

Bilateral Scaphoid Fractures: A Systematic Literature Review

 , , and
, , and
Abstract
:1. Introduction
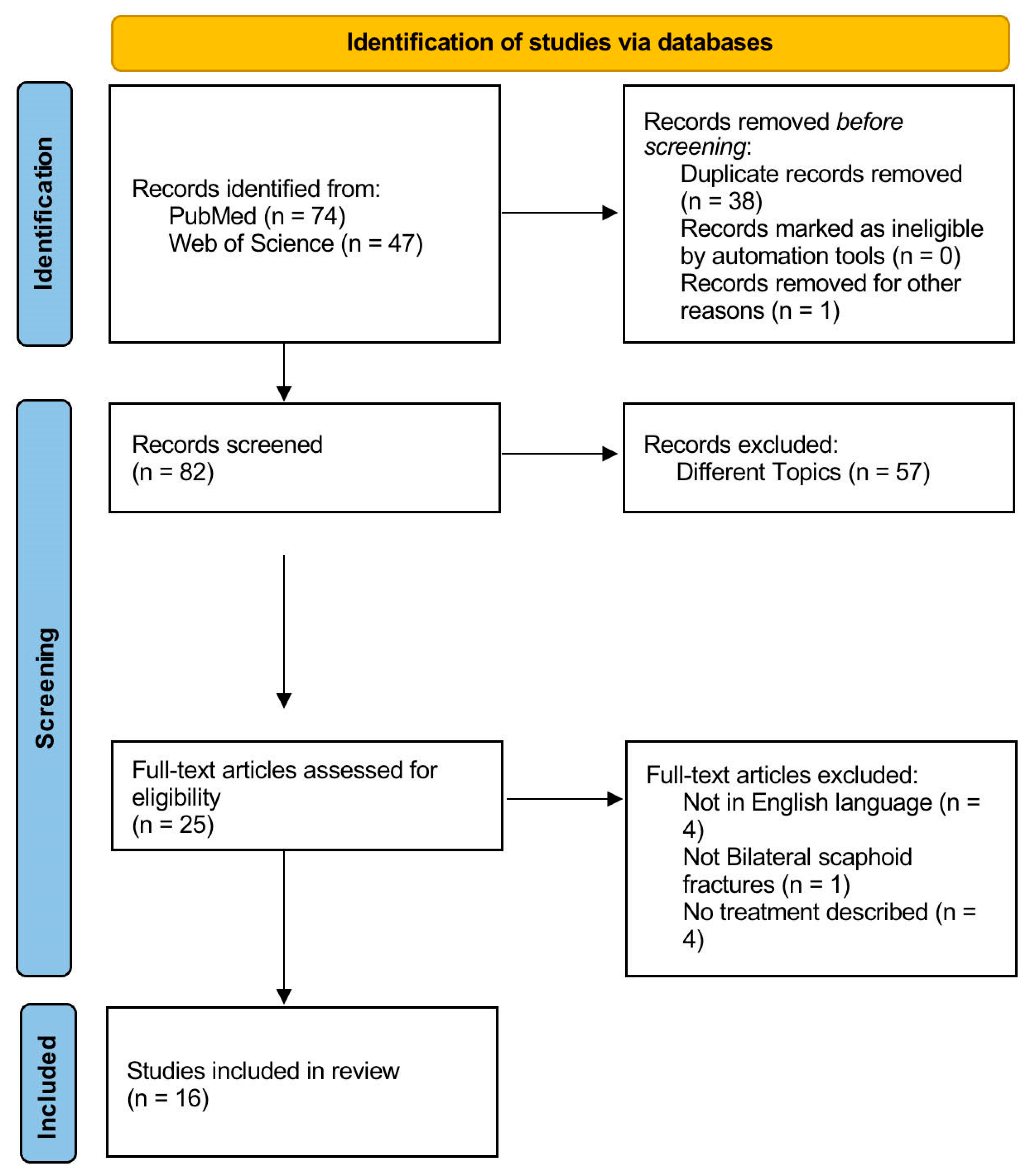
2. Materials and Methods
2.1. Study Selection
2.2. Selection Criteria
2.3. Data Extraction and Criteria Assessment
3. Results
3.1. Subjects
3.2. Mechanism of Injury
3.3. Associated Injuries
3.4. Fracture Site
3.5. Treatment
3.6. Follow-Up and Outcome
4. Discussion
- Yinusa W. et al. [19] described one case (6.25%) with a B2 fracture of the right wrist and a B3 fracture of the left wrist;
- Reigstad et al. [24] described one case (6.25%) with an A2 fracture of the right wrist and a B1 fracture of the left wrist;
- Mohamed Haflah N. H. [18] et al. and Ghargozloo D. [1] et al. each reported two cases (12.5%) of patients presenting with a B2 fracture on the left and a D2 fracture on the right. It was emphasized that the right-sided fracture was asymptomatic in the first case and went undetected for a period of 8 months in the second case.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ghargozloo, D.; Tomarchio, A.; Ballerini, M.; Chitoni, G. Traumatic Bilateral Scaphoid Fractures. Med. Glas. Off. Publ. Med. Assoc. Zenica-Doboj Cant. Bosnia Herzeg. 2021, 18, 222–225. [Google Scholar] [CrossRef]
- Krasin, E.; Goldwirth, M.; Gold, A.; Goodwin, D.R. Review of the Current Methods in the Diagnosis and Treatment of Scaphoid Fractures. Postgrad. Med. J. 2001, 77, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Van Tassel, D.C.; Owens, B.D.; Wolf, J.M. Incidence Estimates and Demographics of Scaphoid Fracture in the U.S. Population. J. Hand Surg. 2010, 35, 1242–1245. [Google Scholar] [CrossRef]
- Winston, M.J.; Weiland, A.J. Scaphoid fractures in the athlete. Curr. Rev. Musculoskelet. Med. 2017, 10, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Hayat, Z.; Varacallo, M. Scaphoid Wrist Fracture. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Sabbagh, M.D.; Morsy, M.; Moran, S.L. Diagnosis and Management of Acute Scaphoid Fractures. Hand Clin. 2019, 35, 259–269. [Google Scholar] [CrossRef]
- Lebowitz, C.; Massaglia, J.; Hoffman, C.; Lucenti, L.; Dheer, S.; Rivlin, M.; Beredjiklian, P.K. The Accuracy of 3D Printed Carpal Bones Generated from Cadaveric Specimens. Arch. Bone Jt. Surg. 2021, 9, 432–438. [Google Scholar] [CrossRef]
- Kattan, A.E.; Almarghoub, M.A.; Alnujaim, N.H.; Barasain, O.; AlLababidi, N.H. Bilateral Scaphoid Fractures: Case Report and Literature Review. Int. J. Surg. Case Rep. 2020, 66, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef]
- Stother, I.G. A Report of 3 Cases of Simultaneous Colles’ and Scaphoid Fractures. Injury 1976, 7, 185–188. [Google Scholar] [CrossRef]
