
Comorbidity Patterns and Management in Inpatients with Endocrine Diseases by Age Groups in South Korea: Nationwide Data

Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials and Study Population
2.2. Variables and Measures
2.3. Data Analysis
3. Results
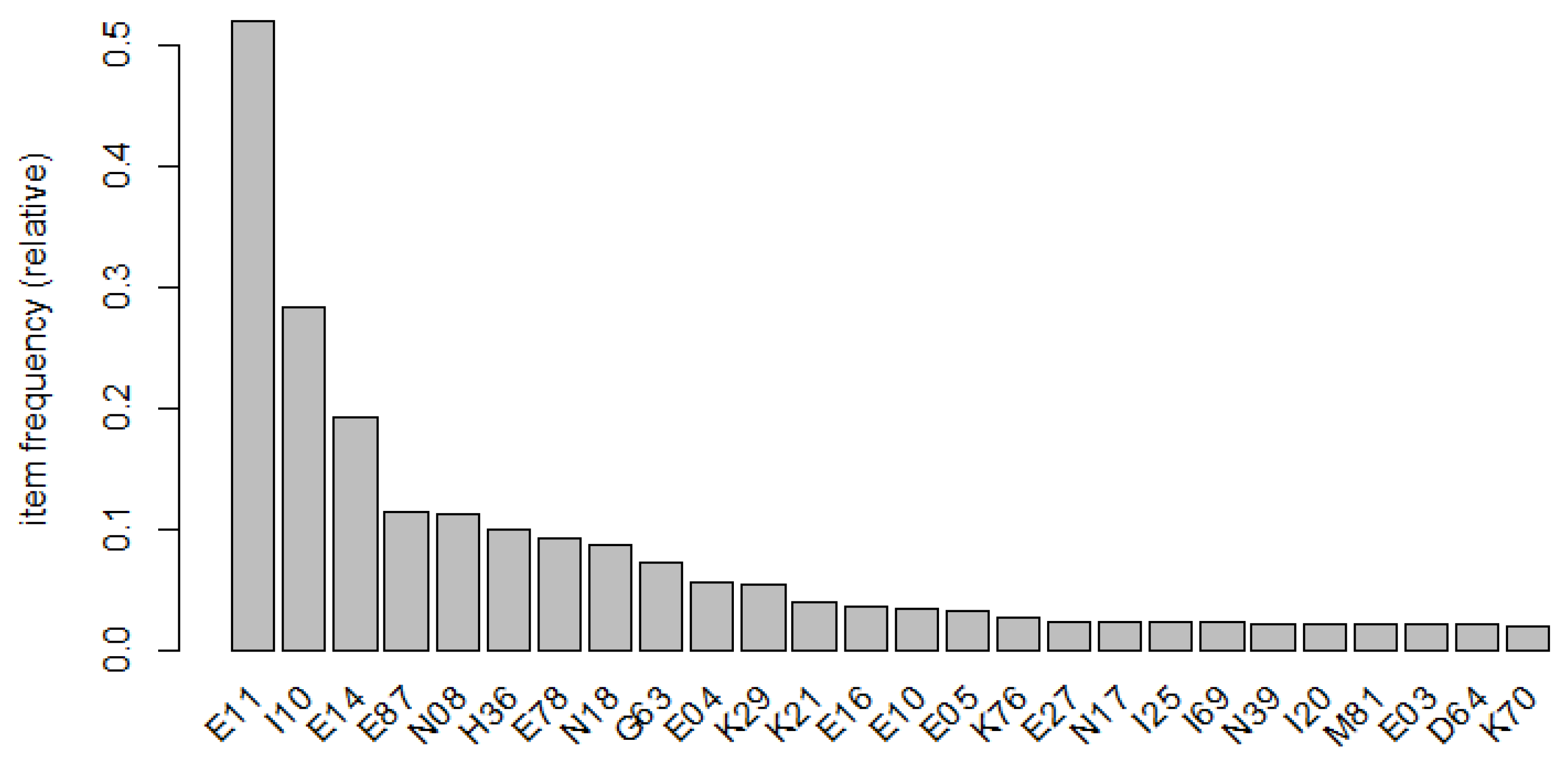
3.1. Characteristics of Study Subjects and Distribution of Comorbidities
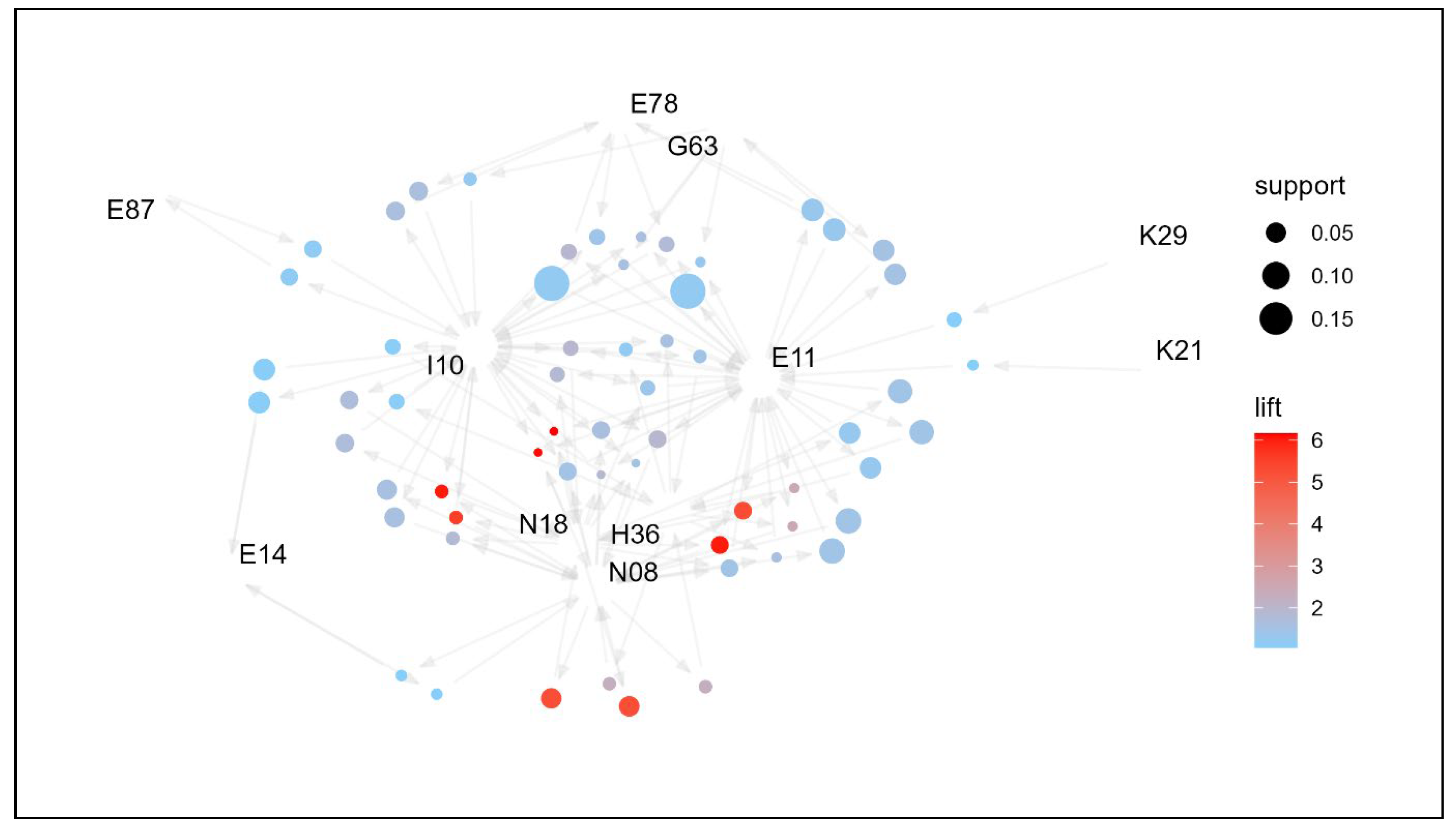
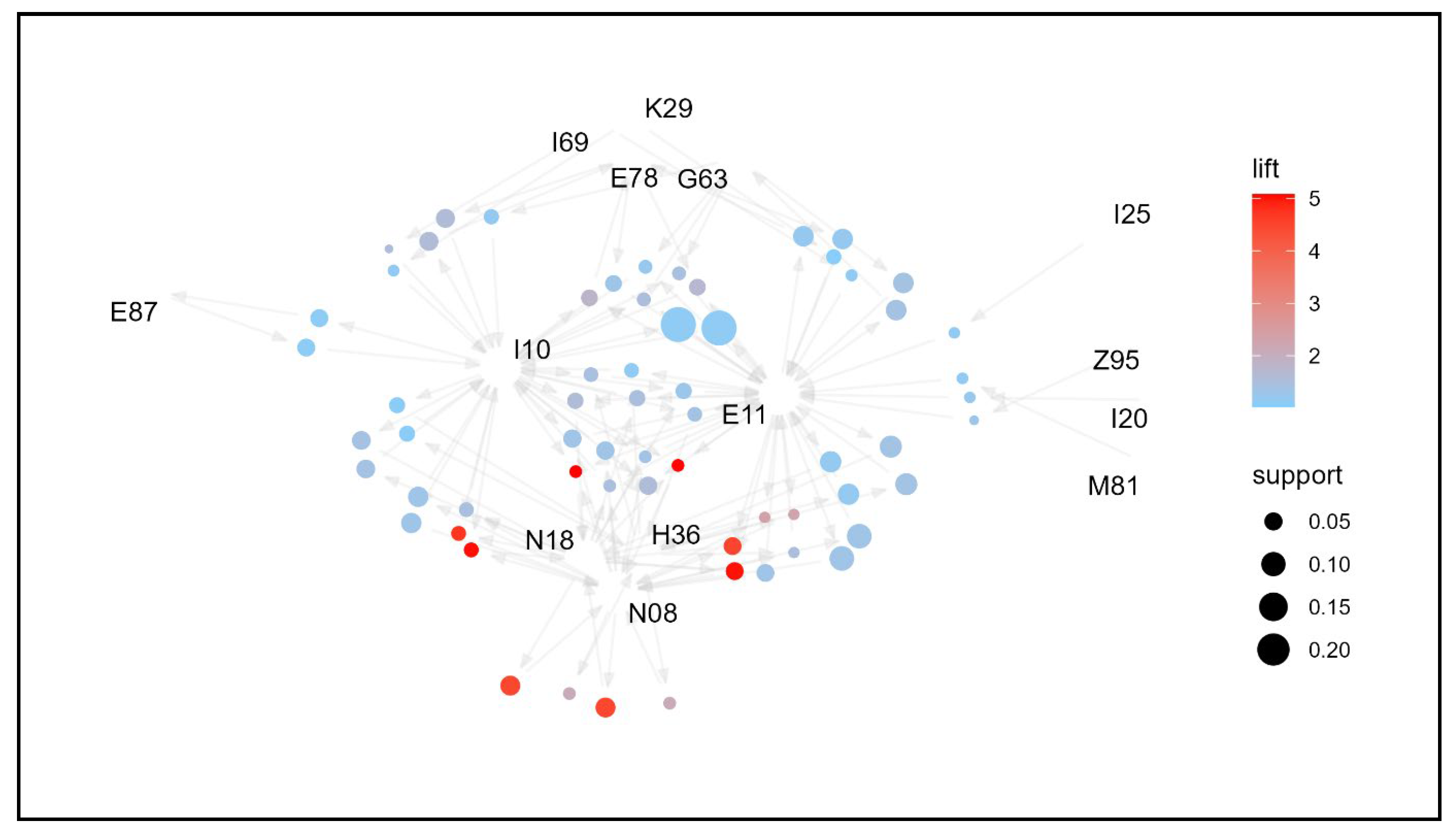
3.2. Overall Association Rule Mining
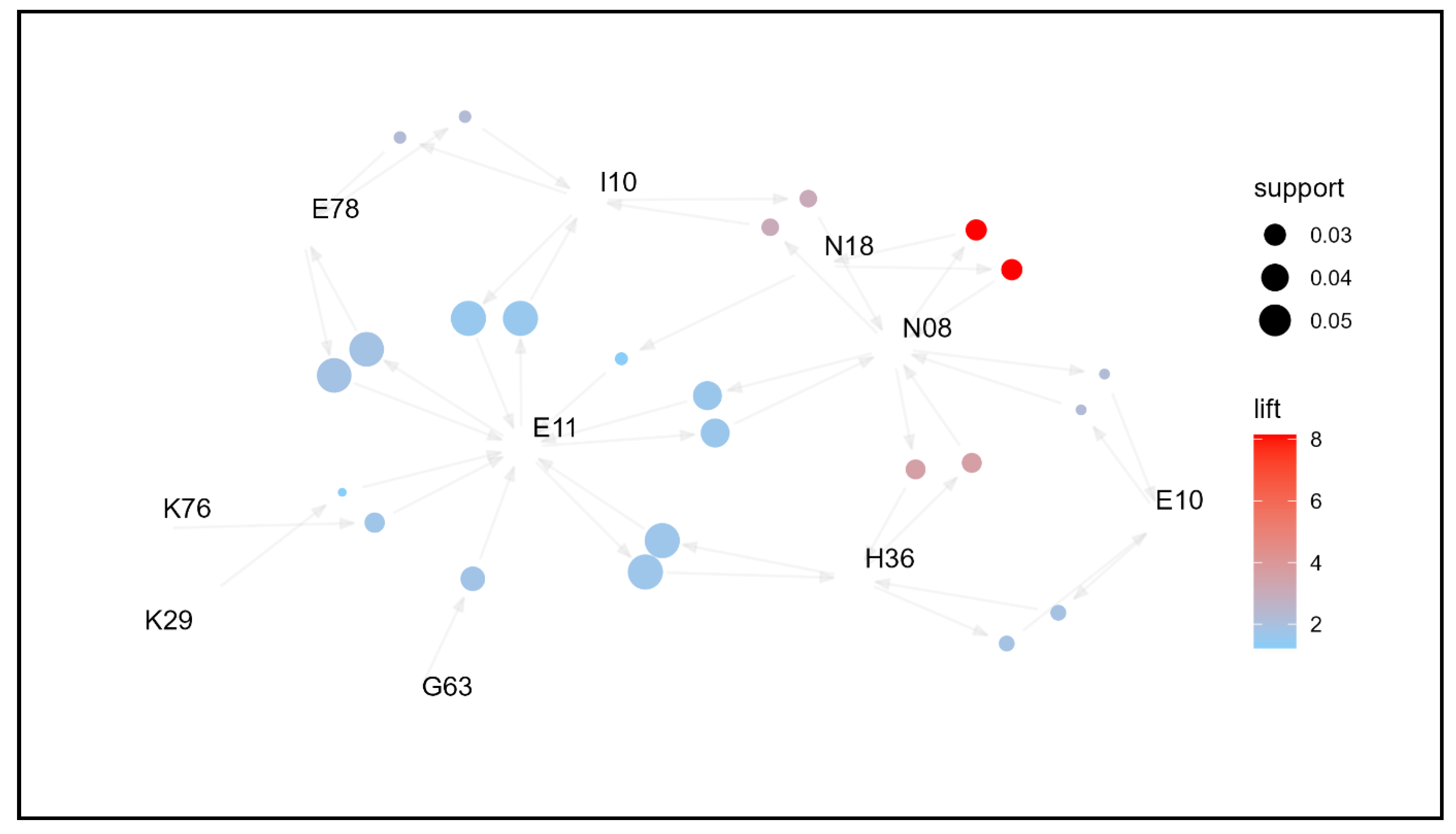
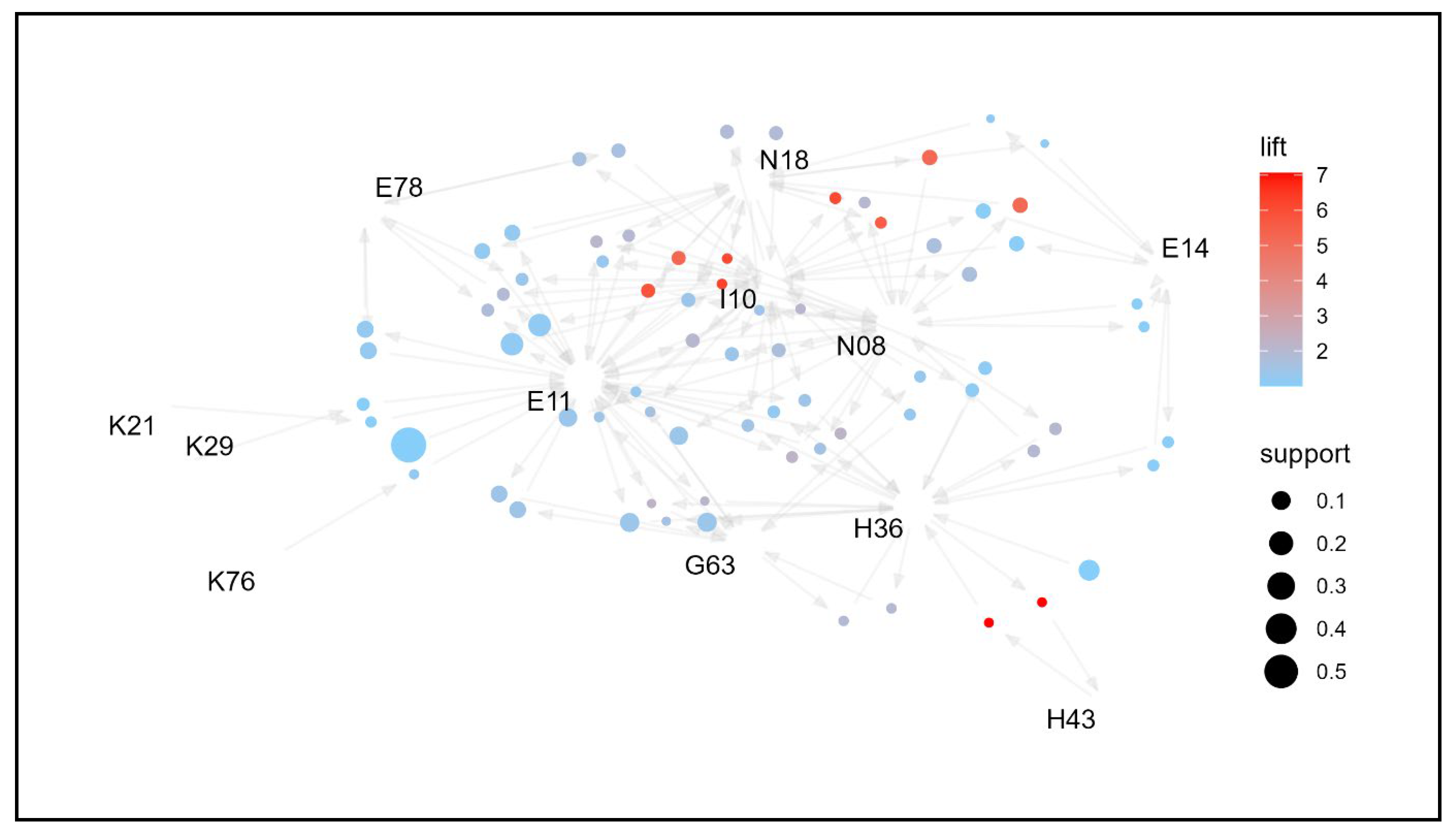
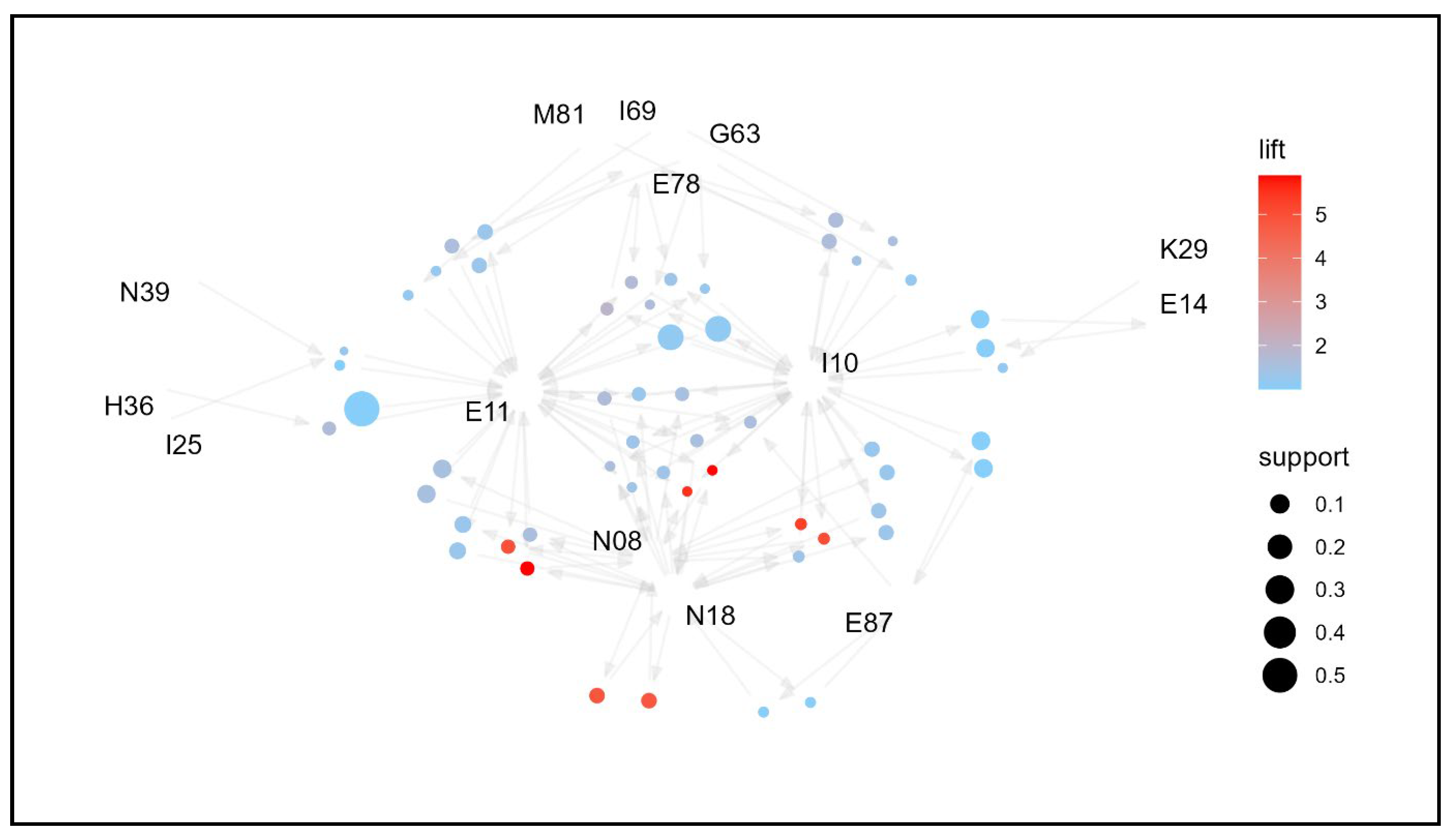
3.3. Comorbidities Association Rule Mining by Age Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Radovick, S. Editorial: Endocrinology and metabolism. Curr. Opin. Pediatr. 2021, 33, 423. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.; Wong, J.L.M.; Sim, Y.J.; Wong, S.S.; Elhassan, S.A.M.; Tan, S.H.; Lim, G.P.L.; Tay, N.W.R.; Annan, N.C.; Bhattamisra, S.K.; et al. Type 1 and 2 diabetes mellitus: A review on current treatment approach and gene therapy as potential intervention. Diabetes Metab. Syndr. 2019, 13, 364–372. [Google Scholar] [CrossRef]
- Goldberg, R.B. Dyslipidemia in Diabetes: When and How to Treat? Endocrinol. Metab. Clin. N. Am. 2022, 51, 603–624. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.-L.; Lin, Y.; Chen, J.-Y. The Association between High-Sensitivity C-Reactive Protein and Metabolic Syndrome in an Elderly Population Aged 50 and Older in a Community Receiving Primary Health Care in Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 13111. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [PubMed]
- Jayasena, C.N.; Anderson, R.A.; Llahana, S.; Barth, J.H.; MacKenzie, F.; Wilkes, S.; Smith, N.; Sooriakumaran, P.; Minhas, S.; Wu, F.C.W.; et al. Society for Endocrinology guidelines for testosterone replacement therapy in male hypogonadism. Clin. Endocrinol. 2022, 96, 200–219. [Google Scholar] [CrossRef] [PubMed]
- Armeni, E.; Paschou, S.A.; Goulis, D.G.; Lambrinoudaki, I. Hormone therapy regimens for managing the menopause and premature ovarian insufficiency. Best. Pr. Res. Clin. Endocrinol. Metab. 2021, 35, 101561. [Google Scholar] [CrossRef]
- Malik, A.; Ananthakrishnan, S. Diabetes Physical Examination. Med. Clin. N. Am. 2022, 106, 483–494. [Google Scholar] [CrossRef]
