
Migrants’ Health Policies and Access to Health Care in Portugal within the European Framework


Abstract
:1. Introduction
2. Materials and Methods
2.1. Document Analysis
2.2. Secondary Statistical Data
2.3. Survey
3. Results
3.1. Health Policy
3.2. Health Status
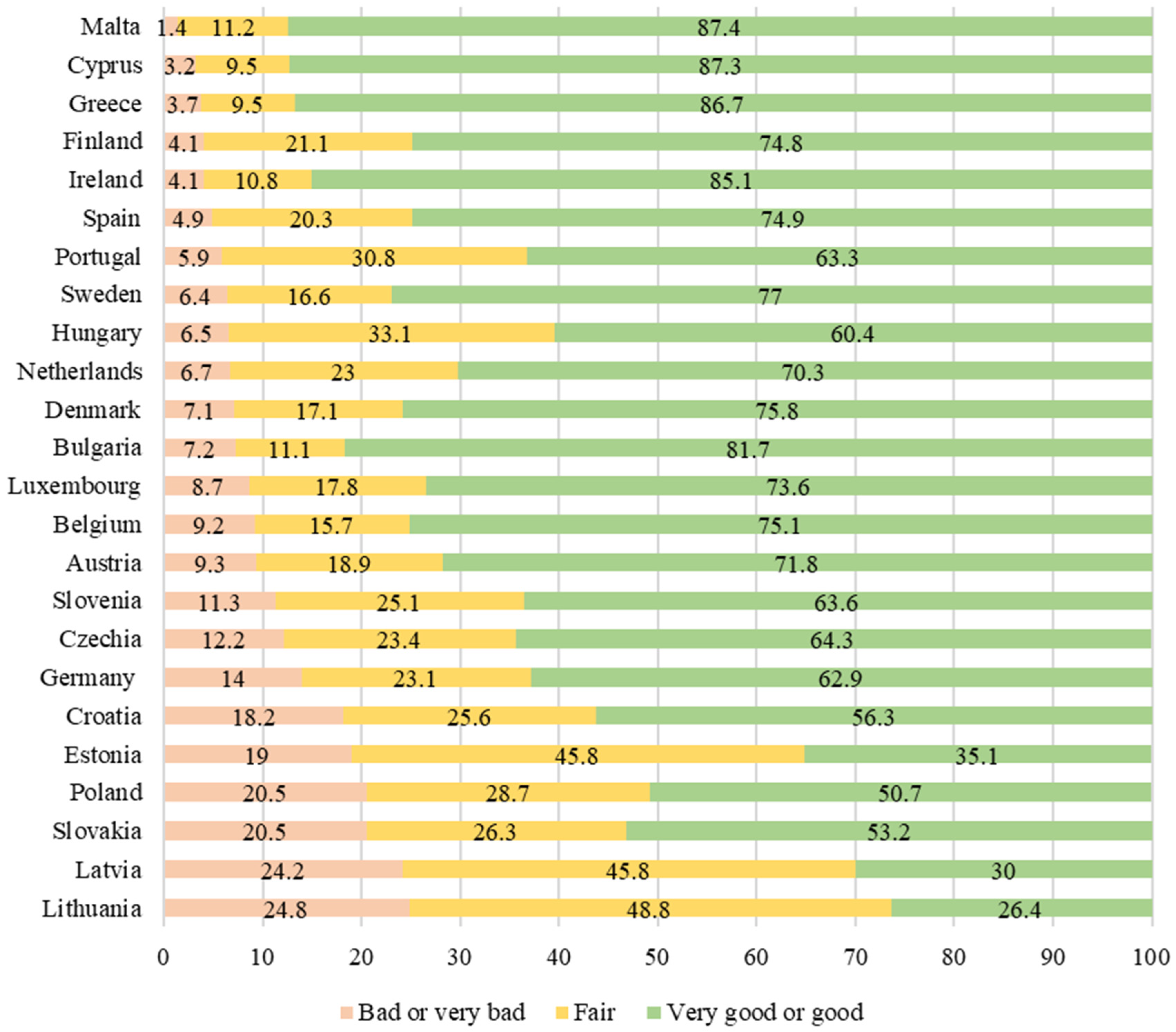
3.2.1. Self-Perceived Health
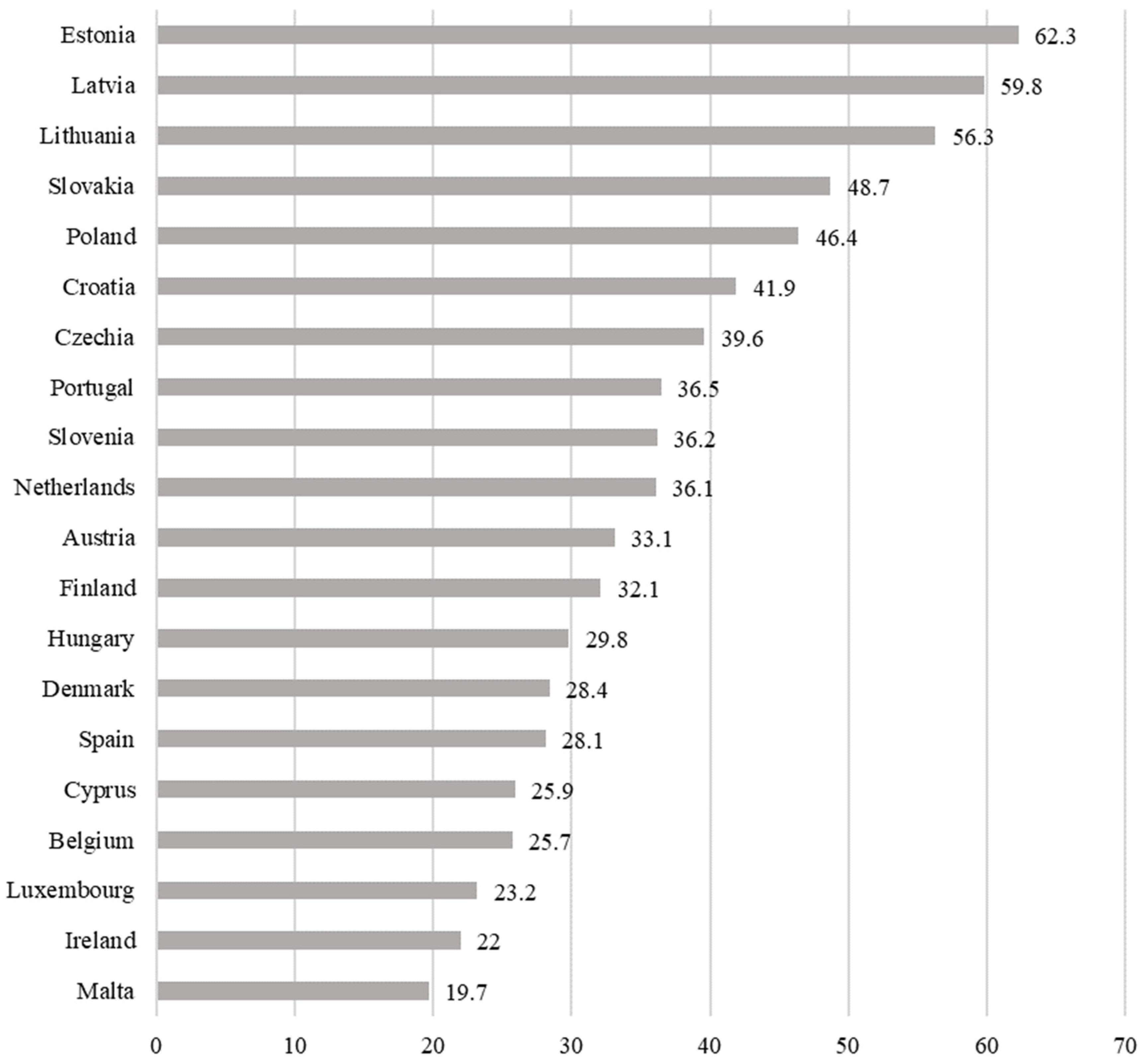
3.2.2. Chronic Morbidity
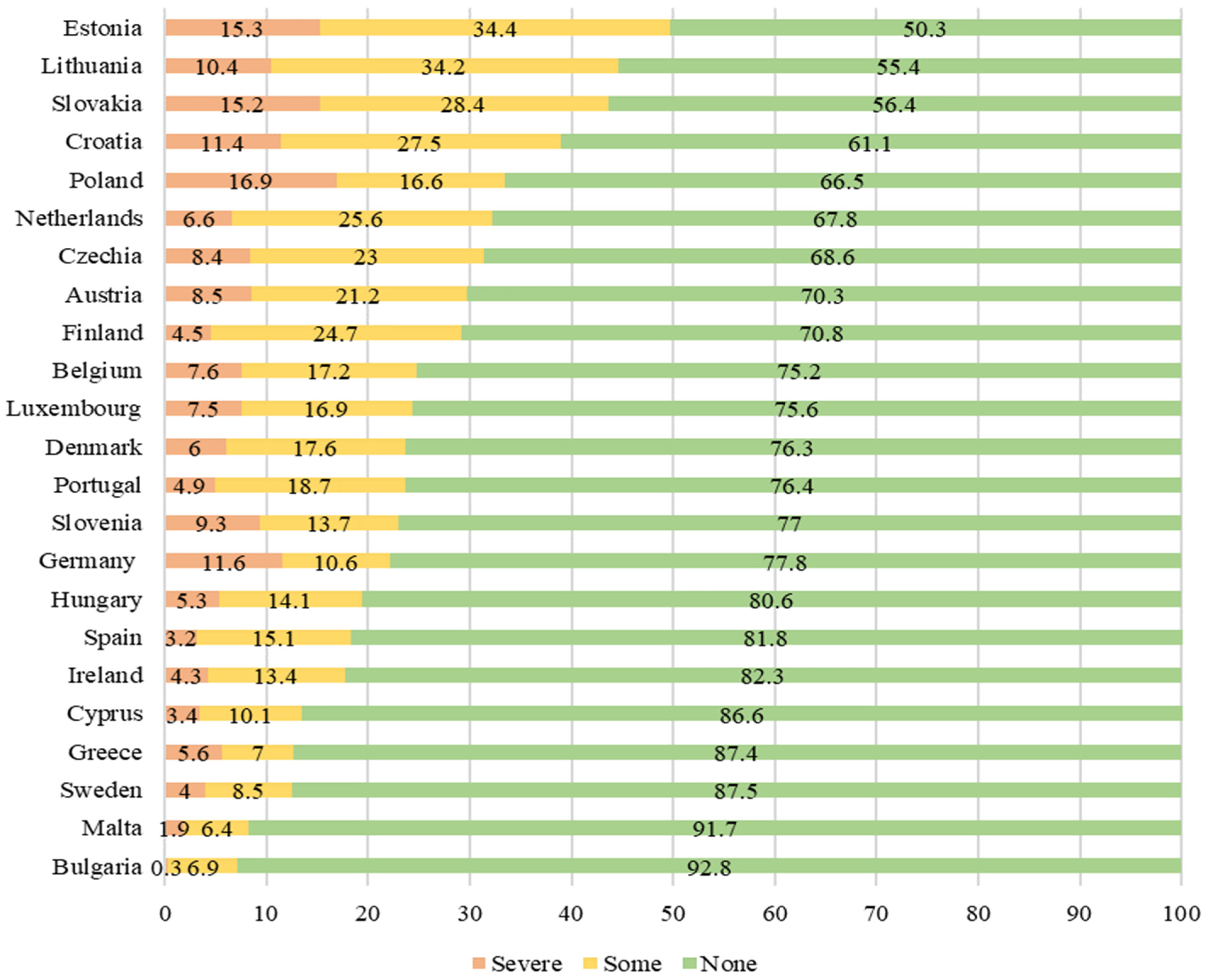
3.2.3. Activity Limitation
3.3. Health Care Services
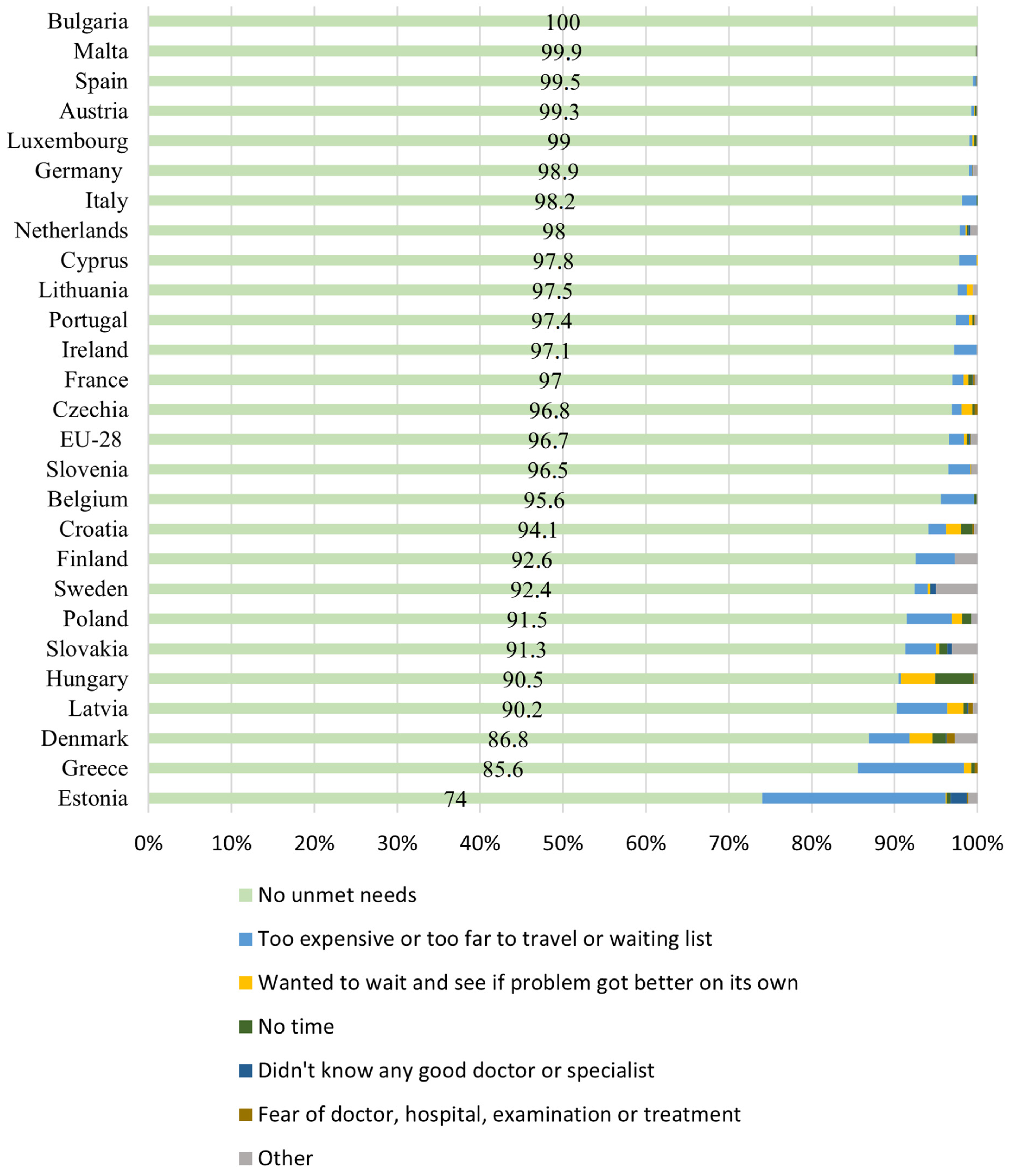
3.3.1. Self-Reported Unmet Needs for Medical Examination
3.3.2. Migrant Health Care Access in European Union