- Kay, R.M.; Kuschner, S.H. Bilateral Proximal Radial and Scaphoid Fractures in a Child. J. Hand Surg. 1999, 24, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, K.; Miyazaki, H.; Yamaguchi, T.; Yanagihara, Y.; Kurosawa, H. Bilateral Transcapholunate Dislocation. Chir. Main 2000, 19, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Ozkan, K.; Ugutmen, E.; Unay, K.; Poyanli, O.; Guven, M.; Eren, A. Fractures of the Bilateral Distal Radius and Scaphoid: A Case Report. J. Med. Case Rep. 2008, 2, 93. [Google Scholar] [CrossRef] [PubMed]
- Yinusa, W.; Adetan, O.; Odatuwa-Omagbemi, D.O.; Eyo, M.U. Bilateral Simultaneous Fracture of the Carpal Scaphoid Successfully Treated with Conservative Cast Immobilisation: A Case Report. West Afr. J. Med. 2010, 29, 425–428. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, C.; Unuvar, F.; Keklikci, K.; Demirtas, M. Bilateral Dorsal Trans-Scaphoid Perilunate Fracture-Dislocation: A Case Report. Int. J. Surg. Case Rep. 2014, 5, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Saglam, F.; Gulabi, D.; Baysal, Ö.; Bekler, H.İ.; Tasdemir, Z.; Elmali, N. Chronic Wrist Pain in a Goalkeeper; Bilateral Scaphoid Stress Fracture: A Case Report. Int. J. Surg. Case Rep. 2015, 7C, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Mohamed Haflah, N.H.; Mat Nor, N.F.; Abdullah, S.; Sapuan, J. Bilateral Scaphoid Stress Fracture in a Platform Diver Presenting with Unilateral Symptoms. Singapore Med. J. 2014, 55, e159–e161. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.R.; Wajekar, S.; Mohan, H.; Dahapute, A.A. A Unique Case of Bilateral Trans-Scaphoid Perilunate Dislocation with Dislocation of Lunate into the Forearm. J. Clin. Orthop. Trauma 2016, 7, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Afshar, A.; Tabrizi, A. Bilateral Scaphocapitate Fracture Syndrome: A Case Report with Long-Term Follow up. J. Hand Surg. 2019, 24, 243–246. [Google Scholar] [CrossRef]
- Meraghni, N.; Lahlali, M.A.; Mohand-Oussaid, A.; Derradji, M.; Kara, Z. Bilateral Combined Fractures of the Scaphoid and Distal Radius: A Case Report. J. Orthop. Case Rep. 2022, 12, 1–4. [Google Scholar] [CrossRef]
- Johnson, N.A.; Kurien, T.; Horton, T.C. Recurrence of Scaphoid Stress Fracture: A Case Report. J. Wrist Surg. 2023, 12, 265. [Google Scholar] [CrossRef] [PubMed]
- Korkoman, A.J.; Fayi, K.A.; Al-Turki, N.; Ramadhan, H.; Alkhathami, A.M. Bilateral Greater Arc Perilunate Injury: A Case Report. Int. J. Surg. Case Rep. 2023, 113, 109070. [Google Scholar] [CrossRef] [PubMed]
- Reigstad, O.; Holm-Glad, T.; Korslund, J.; Thorkildsen, R.; Røkkum, M. Bilateral Carpal Pilon-Type Fractures Due to Clenched Fist Trauma: A Case Report. Ann. Jt. 2023, 8. [Google Scholar] [CrossRef] [PubMed]