- Samson, S.L.; Vellanki, P.; Blonde, L.; Christofides, E.A.; Galindo, R.J.; Hirsch, I.B.; Isaacs, S.D.; Izuora, K.E.; Wang, C.C.L.; Twining, C.L.; et al. American Association of Clinical Endocrinology Consensus Statement: Comprehensive Type 2 Diabetes Management Algorithm—2023 Update. Endocr. Pr. 2023, 29, 305–340. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, K.A.; Moon, J.H.; Chon, S.; Kim, D.J.; Kim, N.H.; A Seo, J.; Kim, M.K.; Lim, J.H.; Song, Y.; et al. 2023 Clinical Practice Guidelines for Diabetes Mellitus of the Korean Diabetes Association. Diabetes Metab. J. 2023, 47, 575–594. [Google Scholar] [CrossRef]
- Lee, Y.-K.; Hong, S.O.; Park, S.-J.; Park, M.; Wang, K.; Jo, M.; Oh, J.; Lee, S.A.; Lee, H.J.; Oh, J.; et al. Data resource profile: The Korea National Hospital Discharge In-depth Injury Survey. Epidemiol. Health 2021, 43, e2021052. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, L.S.; Nielsen, J.; Richter, L.; Schmid, D.; Bustos, N.; Braeye, T.; Denissov, G.; Veideman, T.; Luomala, O.; Möttönen, T.; et al. Excess all-cause mortality during the COVID-19 pandemic in Europe—Preliminary pooled estimates from the EuroMOMO network, March to April 2020. Eurosurveillance 2020, 25, 2001214. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Jang, J.; Choi, D.-W.; Jang, S.-I.; Park, E.-C. The effect of shifting medical coverage from National Health Insurance to Medical Aid type I and type II on health care utilization and out-of-pocket spending in South Korea. BMC Health Serv. Res. 2020, 20, 979. [Google Scholar] [CrossRef]
- Das, S.K.; Rahman, M.Z. A Simplified Architecture to Integrate and Interoperate Heterogeneous and Distributed Healthcare Data. In Proceedings of the 2020 23rd International Conference on Computer and Information Technology (ICCIT), Dhaka, Bangladesh, 19–21 December 2020; pp. 1–6. [Google Scholar]
- Sani, A.; Samuel, N.N.P.; Waseso, B.; Gunadi, G.; Haryanto, T. Data Mining on Sales Transaction Data Using the Association Method with Apriori Algorithm. In Proceedings of the 2022 10th International Conference on Cyber and IT Service Management (CITSM), Yogyakarta, Indonesia, 20–21 September 2022; pp. 1–5. [Google Scholar]
- Alcan, D.; Ozdemir, K.; Ozkan, B.; Mucan, A.Y.; Ozcan, T. A Comparative Analysis of Apriori and FP-Growth Algorithms for Market Basket Analysis Using Multi-level Association Rule Mining. In Proceedings of the Industrial Engineering in the COVID-19 Era, Cham, Switzerland, 6 February 2023; pp. 128–137. [Google Scholar]