3.4. Health Care during COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Commission. Comunicação da Comissão ao Parlamento Europeu, ao Conselho, ao Comité Económico e Social e ao Comité das Regiões sobre um novo Pacto em Matéria de Migração e Asilo. Bruxelas, 23.9.2020. COM(2020) 609 Final. 2020. Available online: https://eur-lex.europa.eu/resource.html?uri=cellar:85ff8b4f-ff13-11ea-b44f-01aa75ed71a1.0013.02/DOC_1&format=PDF (accessed on 18 February 2022).
- Ahmadinia, H.; Eriksson-Backa, K.; Nikou, S. Health-seeking behaviours of immigrants, asylum seekers and refugees in Europe: A systematic review of peer-reviewed articles. J. Doc. 2021, 78, 18–41. [Google Scholar] [CrossRef]
- Oliveira, C.R.; Peixoto, J.; Góis, P. A nova crise dos refugiados na Europa: O modelo de repulsão-atração revisitado e os desafios para as políticas migratórias. Rev. Bras. Estud. Popul. 2017, 34, 73–98. [Google Scholar] [CrossRef] [Green Version]
- Padilla, B.; Ortiz, A. Fluxos Migratórios em Portugal: Do BOOM migratório à desaceleração no contexto de crise—balanços e desafios. Rev. Interdiscip. Mobilidade Hum. 2012, 39, 159–184. [Google Scholar] [CrossRef]
- Sousa, C.U. A Europa no contexto global das migrações. In Janus—Anuário de Relações Exteriores 2018–2019; Observatório de Relações Exteriores da Universidade Autónoma de Lisboa: Lisboa, Portugal, 2019; pp. 10–11. [Google Scholar]
- OECD. Working Together for Local Integration of Migrants and Refugees, OECD Regional Development Studies; OECD Publishing: Paris, France, 2018. [Google Scholar] [CrossRef]
- Legido-Quigley, H.; Karanikolos, M.; Hernandez-Plaza, S.; de Freitas, C.; Bernardo, L.; Padilla, B.; Sá Machado, R.; Diaz-Ordaz, K.; Stuckler, D.; McKee, M. Effects of the financial crisis and Troika austerity measures on health and health care access in Portugal. Health Policy 2016, 120, 833–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padilla, B. Saúde e migrações: Metodologias participativas como ferramentas de promoção da cidadania. Interface-Comun. Saúde Educ. 2017, 21, 273–284. [Google Scholar] [CrossRef] [Green Version]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; UN: New York, NY, USA, 2015; Available online: https://sdgs.un.org/publications/transforming-our-world-2030-agenda-sustainable-development-17981 (accessed on 18 February 2022).
