1. Introduction
Child participation is the continuous process of expressing opinions and actively participating in decision-making in different areas of life affecting children. It is a dialogue between children and adults based on respecting children’s rights, opinions, and attitudes [
1]. Participation of children who are beneficiaries in the social welfare system, more specifically children placed in educational institutions, is important not only when it comes to respecting children’s rights, but also in terms of preventing those children and young people from becoming outsiders [
2] and enabling them to become active holders of their rights who can make their own choices and create outcomes in their own lives. Therefore, child participation is a key factor that can improve treatment outcomes, as it gives the children a sense of autonomy and control over their own life and the course of care [
3]. There are numerous advantages related to child participation and the participatory approach
1 in working with children in residential care
2, including educational institutions. Thus, children who are given the possibility to express their opinions and participate in decisions are more motivated to work on their own problems and develop responsibility and autonomy [
4,
5]. The benefits of the participatory approach in assessing and planning interventions are tangible not only for children, but also for professionals and the community through shared responsibilities and partnerships between professionals and children, the development of relationships between professionals and children, a better understanding of the children’s perspective, and the creation of preconditions for better treatment outcomes [
4].
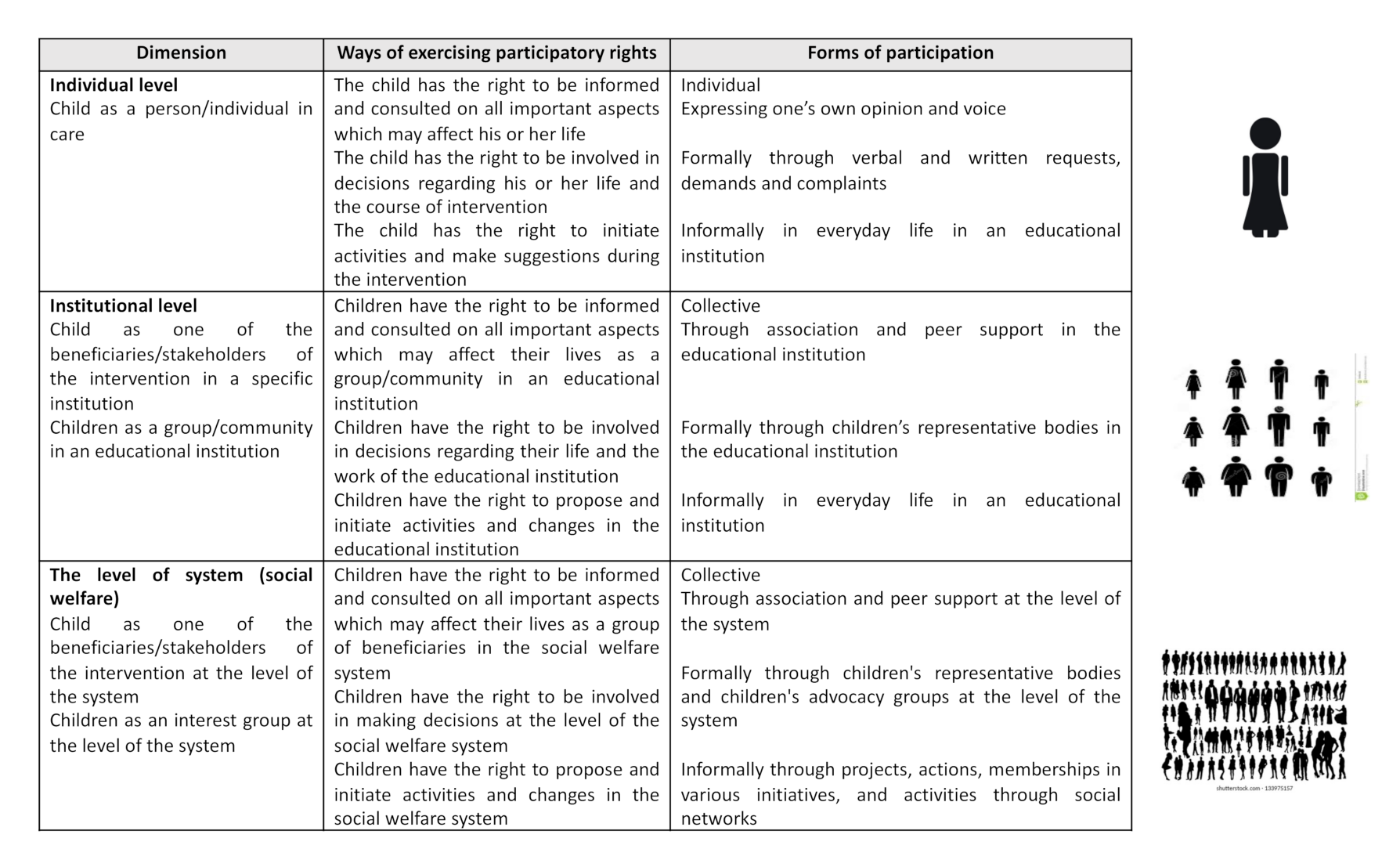
In the context of residential care, more specifically when it comes to care in an educational institution, children can participate at three levels: the individual, institutional, and systemic level. Furthermore, a distinction between individual and collective levels of participation can be made. Individual participation refers to the participation of an individual child in decisions regarding the course of care, while collective participation refers to the participation of children as an interest group expressing opinions and participating in decision-making regarding the social welfare system, policies, and practices [
6].
