Evaluation of Fatigue Behavior in Dental Implants from In Vitro Clinical Tests: A Systematic Review

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Questions
2.2. Inclusion and Exclusion Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Study Quality Assessment
2.7. Statistical Analysis
3. Results
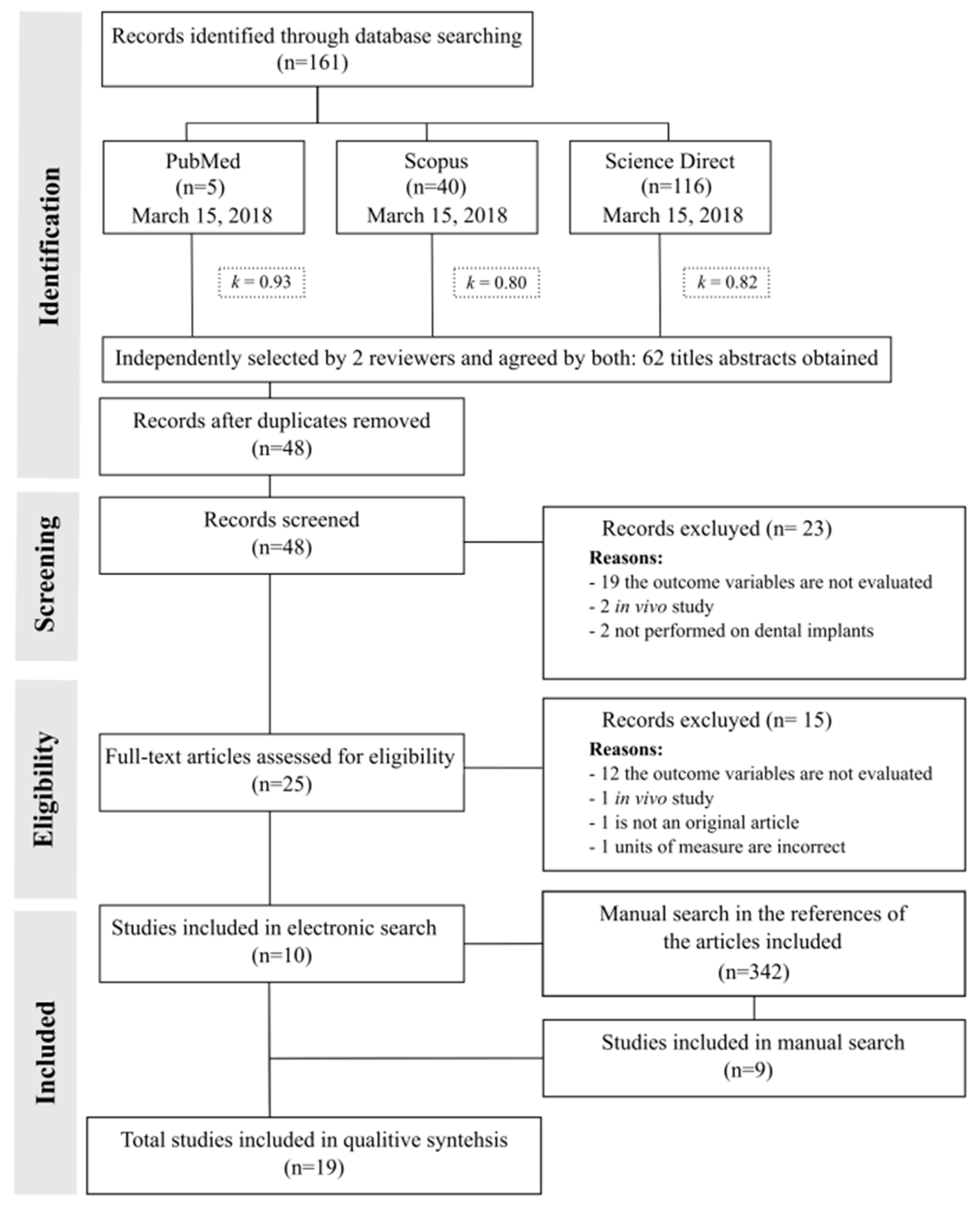
3.1. Study Selection
3.2. Relevant Data from Studies
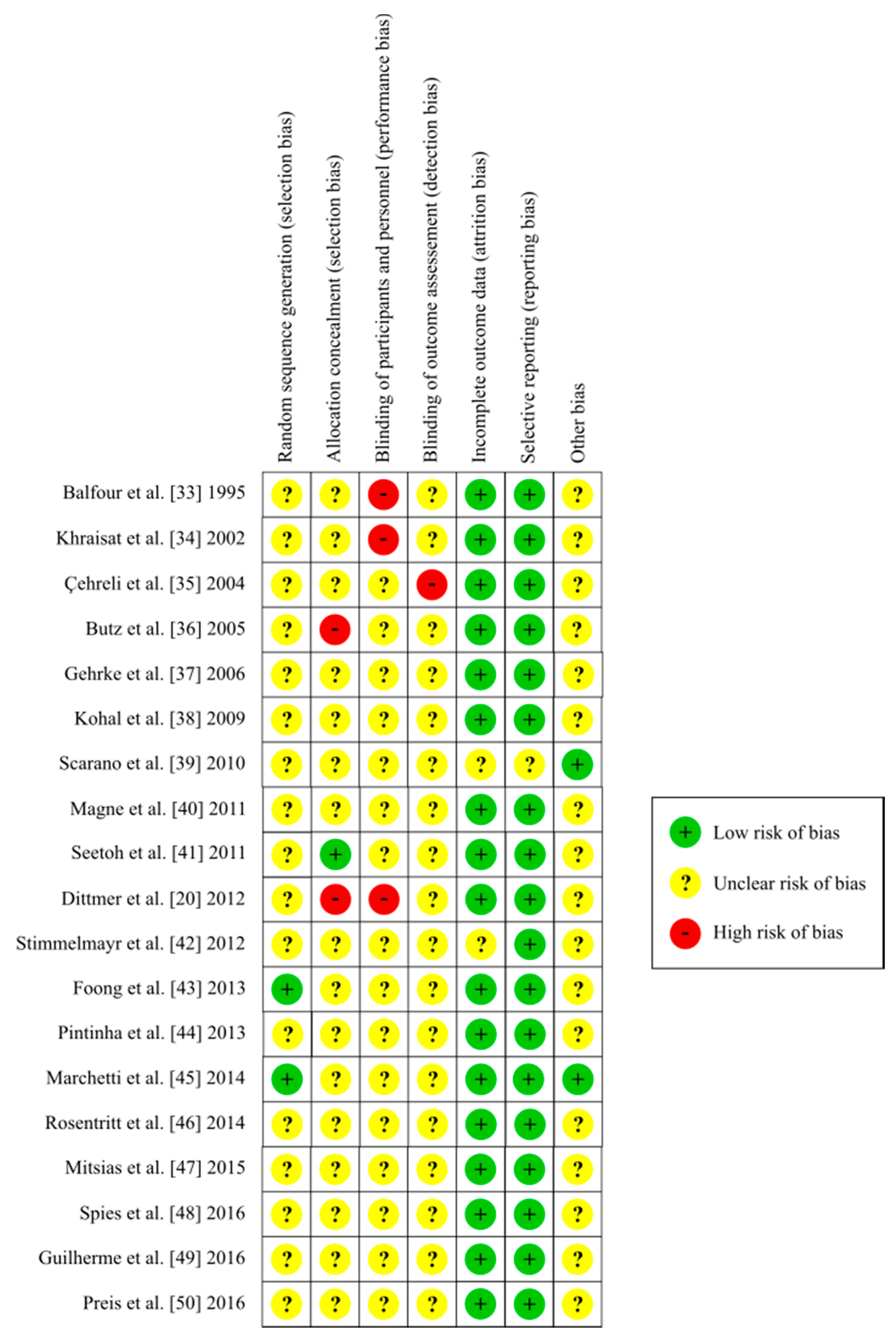
3.3. Study Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Tian, K.; Chen, J.; Han, L.; Yang, J.; Huang, W.; Wu, D. Angled abutments result in increased or decreased stress on surrounding bone of single-unit dental implants: A finite element analysis. Med. Eng. Phys. 2012, 34, 1526–1531. [Google Scholar] [CrossRef] [PubMed]
- Coray, R.; Zeltner, M.; Özcan, M. Fracture strength of implant abutments after fatigue testing: A systematic review and a meta-analysis. J. Mech. Behav. Biomed. Mater. 2016, 62, 333–346. [Google Scholar] [CrossRef] [PubMed]
- Elias, C.N.; Fernandes, D.J.; Resende, C.R.S.; Roestel, J. Mechanical properties, surface morphology and stability of a modified commercially pure high strength titanium alloy for dental implants. Dent. Mater. 2015, 31, e1–e13. [Google Scholar] [CrossRef] [PubMed]
- Osman, R.B.; Swain, M.V. A Critical Review of Dental Implant Materials with an Emphasis on Titanium versus Zirconia. Materials 2015, 8, 932–958. [Google Scholar] [CrossRef] [PubMed]
- Ottria, L.; Lauritano, D.; Andreasi Bassi, M.; Palmieri, A.; Candotto, V.; Tagliabue, A.; Tettamanti, L. Mechanical, chemical and biological aspects of titanium and titanium alloys in implant dentistry. J. Biol. Regul. Homeost. Agents 2018, 32, 81–90. [Google Scholar] [PubMed]
- Kirmanidou, Y.; Sidira, M.; Drosou, M.-E.; Bennani, V.; Bakopoulou, A.; Tsouknidas, A.; Michailidis, N.; Michalakis, K. New Ti-Alloys and Surface Modifications to Improve the Mechanical Properties and the Biological Response to Orthopedic and Dental Implants: A Review. Biomed Res. Int. 2016, 2016, 2908570. [Google Scholar] [CrossRef] [PubMed]
- Kent, D.; Wang, G.; Dargusch, M. Effects of phase stability and processing on the mechanical properties of Ti-Nb based beta Ti alloys. J. Mech. Behav. Biomed. Mater. 2013, 28, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Hatamleh, M.M.; Wu, X.; Alnazzawi, A.; Watson, J.; Watts, D. Surface characteristics and biocompatibility of cranioplasty titanium implants following different surface treatments. Dent. Mater. 2018, 34, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Wennerberg, A. The importance of surface roughness for implant incorporation. Int. J. Mach. Tools Manuf. 1998, 38, 657–662. [Google Scholar] [CrossRef]
- Komasa, S.; Taguchi, Y.; Nishida, H.; Tanaka, M.; Kawazoe, T. Bioactivity of nanostructure on titanium surface modified by chemical processing at room temperature. J. Prosthodont. Res. 2012, 56, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Kubasiewicz-Ross, P.; Dominiak, M.; Gedrange, T.; Botzenhart, U.U. Zirconium: The material of the future in modern implantology. Adv. Clin. Exp. Med. 2017, 26, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Freitas, G.; Hirata, R.; Bonfante, E.; Tovar, N.; Coelho, P. Survival Probability of Narrow and Standard-Diameter Implants with Different Implant-Abutment Connection Designs. Int. J. Prosthodont. 2016, 29, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, D. Implants for life? A critical review of implant-supported restorations. J. Dent. 2007, 35, 768–772. [Google Scholar] [CrossRef] [PubMed]