- Pidemunt, G.; Torres-Claramunt, R.; Ginés, A.; de Zabala, S.; Cebamanos, J. Bilateral Stress Fracture of the Carpal Scaphoid: Report in a Child and Review of the Literature. Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2012, 22, 511–513. [Google Scholar] [CrossRef]
- Testa, G.; Lucenti, L.; D’Amato, S.; Sorrentino, M.; Cosentino, P.; Vescio, A.; Pavone, V. Comparison between Vascular and Non-Vascular Bone Grafting in Scaphoid Nonunion: A Systematic Review. J. Clin. Med. 2022, 11, 3402. [Google Scholar] [CrossRef] [PubMed]
- Lucenti, L.; Lutsky, K.F.; Jones, C.; Kazarian, E.; Fletcher, D.; Beredjiklian, P.K. Antegrade Versus Retrograde Technique for Fixation of Scaphoid Waist Fractures: A Comparison of Screw Placement. J. Wrist Surg. 2020, 9, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Cooney, W.P.; Dobyns, J.H.; Linscheid, R.L. Fractures of the Scaphoid: A Rational Approach to Management. Clin. Orthop. 1980, 149, 90–97. [Google Scholar] [CrossRef]
- Dias, J.J.; Singh, H.P. Displaced Fracture of the Waist of the Scaphoid. J. Bone Jt. Surg. Br. 2011, 93, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Almigdad, A.; Al-Zoubi, A.; Mustafa, A.; Al-Qasaimeh, M.; Azzam, E.; Mestarihi, S.; Khair, Y.; Almanasier, G. A Review of Scaphoid Fracture, Treatment Outcomes, and Consequences. Int. Orthop. 2024, 48, 529–536. [Google Scholar] [CrossRef]
- Jørgsholm, P.; Ossowski, D.; Thomsen, N.; Björkman, A. Epidemiology of Scaphoid Fractures and Non-Unions: A Systematic Review. Handchir. Mikrochir. Plast. Chir. 2020, 52, 374–381. [Google Scholar] [CrossRef]
- Wells, M.E.; Nicholson, T.C.; Macias, R.A.; Nesti, L.J.; Dunn, J.C. Incidence of Scaphoid Fractures and Associated Injuries at US Trauma Centers. J. Wrist Surg. 2021, 10, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Duckworth, A.D.; Jenkins, P.J.; Aitken, S.A.; Clement, N.D.; Court-Brown, C.M.; McQueen, M.M. Scaphoid Fracture Epidemiology. J. Trauma Acute Care Surg. 2012, 72, E41. [Google Scholar] [CrossRef] [PubMed]
- Suh, N.; Grewal, R. Controversies and Best Practices for Acute Scaphoid Fracture Management. J. Hand Surg. Eur. Vol. 2018, 43, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Garcia, R.M.; Leversedge, F.J.; Aldridge, J.M.; Richard, M.J.; Ruch, D.S. Scaphoid Nonunions Treated with 2 Headless Compression Screws and Bone Grafting. J. Hand Surg. 2014, 39, 1301–1307. [Google Scholar] [CrossRef]
- DiPrinzio, E.V.; Dieterich, J.D.; Walsh, A.L.; Warburton, A.J.; Chang, A.L.; Hausman, M.R.; Kim, J.M. Two Parallel Headless Compression Screws for Scaphoid Fractures: Radiographic Analysis and Preliminary Outcome. Hand 2023, 18, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Vigni, G.E.; Cassata, G.; Caldarella, G.; Cirincione, R.; Licciardi, M.; Miceli, G.C.; Puleio, R.; D’Itri, L.; Lo Coco, R.; Camarda, L.; et al. Improved Bone Regeneration Using Biodegradable Polybutylene Succinate Artificial Scaffold in a Rabbit Model. J. Funct. Biomater. 2022, 14, 22. [Google Scholar] [CrossRef] [PubMed]
