Assessment of How House Ownership Shapes Health Outcomes in Urban Ghana

Abstract
:1. Introduction
1.1. Housing Issues in Ghana
“In order to meet the housing challenge in the country, government aims to establish a sustainable housing process which will eventually enable all Ghanaians to secure housing with secure tenure, within a safe and healthy environment and viable communities in a manner that will make a positive contribution to a democratic and integrated society, within the shortest possible time frame”.[14], (p. 10)
1.2. Health Concerns
1.3. Pension Policy
1.4. Power Relations
2. Materials and Methods
2.1. Sample Selection and Size
2.2. Research Instruments
Interviews
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Socio-Demographics
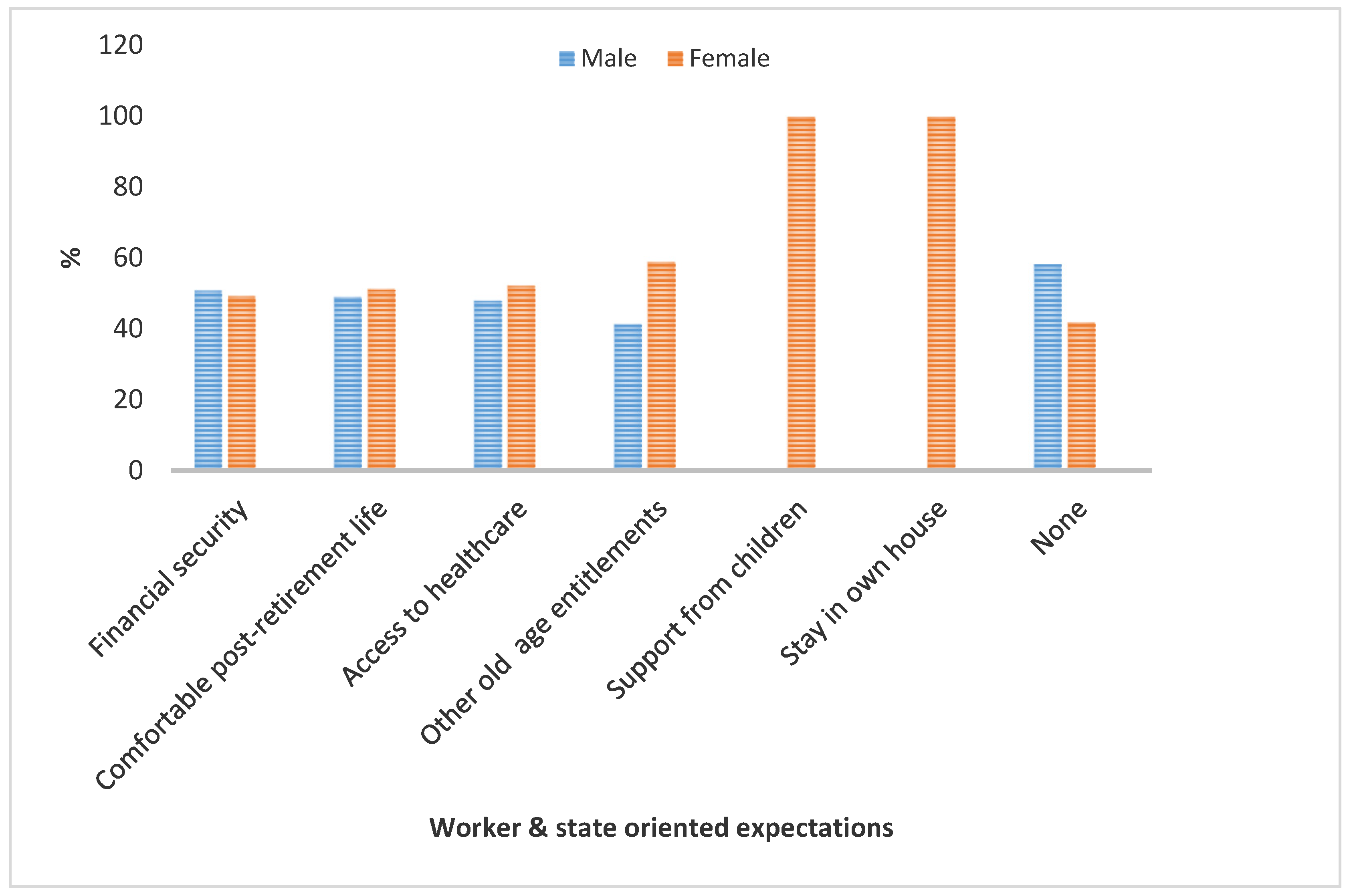
3.2. Workers’ Old Age Oriented Expectations
- National health insurance (NHI)—the registration and renewal of NHI is free for people aged 70+.