Figure 1 provides a more detailed overview of the possibilities offered to children when participating as beneficiaries of interventions regarding the level of participation, ways of exercising participatory rights, and forms of participation, from the authors’ perspective.
Children and young beneficiaries of educational institutions are a particularly vulnerable group which, due to personal, family, and environmental characteristics, are at a greater risk of not exercising the right to participate [
7,
8,
9]. It can be said that this is one of the groups of children whose voice is seldom heard (seldom heard young people), i.e., with fewer possibilities and opportunities to participate, who at the same time face more challenges in exercising this right [
10]. Family separation threatens their rights and freedoms. Therefore, special efforts should be made to ensure these children are given the opportunity to express their views and make decisions regarding their lives [
11]. Before entering care, this group of children has experienced multiple risks such as behavioural problems, inadequate parental care, poverty, and problems in the school environment and the community that consequently lead to family separation [
12]. Their vulnerability and risks of social exclusion are deepened by entering the social welfare system, as well as by the deprivations experienced while in care, such as restrictions on freedom, a lack of privacy, and a lack of choice [
12,
13]. At the same time, the children in care are faced with several important decisions regarding changing their behaviour, choice of education, and future plans after leaving the social welfare system [
14]. The interaction between the many risks they are faced with indirectly affects whether the right to participate is exercised or not, whereby positive treatment outcomes are also linked to the creation of a supportive and structured environment that provides young people with a sense of autonomy and the ability to make decisions that concern them [
15].
Challenges regarding child participation in residential care in general, and specifically in educational institutions, are also evident at the level of the individual characteristics of children, professionals, and parents, as well as in the structural features of the system. In that regard, Duncan [
16] states that participation is limited by the child’s actual maturity and capacity, as well as the child’s maturity and capacity as perceived by professionals and parents. The key concern of professionals is how to simultaneously respect the child’s right to protection and well-being, as well as the right to participate. Underlining the conflict between the right to protection and the child’s right to participation in care, Barry [
17] says that young people often come into the social welfare system from families where they have not been protected and have taken on the role of adults (e.g., caring for siblings) as a result of disrupted family dynamics. The social welfare system protects them from dysfunctional families, but it treats them as children with little influence on decision-making. This significantly reduces children’s responsibilities and autonomy, which negatively affects the opportunities regarding participation and reduces their motivation to participate [
17]. This group of children has also had numerous traumatic experiences, i.e., they have experienced neglect by adults they trusted, making it difficult for them to establish a trusting relationship with the adults in the social welfare system who play a key role in encouraging participation [
14]. It is also evident that professionals declaratively recognise the right of children to participate, but in fact support the paternalist ideology of the social welfare system based primarily on protection [
16]. Professionals also need specific competences in order to develop the participation skills of young people in the social welfare system [
14,
18,
19], first and foremost being relational competences [
20], i.e., developing a respectful and cooperative relationship with children. Opportunities for participation are also limited at the systemic level, as the social welfare system is predominantly based on adultism in assessing the child’s needs and making decisions about their future life and care [
16,
21].