- Pardal-Pelaez, B.; Montero, J. Preload loss of abutment screws after dynamic fatigue in single implant-supported restorations. A systematic review. J. Clin. Exp. Dent. 2017, 9, e1355–e1361. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Delgado-Ruiz, R.A.; Prados Frutos, J.C.; Prados-Privado, M.; Dedavid, B.A.; Granero Marin, J.M.; Calvo Guirado, J.L. Misfit of Three Different Implant-Abutment Connections Before and After Cyclic Load Application: An In Vitro Study. Int. J. Oral Maxillofac. Implant. 2017, 32, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Prados-Privado, M.; Bea, J.A.; Rojo, R.; Gehrke, S.A.; Calvo-Guirado, J.L.; Prados-Frutos, J.C. A New Model to Study Fatigue in Dental Implants Based on Probabilistic Finite Elements and Cumulative Damage Model. Appl. Bionics Biomech. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, C.M.; Nogueira-Filho, G.; Tenenbaum, H.C.; Lai, J.Y.; Brito, C.; Döring, H.; Nonhoff, J. Performance of conical abutment (Morse Taper) connection implants: A systematic review. J. Biomed. Mater. Res. Part A 2014, 102, 552–574. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Sailer, T.; Stawarczyk, B.; Jung, R.E.; Hämmerle, C.H.F. In vitro study of the influence of the type of connection on the fracture load of zirconia abutments with internal and external implant-abutment connections. Int. J. Oral Maxillofac. Implant. 2009, 24, 850–858. [Google Scholar] [CrossRef]
- Kitagawa, T.; Tanimoto, Y.; Odaki, M.; Nemoto, K.; Aida, M. Influence of implant/abutment joint designs on abutment screw loosening in a dental implant system. J. Biomed. Mater. Res. Part B Appl. Biomater. 2005, 75B, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Dittmer, M.P.; Dittmer, S.; Borchers, L.; Kohorst, P.; Stiesch, M. Influence of the interface design on the yield force of the implant–abutment complex before and after cyclic mechanical loading. J. Prosthodont. Res. 2012, 56, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Ritter, J.E. Critique of test methods for lifetime predictions. Dent. Mater. 1995, 11, 147–151. [Google Scholar] [CrossRef]
- Marx, R.; Jungwirth, F.; Walter, P.-O. Threshold intensity factors as lower boundaries for crack propagation in ceramics. Biomed. Eng. Online 2004, 3, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alqahtani, F.; Flinton, R. Postfatigue fracture resistance of modified prefabricated zirconia implant abutments. J. Prosthet. Dent. 2014, 112, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Organization, I.S. ISO 14801: Dentistry—Implants—Dynamic Fatigue Test for Endosseous Dental Implants; ISO: Geneve, Switzerland, 2007. [Google Scholar]
