
Home Birth in Portugal—A Comprehensive Analysis Based on Official Statistical Data


Abstract
:1. Introduction
2. Materials and Methods
3. Results
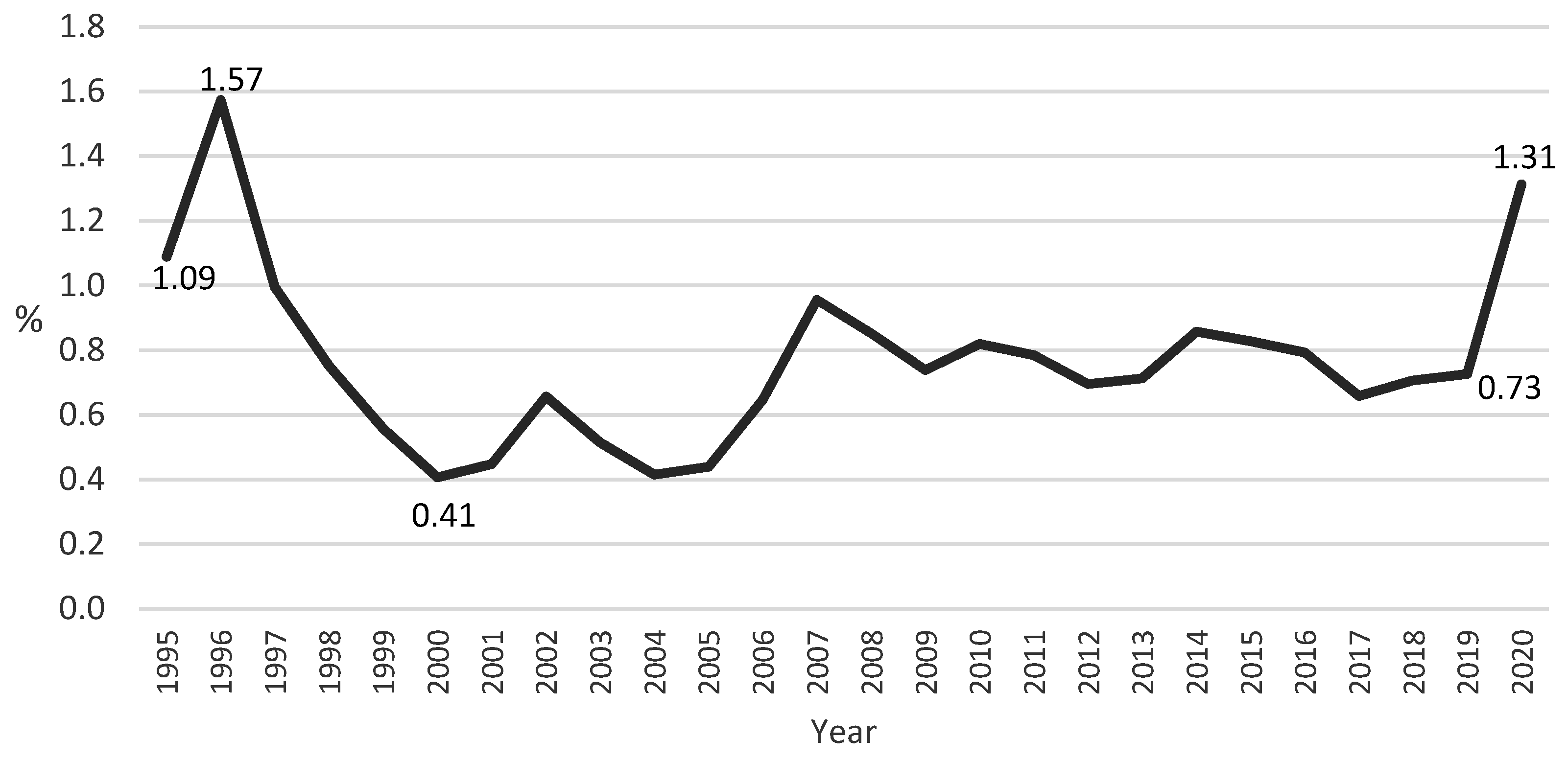
3.1. Place of Birth in Portugal between 1995 and 2020
3.2. Home and Hospital Births in Portugal in 2020
3.2.1. Sociodemographic Characteristics of the Mothers
3.2.2. Nationality and Residence of the Mother
3.2.3. Length of Pregnancy
3.2.4. Parity
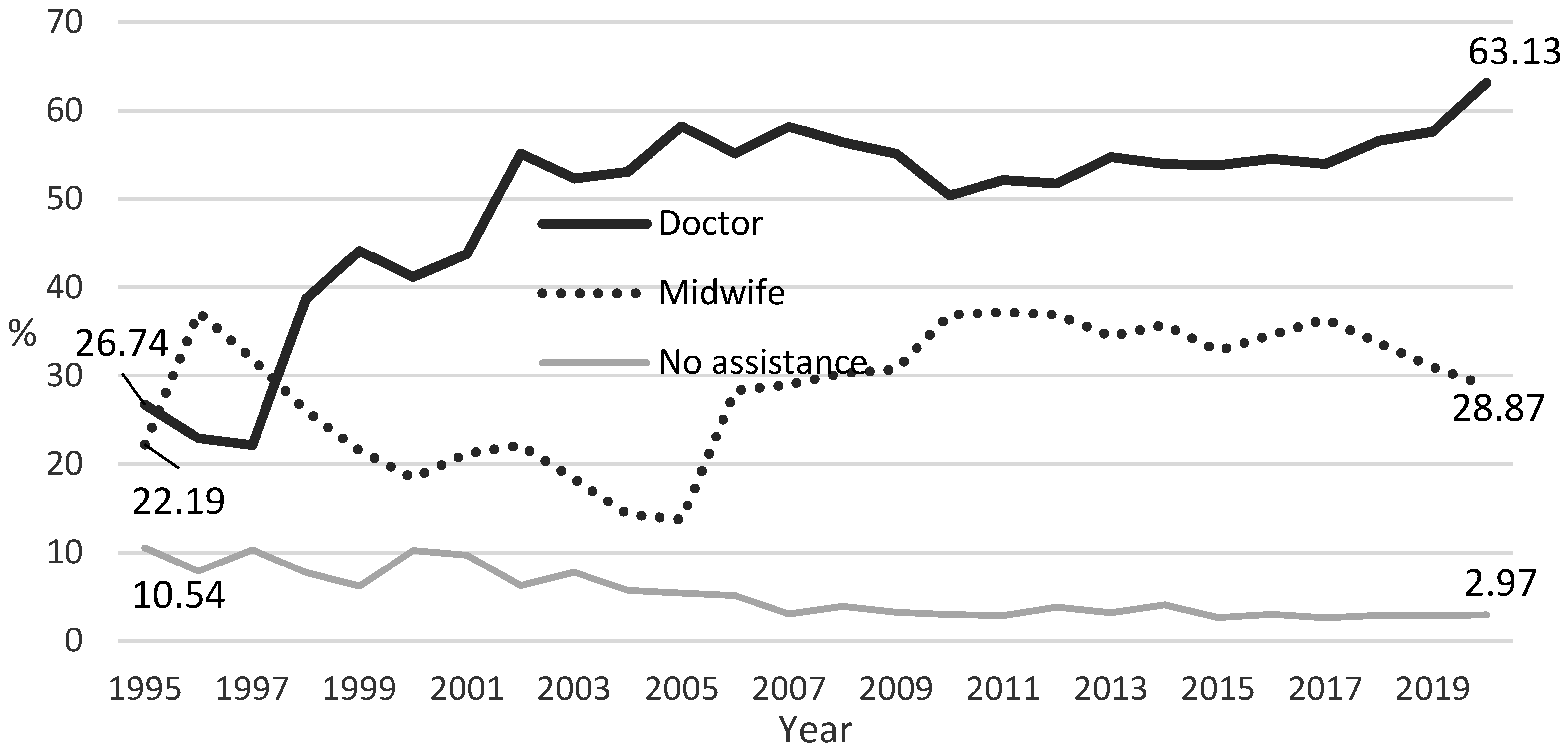
3.2.5. Birth Assistance