- Cicero, L.; Licciardi, M.; Cirincione, R.; Puleio, R.; Giammona, G.; Giglia, G.; Sardo, P.; Edoardo Vigni, G.; Cioffi, A.; Sanfilippo, A.; et al. Polybutylene Succinate Artificial Scaffold for Peripheral Nerve Regeneration. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Cicero, L.; Puleio, R.; Cassata, G.; Cirincione, R.; Camarda, L.; Caracappa, D.; D’Itri, L.; Licciardi, M.; Vigni, G.E. Peripheral Nerve Regeneration at 1 Year: Biodegradable Polybutylene Succinate Artificial Scaffold vs. Conventional Epineurial Sutures. Polymers 2023, 15, 3398. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.R.L.; Halpern, A.L.; King, S.R.; Anderson, J.E. Scaphoid Fracture and Nonunion: New Directions. J. Hand Surg. Eur. Vol. 2023, 48, 4S–10S. [Google Scholar] [CrossRef]
- Liao, J.C.Y.; Chong, A.K.S. Pediatric Hand and Wrist Fractures. Clin. Plast. Surg. 2019, 46, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.L.; Bomar, J.D.; Wallace, C.D.; Edmonds, E.W. Factors influencing surgical decision-making in pediatric and adolescent scaphoid fractures. J. Pediatr. Orthop. B 2022, 31, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Lackey, J.T.; Seiler, P.L.; Lee, B.R.; Sinclair, M.K. Clinically Significant Treatment Delay in Pediatric Scaphoid Fractures. J. Hand Surg. Am. 2024, 49, 108–113. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Year | Lead Author | Article | No. of Patients | Sex | Age |
|---|---|---|---|---|---|
| 1976 | Stother I.G. [11] | A report of 3 cases of simultaneous Colles’ and scaphoid fractures | 1 | Male | 26 |
| 1999 | Kay R.M [12] | Bilateral proximal radial and scaphoid fractures in a child | 1 | Male | 13 |
| 2000 | Kaneko K. [13] | Bilateral transcapholunate dislocation | 1 | Male | 35 |
| 2008 | Ozkan K. [14] | Fractures of the bilateral distal radius and scaphoid: a case report | 1 | Male | 28 |
| 2010 | Yinusa W. [15] | Bilateral Simultaneous Fracture of the Carpal Scaphoid Successfully Treated with Conservative Cast Immobilisation: A Case Report | 1 | Male | 28 |
| 2012 | Pidemunt G. [12] | Bilateral Stress Fracture of the Carpal Scaphoid: Report in a Child and Review of the Literature | 1 | Male | 13 |
| 2014 | Yildirim C. [16] | Bilateral dorsal trans-scaphoid perilunate fracture-dislocation: A case report | 1 | Male | 21 |
| 2014 | Saglam F. [17] | Chronic wrist pain in a goalkeeper; bilateral scaphoid stress fracture: A case report | 1 | Male | 19 |