- Marchetti, E.; Ratta, S.; Mummolo, S.; Tecco, S.; Pecci, R.; Bedini, R.; Marzo, G. Mechanical Reliability Evaluation of an Oral Implant-Abutment System According to UNI EN ISO 14801 Fatigue Test Protocol. Implant Dent. 2016, 25, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.K.; Karl, M.; Kelly, J.R. Evaluation of test protocol variables for dental implant fatigue research. Dent. Mater. 2009, 25, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Snauwaert, K.; Duyck, J.; van Steenberghe, D.; Quirynen, M.; Naert, I. Time dependent failure rate and marginal bone loss of implant supported prostheses: A 15-year follow-up study. Clin. Oral Investig. 2000, 4, 0013–0020. [Google Scholar] [CrossRef]
- Hasan, I.; Bourauel, C.; Mundt, T.; Stark, H.; Heinemann, F. Biomechanics and load resistance of small-diameter and mini dental implants: A review of literature. Biomed. Tech. Eng. 2014, 59, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Altman, D.G.; Liberati, A.; Tetzlaff, J. PRISMA statement. Epidemiology 2011, 22, 128. [Google Scholar] [CrossRef] [PubMed]
- Centre for Rewies and Dissemination, University of York. Systematic Reviews: CRD Guidance for Undertaking Reviews in Health Care; University of York: York, UK, 2009. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G. Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Green, S., Eds.; Wiley: Hoboken, NJ, USA, 2008; pp. 187–241. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Balfour, A.; O’Brien, G.R. Comparative study of antirotational single tooth abutments. J. Prosthet. Dent. 1995, 73, 36–43. [Google Scholar] [CrossRef]
- Khraisat, A.; Stegaroiu, R.; Nomura, S.; Miyakawa, O. Fatigue resistance of two implant/abutment joint designs. J. Prosthet. Dent. 2002, 88, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Cehreli, M.C.; Akca, K.; Iplikcioglu, H.; Sahin, S. Dynamic fatigue resistance of implant-abutment junction in an internally notched morse-taper oral implant: Influence of abutment design. Clin. Oral Implant. Res. 2004, 15, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Butz, F.; Heydecke, G.; Okutan, M.; Strub, J.R. Survival rate, fracture strength and failure mode of ceramic implant abutments after chewing simulation. J. Oral Rehabil. 2005, 32, 838–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gehrke, P.; Dhom, G.; Brunner, J.; Wolf, D.; Degidi, M.; Piattelli, A. Zirconium implant abutments: Fracture strength and influence of cyclic loading on retaining-screw loosening. Quintessence Int. 2006, 37, 19–26. [Google Scholar] [PubMed]
- Kohal, R.-J.; Finke, H.C.; Klaus, G. Stability of prototype two-piece zirconia and titanium implants after artificial aging: An in vitro pilot study. Clin. Implant Dent. Relat. Res. 2009, 11, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Sacco, M.L.; Di Iorio, D.; Amoruso, M.; Mancino, C. Valutazione della resistenza a fatica ciclica di una connessione impianto-abutment cone morse e avvitata. Ital. Oral Surg. 2010, 9, 173–179. [Google Scholar] [CrossRef]
- Magne, P.; Oderich, E.; Boff, L.L.; Cardoso, A.C.; Belser, U.C. Fatigue resistance and failure mode of CAD/CAM composite resin implant abutments restored with type III composite resin and porcelain veneers. Clin. Oral Implant. Res. 2011, 22, 1275–1281. [Google Scholar] [CrossRef] [PubMed]