- European Commission. European Pillar of Social Rights Action Plan; Publications Office of the European Union: Luxembourg, 2021. [Google Scholar]
- European Union. Charter of Fundamental Rights of the European Union, 26 October 2012, 2012/C 326/02. Available online: https://www.refworld.org/docid/3ae6b3b70.html (accessed on 18 February 2022).
- Peixoto, J. Dinâmicas e regimes migratórios: O caso das migrações internacionais em Portugal. Análise Soc. 2007, 42, 445–469. [Google Scholar]
- Casquilho-Martins, I.; Belchior-Rocha, H.; Ferreira, J.M.L. Community Strategies for Intercultural Participation. Trab. Soc. Glob. 2020, 10, 157–179. [Google Scholar] [CrossRef]
- Góis, P.; Marques, J. Retrato de um Portugal migrante: A evolução da emigração, da imigração e do seu estudo nos últimos 40 anos. E-Cadernos CES 2018, 29, 125–152. [Google Scholar] [CrossRef] [Green Version]
- Casquilho-Martins, I.; Matela, T. Inequalities in access to education: A socio-educational intervention with migrant children and youth. In ICERI2021 Proceedings; IATED Academy: Valencia, Spain, 2021; pp. 6888–6895. [Google Scholar] [CrossRef]
- Martins, I.C.D. Políticas de Imigração e Integração: Intervenção do Serviço Social. Interv. Soc. 2015, 46, 57–75. [Google Scholar]
- Peixoto, J.; Iorio, J. Crise, Imigração e Mercado de Trabalho em Portugal: Retorno, regulação ou resistência? Princípia: Cascais, Portugal, 2011. [Google Scholar]
- Matias, A.R.; Pinto, P.F. Overcoming linguistic barriers in Portuguese higher education: The case of international African students. Port. J. Soc. Sci. 2020, 19, 189–214. [Google Scholar] [CrossRef]
- SEF/GEPF. Relatório de Imigração, Fronteiras e Asilo 2020; Serviço de Estrangeiros e Fronteiras: Oeiras, Portugal, 2021. [Google Scholar]
- Estrela, P. A saúde dos imigrantes em Portugal. Rev. Port. De Clínica Geral 2009, 25, 45–55. [Google Scholar] [CrossRef]
- Padilla, B. Saúde dos Imigrantes: Multidimensionalidade, desigualdades e acessibilidades em Portugal. Rev. Interdiscip. Mobilidade Hum. 2013, 21, 49–68. [Google Scholar] [CrossRef]
- Padilla, B.; Rodrigues, V.; Lopes, J.; Ortiz, A. Saúde dos imigrantes: Desigualdades e crise no SNS. In Desigualdades Sociais: Portugal e a Europa; Carmo, R., Sebastião, J., Azevedo, J., Martins, S.C., Costa, A.F., Eds.; Mundos Sociais: Lisboa, Portugal, 2018; pp. 315–334. [Google Scholar]
- Jordão, N.; Freitas, C.; Ramírez, M. Efeitos da crise económica e das políticas de austeridade na saúde e no acesso aos cuidados de saúde da população migrante em países do sul da Europa: Revisão scoping. Rev. Interdiscip. Mobilidade Hum. 2018, 26, 213–230. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Gama, A.; Silva, A.; Cargaleiro, H.; Martins, M. Barreiras no acesso e utilização dos serviços de saúde pelos imigrantes: A perspetiva dos profissionais de saúde. Acta Med. Port. 2011, 24, 511–516. [Google Scholar] [PubMed]
- Heyman, J.; Congress, E. Health and Social Work: Practice, Policy and Research; Springer Publishing Company: New York, NY, USA, 2018. [Google Scholar]
- Gehlert, S.; Brownie, T. Handbook of Health Social Work; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2019. [Google Scholar]
- World Health Organization. Health Inequity and the Effects of COVID-19: Assessing, Responding to and Mitigating the Socioeconomic Impact on Health to Build a Better Future; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Tariq, S.; Woodman, J. Using mixed methods in health research. JRSM Short Rep. 2013, 4, 2042533313479197. [Google Scholar] [CrossRef] [PubMed]
- Bowen, G.A. Document Analysis as a Qualitative Research Method. Qual. Res. J. 2009, 9, 27–40. [Google Scholar] [CrossRef] [Green Version]
- Papanicolas, I.; Mossialos, E.; Gundersen, A.; Woskie, L.; Jha, A.K. Performance of UK National Health Service compared with other high income countries: Observational study. BMJ 2019, 367, l6326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalglish, S.; Khalid, H.; McMahon, S. Document analysis in health policy research: The READ approach. Health Policy Plan. 2020, 35, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- OECD/European Observatory on Health Systems and Policies. Austria: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Belgium: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Bulgaria: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Cyprus: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Czechia: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Estonia: Country Health Profile 