
The Morphology of Nasal Polyps in Different Age Groups: Histopathological Features

 ,
,  ,
,  , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
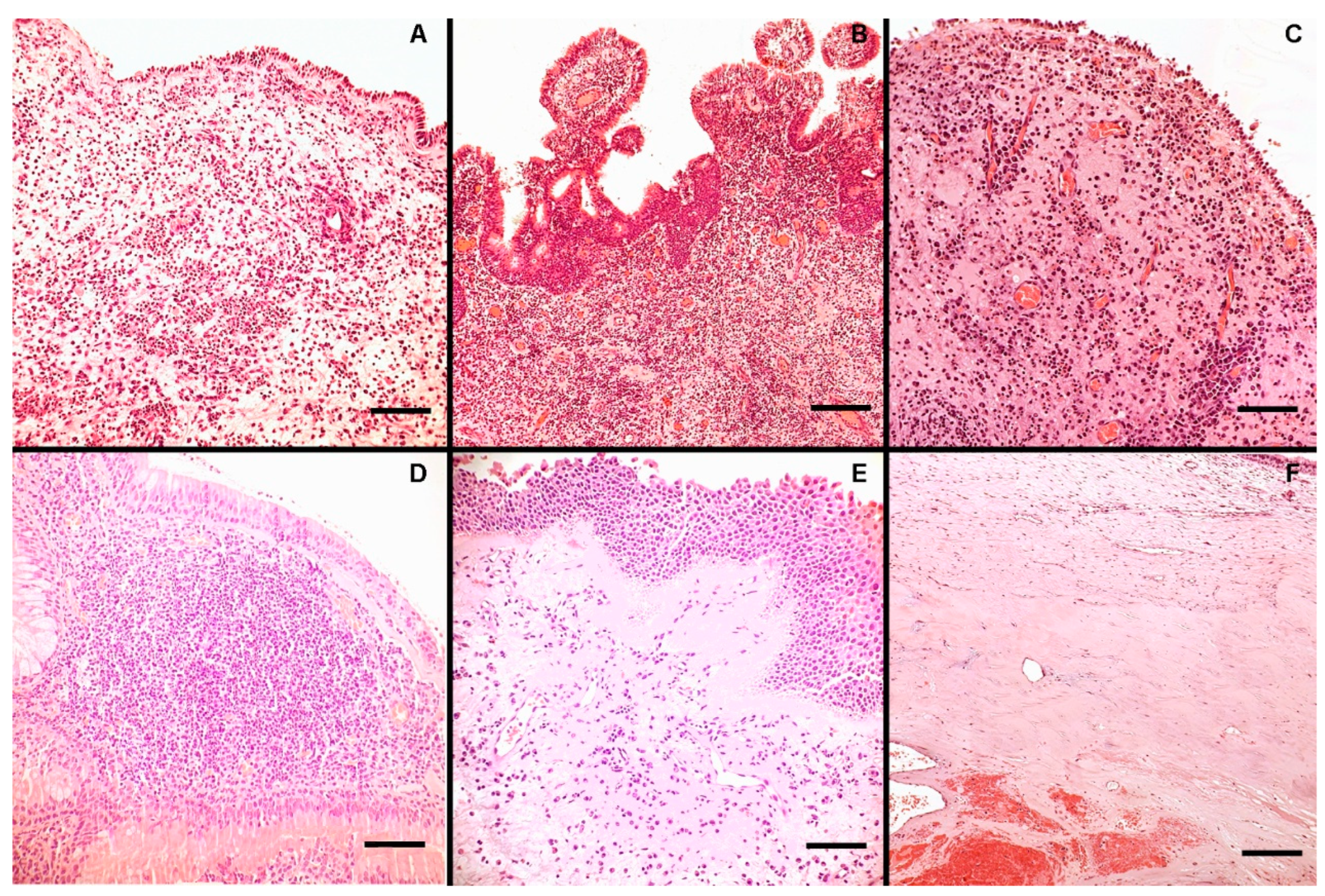
Patients’ Characteristics and Histological and Inflammatory Features of the NPs
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinol. J. 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, K.; Sudarsan, S.S.; Rajkumar, I.; Shree, K.R. Is Nasal Polyp in Pediatric Cases Same as in Adult Population? Int. J. Head. Neck Surg. 2021, 12, 98–100. [Google Scholar] [CrossRef]
- Segal, N.; Gluk, O.; Puterman, M. Nasal polyps in the pediatric population. B-ENT 2012, 8, 265–267. [Google Scholar] [PubMed]
- Frosini, P.; Picarella, G.; De Campora, E. Antrochoanal polyp: Analysis of 200 cases. Acta Otorhinolaryngol. Ital. 2009, 29, 21–26. [Google Scholar] [PubMed]
- Al-Mazrou, K.; Bukhari, M.; Al-Fayez, A. Characteristics of antrochoanal polyps in the pediatric age group. Ann. Thorac. Med. 2009, 4, 133. [Google Scholar] [CrossRef] [PubMed]
- Johansson, L.; Åkerlund, A.; Melén, I.; Holmberg, K.; Bende, M. Prevalence of Nasal Polyps in Adults: The Skovde Population-Based Study. Ann. Otol. Rhinol. Laryngol. 2003, 112, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Rasouli, A.A.; Dyamely, Z. Prevalence of nasal polyps in chronic rhinosinusitis patients undergoing functional endoscopic sinus surgery. Interdiscip. Approaches Med. 2021, 2, 67–71. [Google Scholar] [CrossRef]
- Raciborski, F.; Arcimowicz, M.; Samolinski, B.; Pinkas, W.; Samel-Kowalik, P.; Śliwczyński, A. Recorded prevalence of nasal polyps increases with age. Adv. Dermatol. Allergol. 2021, 38, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Hakim, M.L.; Kristyono, I. Chronic rhinosinusitis patient with nasal polyps at Dr. Soetomo General Academic Hospital Center. Bali Med. J. 2022, 11, 766–770. [Google Scholar] [CrossRef]
- Sowmya, R.; Mahesh, D. A study on aetiopathogenesis and management of nasal polyposis. Int. J. Integr. Med. Sci. 2019, 6, 839–844. [Google Scholar] [CrossRef]