- Seetoh, Y.L.; Tan, K.B.; Chua, E.K.; Quek, H.C.; Nicholls, J.I. Load fatigue performance of conical implant-abutment connections. Int. J. Oral Maxillofac. Implant. 2011, 26, 797–806. [Google Scholar]
- Stimmelmayr, M.; Edelhoff, D.; Güth, J.-F.; Erdelt, K.; Happe, A.; Beuer, F. Wear at the titanium–titanium and the titanium–zirconia implant–abutment interface: A comparative in vitro study. Dent. Mater. 2012, 28, 1215–1220. [Google Scholar] [CrossRef] [PubMed]
- Foong, J.K.W.; Judge, R.B.; Palamara, J.E.; Swain, M.V. Fracture resistance of titanium and zirconia abutments: An in vitro study. J. Prosthet. Dent. 2013, 109, 304–312. [Google Scholar] [CrossRef]
- Pintinha, M.; Camarini, E.T.; Sábio, S.; Pereira, J.R. Effect of mechanical loading on the removal torque of different types of tapered connection abutments for dental implants. J. Prosthet. Dent. 2013, 110, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, E.; Ratta, S.; Mummolo, S.; Tecco, S.; Pecci, R.; Bedini, R.; Marzo, G. Evaluation of an Endosseous Oral Implant System According to UNI EN ISO 14801 Fatigue Test Protocol. Implant Dent. 2014, 23, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Rosentritt, M.; Hagemann, A.; Hahnel, S.; Behr, M.; Preis, V. In vitro performance of zirconia and titanium implant/abutment systems for anterior application. J. Dent. 2014, 42, 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Mitsias, M.E.; Thompson, V.P.; Pines, M.; Silva, N.R.F.A. Reliability and failure modes of two Y-TZP abutment designs. Int. J. Prosthodont. 2015, 28, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Spies, B.C.; Nold, J.; Vach, K.; Kohal, R.-J. Two-piece zirconia oral implants withstand masticatory loads: An investigation in the artificial mouth. J. Mech. Behav. Biomed. Mater. 2016, 53, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Guilherme, N.M.; Chung, K.-H.; Flinn, B.D.; Zheng, C.; Raigrodski, A.J. Assessment of reliability of CAD-CAM tooth-colored implant custom abutments. J. Prosthet. Dent. 2016, 116, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Preis, V.; Kammermeier, A.; Handel, G.; Rosentritt, M. In vitro performance of two-piece zirconia implant systems for anterior application. Dent. Mater. 2016, 32, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Sahin, S.; Cehreli, M.C.; Yalcin, E. The influence of functional forces on the biomechanics of implant-supported prostheses—A review. J. Dent. 2002, 30, 271–282. [Google Scholar] [CrossRef]
- Flanagan, D. Bite force and dental implant treatment: A short review. Med. Devices 2017, 10, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Factors Influencing Early Dental Implant Failures. J. Dent. Res. 2016, 95, 995–1002. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, S.A.; Stanford, C.M.; Buranadham, S.; Fridrich, T.; Wagner, J.; Gratton, D. Dynamic fatigue properties of the dental implant-abutment interface: Joint opening in wide-diameter versus standard-diameter hex-type implants. J. Prosthet. Dent. 2001, 85, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, A.; Scarano, A.; Piattelli, M.; Vaia, E.; Matarasso, S. Hollow implants retrieved for fracture: A light and scanning electron microscope analysis of 4 cases. J. Periodontol. 