| 2014 | Mohamed Haflah N.H. [18] | Bilateral scaphoid stress fracture in a platform diver presenting with unilateral symptoms | 1 | Male | 16 |
| 2016 | Virani S.R. [19] | A unique case of bilateral trans-scaphoid perilunate dislocation with dislocation of lunate into the forearm | 1 | Male | 35 |
| 2019 | Afshar A. [20] | Bilateral Scaphocapitate Fracture Syndrome: A Case Report with Long-Term Follow up | 1 | Male | 25 |
| 2020 | Ghargozloo D. [1] | Traumatic bilateral scaphoid fractures | 1 | Male | 17 |
| 2022 | Meraghni N. [21] | Bilateral Combined Fractures of the Scaphoid and Distal Radius: A Case Report | 1 | Female | 16 |
| 2023 | Johnson N.A. [22] | Recurrence of Scaphoid Stress Fracture: A Case Report | 1 | Male | 20 |
| 2023 | Korkoman A.J [23]. | Bilateral greater arc Perilunate injury: A case report | 1 | Male | 25 |
| 2023 | Reigstad O. [24] | Bilateral carpal pilon-type fractures due to clenched fist trauma: a case report | 1 | Male | 17 |
| Lead Author | Associated Injuries | Mechanism of Fracture | Herbert’s Classification | CT Scan Performed |
|---|---|---|---|---|
| Stother I.G. [11] | Bilateral distal radius epiphysis fractures; D12 fracture | Traumatic: fall from a height | B2 | No |
| Kay R.M. [12] | Bilateral fractures of the proximal radius | Traumatic: fall from a height | A1 | No |
| Kaneko K. [13] | Bilateral carpal bone dislocations | Traumatic: fall from a height | B4 | No |
| Ozkan K. [14] | Bilateral distal radius epiphysis fractures; L1 fracture | Traumatic: fall from a height | B2 | No |
| Yinusa W. [15] | Bilateral subluxation of the scapho-capito-trapezoid joints | Traumatic: FOOSH * | Right: B2 Left: B3 | No |
| Pidemunt G. [12] | Not described | Stress | B2 | Yes |
| Yildirim C. [16] | Bilateral carpal bone dislocations | Traumatic: FOOSH | B4 | No |
| Saglam F. [17] | Not described | Stress: sports-related | B2 | No MRI performed |
| Mohamed Haflah N.H. [18] | Not described | Stress: sports-related | Right: D2 Left: B2 | No |
| Virani S.R. [19] | Bilateral carpal bone dislocations | Traumatic: FOOSH | B4 | Yes |
| Afshar A. [20] | Bilateral carpal bone dislocations; bilateral trans-capitate fractures | Traumatic: fall from a height | B4 | No |
| Ghargozloo D. [1] | Not described | Traumatic: sports-related | Right: D2 Left: B2 | Yes (after 8 months) |
| Meraghni N. [21] | Bilateral distal radius epiphysis fractures | Traumatic: sports-related | A2 | No |
| Johnson N.A. [22] | Not described | Stress: sports-related | B2 | Yes |
| Korkoman A.J. [23] | Bilateral distal radius epiphysis fractures; bilateral carpal bone dislocations | Traumatic: fall from a height | B4 | Yes |
| Reigstad O. [24] | Capitate and hamate fractures on the left wrist; capitate fracture on the right wrist | Traumatic: road traffic accident | Right: A2 Left: B1 | Yes |