- Mainz, J.G.; Koitschev, A. Pathogenesis and Management of Nasal Polyposis in Cystic Fibrosis. Curr. Allergy Asthma Rep. 2012, 12, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Chiarella, E.; Lombardo, N.; Lobello, N.; Aloisio, A.; Aragona, T.; Pelaia, C.; Scicchitano, S.; Bond, H.M.; Mesuraca, M. Nasal Polyposis: Insights in Epithelial-Mesenchymal Transition and Differentiation of Polyp Mesenchymal Stem Cells. Int. J. Mol. Sci. 2020, 21, 6878. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Gevaert, P.; Holtappels, G.; Cuvelier, C.; Van Cauwenberge, P. Nasal Polyposis: From Cytokines to Growth. Am. J. Rhinol. 2000, 14, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Sarisoy, B.A.; Eken, M.; Oktay, A.Z.; Paksoy, M.; Sanli, A. Myeloperoxydase Expression in The Pathogenesis of Nasal Polyps. Indian. J. Otolaryngol. Head. Neck Surg. 2011, 63, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Park, J.; Jeon, C.; Choi, J.; Lee, S. Quantitative Analysis of Eotaxin and RANTES Messenger RNA in Nasal Polyps: Association of Tissue and Nasal Eosinophils. Laryngoscope 2000, 110, 1353–1357. [Google Scholar] [CrossRef] [PubMed]
- Min, Y.G.; Chung, J.W.; Shin, J.S.; Chi, J.G. Histologic Structure of Antrochoanal Polyps. Acta Oto-Laryngol. 1995, 115, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Bayar Muluk, N.; Cingi, C.; Scadding, G.K.; Scadding, G. Chronic Rhinosinusitis—Could Phenotyping or Endotyping Aid Therapy? Am. J. Rhinol. Allergy 2019, 33, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Anjos CPG dos Vasconcelos, A.C.; Crosara, P.F.T.B.; Anjos GC dos Becker, C.G.; Guimarães, R.E.S. Apoptose em pólipos nasais eosinofílicos submetidos in vitro ao tratamento com mitomicina C. Braz. J. Otorhinolaryngol. 2012, 78, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, T.; Sakashita, M.; Haruna, T.; Asaka, D.; Takeno, S.; Ikeda, H.; Nakayama, T.; Seki, N.; Ito, S.; Murata, J.; et al. Novel scoring system and algorithm for classifying chronic rhinosinusitis: The JESREC Study. Allergy 2015, 70, 995–1003. [Google Scholar] [CrossRef]