1998, 69, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Tolman, D.E.; Laney, W.R. Tissue-integrated prosthesis complications. Int. J. Oral Maxillofac. Implants 1992, 7, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Steinebrunner, L.; Wolfart, S.; Ludwig, K.; Kern, M. Implant-abutment interface design affects fatigue and fracture strength of implants. Clin. Oral Implant. Res. 2008, 19, 1276–1284. [Google Scholar] [CrossRef] [PubMed]
- Pita, M.S.; Anchieta, R.B.; Barao, V.A.; Garcia, I.R., Jr.; Pedrazzi, V.; Assuncao, W.G. Prosthetic platforms in implant dentistry. J. Craniofac. Surg. 2011, 22, 2327–2331. [Google Scholar] [CrossRef] [PubMed]
- Gaviria, L.; Salcido, J.P.; Guda, T.; Ong, J.L. Current trends in dental implants. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Finger, I.M.; Castellon, P.; Block, M.; Elian, N. The evolution of external and internal implant/abutment connections. Pract. Proced. Aesthet. Dent. 2003, 15, 625–632. [Google Scholar] [PubMed]
- Binon, P.P. Implants and components: Entering the new millennium. Int. J. Oral Maxillofac. Implant. 2000, 15, 76–94. [Google Scholar]
- Gracis, S.; Michalakis, K.; Vigolo, P.; Vult von Steyern, P.; Zwahlen, M.; Sailer, I. Internal vs. external connections for abutments/reconstructions: A systematic review. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 202–216. [Google Scholar] [CrossRef] [PubMed]
- Macedo, J.P.; Pereira, J.; Vahey, B.R.; Henriques, B.; Benfatti, C.A.; Magini, R.S.; Lopez-Lopez, J.; Souza, J.C. Morse taper dental implants and platform switching: The new paradigm in oral implantology. Eur. J. Dent. 2016, 10, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.C.; Lin, D.H.; Jiang, C.P.; Lee, S.Y. Design improvement and dynamic finite element analysis of novel ITI dental implant under dynamic chewing loads. Biomed. Mater. Eng. 2015, 26 (Suppl. 1), S555–S561. [Google Scholar] [CrossRef] [PubMed]
- Prados-Privado, M.; Prados-Frutos, J.C.; Calvo-Guirado, J.L.; Bea, J.A. A random fatigue of mechanize titanium abutment studied with Markoff chain and stochastic finite element formulation. Comput. Methods Biomech. Biomed. Eng. 2016, 19, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Anchieta, R.B.; Machado, L.S.; Hirata, R.; Bonfante, E.A.; Coelho, P.G. Platform-Switching for Cemented Versus Screwed Fixed Dental Prostheses: Reliability and Failure Modes: An In Vitro Study. Clin. Implant Dent. Relat. Res. 2016, 18, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Bordin, D.; Bergamo, E.T.P.; Fardin, V.P.; Coelho, P.G.; Bonfante, E.A. Fracture strength and probability of survival of narrow and extra-narrow dental implants after fatigue testing: In vitro and in silico analysis. J. Mech. Behav. Biomed. Mater. 