- Shen, M.; Liu, J.; Wang, K. Effect of Traditional Chinese Medicine on Allergic Rhinitis in Children under Data Mining. Comput. Math. Methods Med. 2022, 2022, 700737. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-F.; Chen, W.-Y.; Lee, C.-T.; Shen, Y.-Y.; Lan, C.-C.; Liu, G.-T.; Kuo, C.-Y.; Chen, M.-L.; Hsieh, P.-C. Combinations of scalp acupuncture location for the treatment of post-stroke hemiparesis: A systematic review and Apriori algorithm-based association rule analysis. Front. Neurosci. 2022, 16, 956854. [Google Scholar] [CrossRef] [PubMed]
- Zemedikun, D.; Gray, L.J.; Khunti, K.; Davies, M.J.; Dhalwani, N.N. Patterns of Multimorbidity in Middle-Aged and Older Adults: An Analysis of the UK Biobank Data. Mayo Clin. Proc. 2018, 93, 857–866. [Google Scholar] [CrossRef]
- Sipahutar, S.Y.K.; Panjaitan, A.A.; Sitanggang, D.P.; Fitriyaningsih, I. Implementation of Association Rules with Apriori Algorithm in Determining Customer Purchase Patterns. In Proceedings of the 2022 IEEE International Conference of Computer Science and Information Technology (ICOSNIKOM), North Sumatra, Indonesia, 19–21 October 2022; pp. 1–6. [Google Scholar]
- Feng, J.; Mu, X.-M.; Ma, L.-L.; Wang, W. Comorbidity Patterns of Older Lung Cancer Patients in Northeast China: An Association Rules Analysis Based on Electronic Medical Records. Int. J. Environ. Res. Public Health 2020, 17, 9119. [Google Scholar] [CrossRef]
- Hahsler, M.; Chelluboina, S.; Hornik, K.; Buchta, C. The arules R-Package Ecosystem: Analyzing Interesting Patterns from Large Transaction Data Sets. J. Mach. Learn. Res. 2011, 12, 2021–2025. [Google Scholar]
- Pasquel, F.J.; Lansang, M.C.; Dhatariya, K.; Umpierrez, G.E. Management of diabetes and hyperglycaemia in the hospital. Lancet Diabetes Endocrinol. 2021, 9, 174–188. [Google Scholar] [CrossRef]
- Kochar, A.; Saini, D.; Poonia, R. Clinical correlation of diabetic retinopathy with nephropathy and neuropathy. Indian. J. Ophthalmol. 2021, 69, 3364–3368. [Google Scholar] [CrossRef]
- Alalawi, F.; Bashier, A. Management of diabetes mellitus in dialysis patients: Obstacles and challenges. Diabetes Metab. Syndr. 2021, 15, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Georgianos, P.I.; Vaios, V.; Eleftheriadis, T.; Papachristou, E.; Liakopoulos, V. Therapeutic Advances in Diabetic Kidney Disease. Int. J. Mol. Sci. 2023, 24, 2803. [Google Scholar] [CrossRef] [PubMed]
- Koye, D.N.; Magliano, D.J.; Nelson, R.G.; Pavkov, M.E. The Global Epidemiology of Diabetes and Kidney Disease. Adv. Chronic Kidney Dis. 2018, 25, 121–132. [Google Scholar] [CrossRef]