- Gan, W.; Zhang, H.; Yang, F.; Liu, S.; Liu, F.; Meng, J. The influence of nasal microbiome diversity and inflammatory patterns on the prognosis of nasal polyps. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Mirza, N.; Kroger, H.; Doty, R.L. Influence of Age on the ‘Nasal Cycle’. Laryngoscope 1997, 107, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Vaitkus, J.; Vitkauskienė, A.; Simuntis, R.; Vaitkus, Ž.; Šiupšinskienė, N.; Vaitkus, S. Chronic Rhinosinusitis with Nasal Polyps: Age and Disease Severity Differences in the Levels of Inflammatory Markers. Medicina 2021, 57, 282. [Google Scholar] [CrossRef] [PubMed]
- Larsen, K.; Tos, M. The Estimated Incidence of Symptomatic Nasal Polyps. Acta Oto-Laryngol. 2002, 122, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Cavaliere, C.; Masieri, S.; Begvarfaj, E.; Loperfido, A.; Baroncelli, S.; Cascone, F.; Ciofalo, A. Long-Term Perspectives on Chronic Rhinosinusitis with Nasal Polyps: Evaluating Recurrence Rates after Functional Endoscopic Sinus Surgery in the Biologics Era—A 5-Year Follow-Up Study. J. Pers. Med. 2024, 14, 297. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.N.; Lee, W.H.; Lee, S.H.; Rhee, C.-S.; Lee, C.H.; Kim, J.-W. Chronic rhinosinusitis with nasal polyps is associated with chronic otitis media in the elderly. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 1463–1470. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Ahn, H.S.; Kang, T.; Bachert, C.; Song, W.-J. Nasal polyps and future risk of head and neck cancer: A nationwide population-based cohort study. J. Allergy Clin. Immunol. 2019, 144, 1004–1010.e4. [Google Scholar] [CrossRef] [PubMed]
- Dell’aquila, M.; Fiorentino, V.; Martini, M.; Capodimonti, S.; Cenci, T.; Lombardi, C.P.; Raffaelli, M.; Pontecorvi, A.; Fadda, G.; Pantanowitz, L.; et al. How limited molecular testing can also offer diagnostic and prognostic evaluation of thyroid nodules processed with liquid-based cytology: Role of TERT promoter and BRAF V600E mutation analysis. Cancer Cytopathol. 2021, 129, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.X.; Cao, P.P.; Li, Z.Y.; Zhai, G.T.; Liao, B.; Lu, X.; Liu, Z. A retrospective study of changes of histopathology of nasal polyps in adult Chinese in central China. Rhinol. J. 2019, 57, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Loftus, P.A.; Wise, S.K.; Nieto, D.; Panella, N.; Aiken, A.; DelGaudio, J.M. Intranasal volume increases with age: Computed tomography volumetric analysis in adults. Laryngoscope 2016, 126, 2212–2215. [Google Scholar] [CrossRef]