3.3. Home and Hospital Births in Portugal in 2020
4. Discussion
4.1. Place of Birth: Characteristics of Mothers, Pregnancy, and Type of Care
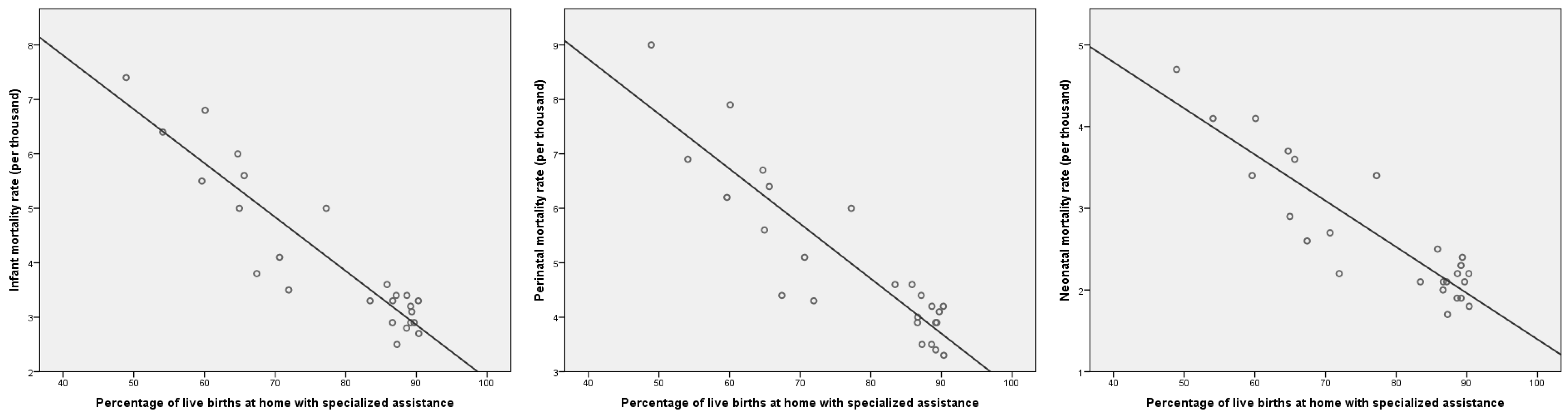
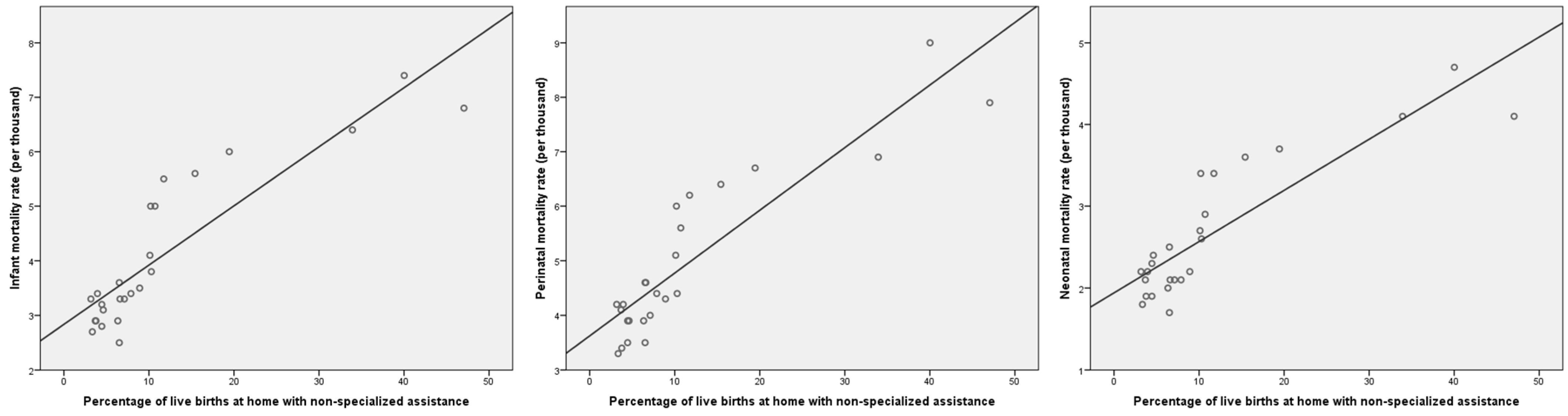
4.2. Home Birth and Health Outcomes
4.3. Home Birth and Maternity Care Systems
4.4. Sources, Availability, and Quality of Data
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baptista, Virginia. 2016. Os partos e as maternidades em Portugal (1889–1943)—Os casos nas cidades de Lisboa, Porto e Coimbra. Revista de História Regional 21: 364–88. [Google Scholar] [CrossRef]
- Barata, Catarina, Dulce M. Neves, and Mário J. D. S. Santos. 2020. COVID-19 Containment Measures, Perinatal Experiences, and the Fight for Childbirth Rights in Portugal. Medical Anthropology Quarterly Rapid Response Blog Series. Available online: https://medanthroquarterly.org/rapid-response/2020/08/covid-19-containment-measures-perinatal-experiences-and-the-fight-for/ (accessed on 19 November 2022).