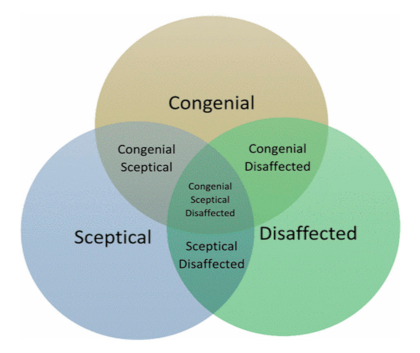
Based on studies involving children who have been in alternative care, Duncan [
16] points out that child participation in this system is generally characterised by constrained participation and defines the typology of child participation in alternative care (
Figure 2). When it comes to constrained participation, the typology presumes that children choose to participate in a congenial (congenial participation), sceptical, or disaffected manner. In doing so, congenial participation is characterised by cooperative relationships between children and adults and authorities, while sceptical participation is characterised by the child’s hesitation to participate due to doubts, insecurities, and fear of consequences when expressing opinions. On the other hand, disaffected participation is characterised by conflicts with authorities and withdrawal from the process due to dissatisfaction with the system and a lack of trust in professionals [
16]. It is also important to emphasise that these types of participation are not static and stable, but they change as the child spends time in the system, i.e., as the child matures and experiences life in the social welfare system. These types of participation also depend on the adults with whom the child interacts in the social welfare system. It is precisely because of this dynamic nature and the variety of constrained opportunities for participation that children can simultaneously experience several different types of participation [
16].
The meta-analysis of previous studies on the topic of child participation in residential care indicates that children have abundant experience in terms of non-participation in decisions regarding everyday life in care, care planning, participation in the management meetings related to living in the social welfare system, information about admission, course of treatment, and leaving care [
14,
22,
23]. The results of the research show that some children participate in the day-to-day decision-making, but that a large part of them are excluded from decisions concerning their life, education, and social relations [
14]. A satisfactory practice of participation is supported by a study dealing with the attitudes of children and young people in alternative care in Australia [
24]. A total of 2083 children participated in the study. The results showed that 67% of children are given the opportunity to express their views and be heard, 74% have said they are informed regarding the decisions concerning them, while only 17% feel they are not given an opportunity to be heard and to express their opinion (10%). Furthermore, Henriksen [
21] analysed the perspective of young people and professionals (case managers) on three key topics: trust and continuity in relationships, access to information and understanding care, and the impact on decision-making. The study showed that an important step in promoting young people’s participation in decision-making is creating a space for mutual trust and a continuous quality relationship between professionals and children. At the same time, a particular challenge for young people is the fluctuation of professionals with whom they interact, and numerous ineffective systemic interventions that have not helped them solve their difficulties. When it comes to access to information and understanding the process of care, the results clearly showed that most young people lack an understanding of how the system works, the reasons and purpose of their placement, and their life after leaving the social welfare system. Moreover, they perceive the system as extremely intrusive to their lives and relationships. Young people have also experienced that many adults (both parents and professionals) discuss and exchange information about their lives, with adults taking all the responsibility for decision-making. The influence of young people in decision-making is an example of “tokenism”, where children participate in discussions about their lives, but their opinion is neither heard nor can it affect the course of care [
21]. Furthermore, Sierward and Wolf [
25] conducted two studies on participation involving 1067 young people in residential care in Germany. The results showed that the participation of young people is relatively low and that a large number them do not feel fully involved in the life of the institution of their placement. The most frequent participation was observed in aspects of everyday life in the institution (e.g., food, pocket money, leisure time in the home, creation of group rules), while young people were given no opportunity to participate in the choice of their roommate, the course of care, and the selection of employees. Analyses of recent studies have also shown that adults are one of the key elements in the involvement of young people in decision-making, but also in developing their capacity to participate [
5,
14,
22,
23]. For example, young people agree that it is easier to share their thoughts with interested, involved, and available professionals with whom they have established a good and lasting relationship [
18]. Moreover, the impact on future life and care has been shown to be of relevance when it comes to the participation of young people. For example, the results of a qualitative study in Australia, carried out with 121 children in the social welfare system, showed that the children feel the safest in an institution when they have a degree of control over their space and the situations occurring in the institution [
26]. Furthermore, the children clearly expressed their desire for more influence in decision-making, not only in terms of what they have for dinner, but in terms of choosing their roommate, choosing available programs, maintaining relationships with friends and family, and choosing professionals and programs which can help them change their behaviour. Negative experiences with participation at the institution level, such as not getting feedback and having their opinions ignored, lead to children losing motivation and confidence in participation, which consequently further reduces their participation [
5]. A survey with children in the social welfare system in Ireland showed that children need to have more self-confidence and life skills in order to feel ready for participation. Children are aware of their own lack of social skills, as well as the fact that their aggressive behaviour sometimes hinders their access to participation [
18]. In this regard, they need informal and formal participation spaces, as well as professionals with the necessary skills to encourage meaningful participation.