- Property and sewerage rebate, which offers a 30% property rebate for people aged 60+ for Tema residents.
3.3. House Ownership
I have acquired an apartment. I also have a house so that when I retire, I don’t have to struggle with issues of accommodation. This, I learnt from my father. It will make life easy for me.(Near-retired male)
I have a 2 bedroom house that I intend to live in, when I finally retire.(Near-retired female)
I acquired a house long before I retired about 10 years ago. I live in it with my children. At least, I have a roof over my head.(Retired female)
I live in my own house with my wife and children. Now that I have retired, I have a sound mind because of this property. If the rest of my children marry, the family size will only reduce but it still will remain intact in this house.(Retired male)
My late husband’s organization made him an offer regarding the purchase of the residence we were occupying. He discussed the issue with me and I encouraged him to purchase the apartment. He rather told me that he intended to build a house in his hometown in another region other than our region of residence - the Volta Region of Ghana. I vehemently detested that. As a result, I threatened him that if he does not buy the house on offer for us to stay in and he goes building in his hometown, when he retires, my children and I will not follow him to his hometown. He will go alone. You still have the choice of purchasing the property, where we have spent most of our adult lives, I said. However, he did not mind me. He rather continued with his diabolical plan of building elsewhere. A few years after that he retired, the Company’s Estate Unit notified him to vacate the residential premises. So, we moved bags and baggage out of the flat. He decided that we go to the village. I blatantly refused. Rather, I reminded him of what I told him earlier. It became a whole argument that brought in other people to intervene. But I did not budge. He packed off to the village. My five children and I rented a house here in Tema and relocated there. He on the other hand, got to the village alright but alone without the children and me. Later we heard that his health condition took a down turn with hypertension and diabetes. With time, his health deteriorated and he died as a result of that, just after two years of retirement.(Retired female)
3.4. Provision of End-of-Service Benefits
- The core constituents of TDC’s ESB system include medical care and a housing scheme that comprises plots of land and houses.
- Workers of SSNIT also enjoy employers’ retirement benefits in the form of medical care till death, house provision or housing loan.
3.5. Linkage between House Ownership and Health Outcomes
4. Discussion
I have always considered it is degrading in industrialized societies; that old people are put in old people’s homes where they are visited by their children from time to time. We must desist from creating or introducing such life’s dead ends into Ghanaian life. For me, the day we adopt such a culturally humiliating system will be gloomy one indeed. Let us continue to keep the aged in their homes with their children and grandchildren.(p. 19)
5. Conclusions
Funding
Conflicts of Interest
References
- De-Graft Aikins, A.; Apt, N.A. Aging in Ghana: Setting priorities for research, intervention and policy. Ghana Stud. J. 2016, 19, 35–45. [Google Scholar] [CrossRef]
- GSS. 2010 Population and Housing Census Summary Report of Final Results. 2010. Available online: http://statsghana.gov.gh/docfiles/2010phc/Census2010_Summary_report_of_final_results.pdf (accessed on 23 November 2015).
- GSS. 2010 Population and Housing Census: National Analytical Report; GSS: Accra, Ghana, 2013. [Google Scholar]
- Obiri-Yeboah, D.A.; Obiri-Yeboah, H. Ghana’s pension reform in perspective: Can the pension benefits provide a house a real need of the retiree? Eur. J. Bus. Manag. 2014, 6, 121–133. [Google Scholar]
- Dovie, D.A.; Ayimey, I.R.; Adodo-Samani, P. Pension policy dimension to Ghanaian workers’ housing needs provision. Soc. Novas Mod. 2018, 35, 30–56. [Google Scholar] [CrossRef]
- Dovie, D.A. Systematic preparation process and resource mobilisation towards postretirement life in urban Ghana: An exploration. Ghana Soc. Sci. J. 2018, 15, 64–97. [Google Scholar]
- Moons, N. The Right to Housing Laws and Society, 1st ed.; Routledge: New York, NY, USA, 2018. [Google Scholar]
- Berger, A. Encyclopedic Dictionary of Roman Law; American Philosophical Society: Philadelphia, PA, USA, 1980; ISBN 978-0-87169-432-4. [Google Scholar]
- Government of Ghana. Constitution of Republic of Ghana; National Commission on Civic Education: Accra, Ghana, 1992.