- Navaneethan, S.D.; Zoungas, S.; Caramori, M.L.; Chan, J.C.; Heerspink, H.J.; Hurst, C.; Liew, A.; Michos, E.D.; Olowu, W.A.; Sadusky, T.; et al. Diabetes Management in Chronic Kidney Disease: Synopsis of the KDIGO 2022 Clinical Practice Guideline Update. Ann. Intern. Med. 2023, 176, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Lundeen, E.A.; Burke-Conte, Z.; Rein, D.B.; Wittenborn, J.S.; Saaddine, J.; Lee, A.Y.; Flaxman, A.D. Prevalence of Diabetic Retinopathy in the US in 2021. JAMA Ophthalmol 2023, 141, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.-E.; Wong, T.Y. Diabetic retinopathy: Looking forward to 2030. Front. Endocrinol. 2022, 13, 1077669. [Google Scholar] [CrossRef]
- Perais, J.; Agarwal, R.; Evans, J.R.; Loveman, E.; Colquitt, J.L.; Owens, D.; Hogg, R.E.; Lawrenson, J.G.; Takwoingi, Y.; Lois, N. Prognostic factors for the development and progression of proliferative diabetic retinopathy in people with diabetic retinopathy. Cochrane Database Syst. Rev. 2023, 2023, CD013775. [Google Scholar] [CrossRef]
- Do, D.V.; Han, G.; Abariga, S.A.; Sleilati, G.; Vedula, S.S.; Hawkins, B.S. Blood pressure control for diabetic retinopathy. Emergencias 2023, 2023, CD006127. [Google Scholar] [CrossRef]
- Flaxel, C.J.; Adelman, R.A.; Bailey, S.T.; Fawzi, A.; Lim, J.I.; Vemulakonda, G.A.; Ying, G.-S. Diabetic Retinopathy Preferred Practice Pattern®. Ophthalmology 2020, 127, P66–P145. [Google Scholar] [CrossRef]
- Estil, S.; Steinarsson, A.; Einarsson, S.; Aspelund, T.; Stefánsson, E. Diabetic eye screening with variable screening intervals based on individual risk factors is safe and effective in ophthalmic practice. Acta Ophthalmol. 2020, 98, 343–346. [Google Scholar] [CrossRef]
- Wong, T.Y.; Sun, J.; Kawasaki, R.; Ruamviboonsuk, P.; Gupta, N.; Lansingh, V.C.; Maia, M.; Mathenge, W.; Moreker, S.; Muqit, M.M.; et al. Guidelines on Diabetic Eye Care: The International Council of Ophthalmology Recommendations for Screening, Follow-up, Referral, and Treatment Based on Resource Settings. Ophthalmology 2018, 125, 1608–1622. [Google Scholar] [CrossRef]
- Kim, S.S.; Won, J.C.; Kwon, H.S.; Kim, C.H.; Lee, J.H.; Park, T.S.; Ko, K.S.; Cha, B.Y. Prevalence and clinical implications of painful diabetic peripheral neuropathy in type 2 diabetes: Results from a nationwide hospital-based study of diabetic neuropathy in Korea. Diabetes Res. Clin. Pr. 2014, 103, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Oh, J. Clinical spectrum and diagnosis of diabetic neuropathies. Korean J. Intern. Med. 2020, 35, 1059–1069. [Google Scholar] [CrossRef]