2017, 71, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-W.; Covel, N.S.; Guess, P.C.; Rekow, E.D.; Zhang, Y. Concerns of hydrothermal degradation in CAD/CAM zirconia. J. Dent. Res. 2010, 89, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Kawai, Y.; Uo, M.; Wang, Y.; Kono, S.; Ohnuki, S.; Watari, F. Phase transformation of zirconia ceramics by hydrothermal degradation. Dent. Mater. J. 2011, 30, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Krithikadatta, J.; Gopikrishna, V.; Datta, M. CRIS Guidelines (Checklist for Reporting In-vitro Studies): A concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J. Conserv. Dent. 2014, 17, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Palmas, W. The CONSORT guidelines for noninferiority trials should be updated to go beyond the absolute risk difference. J. Clin. Epidemiol. 2017, 83, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Machado, L.S.; Bonfante, E.A.; Anchieta, R.B.; Yamaguchi, S.; Coelho, P.G. Implant-abutment connection designs for anterior crowns: Reliability and failure modes. Implant Dent. 2013, 22, 540–545. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Database | Search Strategy | Search Data |
|---|---|---|
| MEDLINE/PubMed | (dental AND (implant OR abutment) OR tooth implant) AND (cyclic loading) AND ((internal OR external) connection) AND (fatigue OR moment OR stress) AND (“in vitro” OR “experimental study”) NOT (review) | 15 March 2018 |
| Scopus | (dental AND (implant OR abutment) OR tooth implant) AND (cyclic loading) AND ((internal OR external) connection) AND (fatigue OR moment OR stress) AND (“in vitro” OR “experimental study”) AND NOT (review) | 15 March 2018 |
| Science Direct | (dental AND (implant OR abutment) OR tooth implant) AND (cyclic loading) AND ((internal OR external) connection) AND (fatigue OR moment OR stress) AND (“in vitro” OR “experimental study”) AND NOT (review) | 15 March 2018 |
| Author/Year | Country | Journal | n | G | Financing |
|---|---|---|---|---|---|
| Balfour et al. [33] 1995 | United States | Journal of Prosthetic Dentistry | 21 | 3 | U |
| Khraisat et al. [34] 2002 | Japan | Journal of Prosthetic Dentistry | 14 | 2 | U |
| Çehreli et al. [35] 2004 | Turkey | Clinical Oral Implants Research | 8 | 1 | Y |
| Butz et al. [36] 2005 | United States | Journal of Oral Rehabilitation | 48 | 3 | Y |
| Gehrke et al. [37] 2006 | Germany | Quintessence International | 7 | 1 | U |
| Kohal et al. [38] 2009 | Germany | Clinical Implant Dentistry and Related Research, | 48 | 3 | U |
| Scarano et al. [39] 2010 | Italy | Italian Oral Surgery | 20 | 1 | N |
| Magne et al. [40] 2011 | Switzerland | Clinical Oral Implants Research | 28 | 2 | Y |
| Seetoh et al. [41] 2011 | Republic of Singapore | The International Journal of Oral & Maxillofacial Implants | 30 | 6 | Y |
| Dittmer et al. [20] 2012 | Germany | Journal of Prosthodontic Research | 60 | 2 | Y |
| Stimmelmayr et al. [42] 2012 | Germany | Dental Materials | 6 | 2 | Y |
| Foong et al. [43] 2013 | Australia | Journal of Prosthetic Dentistry | 22 | 2 | Y |
| Pintinha et al. [44] 2013 | Brazil | Journal of Prosthetic Dentistry | 48 | 2 | U |
| Marchetti et al. [45] 2014 | Italy | Implant Dentistry | 15 | 2 | N |
| Rosentritt et al. [46] 2014 | Germany | Journal of Dentistry | 64 | 8 | Y |