- Government of Ghana. Labour Act, 2003: Arrangement of Sections. 2003. Available online: http://www.nlcghana.org/nlc/privatecontent/document/LABOURACT2003.pdf (accessed on 15 February 2016).
- Hodges, J.; Baah, A. National Labour Law Profile: Ghana. 2019. Available online: http://www.ilo.org/ifpdial/information-resources/national-labour-law-profiles/WCMS_158898/lang--en/index.htm (accessed on 13 April 2019).
- Diamond, R. What Does Economic Evidence Tell Us about the Effects of Rent Control? 2018. Available online: https://www.brookings.edu/research/what-does-economic-evidence-tell-us-about-the-effects-of-rent-control/ (accessed on 15 April 2019).
- Diamond, R.; McQuadey, T.; Qian, F. The effects of Rent Control Expansion on Tenants, Landlords, and Inequality: Evidence from San Francisco. 2017. Available online: https://cepr.org/sites/default/files/McQuade,%20Tim%20DMQ_Paris.pdf (accessed on 15 April 2019).
- Government of Ghana. National Housing Policy. 2015. Available online: https://www.gredaghana.org/policy/National%20Housing%20Policy.pdf (accessed on 17 April 2019).
- Lusardi, A.; Mitchell, O.S. Older Adult Debt and Financial Frailty; Research Paper No. 2013–291; Michigan Retirement Research Center, University of Michigan: Ann Arbor, MI, USA; Available online: https://mrdrc.isr.umich.edu/publications/papers/pdf/wp291.pdf (accessed on 6 March 2019).
- Chesser, A.K.; Keene Woods, N.; Smothers, K.; Rogers, N. Health literacy and older adults: A systematic review. Gerontol. Geriatr. Med. 2016, 2. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.; Gazmararian, J.A.; Baker, D.W. Health literacy and functional health status among older adults. Arch. Intern. Med. 2015, 165, 1946–1952. [Google Scholar] [CrossRef] [PubMed]
- Dury, S.; Dierckc, E.; van der Vorst, A.; van der Elst, M.; Fret, B.; Duppen, D.; Hoeyberghs, L.; De Roeck, E.; Lambotte, D.; Smetcoren, A.-S.; et al. Detecting frail, older adults and identifying their strengths: Results of a mixed-methods study. BMC Public Health 2018, 18, 191. [Google Scholar] [CrossRef] [PubMed]
- Hardy, S.E.; Concato, J.; Gill, T.M. Stressful life events among community-living older persons. J. Gen. Intern. Med. 2002, 17, 841–847. [Google Scholar] [CrossRef] [Green Version]
- Apt, N.A. Ageing and the Changing Role of the Family and the Community: An African Perspective. Int. Soc. Secur. Rev. 2002, 55, 39–47. [Google Scholar] [CrossRef]
- Dovie, D.A. Leveraging healthcare opportunities for improved access among Ghanaian retirees: The case of active ageing. J. Soc. Sci. 2018, 7, 92. [Google Scholar] [CrossRef]
- Sharma, S.; Mueller, C.; Stewart, R.; Veronese, N.; Vancampfort, D.; Koyanagi, A.; Lamb, S.E.; Perera, G.; Stubbs, B. Predictors of falls and fractures leading to hospitalization in people with dementia: A representative cohort study. J. Am. Med. Dir. Assoc. 2018, 19, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Ayete-Nyampong, S. Ageing in Contemporary Ghana; Paper and Ink Media: Accra, Ghana, 2015. [Google Scholar]
- Zheng, C.; Yuetao, S.; Jia, Y.; Jintang, W. Differential development strategies of aged care support and community services in China, Japan and Australia. J. Clin. Gerontol. 2014, 5, 36–41. [Google Scholar] [CrossRef]
- Barrow, G.M. Ageing, the Individual and Society, 3rd ed.; West Publishing for Company: New York, NY, USA, 1986. [Google Scholar]
- Moody, H.R. Ageing: Concepts and Controversies, 6th ed.; Fine Forge Press: Los Angeles, CA, USA, 2010. [Google Scholar]
- Dovie, D.A. Financial literacy in an African society: An essential tool for retirement planning. Contemp. J. Afr. Stud. 2018, 5, 26–59. [Google Scholar]