- Kalmovich, L.M.; Elad, D.; Zaretsky, U.; Adunsky, A.; Chetrit, A.; Sadetzki, S.; Segal, S.; Wolf, M. Endonasal Geometry Changes in Elderly People: Acoustic Rhinometry Measurements. J. Gerontol. Ser. A 2005, 60, 396–398. [Google Scholar] [CrossRef]
- Edelstein, D.R. Aging of the Normal Nose in Adults. Laryngoscope 1996, 106, 1–25. [Google Scholar] [CrossRef]
- Valdés, C.J.; Tewfik, M.A. Rhinosinusitis and Allergies in Elderly Patients. Clin. Geriatr. Med. 2018, 34, 217–231. [Google Scholar] [CrossRef]
- Merrill, T.; Kanaan, A. Managing Chronic Rhinosinusitis with Nasal Polyps in the Elderly: Challenges and Solutions. Clin. Interv. Aging 2022, 17, 685–698. [Google Scholar] [CrossRef]
- Renteria, A.E.; Mfuna Endam, L.; Desrosiers, M. Do Aging Factors Influence the Clinical Presentation and Management of Chronic Rhinosinusitis? Otolaryngol. Neck Surg. 2017, 156, 598–605. [Google Scholar] [CrossRef]
- Cho, S.H.; Hong, S.J.; Han, B.; Lee, S.H.; Suh, L.; Norton, J.; Lin, D.; Conley, D.B.; Chandra, R.; Kern, R.C.; et al. Age-related differences in the pathogenesis of chronic rhinosinusitis. J. Allergy Clin. Immunol. 2012, 129, 858–860.e2. [Google Scholar] [CrossRef]
- Bende, M. Blood Flow with 133 Xe in Human Nasal Mucosa in Relation to Age, Sex and Body Position. Acta Oto-Laryngol. 1983, 96, 175–179. [Google Scholar] [CrossRef]
- DelGaudio, J.M.; Panella, N.J. Presbynasalis. Int. Forum Allergy Rhinol 2016, 6, 1083–1107. [Google Scholar] [CrossRef]
- Bauer, A.M.; Turner, J.H. Personalized Medicine in Chronic Rhinosinusitis. Immunol. Allergy Clin. N. Am. 2020, 40, 281–293. [Google Scholar] [CrossRef]
- Shun, C.T.; Lin, S.K.; Hong, C.Y.; Lin, C.F.; Liu, C.M. Sirtuin 6 Modulates Hypoxia-Induced Autophagy in Nasal Polyp Fibroblasts via Inhibition of Glycolysis. Am. J. Rhinol. Allergy 2016, 30, 179–185. [Google Scholar] [CrossRef]
- Moon, Y.M.; Kang, H.J.; Cho, J.S.; Park, I.H.; Lee, H.M. Nox4 Mediates Hypoxia-Stimulated Myofibroblast Differentiation in Nasal Polyp-Derived Fibroblasts. Int. Arch. Allergy Immunol. 2012, 159, 399–409. [Google Scholar] [CrossRef]