- Birthplace in England Collaborative Group. 2011. Perinatal and maternal outcomes by planned place of birth for healthy women with low risk pregnancies: The Birthplace in England national prospective cohort study. BMJ 343: d7400. [Google Scholar] [CrossRef] [PubMed]
- Campbell, Kim, George Carson, Hussam Azzam, and Eileen Hutton. 2019. No. 372-Statement on Planned Homebirth. Journal of Obstetrics and Gynaecology Canada 41: 223–27. [Google Scholar] [CrossRef]
- Carneiro, Marinha. 2008. Ajudar a nascer: Parteiras, saberes obstétricos e modelos de formação: Séculos XV-XX. Porto: Universidade do Porto. [Google Scholar]
- Circular nr. 7495/2006 (Defines the Reorganisation of the National Network of Hospitals with Labour and Delivery Wards, Centralising the Public Provision of Childbirth Care in Maternity Units with Larger Volumes of Deliveries). Available online: https://dre.pt/application/conteudo/958060 (accessed on 20 October 2022).
- Cohen, Jacob. 1988. Statistical Power Analysis for the Behavioural Sciences, 2nd ed. Hillsdale: Erlbaum. [Google Scholar]
- Comeau, Amanda, Eileen K. Hutton, Julia Simioni, Ella Anvari, Megan Bowen, Samantha Kruegar, and Elizabeth K. Darling. 2018. Home birth integration into the health care systems of eleven international jurisdictions. Birth 45: 311–21. [Google Scholar] [CrossRef]
- Dahlen, Hannah G., Bashi Kumar-Hazard, and Mary Chiarella. 2020. How COVID-19 Highlights an Ongoing Pandemic of Neglect and Oppression When It Comes to Women’s Reproductive Rights. Journal of Law and Medicine 27: 812–28. [Google Scholar] [PubMed]
- Davis-Floyd, Robbie, Kim Gutschow, and David A. Schwartz. 2020. Pregnancy, Birth and the COVID-19 Pandemic in the United States. Medical Anthropology 39: 413–27. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, Ank, Caroline C. Geerts, Birgit Y. Van Der Goes, Ben W. Mol, Simone E. Buitendijk, and Jan G. Nijhuis. 2015. Perinatal mortality and morbidity up to 28 days after birth among 743 070 low-risk planned home and hospital births: A cohort study based on three merged national perinatal databases. BJOG: An International Journal of Obstetrics and Gynaecology 122: 720–28. [Google Scholar] [CrossRef]
- De Jonge, Ank, Jeanette A. J. M. Mesman, Judith Manniën, Joost J. Zwart, Jeroen Van Dillen, and Jos Van Roosmalen. 2013. Severe adverse maternal outcomes among low risk women with planned home versus hospital births in the Netherlands: Nationwide cohort study. BMJ 346: f3263. [Google Scholar] [CrossRef]
- de Vries, Raymond G., Yasaswi Paruchuri, Kathleen Lorenz, and Saraswathi Vedam. 2013. Moral science: Ethical argument and the production of knowledge about place of birth. The Journal of Clinical Ethics 24: 225–38. [Google Scholar] [CrossRef]
- Fedele, Anna, and Florence P. Guignard. 2018. Pushing from the Margins: “Natural childbirth” in holistic spiritualities and natural parenting in France and Portugal. In Sacred Inception: Reclaiming the Spirituality of Birth in the Modern World. Edited by Marianne Delaporte and Morag Martin. Lanham: Lexington Books, pp. 131–49. [Google Scholar]
- Galková, Gabriela, Pavel Böhm, Zdeněk Hon, Tomáš Heřman, Radan Doubrava, and Leoš Navrátil. 2022. Comparison of Frequency of Home Births in the Member States of the EU Between 2015 and 2019. Global Pediatric Health 9: 1–8. [Google Scholar] [CrossRef]
- Gregory, Elizabeth C. W., Michele J. K. Osterman, and Valenzuela Claudia P. 2021. Changes in Home Births by Race and Hispanic Origin and State of Residence of Mother: United States, 2018–2019 and 2019–2020. In National Vital Statistics Reports; p. 70. Available online: https://www.cdc.gov/nchs/data/nvsr/nvsr70/NVSR70-15.pdf (accessed on 25 November 2022).