- Moon, S.-S.; Kim, C.H.; Kang, S.M.; Kim, E.S.; Oh, T.J.; Yun, J.-S.; Cho, H.C.; Kim, D.J.; Park, T.S. Status of Diabetic Neuropathy in Korea: A National Health Insurance Service-National Sample Cohort Analysis (2006 to 2015). Diabetes Metab. J. 2021, 45, 459–460. [Google Scholar] [CrossRef] [PubMed]
- Pop-Busui, R.; Ang, L.; Boulton, A.J.M.; Feldman, E.L.; Marcus, R.L.; Mizokami-Stout, K.; Singleton, J.R.; Ziegler, D. Diagnosis and Treatment of Painful Diabetic Peripheral Neuropathy. In Diagnosis and Treatment of Painful Diabetic Peripheral Neuropathy; American Diabetes Association: Arlington, VA, USA, 2022. [Google Scholar]
- Agathos, E.; Tentolouris, A.; Eleftheriadou, I.; Katsaouni, P.; Nemtzas, I.; Petrou, A.; Papanikolaou, C.; Tentolouris, N. Effect of α-lipoic acid on symptoms and quality of life in patients with painful diabetic neuropathy. J. Int. Med. Res. 2018, 46, 1779–1790. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, S.; Oishi, M.; Aso, H.; Arai, K.; Sasaki, Y.; Tochikura, N.; Ootsuka, S.; Fukuoka, N.; Ooba, N.; Kikuchi, N. Effects of angiotensin II receptor blockers on serum potassium level and hyperkalemia risk: Retrospective single-centre analysis. Eur. J. Hosp. Pharm. Sci. Pract. 2021, 30, 208–213. [Google Scholar] [CrossRef]
- Whitlock, R.; Leon, S.J.; Manacsa, H.; Askin, N.; Rigatto, C.; Fatoba, S.T.; Farag, Y.M.K.; Tangri, N. The association between dual RAAS inhibition and risk of acute kidney injury and hyperkalemia in patients with diabetic kidney disease: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2023, 38, 2503–2516. [Google Scholar] [CrossRef]
- Araujo-Castro, M.; Parra-Ramírez, P. Diagnosis of primary hyperaldosteronism. Med. Clin. 2022, 158, 424–430. [Google Scholar] [CrossRef]
- Shrimanker, I.; Bhattarai, S. Electrolytes. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Duan, H.; Cai, X.; Luan, Y.; Yang, S.; Yang, J.; Dong, H.; Zeng, H.; Shao, L. Regulation of the Autonomic Nervous System on Intestine. Front. Physiol. 2021, 12, 700129. [Google Scholar] [CrossRef]
- Kim, H.-S.; Kim, J.H. Proceed with Caution When Using Real World Data and Real World Evidence. J. Korean Med. Sci. 2019, 34, e28. [Google Scholar] [CrossRef]
- Kim, H.-S.; Kim, D.-J.; Yoon, K.-H. Medical Big Data Is Not Yet Available: Why We Need Realism Rather than Exaggeration. Endocrinol. Metab. 2019, 34, 349–354. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Male | Female | p |
|---|---|---|---|
| N (%) or Mean ± SD | N (%) or Mean ± SD | ||
| N | 32,140 | 36,375 | |
| Age (year) | 58.6 ± 15.0 | 61.2 ± 17.2 | <0.001 |