Studies regarding the collective participation of children in residential care are less common. In a study dealing with the manner of participation of children in care, Ten Brummelaar et al. [
23] concluded that children rarely participate both in meetings dealing with the organisation and functioning of the institution, and in the beneficiary councils. In a study conducted in the USA by Brown et al. [
27], it was established that out of 126 institutions with a beneficiary council, only 35 of them had meaningfully involved young people in decision-making and allowed them to assist in ensuring the quality of care. A recent study by Gazit and Perry-Hazan [
28] showed that the collective participation of young people in care is faced with a number of challenges. Key challenges refer to contextual factors regarding young people’s lives, such as a lack of family support, lack of perseverance, lack of support from adults, and engaging in high-risk behaviours that consequently limit young people’s ability to participate. While the survey clearly revealed the challenges young people face, the results also showed three factors contributing to overcoming these obstacles. The collective participation process facilitates young people’s sense of belonging to a group, their ability to participate in forms which are tailor-made for them and flexible, accompanied by the continuous mediation of adult managers, and a sense of participation in bodies as an alternative to non-participation in bodies such as student councils in schools [
28].
1.1. Context of the Research
Since this paper focuses on the experience of participation of young people in educational institutions in the Republic of Croatia, it is important to briefly clarify the national context related to this topic. The key processes in the last decade in Croatia regarding services for children with behavioural problems and the improvement of those services are the processes of deinstitutionalization and transformation of the social welfare institutions. Until 2019, only two institutions for adolescents with behavioural problems had changed their legal status and title and transformed to centres for services in a community; however, this was without any significant changes related to the quality of care or newly developed services. The process of deinstitutionalization has been slow with many delays and obstacles in implementation (more in Borić and Ćosić [
29]). Therefore, services for children with behavioural problems in Croatia are still mainly based on a residential type of care (educational institutions) since there is a lack of structured interventions in the community and there is still no specialized therapeutic foster care. The research was conducted on the territory of the Republic of Croatia, in educational institutions in the field of child welfare. In the Republic of Croatia, children and young people aged between 7 and 21 who show behavioural problems that endanger their psychosocial functioning, their family, and their environment over a longer period of time are placed in educational institutions. There are currently ten educational institutions of this type in the whole of Croatia, providing care and specialized intervention for children and young people with behaviour problems. There are seven centre-based homes and three residential care homes. At any moment, there are around 350 children and young people in these institutions [
30].
Child participation in residential care in Croatia in general, and including educational institutions, is defined in various relevant national laws, policies, and guidelines. The National Strategy on the Rights of Children 2014–2020 [
31] states that “children who are beneficiaries of rights in the social welfare system require increased adult responsibility and special attention from public policies. In this system, children should be given access to information and services, and the opportunity to advocate for their rights and interests, so that they can choose between forms of support and participate in situations and decisions related to their future lives, as well as in the evaluation of treatment outcomes” (pp. 27–28). Child participation in the social welfare system, which includes children in educational institutions, is defined in the following national laws: the Social Welfare Act [
32], the Family Act [
33], and the Foster Care Act [
34]. Furthermore, the Ordinance on Social Services Quality Standards [
35] in Croatia prescribes the following standards regarding children as the beneficiaries of the social welfare system:
the standard of access to information (current and potential beneficiaries need to receive all the information on the social services they are entitled to so that they may choose the right services which best meet their needs); the standard of decision-making and self-determination (beneficiaries are encouraged to actively shape their own lives, and they are enabled in every way to make their own choices and decisions on all aspects of their lives); and the standard of privacy and confidentiality (the recognition of every beneficiary’s right to privacy, confidentiality, and dignity in all aspects of their lives). At the prescriptive and normative level, as Jeđud Borić, Mirosavljević, and Šalinović [
36] conclude, child participation is well regulated. However, it lacks clear mechanisms for monitoring and evaluating legislation and strategies. Moreover, it lacks sanction mechanisms in cases of non-compliance with the regulations, and measures and information about normative documents (laws, strategies, guidelines) related to children provided in a child-friendly format.