- Grünebaum, Amos, Laurence B. McCullough, Brooke Orosz, and Frank A. Chervenak. 2020. Neonatal mortality in the United States is related to location of birth (hospital versus home) rather than the type of birth attendant. American Journal of Obstetrics and Gynecology 223: 254.e1–54.e8. [Google Scholar] [CrossRef] [PubMed]
- Hildingsson, Ingegerd, Ingela Rådestad, and Helena Lindgren. 2010. Birth Preferences that Deviate from the Norm in Sweden: Planned Home Birth versus Planned Cesarean Section. Birth 37: 288–95. [Google Scholar] [CrossRef] [PubMed]
- Hutton, Eileen K., Angela Reitsma, Julia Simioni, Ginny Brunton, and Karyn Kaufman. 2019. Perinatal or neonatal mortality among women who intend at the onset of labour to give birth at home compared to women of low obstetrical risk who intend to give birth in hospital: A systematic review and meta-analyses. EclinicalMedicine 14: 59–70. [Google Scholar] [CrossRef]
- INE. 2022. Área Metropolitana de Lisboa em Números—2020; Lisboa: INE. Available online: https://www.ine.pt/ngt_server/attachfileu.jsp?look_parentBoui=547352935&att_display=n&att_download=y (accessed on 14 September 2022).
- INSERM. 2021. Les morts maternelles en France: Mieux comprendre pour mieux prévenir. 6e rapport de l’Enquête Nationale Confidentielle sur les Morts Maternelles (ENCMM), 2013–2015. Santé publique France. Available online: www.santepubliquefrance.fr (accessed on 12 December 2022).
- Janssen, Patricia A., Lee Saxell, Lesley A. Page, Michael C. Klein, Robert M. Liston, and Shoo K. Lee. 2009. Outcomes of planned home birth with registered midwife versus planned hospital birth with midwife or physician. CMAJ 181: 377–83. [Google Scholar] [CrossRef]
- Law nr. 15/2014 (Consolidates the Legislation in Respect to the Rights and Duties of Health Services Users). Available online: https://data.dre.pt/eli/lei/15/2014/03/21/p/dre/pt/html (accessed on 12 December 2022).
- Loudon, Irvine. 1992. Death in Childbirth: An International Study of Maternal Care and Maternal Mortality 1800–1950. Oxford: Oxford University Press. [Google Scholar]
- MacDorman, Marian F., Fay Menacker, and Eugene Declercq. 2010. Trends and characteristics of home and other out-of-hospital births in the United States, 1990–2006. In National Vital Statistics Reports; 58, pp. 1–14, 16. Available online: https://www.cdc.gov/nchs/data/nvsr/nvsr58/nvsr58_11.pdf (accessed on 17 November 2022).
- Matos, Ana Raquel. 2010. De longe se faz «parto»!—Os movimentos de protesto sobre o encerramento de maternidades em Portugal enquanto modalidade legítima de participação cidadã nas decisões políticas. O Cabo Dos Trabalhos. Available online: https://cabodostrabalhos.ces.uc.pt/n4/ (accessed on 2 December 2022).