- Agrawal, G.; Arokiasamy, P. Morbidity prevalence and healthcare utilization among older adults in India. J. Appl. Gerontol. 2010, 29, 155–179. [Google Scholar] [CrossRef]
- Van der Geest, S. Will families in Ghana continue to care for older people? Logic and contradiction in policy. In Ageing in Sub-Saharan Africa: Spaces and Practices of Care; Hoffman, J., Pype, K., Eds.; Policy Press: London, UK, 2016; pp. 21–42. [Google Scholar]
- Bloom, D.E.; Chatterji, S.; Kowal, P.; Lloyd-Sherlock, P.; Mckee, M.; Rechel, B.; Smith, J.P. Microeconomic implications of population aging and selected policy responses. Lancet 2015, 385, 649–657. [Google Scholar] [CrossRef]
- Chen, L.K. Towards elder-friendly outpatient services. J. Chin. Med Assoc. 2012, 75, 617–618. [Google Scholar] [CrossRef] [Green Version]
- Lukes, S. Power. A Radical View, 1st ed.; MacMillan Education: London, UK, 2005; p. 1. [Google Scholar]
- Barnett, M.; Duvall, R. Power in international politics. Int. Org. 2005, 59, 39–75. [Google Scholar] [CrossRef]
- Moore, D.R.; McCabe, G.P. Introduction to the Practice of Statistics, 2nd ed.; W.H. Freeman and Company: New York, NY, USA, 1993. [Google Scholar]
- Ghana Statistical Service. 2010 Population and Housing Census: District Analytical Report—Accra Metropolitan. 2012. Available online: http://www.statsghana.gov.gh/gssmain/storage/img/marqueeupdater/Census2010_Summary_report_of_final_results.pdf (accessed on 1 February 2016).
- Perneger, T.V.; Courvoisier, D.S.; Hudelson, P.M.; Gayet-Ageron, A. Sample size for pre-test of questionnaires. Qual. Life Res 2015, 2, 147–151. [Google Scholar] [CrossRef]
- Nardi, P. Doing Survey Research: A Guide to Quantitative Methods; Pearson: Boston, MA, USA, 2006. [Google Scholar]
- Neuman, W.L. Basics of Social Research: Qualitative and Quantitative Approaches; Pearson: Boston, MA, USA, 2004. [Google Scholar]
- Greenstein, R.; Roberts, B.; Sitas, A. Research Methods Training Manual. Compiled and Edited by Ran Greenstein. 2003. Available online: https://www.academia.edu/3198713/Research_Methods_Training_Manual (accessed on 14 March 2019).
- Joffe, H.; Yardley, L. Content and thematic analysis. In Research Methods for Clinical and Health Psychology; Marks, D.F., Yardley, L., Eds.; SAGE Publications: Thousand Oaks, CA, USA, 2004; pp. 56–68. [Google Scholar]
- Johnstone, P.L. Reflexivity and transparency in weighting up triangulating and contradictory evidence in mixed methods organisational research. In Proceedings of the 2nd Qualitative Research as Interpretive Practice Conference; Charles, S., Ed.; University of Michigan Medical Center Journal: Ann Arbor, MI, USA, 2006. [Google Scholar]
- Bazeley, P.; Jackson, K. Qualitative Data Analysis with Nvivo, 2nd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Dovie, D.A. The influence of MIPAA in formal support infrastructure development for the Ghanaian elderly. Int. J. Ageing Dev. Ctries. 2019, 3, 47–59. [Google Scholar]
- Dovie, D.A. Utilization of Digital Literacy in Retirement Planning Among Ghanaian Formal and Informal Sector Workers. Interações Soc. Novas Mod. 2018, 34, 113–140. [Google Scholar] [CrossRef]
- Holzmann, R.; Stiglitz, J. Introduction. In Toward Sustainable Pension Systems in the 21st Century: New Ideas about Old Age Security; Holzmann, R., Stiglitz, J., Fox, L., James, E., Orszag, P., Eds.; The World Bank: Washington, DC, USA, 2001; pp. 1–16. [Google Scholar]
- Government of Ghana. National Pension Act, 2008—Act 766; National Pensions Regulatory Authority: Accra, Ghana, 2008.