- Lin, S.K.; Shun, C.T.; Kok, S.H.; Wang, C.C.; Hsiao, T.Y.; Liu, C.M. Hypoxia-Stimulated Vascular Endothelial Growth Factor Production in Human Nasal Polyp Fibroblasts. Arch. Otolaryngol. Neck Surg. 2008, 134, 522–527. [Google Scholar] [CrossRef]
- Ho, J.C.; Chan, K.N.; Hu, W.H.; Lam, W.K.; Zheng, L.; Tipoe, G.L.; Sun, J.; Leung, R.; Tsang, K.W. The Effect of Aging on Nasal Mucociliary Clearance, Beat Frequency, and Ultrastructure of Respiratory Cilia. Am. J. Respir. Crit. Care Med. 2001, 163, 983–988. [Google Scholar] [CrossRef]
- de Oliveira-Maul, J.P.; de Carvalho, H.B.; Goto, D.M.; Maia, R.M.; Fló, C.; Barnabé, V.; Franco, D.R.; Benabou, S.; Perracini, M.R.; Jacob-Filho, W.; et al. Aging, Diabetes, and Hypertension Are Associated with Decreased Nasal Mucociliary Clearance. Chest 2013, 143, 1091–1097. [Google Scholar] [CrossRef]
- Brescia, G.; Barion, U.; Pedruzzi, B.; Cinetto, F.; Giacomelli, L.; Pendolino, A.L.; Marino, F.; Manzato, E.; Martini, A.; Marioni, G. Sinonasal Polyposis in the Elderly. Am. J. Rhinol. Allergy 2016, 30, e153–e156. [Google Scholar] [CrossRef]
- Yang, S.K.; Cho, S.-H.; Kim, D.W. Interpretation of Clinical Efficacy of Biologics in Chronic Rhinosinusitis With Nasal Polyps via Understanding the Local and Systemic Pathomechanisms. Allergy Asthma Immunol. Res. 2022, 14, 465–478. [Google Scholar] [CrossRef]
- Galletti, C.; Ragusa, M.; Sireci, F.; Ciodaro, F.; Barbieri, M.A.; Giunta, G.; Grigaliute, E.; Immordino, A.; Lorusso, F.; Dispenza, F.; et al. Dupilumab in chronic rhinosinusitis with nasal polyps: Real life data in a multicentric Sicilian experience. Am. J. Otolaryngol. 2024, 45, 104106. [Google Scholar] [CrossRef]
- Galletti, C.; Barbieri, M.A.; Ciodaro, F.; Freni, F.; Galletti, F.; Spina, E.; Galletti, B. Effectiveness and Safety Profile of Dupilumab in Chronic Rhinosinusitis with Nasal Polyps: Real-Life Data in Tertiary Care. Pharmaceuticals 2023, 16, 630. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Younger | Adult | Elderly | ||
|---|---|---|---|---|---|---|