Koller-Trbović and Širanović [
37] point out that significant interest in the topic of participation of at-risk children has been evident in the Croatian research discourse only in the last fifteen years or so, while the research encompasses several contexts and topics (e.g., the participatory rights of children in educational institutions, of children who are in the process of a needs analysis and intervention planning, who are in foster care, or who are undergoing non-institutional treatment). Even though these are smaller and most often qualitative studies, the results almost unambiguously indicate that children’s participatory rights are insufficiently observed and very diversely perceived in practice. It is also interesting to analyse the survey results regarding the time continuum and the attitude of young people towards participation. For example, it is evident that young people in the first studies on participation in care [
38] consider that it is important to participate in decision-making but see themselves as not sufficiently capable or mature for this role. In subsequent studies, young people clearly point out the need to make changes in the relationship between the professionals and the beneficiaries, and the importance of active and responsible participation. They also consider themselves as capable of providing relevant information about themselves and their own lives [
39,
40,
41]. This also shows an increasing awareness of young people about their right to participate, but also the need to develop a participatory approach in residential care. As regards this group of children, it is also evident there is no indication of how statutory mechanisms work, such as beneficiary councils, which should ensure the collective participation of children in care [
9]. It may be concluded that the results of key Croatian studies on this topic unequivocally show the children’s readiness to participate, but also their continued insufficient involvement and partnership with adults, especially in terms of participating in decisions on their future lives. In direct treatment, children report better opportunities for participation than in the process of needs analysis and intervention planning, even if such opportunities are still insufficient [
37]. Therefore, this research was conducted with the aim of deepening the knowledge and understanding of participation of adolescents in various aspects of institutional life. The motivation for the research was the largely untapped (and unexplored) space in relation to the characteristics and possibilities of the collective participation of in-care adolescents as an interest group which makes decisions related to the practice and the policy of residential care for children and young people.
1.2. The Aim of the Research and Research Questions
The aim of this paper is to deepen the knowledge and understanding of the participation of adolescents in educational institutions. More specifically, the following research questions were defined: (1) How do adolescents who are beneficiaries of educational institutions describe their own participation in the institution? (2) How do adolescents’ representative bodies in educational institutions (beneficiary councils) operate?
2. Methods
This research was based on an exploratory qualitative approach, which is in accordance with the nature and the subject of the research and allows adolescents’ (educational institution beneficiaries) voices to be heard. According to Flick [
42], a qualitative approach allows us to examine locally, temporally, and situationally relevant perspectives.
Considering the fact that child participation in the social welfare system is well regulated, the research is focused on two aspects: (1) analysing the activities of beneficiary councils in educational institutions through the perspective of adults, i.e., professionals who manage these institutions and (2) the perspective of educational institution beneficiaries as told from their own experience. Two forms of participation are intertwined in the research: the formal collective form, described through the perspective of beneficiary councils, and the individual form, as told from the adolescents’ perspective.
2.1. Participants
Given the two above-mentioned aspects, the first aspect of the research includes educational institutions in Croatia (a total of 8 institutions
3), while the second aspect of the research includes children from the largest educational institution in Croatia, which is located in Zagreb, the capital city of Croatia. A total of 11 adolescents, beneficiaries of an educational institution aged from 13 to 17, participated in the research. There were two focus groups with 4 participants in one and 7 participants in other. The sample is intentional and follows the logic of sample defining in qualitative research as described by Patton [
43], i.e., information-rich respondents that can offer in-depth understanding of the researched phenomenon. The time spent in an educational institution was two years on average (from one to four years of experience in residential care in general).
2.2. Ethical Considerations
In the phase of preparation and implementation of the entire research, the principles of the Ethical Code for Research with Children in the Republic of Croatia [
44] were applied. For the purposes of conducting research with children, the educational institution has given its consent. Before the focus group was held, the participants were presented with the research and given an overview of the topic, the aims of the research, the method of data collection, and the results. Since consent is an integral part of the research process and is based on the principle of participant autonomy and the principle of protecting their best interests and causing no harm, the participants were asked to give verbal consent for participation and the permission to be recorded, with a prior explanation of the need and the importance of recording and the future use of obtained information. The participants were also informed that they were allowed to withdraw from the research at any point.