| Lead Author | Treatment | Complications | Outcome | Follow-Up (in Months) |
|---|---|---|---|---|
| Stother I.G. [11] | Conservative | Not described | Union | 11 |
| Kay R.M. [12] | Conservative | Not described | No pain | 1 |
| Kaneko K. [13] | Bilateral headless compression screws | Not described | Union | 24 |
| Ozkan K. [14] | Bilateral headless compression screws | Not described | Union | 9 |
| Yinusa W. [15] | Conservative | Not described | Union | 3 |
| Pidemunt G. [12] | Two-stage (right first, left after 6 months) curettage, iliac crest bone grafting, and fixation with headless compression screws | Not described | No pain | 15 |
| Yildirim C. [16] | Bilateral headless compression screws | Non-union of the right scaphoid | Left: union Right: non-union without symptoms | 24 |
| Saglam F. [17] | Conservative | Not described | Union | 28 |
| Mohamed Haflah N.H. [18] | Bilateral headless compression screws | Not described | Union | 4 |
| Virani S.R. [19] | Bilateral headless compression screws | Not described | Union | 12 |
| Afshar A. [20] | Bilateral headless compression screws | Not described | Union | 60 |
| Ghargozloo D. [1] | Bilateral headless compression screws (right: with non-vascularized bone graft) | Not described | Union | 11 |
| Meraghni N. [21] | K-wires percutaneous fixation | Not described | Union | 12 |
| Johnson N.A. [22] | Conservative | Recurrent stress fracture of the right scaphoid after 9 months treated with headless compression screws | Union | 12 |
| Korkoman A.J. [23] | Bilateral headless compression screws | Not described | Union | 12 |
| Reigstad O. [24] | Bilateral headless compression screws | Not described | Union | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Itri, L.; Gattuso, M.S.; Cobisi, C.D.; Ferruzza, M.; Lucenti, L.; Camarda, L. Bilateral Scaphoid Fractures: A Systematic Literature Review. J. Pers. Med. 2024, 14, 424. https://doi.org/10.3390/jpm14040424
D’Itri L, Gattuso MS, Cobisi CD, Ferruzza M, Lucenti L, Camarda L. Bilateral Scaphoid Fractures: A Systematic Literature Review. Journal of Personalized Medicine. 2024; 14(4):424. https://doi.org/10.3390/jpm14040424
Chicago/Turabian StyleD’Itri, Lorenzo, Maria Serena Gattuso, Claudio Domenico Cobisi, Massimo Ferruzza, Ludovico Lucenti, and Lawrence Camarda. 2024. "Bilateral Scaphoid Fractures: A Systematic Literature Review" Journal of Personalized Medicine 14, no. 4: 424. https://doi.org/10.3390/jpm14040424
APA StyleD’Itri, L., Gattuso, M. S., Cobisi, C. D., Ferruzza, M., Lucenti, L., & Camarda, L. (2024). Bilateral Scaphoid Fractures: A Systematic Literature Review. Journal of Personalized Medicine, 14(4), 424. https://doi.org/10.3390/jpm14040424