| Mitsias et al. [47] 2015 | Greece | The International Journal of Prosthodontics | 36 | 2 | N |
| Spies et al. [48] 2016 | Germany | Journal of the Mechanical Behavior of Biomedical Materials | 48 | 3 | Y |
| Guilherme et al. [49] 2016 | United States | Journal of Prosthetic Dentistry | 57 | 3 | Y |
| Preis et al. [50] 2016 | Germany | Dental Materials | 60 | 6 | Y |
| Author/Year | Implant | Abutment | Applied Load | Cycles | Failure | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Connection | Material | Diameter | Length | Material | Length | Magnitude (N) | Angulation (°) | Frequency (Hz) | |||
| Çehreli et al. [35] 2004 | - | - | 10 | - | - | - | 75 ± 5 | 20 | 0.5 | 500,000 | N |
| Butz et al. [36] 2005 | E | - | 4 | 13 | Ti | - | 30 | 130 | 1.3 | 1,200,000 | Y |
| - | - | 4 | 13 | Zr | - | 30 | 130 | 1.3 | 1,200,000 | Y | |
| - | - | 4 | 13 | Ti | - | 30 | 130 | 1.3 | 1,200,000 | Y | |
| Gehrke et al. [37] 2006 | I | - | 4.5 | 18 | Zi | - | 100–450 | - | 15 | 5,000,000 | Y |
| I | - | 4.5 | 18 | Zi | - | 100–450 | - | 15 | 5,000,000 | Y | |
| I | - | 4.5 | 18 | Zi | - | 100–450 | - | 15 | 5,000,000 | Y | |
| Kohal et al. [38] 2009 | M | Zr | - | - | Zi | - | 45 | - | - | 1,200,000 | Y |
| M | Zr | - | - | Zi | - | 45 | - | - | 1,200,000 | Y | |
| M | Ti | - | - | P | - | 45 | - | - | 1,200,000 | Y | |
| Scarano et al. [39] 2010 | M | Ti | 4 | 13 | - | - | 5–230 | 30 | 4 | 1,000,000 | N |
| Magne et al. [40] 2011 | I | - | 4.1 | 12 | Metal | 12 | 80–280 | 30 | 5 | 20,000 | Y |
| Dittmer et al. [20] 2012 | I | - | 4.5 | 13 | Ti | 1.5 | 100 | 30 | 2 | 1,000,000 | Y |
| I | - | 4.5 | 13 | Ti | 4.1 | 100 | 30 | 2 | 1,000,000 | Y | |
| E | - | 4.3 | 13 | - | 11 | 100 | 30 | 2 | 1,000,000 | Y | |
| I | - | 4.5 | 14 | - | - | 100 | 30 | 2 | 1,000,000 | Y | |
| E | - | 4 | 13 | - | 1 | 100 | 30 | 2 | 1,000,000 | Y | |
| I | - | 4.1 | 14 | Ti | 5.5 | 100 | 30 | 2 | 1,000,000 | Y | |
| Stimmelmayr et al. [42] 2012 | I | Ti | 3.8 | 13 | Ti | 10 | 100 | - | 1.2 | 1,200,000 | N |
| I | Ti | 3.8 | 13 | Zr | 10 | 100 | - | 1.2 | 1,200,000 | N | |
| Pintinha et al. [44] 2013 | I | Ti | 4 | 10 | Ti | 8.7 | 100 ± 5 | 20 | 2 | 500 | N |
| I | Ti | 4 | 10 | Ti | 9 | 100 ± 5 | 20 | 2 | 500 | N | |
| Rosentritt et al. [46] 2014 | I | Zr | 4.1 | 10 | Zr | - | 50 | 45 | 1.6 | 1,200,000 | Y |
| I | Zr | 4 | 10 | Zr | - | 50 | 45 | 1.6 | 1,200,000 | N | |
| I | Zr | 4.1 | 11 | Zr | - | 50 | 45 | 1.6 | 1,200,000 | Y | |
| I | Zr | 4.1 | 14 | Zr | - | 50 | 45 | 1.6 | 1,200,000 | Y | |
| I | Ti | 4 | 10 | Ti | - | 50 | 45 | 1.6 | 1,200,000 | Y | |
| I | Ti | 4.1 | 15 | Ti | - | 50 | 45 | 1.6 | 1,200,000 | N | |
| I | Zr | 4.5 | 12 | Zr | - | 50 | 45 | 1.6 | 1,200,000 | N | |
| I | Zr | 4 | 10 | Zr | - | 50 | 45 | 1.6 | 1,200,000 | N | |
| Mitsias et al. [47] 2015 | M | - | - | - | Y-TZP | - | 400 | 30 | - | 100,000 | Y |
| M | - | - | - | Y-TPZ | - | 400 | 30 | - | 100,000 | Y | |
| Spies et al. [48] 2015 | E | ATZ | 4.4/4.1/4.2 | 12 | - | - | 98 | - | 2 | 10,000,000 | N |
| I | Y-TZP-A | 4.1 | 12 | Y-TZP-A | 6 | 98 | - | 2 | 10,000,000 | N | |
| E | Y-TZP-A | 4.2 | 12 | ATZ | 6 | 98 | - | 2 | 10,000,000 | N | |