| Age group | <0.001 | ||
| 19–44 | 5653 (17.6%) | 6575 (18.1%) | |
| 45–64 | 14,523 (45.2%) | 11,813 (32.5%) | |
| 65–74 | 6815 (21.2%) | 8552 (23.5%) | |
| ≥75 | 5149 (16.0%) | 9435 (25.9%) | |
| Insurance type | <0.001 | ||
| National health | 26,216 (81.6%) | 30,728 (84.5%) | |
| Medicaid type 1 | 4759 (14.8%) | 4803 (13.2%) | |
| Medicaid type 2 | 663 (2.1%) | 600 (1.6%) | |
| Others | 502 (1.6%) | 244 (0.7%) | |
| Admission route | 0.862 | ||
| Emergency | 9799 (30.5%) | 11,048 (30.4%) | |
| Outpatient | 22,310 (69.4%) | 25,288 (69.5%) | |
| Others | 31 (0.1%) | 39 (0.1%) | |
| Treatment outcome | <0.001 | ||
| Improved | 30,566 (95.1%) | 34,958 (96.1%) | |
| Not improved | 1085 (3.4%) | 1032 (2.8%) | |
| Death | 453 (1.4%) | 350 (1.0%) | |
| Others | 36 (0.1%) | 35 (0.1%) | |
| Length of stay (day) | 12.0 ± 19.0 | 9.6 ± 16.5 | <0.001 |
| Death Y/N | <0.001 | ||
| Yes | 453 (1.4%) | 350 (1.0%) | |
| No | 31,687 (98.6%) | 36,025 (99.0%) | |
| Operation Y/N | 0.010 | ||
| Yes | 5520 (17.2%) | 6521 (17.9%) | |
| No | 26,620 (82.8%) | 29,854 (82.1%) | |
| Comorbidity Y/N | <0.001 | ||
| Yes | 26,522 (82.5%) | 29,162 (80.2%) | |
| No | 5618 (17.5%) | 7213 (19.8%) | |
| Bed size | <0.001 | ||
| 100–299 | 9400 (29.2%) | 9812 (27.0%) | |
| 300–499 | 4453 (13.9%) | 5153 (14.2%) | |
| 500–999 | 13,784 (42.9%) | 16,306 (44.8%) | |
| ≥1000 | 4503 (14.0%) | 5104 (14.0%) |
| No | Rules | N | Support | Confidence | Lift | IS |
|---|---|---|---|---|---|---|
| 1 | N08 → N18 | 3523 | 0.051 | 0.457 | 5.239 | 0.519 |
| 2 | N18 → N08 | 3523 | 0.051 | 0.589 | 5.239 | 0.519 |
| 3 | E11, N18 → N08 | 2683 | 0.039 | 0.677 | 6.017 | 0.485 |
| 4 | I10 → E11 | 12,259 | 0.179 | 0.632 | 1.217 | 0.467 |
| 5 | E11 → I10 | 12,259 | 0.179 | 0.344 | 1.217 | 0.467 |
| 6 | E11, N08 → N18 | 2683 | 0.039 | 0.462 | 5.294 | 0.455 |
| 7 | I10, N08 → N18 | 1811 | 0.026 | 0.525 | 6.018 | 0.399 |
| 8 | I10, N18 → N08 | 1811 | 0.026 | 0.626 | 5.561 | 0.383 |
| 9 | E11, I10, N08 → N18 | 1429 | 0.021 | 0.537 | 6.159 | 0.358 |
| 10 | E11, I10, N18 → N08 | 1429 | 0.021 | 0.689 | 6.128 | 0.358 |
| 11 | E11 → N08 | 5808 | 0.085 | 0.163 | 1.451 | 0.351 |
| 12 | N08 → E11 | 5808 | 0.085 | 0.754 | 1.451 | 0.351 |
| 13 | H36 → E11 | 5256 | 0.077 | 0.757 | 1.457 | 0.334 |
| 14 | E11 → H36 | 5256 | 0.077 | 0.148 | 1.457 | 0.334 |
| 15 | G63 → E11 | 3973 | 0.058 | 0.791 | 1.522 | 0.297 |
| 16 | E11 → G63 | 3973 | 0.058 | 0.112 | 1.522 | 0.297 |
| 17 | E78 → E11 | 4406 | 0.064 | 0.683 | 1.314 | 0.291 |
| 18 | E11 → E78 | 4406 | 0.064 | 0.124 | 1.314 | 0.291 |