2019—State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Finland: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. France: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Germany: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Greece: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Italy: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Luxembourg: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Malta: Country Health Profile 2019, State of Health in the EU. European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Portugal: Country Health Profile 2019, State of Health in the EU European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Romania: Country Health Profile 2019, State of Health in the EU European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Slovakia: Country Health Profile 2019, State of Health in the EU European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Slovenia: Country Health Profile 2019, State of Health in the EU European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Spain: Country Health Profile 2019, State of Health in the EU, European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. Sweden: Country Health Profile 2019, State of Health in the EU, European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- OECD/European Observatory on Health Systems and Policies. United Kingdom: Country Health Profile 2019, State of Health in the EU, European Observatory on Health Systems and Policies; OECD Publishing: Brussels, Belgium, 2019. [Google Scholar]
- Solano, G.; Huddleston, T. Migrant Integration Policy Index 2020; CIDOB: Barcelona, Spain; MPG: Brussels, Belgium, 2020. [Google Scholar]
- European Centre for Disease Prevention and Control. Reducing COVID-19 Transmission and Strengthening Vaccine Uptake among Migrant Populations in the EU/EEA—3 June 2021; ECDC: Stockholm, Sweden, 2021. [Google Scholar]
- Migrant Integration Policy Index (MIPEX). Available online: https://www.mipex.eu/play/ (accessed on 5 December 2021).
- Eurostat. Glossary: Minimum European Health Module (MEHM). Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:Minimum_European_Health_Module_(MEHM) (accessed on 5 December 2021).
- Vilelas, J. Investigação: O Processo de Construção do Conhecimento, 3rd ed.; Edições Sílabo: Lisboa, Portugal, 2020. [Google Scholar]
- Eurostat. Health variables of EU-SILC Reference Metadata in Euro SDMX Metadata Structure (ESMS). Available online: https://ec.europa.eu/eurostat/cache/metadata/en/hlth_silc_01_esms.htm (accessed on 3 December 2021).
- International Organization for Migration. Summary Report on the MIPEX Health Strand and Country Reports; International Organization for Migration: Geneva, Switzerland, 2016. [Google Scholar]
- Food and Agriculture Organization of the United Nations. Migrant Workers and the COVID-19 Pandemic. 2020. Available online: http://www.fao.org/3/ca8559en/CA8559EN.pdf (accessed on 12 December 2021).
- Peixoto, J. O que nos ensina a pandemia sobre migrações internacionais? O caso português e o contexto mundial. In Migrações Internacionais e a Pandemia de COVID-19; Baeninger, R., Vedovato, L.R., Nandy, S., Eds.; NEPO/UNICAMP: Campinas, SP, Brasil, 2020; pp. 132–137. [Google Scholar]
- European Commission. Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of Region Action plan on Integration and Inclusion 2021–2027. Brussels, 24.11.2020. COM(2020) 758 Final. Available online: https://ec.europa.eu/migrant-integration/news/ec-reveals-its-new-eu-action-plan-integration-and-inclusion-2021-2027_en (accessed on 18 February 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicators—Variables | Time | Geopolitical Territory | Source |
|---|---|---|---|
| Health status—Self-perceived health (%) | 2019–2020 | European Union—28 countries | Eurostat |
| Health status—People having a long-standing illness or health problem (%) | 2019–2020 | European Union—28 countries | Eurostat |
| Health status—Self-perceived long-standing limitations in usual activities due to health problem (%) | 2019–2020 | European Union—28 countries | Eurostat |
| Health care—Self-reported unmet needs for medical examination by main reasons declared (%) | 2019–2020 | European Union—28 countries | Eurostat |
| Migrant Integration Policy—Overall score (index) | 2019 | European Union—28 countries | Mipex |
| Migrant Integration Policy—Overall score with health (index) | 2019 | European Union—28 countries | Mipex |
| Migrant Integration Policy—Health (index) | 2019 | European Union—28 countries | Mipex |
| Integration Policy Indicators | |||
|---|---|---|---|
| Geopolitical Territory | Overall Score (with Health) | Overall Score | Health |
| Sweden | 86 | 87 | 83 |
| Finland | 85 | 87 | 67 |
| Portugal | 81 | 84 | 65 |