| Guilherme et al. [49] 2016 | M | - | 4.3 | 10 | Zr | - | 150–200 | - | 2 | 100 | N |
| M | - | 4.3 | 10 | LD | - | 150–200 | - | 2 | 100 | N | |
| M | - | 4.3 | 10 | R-BC | - | 150–200 | - | 2 | 100 | N | |
| Preis et al. [50] 2016 | I | Zr | 4.1 | 10 | Zr | - | 100 | 45 | 1.6 | 3,600,000 | N |
| I | Zr | 4.1 | 10 | Zr | - | 100 | 45 | 1.6 | 3,600,000 | Y | |
| I | Zr | 3.8 | 11 | Zr | - | 100 | 45 | 1.6 | 3,600,000 | Y | |
| I | Zr | 4.6 | 11 | Zr | - | 100 | 45 | 1.6 | 3,600,000 | Y | |
| I | Zr | 4.1 | 10 | Zr | - | 100 | 45 | 1.6 | 3,600,000 | Y | |
| I | Zr | 4.1 | 10 | Zr | - | 100 | 45 | 1.6 | 3,600,000 | Y | |
| I | Ti | 4.1 | 12 | Ti | - | 100 | 45 | 1.6 | 3,600,000 | N | |
| Author/Year | Implant | Abutment | Applied Load | Cycles | Failure | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Connection | Material | Diameter | Length | Material | Length | Magnitude | Angulation | Frequency | |||
| Balfour et al. [33] 1995 | E | Ti | - | - | Ti | - | 242 | 30 | 14 | 5,000,000 | Y |
| I | Ti | - | - | Ti | - | 400 | 30 | 14 | 5,000,000 | Y | |
| I | Ti | - | - | Ti | - | 367 | 30 | 14 | 5,000,000 | Y | |
| Khraisat et al. [34] 2002 | E | Ti | 4 | 10 | Ti | 3 | 100 | 90 | 1,25 | 1,800,000 | Y (1,178,023 and 1,733,526) |
| M | Ti | 4.1 | 10 | Ti | 10 | 100 | 90 | 1,25 | 1,800,000 | Y (more 1,800,000) | |
| Seetoh et al. [41] 2011 | M | - | 4.5 | 15 | Zr/Ti | - | 21 | 45 | 10 | 5,000,000 | Y |
| I | - | 4 | 15 | Zr/Ti | - | 21 | 45 | 10 | 5,000,000 | Y | |
| M | - | 4.1 | 14 | Zr/Ti | - | 21 | 45 | 10 | 5,000,000 | Y | |
| Foong et al. [43] 2013 | I | Ti | 4 | 9 | Ti | 1.5 | 50–400 | 30 | 2 to 5 | 5,000–20,000 | Y (mean of 81,935) |
| I | Ti | 4 | 9 | Zr | 1.5 | 50–400 | 30 | 2 to 5 | 5,000–20,000 | Y (mean of 26,926) | |
| Marchetti et al. [45] 2014 | I | Ti | 3.8 | 13 | Ti | - | 400 | 30 ± 2 | 15 | 5,000,000 | Y (12,678 and 15,387) |
| I | Ti | 3.8 | 13 | Ti | - | 300 | 30 ± 2 | 15 | 5,000,000 | Y (more 27,732) | |
| Mitsias et al. [47] 2015 | M | - | - | - | Y-TZP | - | 400 | 30 | - | 100,000 | Y (less than 50,000) |
| M | - | - | - | Y-TPZ | - | 400 | 30 | - | 100,000 | Y (less than 50,000) | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojo, R.; Prados-Privado, M.; Reinoso, A.J.; Prados-Frutos, J.C. Evaluation of Fatigue Behavior in Dental Implants from In Vitro Clinical Tests: A Systematic Review. Metals 2018, 8, 313. https://doi.org/10.3390/met8050313
Rojo R, Prados-Privado M, Reinoso AJ, Prados-Frutos JC. Evaluation of Fatigue Behavior in Dental Implants from In Vitro Clinical Tests: A Systematic Review. Metals. 2018; 8(5):313. https://doi.org/10.3390/met8050313
Chicago/Turabian StyleRojo, Rosa, María Prados-Privado, Antonio José Reinoso, and Juan Carlos Prados-Frutos. 2018. "Evaluation of Fatigue Behavior in Dental Implants from In Vitro Clinical Tests: A Systematic Review" Metals 8, no. 5: 313. https://doi.org/10.3390/met8050313
APA StyleRojo, R., Prados-Privado, M., Reinoso, A. J., & Prados-Frutos, J. C. (2018). Evaluation of Fatigue Behavior in Dental Implants from In Vitro Clinical Tests: A Systematic Review. Metals, 8(5), 313. https://doi.org/10.3390/met8050313