| 19 | N08 → I10 | 3449 | 0.050 | 0.448 | 1.581 | 0.282 |
| 20 | I10 → N08 | 3449 | 0.050 | 0.178 | 1.581 | 0.282 |
| 21 | E11, I10 → N08 | 2659 | 0.039 | 0.217 | 1.928 | 0.274 |
| 22 | N18 → E11 | 3964 | 0.058 | 0.663 | 1.277 | 0.272 |
| 23 | E11 → N18 | 3964 | 0.058 | 0.111 | 1.277 | 0.272 |
| 24 | E78 → I10 | 3008 | 0.044 | 0.466 | 1.647 | 0.269 |
| 25 | I10 → E78 | 3008 | 0.044 | 0.155 | 1.647 | 0.269 |
| 26 | I10 → N18 | 2895 | 0.042 | 0.149 | 1.711 | 0.269 |
| 27 | N18 → I10 | 2895 | 0.042 | 0.484 | 1.711 | 0.269 |
| 28 | E14 → I10 | 4079 | 0.060 | 0.309 | 1.093 | 0.255 |
| 29 | I10 → E14 | 4079 | 0.060 | 0.210 | 1.093 | 0.255 |
| 30 | E11, N08 → I10 | 2659 | 0.039 | 0.458 | 1.617 | 0.251 |
| 31 | E11, I10 → E78 | 2226 | 0.032 | 0.182 | 1.928 | 0.250 |
| 32 | H36 → N08 | 1778 | 0.026 | 0.256 | 2.275 | 0.243 |
| 33 | N08 → H36 | 1778 | 0.026 | 0.231 | 2.275 | 0.243 |
| 34 | E11, I10 → N18 | 2073 | 0.030 | 0.169 | 1.938 | 0.242 |
| 35 | E11, E78 → I10 | 2226 | 0.032 | 0.505 | 1.785 | 0.241 |
| 36 | I10, N08 → E11 | 2659 | 0.039 | 0.771 | 1.484 | 0.240 |
| 37 | N08, N18 → E11 | 2683 | 0.039 | 0.762 | 1.466 | 0.240 |
| 38 | E11, N18 → I10 | 2073 | 0.030 | 0.523 | 1.847 | 0.236 |
| 39 | E11, N08 → H36 | 1467 | 0.021 | 0.253 | 2.491 | 0.231 |
| 40 | E11, H36 → N08 | 1467 | 0.021 | 0.279 | 2.481 | 0.230 |
| 41 | N08, N18 → I10 | 1811 | 0.026 | 0.514 | 1.816 | 0.219 |
| 42 | E78, I10 → E11 | 2226 | 0.032 | 0.740 | 1.425 | 0.215 |
| 43 | E87 → I10 | 2614 | 0.038 | 0.333 | 1.178 | 0.212 |
| 44 | I10 → E87 | 2614 | 0.038 | 0.135 | 1.178 | 0.212 |
| 45 | I10, N18 → E11 | 2073 | 0.030 | 0.716 | 1.379 | 0.204 |
| 46 | H36, I10 → E11 | 1789 | 0.026 | 0.825 | 1.589 | 0.204 |
| 47 | E11, N08, N18 → I10 | 1429 | 0.021 | 0.533 | 1.882 | 0.198 |
| 48 | E11, I10 → H36 | 1789 | 0.026 | 0.146 | 1.439 | 0.194 |
| 49 | E11, I10 → G63 | 1483 | 0.022 | 0.121 | 1.650 | 0.189 |
| 50 | H36 → I10 | 2168 | 0.032 | 0.312 | 1.102 | 0.187 |
| 51 | I10 → H36 | 2168 | 0.032 | 0.112 | 1.102 | 0.187 |
| 52 | G63, I10 → E11 | 1483 | 0.022 | 0.829 | 1.596 | 0.186 |
| 53 | H36, N08 → E11 | 1467 | 0.021 | 0.825 | 1.588 | 0.184 |
| 54 | G63 → I10 | 1789 | 0.026 | 0.356 | 1.258 | 0.181 |
| 55 | I10, N08, N18 → E11 | 1429 | 0.021 | 0.789 | 1.519 | 0.178 |
| 56 | K29 → E11 | 2052 | 0.030 | 0.549 | 1.056 | 0.178 |
| 57 | E11, H36 → I10 | 1789 | 0.026 | 0.340 | 1.202 | 0.177 |
| 58 | E11, G63 → I10 | 1483 | 0.022 | 0.373 | 1.319 | 0.169 |
| 59 | N08 → E14 | 1560 | 0.023 | 0.202 | 1.052 | 0.155 |