| Belgium | 69 | 69 | 73 |
| Ireland | 64 | 61 | 85 |
| Luxembourg | 64 | 66 | 46 |
| Spain | 60 | 57 | 81 |
| Germany | 58 | 58 | 63 |
| Italy | 58 | 55 | 79 |
| Netherlands | 57 | 56 | 65 |
| France | 56 | 55 | 65 |
| United Kingdom | 56 | 54 | 75 |
| Czechia | 50 | 48 | 61 |
| Estonia | 50 | 53 | 29 |
| Denmark | 49 | 48 | 56 |
| Romania | 49 | 50 | 46 |
| EU28 | 49 | 50 | 53 |
| Malta | 48 | 47 | 56 |
| Slovenia | 48 | 50 | 33 |
| Austria | 46 | 41 | 81 |
| Greece | 46 | 46 | 48 |
| Hungary | 43 | 45 | 29 |
| Cyprus | 41 | 41 | 36 |
| Bulgaria | 40 | 41 | 29 |
| Poland | 40 | 42 | 27 |
| Croatia | 39 | 41 | 27 |
| Slovakia | 39 | 37 | 50 |
| Latvia | 37 | 38 | 31 |
| Lithuania | 37 | 38 | 31 |
| 2019 | 2020 | ||||
|---|---|---|---|---|---|
| EU28 | EA19 | PT | PT | ||
| Too expensive | Foreign population (total) | 1 | 1 | 1.3 | 1.1 |
| Foreign population (Non-EU28 countries) | 1.1 | 1.2 | 1 | 1.2 | |
| Foreign population (EU28 countries) | 0.8 | 0.8 | 2.6 | 0.7 | |
| National population | 0.9 | 0.8 | 1.4 | 1.1 | |
| Too far to travel | Foreign population (total) | 0.1 | 0 | 0 | 0.1 |
| Foreign population (Non-EU28 countries) | 0.1 | 0 | 0 | 0 | |
| Foreign population (EU28 countries) | 0 | 0 | 0.1 | 0.3 | |
| National population | 0.1 | 0 | 0 | 0.1 | |
| No time | Foreign population (total) | 0.3 | 0.2 | 0.2 | 0.3 |
| Foreign population (Non-EU28 countries) | 0.3 | 0.2 | 0.1 | 0.4 | |
| Foreign population (EU28 countries) | 0.2 | 0.1 | 0.3 | 0 | |
| National population | 0.3 | 0.2 | 0.2 | 0.2 | |
| Didn’t know any doctor or specialist | Foreign population (total) | 0.1 | 0 | 0 | 0 |
| Foreign population (Non-EU28 countries) | 0.1 | 0.1 | 0 | 0 | |
| Foreign population (EU28 countries) | 0.1 | 0 | 0 | 0 | |
| National population | 0.1 | 0 | 0 | 0 | |
| Waiting list | Foreign population (total) | 0.8 | 0.3 | 0.2 | 0.2 |
| Foreign population (Non-EU28 countries) | 0.9 | 0.4 | 0.3 | 0.2 | |
| Foreign population (EU28 countries) | 0.7 | 0.3 | 0 | 0 | |
| National population | 1 | 0.5 | 0.3 | 0.5 | |
| Fear of doctor, hospital, examination or treatment | Foreign population (total) | 0.1 | 0.1 | 0.1 | 0 |
| Foreign population (Non-EU28 countries) | 0.1 | 0.1 | 0.1 | 0 | |
| Foreign population (EU28 countries) | 0.1 | 0.1 | 0.1 | 0 | |
| National population | 0.1 | 0.1 | 0.3 | 0.3 | |
| Wanted to wait and see if the problem got better on its own | Foreign population (total) | 0.3 | 0,2 | 0,4 | 0.2 |
| Foreign population (Non-EU28 countries) | 0.3 | 0,2 | 0,5 | 0.1 | |
| Foreign population (EU28 countries) | 0.2 | 0,1 | 0,1 | 0.5 | |
| National population | 0.6 | 0,3 | 0,4 | 0.3 | |
| No unmet needs to declare | Foreign population (total) | 96.7 | 97.8 | 97.4 | 97.3 |
| Foreign population (Non-EU28 countries) | 96.4 | 97.6 | 97.7 | 97 | |
| Foreign population (EU28 countries) | 97 | 98.2 | 96.4 | 98.1 | |
| National population | 96.5 | 97.9 | 97.3 | 96 | |
| Country | Health Profiles 2019 |
|---|---|
| Austria | Population coverage by health system is near-universal, including registered asylum seekers. Asylum seekers have good accessibility to outpatient clinics in public hospitals. A small number of people remain uninsured, including irregular migrants [32]. |
| Belgium | Large population covered for health services. Asylum seekers are entitled to medical care as the responsibility of reception centers that pays for any needed medical services. Irregular migrants are not covered and are excluded from the population covered because of the lack of legal resident authorization or regular address [33]. |
| Bulgaria | Lack of health system coverage as barrier to access to medical care for a considerable proportion of the population. Irregular migrants and population without a valid ID card (are not covered) [34]. |
| Cyprus | Only three quarters of residents are being covered free of charge to access the public health service (under the old system). The new General Health Care System aims to provide health coverage for third country nationals with legal residence and documented asylum seekers [35]. |
| Czechia | Most of the population benefited from the health system which is linked to permanent residence. Asylum seekers are also covered, but non-EU population, who are not employed or self-employed in Czechia, must purchase private health insurance to be allowed to stay in the country and have access to health care [36]. |
| Estonia | Many populations have not been granted access for their health needs. The non-Estonian-speaking population, near a quarter of the population, is more likely to be uninsured for health access [37]. |