2.3. Methods of Data Collection and Analysis
The data were collected using two methods: online questionnaires for educational institutions aimed at describing beneficiary councils and focus groups with adolescents in terms of their experience of participation in educational institutions. Online questionnaires were sent to institution directors via e-mail and were subsequently analysed as text material. Online questionaries included the following open-ended questions: existence of a council of beneficiaries in the institution, structure and number of members of beneficiaries’ councils, scope of work, topics of council meetings, frequency of meetings, and actions as a result of councils meetings. Focus groups were held on the premises of educational institutions. Two researchers (authors of this paper), experienced in the field of research and in work with children in educational institutions, conducted the focus groups. A protocol for discussion in the focus groups was created in the preparatory phase of the research, including topics and specific questions for discussion. Key domains of the protocol were rights of children, rights of children in educational institutions, child participation in general, child participation in educational institutions, and beneficiaries’ councils. A distracting factor in one of the focus groups was the presence of educators in the adjacent room, with the door open. The researchers feel that the participants of this focus group were somewhat reluctant to respond, which was discussed with the participants. The participants reflected that they were used to the presence of the educators and that they could speak freely. An important advantage of the focus group method is the interaction of participants and the possibility of simultaneous reflection on one’s own experience as well as the collective experience (group experience).
The following steps were taken for the data analysis. The responses collected through online questionnaires were systematized according to the key areas of the questionnaire. Moreover, qualitative content analysis procedures were applied: editing materials, defining categories, encoding the framework, initial coding (interpreting data with a focus on parts corresponding to the defined categories), final coding (coding check after the categories have been applied to the entire material), and establishing patterns (meanings). Data from focus groups were analysed as follows: the conversations in focus groups were rewritten verbatim and edited, followed by the initial coding of the material. The initial codes were then grouped into the code list, revised, and redefined where necessary. After that, the codes were grouped into categories and themes according to their meaning, i.e., according to the recognized patterns in the data. Three researchers (authors of the paper) conducted the data analysis. Each researcher individually conducted initial coding and categorization, which was followed by a joint discussion and definition of the final codes, categories, and themes. Results were described according to the defined themes and categories.
The data collected through the online questionnaires and focus groups will be presented separately and considered in the conclusion in terms of their interrelation with the common themes, in order to gain insight into the formal and personal forms of adolescent participation in educational institutions.
4. Discussion
Based on the results of this research, it can be concluded that the experiences of child participation in educational institutions are determined by the context of care (i.e., educational institutions), by the predominant forms of participation, and by the personal experiences and characteristics of adolescents. These three dimensions are in relation to one another, and their interplay decides whether the children can exercise their rights or not. Each of these three dimensions has a metaphorical meaning/meaning in terms of value and a concrete/operational meaning. The data from this research directly point to the operational, everyday meaning and experiences of participation, but this aspect also leads to an indirect conclusion about the value aspect of participation.
In relation to the context of care, based on the discussions with the adolescents, it is concluded that they do not see any greater significance of beneficiary participation. Their previous experiences of participation are very modest, even at the level of information about the social welfare system, where it has been established that most adolescents are not adequately informed about the interventions, and some have even been deliberately misinformed. Adolescents also gave very short responses about participation in the educational institution and do not see participation as a specific right or an area in which they could be affirmed. In an operational everyday context, young people believe their rights are important, but consider them in relation to the rules which define their institutional life. Such a restrictive context of care, i.e., in an educational institution, with numerous rules, a lack of choice, and the inability to participate in decision-making, even at the level of decorating their living space, discourages adolescents from participating and leads to resignation. Young people want to have a choice, they want a life that resembles family life: decorating their room, the possibility of having a pet, and using mobile phones. Their requirements are realistic and age-appropriate, but they do not comply with the requirements of an (overly) institutionalised life, which operates in a rigid framework and discourages participation. This kind of context of care is probably a reflection of adultism and ideas about organising the environment and care in educational institutions. This means it is important for adults (professionals) to listen to children’s voices and create new, better, and more flexible conditions of care and treatment for them (38).