- Barrientos, A. Comparing pension schemes in Chile, Singapore, Brazil and South Africa. In Living longer: Ageing, Development and Social Protection; Lloyd-Sherlock, P., Ed.; Zed Books: London, UK, 2004; pp. 122–140. [Google Scholar]
- Frank, A. The individual in ageing Germany: How the self-employed plan for their old age. In Population Ageing from a Lifecourse Perspective: Critical & International Approaches; Komp, K., Johanson, S., Eds.; Policy Press: Bristol, UK, 2015. [Google Scholar]
- Dovie, D.A. The status of older adult care in contemporary Ghana: A profile of some emerging issues. Front. Sociol. 2019, 4, 25. [Google Scholar] [CrossRef]
- Aboderin, I. International Support and Old Age in Africa; Transaction Publishers: London, UK, 2006. [Google Scholar]
- Olenick, M.; Flowers, M.; Muñecas, T.; Maltsev, T. Positive and negative factors that influence health care faculty intent to engage in interprofessional education (IPE). Healthcare 2019, 7, 29. [Google Scholar] [CrossRef]
- Kpessa, W.M. The politics of retirement Income security policy in Ghana: Historical trajectories and transformative capabilities. Afr. J. Political Sci. Int. Relat. 2011, 5, 92–102. [Google Scholar]
- Daly, T.; Armstrong, P.; Lowndes, R. Liminality in Ontario’s long-term care Facilities: Private companions’ care work in the space ‘betwixt and between”. Compet. Chang. 2015, 19, 246–263. [Google Scholar] [CrossRef] [PubMed]
- Sarpong, P.K. Ageing and tradition. In Ageing and Social Change: A Ghanaian Perspective; Opare-Abetia, J., Ed.; Institute of Adult Education: Legon, Ghana, 1983; pp. 13–20. [Google Scholar]
- Suliman, N.N. The Intertwined Relationship between Power and Patriarchy: Examples from Resource Extractive Industries. Societies 2019, 9, 14. [Google Scholar] [CrossRef]
- Shah, A.K.; Mullainathan, S.; Shafir, E. Some consequences of having too little. Science 2012, 338, 682–685. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Values | df | Asymp. Sig (2-Sided) | |
|---|---|---|---|
| Pearson Chi-Square | 120.453 | 6 | 0.000 |
| N of valid Cases | 442 |
| Tests | Values | Degrees of Freedom | Asymp. Sig. (2-Sided) |
|---|---|---|---|
| Pearson Chi-Square | 150.801a | 10 | 0.000 |
| Cramer’s V | 0.750 | 10 | 0.000 |
| N of Valid Cases | 442 |
| Variables | Characteristics | Frequency | Percent (%) |
|---|---|---|---|
| Age | 18–24 | 21 | 4.8 |
| 25–29 | 42 | 9.5 | |
| 30–34 | 81 | 18.3 | |
| 35–39 | 58 | 13.1 | |
| 40–44 | 67 | 15.2 | |
| 45–49 | 59 | 13.3 | |
| 50–54 | 54 | 12.2 | |
| 55–59 | 60 | 13.6 | |
| Gender | Male | 213 | 48.2 |
| Female | 229 | 51.8 | |
| Educational level | No-formal education | 24 | 5.4 |
| Pre-tertiary education | 212 | 48.0 | |
| Tertiary | 206 | 46.4 | |
| Sector of work | Formal | 221 | 50 |
| Informal | 221 | 50 |
| Age Category | Yes | No | Cannot Tell |
|---|---|---|---|
| 18–29 | 26.9% | 68.7% | 4.5% |
| 30–39 | 62.4% | 25.5% | 12.1% |
| 40–49 | 61.3% | 33.9% | 4.8% |
| 50–59 | 53.6% | 36.4% | 10% |
| Benefits | Organizations | |
|---|---|---|
| SSNIT | TDC | |
| House | • | • |
| Housing loans | • | • |
| Plots of land | • | |
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dovie, D.A. Assessment of How House Ownership Shapes Health Outcomes in Urban Ghana. Societies 2019, 9, 43. https://doi.org/10.3390/soc9020043
Dovie DA. Assessment of How House Ownership Shapes Health Outcomes in Urban Ghana. Societies. 2019; 9(2):43. https://doi.org/10.3390/soc9020043
Chicago/Turabian StyleDovie, Delali A. 2019. "Assessment of How House Ownership Shapes Health Outcomes in Urban Ghana" Societies 9, no. 2: 43. https://doi.org/10.3390/soc9020043
APA StyleDovie, D. A. (2019). Assessment of How House Ownership Shapes Health Outcomes in Urban Ghana. Societies, 9(2), 43. https://doi.org/10.3390/soc9020043