| Finland | Public health services are provided to all permanent residents if they are registered as residents in one of the municipalities. Irregular immigrants and asylum seekers who have not been granted asylum are the only people not covered by health services [38]. |
| France | The public health system covers most of the population, including costs for medical services provided in and outside hospitals. Irregular immigrants have access to a standard health benefit package [39]. |
| Germany | Health system coverage is mostly universal with a broad social benefit to population. Refugees, asylum seekers and irregular migrants have limited coverage and access to health care services, depending on their individual status [40]. |
| Greece | Universal coverage for health care for all population. Irregular migrants and asylum seekers (until they receive refugee status) and Roma population face further barriers in access to health services [41]. |
| Italy | Nearly all resident populations have automatic coverage of health services, including legal foreign residents, and have access to universal health care and medical services. Irregular immigrants’ access to health coverage in urgent and essential services [42]. |
| Luxembourg | Good coverage for health services to resident population with limitations for some vulnerable population groups, such as third-country nationals, for who inequalities to health access are higher [43]. |
| Malta | All resident population are covered by health system, as well as refugees and asylum seekers with a good population coverage. Free health care includes migrants, but with exclusions for those who are not entitled to work in the formal sector [44]. |
| Portugal | Residents are covered by health system, including all immigrants (who are in Portugal for more than 90 days) regardless of their legal status. Irregular migrants have granted access to public health services but face some barriers such as language and cultural differences [45]. |
| Romania | Health system aims to provide universal coverage. Those who are not covered by health system have access to a restricted minimum benefit package. The number of population without coverage is difficult to quantify (data are reported for the general population only and statistics by ethnic group is prohibited), but people without an identification document are excluded from statutory coverage [46]. |
| Slovakia | Health system provides a comprehensive benefit package to nearly the entire population and is generally good, though hospital-centric. The Roma have guaranteed access to health care on equal terms, but with a low use of health services marked by limitations such as language, cultural and information barriers, and discrimination [47]. |
| Slovenia | Mostly all population residents are covered by health system if having permanent residency. Undocumented migrants, ethnic minorities and people with difficulty to meet formal residency requirements are excluded from health care access [48]. |
| Spain | Nearly all populations have access to health services provided and covered by the health system, but irregular migrants and asylum seekers face greater barriers in accessing health care [49]. |
| Sweden | All residents are automatically entitled to public health services, including new immigrants, and access to health care is generally good [50]. |
| United Kingdom | Health services are granted to people who are normal residents. Access to services is based on need rather than ability to pay. Irregular migrants have a limited benefit package that covers some health care. Non-European Economic Area migrants (until they have been awarded ‘indefinite leave to remain’) are required to pay for health services, but refugees and asylum seekers have free access to it [51]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casquilho-Martins, I.; Ferreira, S. Migrants’ Health Policies and Access to Health Care in Portugal within the European Framework. Societies 2022, 12, 55. https://doi.org/10.3390/soc12020055
Casquilho-Martins I, Ferreira S. Migrants’ Health Policies and Access to Health Care in Portugal within the European Framework. Societies. 2022; 12(2):55. https://doi.org/10.3390/soc12020055
Chicago/Turabian StyleCasquilho-Martins, Inês, and Soraia Ferreira. 2022. "Migrants’ Health Policies and Access to Health Care in Portugal within the European Framework" Societies 12, no. 2: 55. https://doi.org/10.3390/soc12020055
APA StyleCasquilho-Martins, I., & Ferreira, S. (2022). Migrants’ Health Policies and Access to Health Care in Portugal within the European Framework. Societies, 12(2), 55. https://doi.org/10.3390/soc12020055