In further discussions about the forms of participation, one may distinguish between collective formal participation and individual participation. The formal collective participation of children refers to beneficiary councils. Based on this research, one may conclude that the compliance with normative standards is merely declarative and procedural, failing to offer a meaningful, guided, and influential form of participation in educational institutions. The data collected on the activities of the beneficiary councils through online questionnaires were generally of a formal nature, without personal impressions or comments from the institutions that participated in the research. Knowledge was obtained about the technical side of the beneficiary council’s activities, but no information was obtained about the quality of such activities or about the perception of beneficiary councils and their influence. Information on these aspects was not formally requested in the questionnaire, but institutions did not provide them in the questionnaire on their own initiative, which may suggest that subsequent studies should focus on a more personal approach and additional methods of data collection (e.g., interviews), but also that there may not be much information about the beneficiary council’s activities to be shared. Formal forms of participation in beneficiary councils, i.e., children’s representative bodies at the level of a specific educational institution, mainly operate in a similar way: all the institutions stated that they have established beneficiary councils, which is their obligation in accordance with the applicable regulations in the social welfare system. Most institutions stated that all the children participate in the beneficiary councils, while some institutions have established beneficiary councils based on the criteria of representation (representatives of educational groups are members of the beneficiary council). Beneficiary councils generally meet on a regular basis, even though there is a notable difference between institutions (some councils meet monthly, while some meet once every nine months). The topics addressed by beneficiary councils are also rather universal: diet, leisure time, material demands. Topics such as peer education, rewarding beneficiaries, and the participation of beneficiaries in the process of adopting documents relevant for institutional life are rarely on the agenda or in the focus of beneficiary councils. Beneficiary councils are led by adults, and the conclusions made at council meetings are passed on to directors. Similar results were reported by Sierward and Wolf [
25] in a study on child participation in residential care in Germany: children participate most in debates on topics related to everyday life in the institution and do not participate in topics related to the decision-making regarding the course of care. The mode of action and topics addressed by children’s representative bodies, as well as obtaining feedback from adults, have a strong impact on the children’s motivation to participate. Numerous studies in the field of school and student councils and children’s councils in cities and municipalities, which are equivalent to beneficiary councils, show that dealing exclusively with everyday issues, such as diet and decorating personal space, discourages children from participating. Moreover, they want to participate in more relevant topics such as the ability to influence policies and decisions [
45,
46,
47,
48,
49,
50,
51]. Therefore, Yamashita and Davies [
52] argue that ineffective student councils may have a negative impact on children and make them question the meaning of participation, giving them the impression that such participation is a waste of time. Students become frustrated and alienated from the idea of participation and can get the impression that adults do not truly want to hear their voice. By choosing exclusively mundane and repetitive topics, adults (and consequently children) stay in their comfort zone, enacting known roles and relationships, and fail to make new opportunities for mutual influence, learning, and action. When it comes to beneficiary council activities, the focus groups involving children have evidenced the need for deeper research and questioning of how beneficiary councils work and their purpose. The adolescents who participated in the research were not aware of the existence of beneficiary councils in their institution, which means such councils have no role or influence in their lives, nor do the children give them any importance, showing no motivation to engage in their activities. However, regardless of the currently inadequate activities of beneficiary councils, their potential must be used. Studies show that the process of collective participation also allows adolescents to feel a sense of belonging to a group, offers the possibility of tailor-made and flexible forms of participation, and the possibility of participation in children’s representative bodies as an alternative to non-participation in similar bodies in regular environments, e.g., student councils in schools [
28]. Participation in beneficiary councils can thus become a place where adolescents are empowered to participate in other environments where they are very often on the margins, precisely because they are viewed through the prism of “care beneficiaries”. Likewise, the activities of beneficiary councils may help adolescents develop better social skills and learn various pro-social behaviours, which is also an important treatment outcome. In relation to the individual level of participation, in addition to the relative lack of information provided to adolescents, which is the first step in the participatory process, the results show that adolescents insufficiently participate in everyday institutional life, even though they would like to. When expressing their desire to participate, young people mention very specific topics/decisions in which they would like to be involved and which are very important for their quality of life in the institution: the choice of beneficiaries who come into their group, persons with whom they wish to share their living space, the choice of activities in which they want to be involved, and the possibility of influencing the decisions at the level of the social welfare system (such as the amount they get as pocket money). So far, studies have also shown that children in residential care mostly have abundant experience regarding non-participation in everyday decisions, care planning, management meetings related to their life in care, information about admission, the course of treatment, and leaving the social welfare system [
14,
22,
23]. It is important to bear in mind that this group of adolescents exhibit (at least) two vulnerabilities in parallel, i.e., they are both children and beneficiaries of the social welfare system. In this context, enabling them to participate is even more important. Adolescents mention educators as the key factor in encouraging participation, as their actions enable or disable participation. In particular, the characteristics of educators, such as interest, availability, and concern, are necessary components of quality supportive relationships [
18]. In addition, the continuity of the relationship between adolescents and educators is an important element, as many adolescents have no experience of stability and continuity due to numerous interventions in which they were involved, as well as the fluctuations of caretakers. Previous studies also confirm the conclusion that adults (professionals) are one of the key elements for the inclusion of children in decision-making, but also for the development of young people’s participation capacities [
5,
14,
18,
21,
22,
23,
53].