- Minkoff, Howard, and Jeffrey Ecker. 2013. A reconsideration of home birth in the United States. The Journal of Clinical Ethics 24: 207–14. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, Catarina R. 2020. Indicadores de integração de imigrantes: Relatório estatístico anual 2020; Lisboa: Observatório das Migrações. Available online: https://www.om.acm.gov.pt/documents/58428/383402/Relatorio+Estatistico+Anual+2020+-+Indicadores+de+Integracao+de+Imigrantes/472e60e5-bfff-40ee-b104-5e364f4d6a63 (accessed on 2 December 2022).
- Olsen, Ole, and Jette Clausen. 2023. Planned hospital birth compared with planned home birth for pregnant women at low risk of complications. Cochrane Database of Systematic Reviews 3: CD000352. [Google Scholar] [CrossRef]
- Pintassilgo, Sónia. 2014. O Risco e as Condições Sociais e Assistenciais da Maternidade em Portugal. Unpublished doctoral thesis, ISCTE-IUL, Lisboa, Portugal. Available online: https://repositorio.iscte-iul.pt/handle/10071/7898 (accessed on 27 November 2022).
- Pintassilgo, Sónia, and Helena Carvalho. 2017. Trends and consequences of the technocratic paradigm of childbirth in Portugal: A population-based analysis of birth conditions and social characteristics of parents. Sexual & Reproductive Healthcare 13: 58–67. [Google Scholar] [CrossRef]
- Pintassilgo, Sónia, Dulce M. Neves, and Mário J. D. S. Santos. 2022. A mortalidade materna em Portugal: O que dizer da sua evolução? The Laboratory for Social Studies on Childbirth (nascer.pt) Blog Series. Available online: https://nascer.pt/2022/05/27/a-mortalidade-materna-em-portugal-o-que-dizer-da-sua-evolucao/ (accessed on 2 December 2022).
- Quattrocchi, Patrizia. 2014. Homebirth and the NHS in Italy. Canadian Journal of Midwifery Research and Practice 13: 32–39. Available online: https://www.cjmrp.com/files/v13n3_quattrochi_homebirthitaly.pdf (accessed on 29 November 2022).
- Reitsma, Angela, Julia Simioni, Ginny Brunton, Karyn Kaufman, and Eileen K. Hutton. 2020. Maternal outcomes and birth interventions among women who begin labour intending to give birth at home compared to women of low obstetrical risk who intend to give birth in hospital: A systematic review and meta-analyses. EClinicalMedicine 21: 100319. [Google Scholar] [CrossRef]
- Rocha, Sónia B. da. 2016. Partos no domicílio—Contributo do enfermeiro especialista em saúde materna e obstetrícia. Sinais Vitais. pp. 15–25. Available online: http://www.sinaisvitais.pt/index.php/revista-sinais-vitais-publicacoes-78/revistas-2015/735-sinais-vitais-121 (accessed on 30 September 2022).
- Romanis, Elizabeth C., and Anna Nelson. 2020. Homebirthing in the United Kingdom during COVID-19. Medical Law International 20: 183–200. [Google Scholar] [CrossRef]
- Santos, Mário J. D. S. 2020. Knowledge, power and new professional dynamics in Portuguese home births. Unpublished doctoral thesis, ISCTE-IUL, Lisboa, Portugal. Available online: http://hdl.handle.net/10071/20580 (accessed on 15 December 2022).
- Santos, Mário, and Amélia Augusto. 2016. “Se estava tudo bem, porque é que eu havia de ir a uma obstetra?”—Identidade, risco e consumo de tecnologia médica no parto domiciliar em Portugal. Sociologia, Problemas e Práticas, 49–67. [Google Scholar] [CrossRef]
- Santos, Mário. 2014. Trajetórias de desintitucionalização do parto. A rejeição da hegemonia biomédica na opção pelo parto em casa. VII Congresso Português de Sociologia. Available online: http://www.aps.pt/viii_congresso/VIII_ACTAS/VIII_COM0021.pdf (accessed on 5 December 2022).