| Number of patients, n (%) | 143 (100) | 6 (4.2) | 58 (40.6) | 79 (55.2) | ||
| Age, mean (±SD) | 51.7 (15.8) | 12.7 (4.5) | 45.9 (9.2) | 70.3 (7.5) | ||
| Male gender, n (%) | 110 (76.9) | 3 (50) | 46 (79.3) | 61 (77.2) | ||
| Female gender, n (%) | 33 (23.1) | 3 (50) | 12 (20.7) | 18 (22.8) | ||
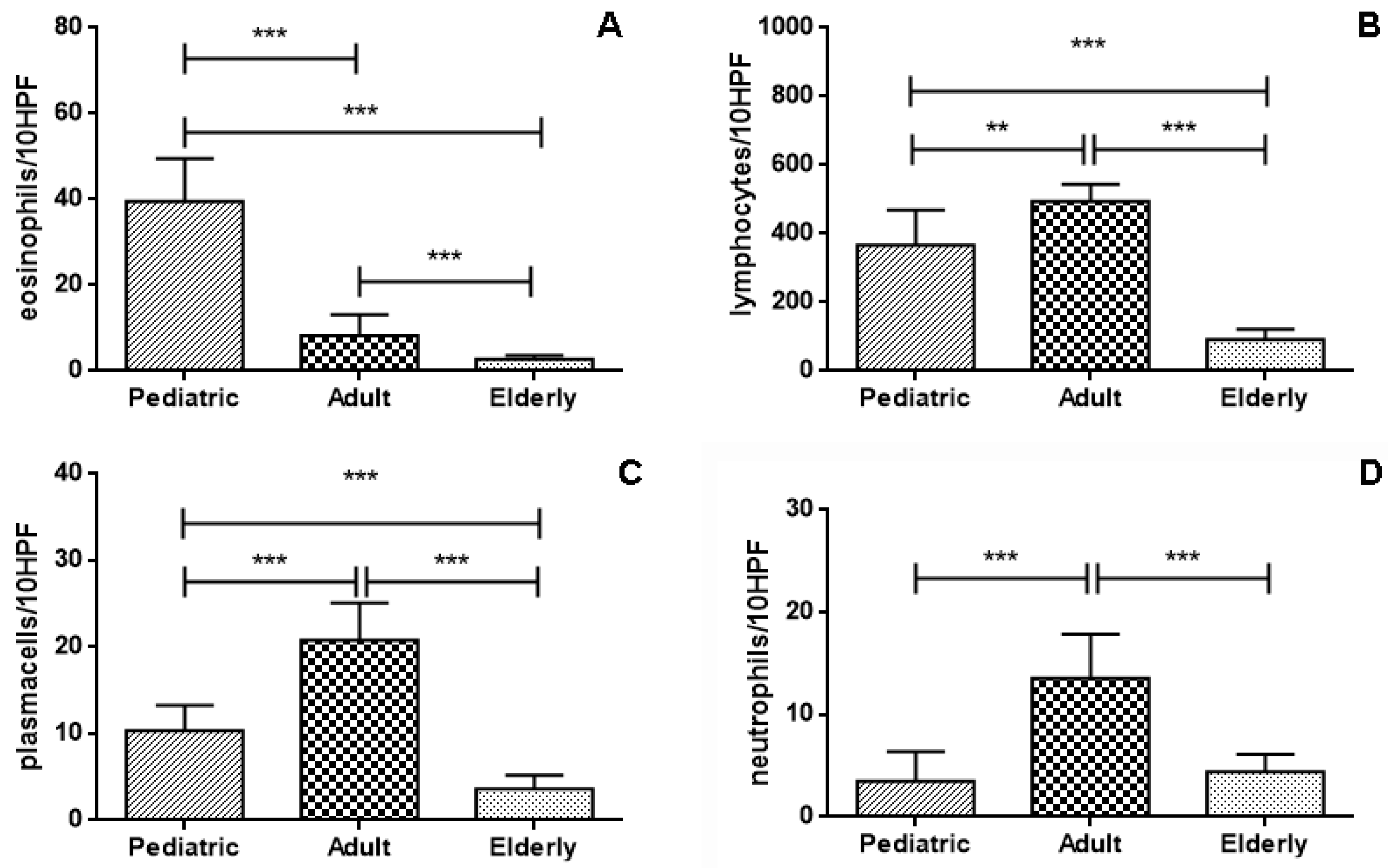
| Eosinophils/10HPF, mean (±SD) | 6.5 (8.3) | 39.5 (9.9) | 8.26 (4.9) | 2.67 (0.8) | ||
| Lymphocytes/10HPF, mean (±SD) | 262.5 (198.3) | 266.7 (39.8) | 493.9 (50.6) | 92.3 (30.0) | ||
| Neutrophils/10HPF, mean (±SD) | 8 (5.5) | 1.3 (1.0) | 13.5 (4.3) | 4.4 (1.7) | ||
| Plasma cells/10HPF, mean (±SD) | 10.9 (8.9) | 11.0 (3.7) | 20.8 (4.3) | 3.6 (1.6) | ||
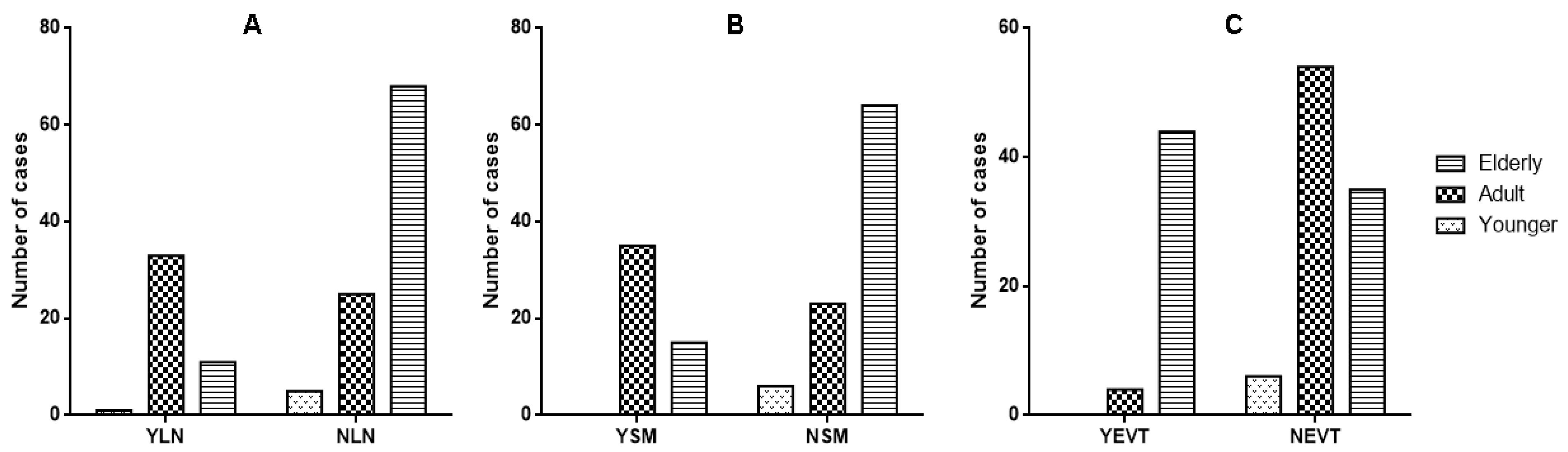
| Lymphoid nodules, n (Y/N) | 45/98 | 1/5 | 33/25 | 11/68 | ||
| Squamous metaplasia, n (Y/N) | 50/93 | 0/6 | 35/23 | 15/64 | ||
| Angioectasias, n (Y/N) | 48/95 | 0/6 | 4/54 | 44/35 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorentino, V.; Martini, M.; Galletti, C.; Pizzimenti, C.; Franchina, M.; Ieni, A.; Fadda, G.; Galletti, B.; Tuccari, G. The Morphology of Nasal Polyps in Different Age Groups: Histopathological Features. J. Pers. Med. 2024, 14, 414. https://doi.org/10.3390/jpm14040414
Fiorentino V, Martini M, Galletti C, Pizzimenti C, Franchina M, Ieni A, Fadda G, Galletti B, Tuccari G. The Morphology of Nasal Polyps in Different Age Groups: Histopathological Features. Journal of Personalized Medicine. 2024; 14(4):414. https://doi.org/10.3390/jpm14040414
Chicago/Turabian StyleFiorentino, Vincenzo, Maurizio Martini, Cosimo Galletti, Cristina Pizzimenti, Mariausilia Franchina, Antonio Ieni, Guido Fadda, Bruno Galletti, and Giovanni Tuccari. 2024. "The Morphology of Nasal Polyps in Different Age Groups: Histopathological Features" Journal of Personalized Medicine 14, no. 4: 414. https://doi.org/10.3390/jpm14040414
APA StyleFiorentino, V., Martini, M., Galletti, C., Pizzimenti, C., Franchina, M., Ieni, A., Fadda, G., Galletti, B., & Tuccari, G. (2024). The Morphology of Nasal Polyps in Different Age Groups: Histopathological Features. Journal of Personalized Medicine, 14(4), 414. https://doi.org/10.3390/jpm14040414