When it comes to the personal characteristics and the experiences of adolescents in relation to exercising their rights in an institution, their (both individual and collective) participation will depend on their personality and skills, but also on their previous participation experiences in the family, school, and the social welfare system. Apart from the experience of participation, experiences with important adults and with the intervention system are also of relevance. If the adolescents did not have positive experiences with adults in their earlier life and in the course of care, they will be less inclined to participate. The results of this research show that some young people do not trust adults (professionals and parents) due to being inadequately informed (and misinformed) about the duration of placement, the form of placement, etc. Also, some participants feel a “care fatigue” and their only desire is to “get out” as soon as possible, showing no desire to participate (. Numerous traumatic experiences of children in educational institutions, as well as the neglect from adults whom they had trusted, are cited as challenges in the exercise of participatory rights [
14]. In that regard, Vosz et al. [
5] point out that negative experiences with participation are reflected in the fact that children’s opinions are often disregarded, and they do not receive feedback on their participation, which also reduces their desire for future participation. In relation to the individual experiences of adolescents and their characteristics in the context of life in care, children describe institutional life as the relationship between their behaviour and the possibility of exercising their rights (including the right to participate): if they behave appropriately (and according to the rules), they receive benefits (rights). Regarding the issue of participation, one should ask whether we “hear” the adolescents’ voices in educational institutions as a sign of participation, or as disobedience and rebellion. In fact, very often (which has been shown in focus groups) adolescents in educational institutions communicate violently, impatiently, and loudly, which reflects their authenticity, but it can also be challenging when it comes to offering guidance and direction.
Summarising the above, one may conclude that the restrictive context of care, declaratory collective participation, and limited individual participation, along with distrust in adults and “care fatigue”, discourage adolescents from participating in educational institutions. These operational aspects also shed light on value aspects, i.e., recognising the importance of adolescent participation in ensuring the quality of care, encouraging participatory culture at the institutional level, and promoting participation as a value, as well as promoting the awareness and faith of adolescents in their ability to influence their lives and their living environment. Keeping in mind the characteristics of beneficiaries’ participation in educational institutions, it seems that participation and its potential to improve the quality of care have not (yet) been recognised as a real value in the social welfare system (more specifically educational institutions), neither generally nor specifically at the level of institutions. In terms of value, and based on specific descriptions of behaviour, experiences, and perceptions, it seems that adolescents have little faith in being able to influence their living environment and change their lives. In relation to the typology of child participation in the context of alternative care as presented by Duncan [
16], one may conclude that adolescents in this research show scepticism and dissatisfaction regarding participation, as well as suspicion, uncertainty, disappointment, and a lack of trust. However, they also show a desire for participation.
Considering the findings of this research, a number of opportunities are presented in terms of achieving the more meaningful participation of adolescents in educational institutions. First, an emphasis should be placed on a holistic approach when considering the children and their contributions in the context of educational institution. Adolescents’ participation should be integrated into the culture and the structure of the social welfare system, but also into each institution. In this regard, participation should be fostered as a benefit and the backbone of the relationship between children and adults in educational institutions. At the institutional level, one must invest in the development of organisational structures that enable participation (participation infrastructure), such as participation strategies, action plans, and guidelines for working with adolescents. Furthermore, providing resources for participation in terms of people, space, and time is also of relevance. Mannion [
54] cites the respective and spatial dimension of participation, whereby the respective dimension implies changes in the perception of power and coexistence (communion) in the relationship between children and adults, while the spatial dimension refers to safe environments, information, time, and support from adults so that children can articulate their views. Furthermore, it has been shown that adults are crucial in encouraging adolescents’ participation. In this sense, it is important to educate professionals about the concept, forms, and levels of participation, as well as about developing relational competences when dealing with adolescents. Adult’s dedication, interest, and availability, along with their belief that participation makes sense, will increase adolescents’ motivation to participate. Finally, the results have shown that this topic needs to be further deepened and explored. In this context, it also seems crucial to foster a participatory approach of including in-care children and young people in all stages of the research process.





{kind=link}
{kind=link}