| 60 | E14 → N08 | 1560 | 0.023 | 0.118 | 1.052 | 0.155 |
| 61 | K21 → E11 | 1533 | 0.022 | 0.553 | 1.064 | 0.154 |
| ICD-10 | Code Description | Age Group | ||||
|---|---|---|---|---|---|---|
| 19~44 | 45~64 | 65~74 | 75+ | All Age | ||
| E10 | Type 1 diabetes mellitus | O | ||||
| E11 | Type 2 diabetes mellitus | O | O | O | O | O |
| E14 | Unspecified diabetes mellitus | O | O | O | ||
| E78 | Disorders of lipoprotein metabolism and other lipidemias | O | O | O | O | O |
| E87 | Other disorders of fluid, electrolyte, and acid-base balance | O | O | O | ||
| G63 | Polyneuropathy in diseases classified elsewhere | O | O | O | O | O |
| H36 | Retinal disorders in diseases classified elsewhere | O | O | O | O | O |
| H43 | Disorders of vitreous body | O | ||||
| I10 | Essential (primary) hypertension | O | O | O | O | O |
| I20 | Angina pectoris | O | ||||
| I25 | Chronic ischemic heart disease | O | O | |||
| I48 | Atrial fibrillation and flutter | |||||
| I69 | Sequelae of cerebrovascular disease | O | O | |||
| K21 | Gastro-esophageal reflux disease | O | O | |||
| K29 | Gastritis and duodenitis | O | O | O | O | O |
| K76 | Other diseases of liver | O | O | |||
| M81 | Osteoporosis without pathological fracture | O | O | |||
| N08 | Glomerular disorders in diseases classified elsewhere | O | O | O | O | O |
| N17 | Acute renal failure | |||||
| N18 | Chronic kidney disease | O | O | O | O | O |
| N39 | Other disorders of urinary system | O | ||||
| Z95 | Presence of cardiac and vascular implants and grafts | O | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-S.; Kim, H.-S. Comorbidity Patterns and Management in Inpatients with Endocrine Diseases by Age Groups in South Korea: Nationwide Data. J. Pers. Med. 2024, 14, 42. https://doi.org/10.3390/jpm14010042
Kim S-S, Kim H-S. Comorbidity Patterns and Management in Inpatients with Endocrine Diseases by Age Groups in South Korea: Nationwide Data. Journal of Personalized Medicine. 2024; 14(1):42. https://doi.org/10.3390/jpm14010042
Chicago/Turabian StyleKim, Sung-Soo, and Hun-Sung Kim. 2024. "Comorbidity Patterns and Management in Inpatients with Endocrine Diseases by Age Groups in South Korea: Nationwide Data" Journal of Personalized Medicine 14, no. 1: 42. https://doi.org/10.3390/jpm14010042
APA StyleKim, S. -S., & Kim, H. -S. (2024). Comorbidity Patterns and Management in Inpatients with Endocrine Diseases by Age Groups in South Korea: Nationwide Data. Journal of Personalized Medicine, 14(1), 42. https://doi.org/10.3390/jpm14010042