6.7) | 0.04 |
| Number of primary care physicians | 118 (8.0) | 82 (7.4) | 25 (11.1) | 0.06 |
| Number of genetic counsellors | 113 (7.7) | 74 (6.7) | 26 (11.6) | 0.01 |
| Time allocated to a patient-nurse practitioner appointment | 71 (4.8) | 50 (4.5) | 13 (5.8) | 0.42 |
| Number of geneticists | 46 (3.1) | 36 (3.3) | 6 (2.7) | 0.64 |
| Remuneration of healthcare professionals | 34 (2.3) | 26 (2.4) | 7 (3.1) | 0.51 |
| None, I believe the healthcare system is ready | 6 (0.4) | 6 (0.5) | 0 (0.0) | 0.27 |
| Other | 17 (1.2) | 2 (0.2) | 4 (1.8) | <0.01 |
| Physicians | Nurses | |||
|---|---|---|---|---|
| Québec (n = 76) | Other Provinces (n = 23) | Québec (n = 276) | Other Provinces (n = 46) | |
| Access to a primary care physician | 21 | 10 | 151 | 10 |
| Number of nurse practitioners | 13 | 2 | 130 | 21 |
| Access to breast screening (e.g., mammogram, MRI) | 15 | 8 | 108 | 18 |
| Time allocated to a patient-physician appointment | 35 | 11 | 74 | 11 |
| Access to a nurse or nurse practitioner | 8 | 3 | 105 | 21 |
| Medical training | 39 | 3 | 78 | 12 |
| Number of primary care physicians | 24 | 11 | 51 | 11 |
| Number of genetic counsellors | 28 | 10 | 37 | 10 |
| Time allocated to a patient-nurse practitioner appointment | 6 | 1 | 43 | 11 |
| Number of geneticists | 14 | 2 | 16 | 3 |
| Remuneration of healthcare professionals | 5 | 4 | 20 | 3 |
| None, I believe the healthcare system is ready | 2 | 0 | 4 | 0 |
| Other | 2 | 1 | 0 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lapointe, J.; Côté, J.-M.; Mbuya-Bienge, C.; Dorval, M.; Pashayan, N.; Chiquette, J.; Eloy, L.; Turgeon, A.; Lambert-Côté, L.; Brooks, J.D.; et al. Canadian Healthcare Professionals’ Views and Attitudes toward Risk-Stratified Breast Cancer Screening. J. Pers. Med. 2023, 13, 1027. https://doi.org/10.3390/jpm13071027
Lapointe J, Côté J-M, Mbuya-Bienge C, Dorval M, Pashayan N, Chiquette J, Eloy L, Turgeon A, Lambert-Côté L, Brooks JD, et al. Canadian Healthcare Professionals’ Views and Attitudes toward Risk-Stratified Breast Cancer Screening. Journal of Personalized Medicine. 2023; 13(7):1027. https://doi.org/10.3390/jpm13071027
Chicago/Turabian StyleLapointe, Julie, Jean-Martin Côté, Cynthia Mbuya-Bienge, Michel Dorval, Nora Pashayan, Jocelyne Chiquette, Laurence Eloy, Annie Turgeon, Laurence Lambert-Côté, Jennifer D. Brooks, and et al. 2023. "Canadian Healthcare Professionals’ Views and Attitudes toward Risk-Stratified Breast Cancer Screening" Journal of Personalized Medicine 13, no. 7: 1027. https://doi.org/10.3390/jpm13071027
APA StyleLapointe, J., Côté, J.-M., Mbuya-Bienge, C., Dorval, M., Pashayan, N., Chiquette, J., Eloy, L., Turgeon, A., Lambert-Côté, L., Brooks, J. D., Walker, M. J., Blackmore, K. M., Joly, Y., Knoppers, B. M., Chiarelli, A. M., Simard, J., & Nabi, H. (2023). Canadian Healthcare Professionals’ Views and Attitudes toward Risk-Stratified Breast Cancer Screening. Journal of Personalized Medicine, 13(7), 1027. https://doi.org/10.3390/jpm13071027