- Santos, Mário. 2017. Where the thread of home births never broke—An interview with Susanne Houd. Women and Birth 30: 159–65. [Google Scholar] [CrossRef]
- Santos, Mário. 2018. Can the unequal access to home birth be framed as a source of inequalities? A comparison between Portugal and Denmark. Portuguese Journal of Social Science 17: 335–47. [Google Scholar] [CrossRef] [PubMed]
- Shaw, Dorothy, Jeanne-Marie Guise, Neel Shah, Kristina Gemzell-Danielsson, K.S. Joseph, Barbara Levy, Fontayne Wong, Susannah Woodd, and Elliot K. Main. 2016. Drivers of maternity care in high-income countries: Can health systems support woman-centred care? The Lancet 388: 2282–95. [Google Scholar] [CrossRef]
- Snowden, Jonhathan M., Ellen L. Tilden, Janice Snyder, Brian Quigley, Aaron B. Caughey, and Yvonne W. Cheng. 2015. Planned Out-of-Hospital Birth and Birth Outcomes. New England Journal of Medicine 373: 2642–53. [Google Scholar] [CrossRef]
- Vallgårda, Signild. 2012. Hospitalization of deliveries: The change of place of birth in Denmark and Sweden from the late nineteenth century to 1970. Medical History 40: 173–96. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Place of Birth | N. | % |
|---|---|---|
| Home | 1112 | 1.3 |
| Hospital | 82,205 | 97.1 |
| Other place | 1374 | 1.6 |
| Total | 84,691 | 100 |
| Dimension | Variable | Category | Place of Birth | ||
|---|---|---|---|---|---|
| Home | Hospital | Other Place | |||
| Mothers | Mother’s educational level | Until primary | 7 | 6.8 | 2.1 |
| Lower secondary | 16.3 | 15.1 | 4.7 | ||
| Upper secondary | 31.9 | 33.7 | 8.4 | ||
| Tertiary | 36.2 | 37.3 | 6.8 | ||
| Unknown | 8.6 | 7 | 77.9 | ||
| Nationality | Portuguese | 84.1 | 86.4 | 94 | |
| Other | 15.9 | 13.6 | 6 | ||
| Pregnancy | Length of pregnancy (in weeks) | Until 35 | 3.5 | 3.9 | 1.3 |
| 36 | 3.2 | 2.8 | 0.5 | ||
| 37 | 6.7 | 7.3 | 1.5 | ||
| 38 | 17.8 | 18.2 | 3.6 | ||
| 39 | 34 | 33.3 | 8.6 | ||
| 40 | 25.8 | 25.1 | 6 | ||
| 41 | 7.9 | 8.7 | 1.5 | ||
| 42 or more | 0.4 | 0.2 | 0.1 | ||
| Unknown | 0.8 | 0.3 | 76.9 | ||
| Parity | 1 | 50.7 | 53.6 | 87.6 | |
| 2 | 33.5 | 33.4 | 9 | ||
| 3 | 11.1 | 9.6 | 2.8 | ||
| 4 or more | 4.7 | 3.3 | 0.7 | ||
| Assistance | Care provider | Doctor | 63.1 | 75.4 | 15.9 |
| Midwife | 28.9 | 24.2 | 4.9 | ||
| Nurse | 1.3 | 0.3 | 0.5 | ||
| Other | 3.4 | 0 | 1.2 | ||
| No care provider | 3 | 0 | 0.4 | ||
| Ignored | 0.4 | 0 | 77.1 | ||
| Mother’s Continent (Nationality) | Place of Birth | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Home | Hospital | |||||||||
| Countries (N.) | Countries (%) | Live Births (N.) | Live Births (%) | Most Represented Country | Countries (N.) | Countries (%) | Live Births (N.) | Live Births (%) | Most Represented Country | |
| Africa | 9 | 22.5 | 28 | 15.8 | Cape Verde | 40 | 28.4 | 3065 | 27.4 | Angola |
| America | 5 | 12.5 | 67 | 37.9 | Brazil | 44 | 31.2 | 4558 | 40.8 | Brazil |
| Asia | 6 | 15.0 | 15 | 8.5 | Nepal | 28 | 19.9 | 1701 | 15.2 | Nepal |
| Europe | 20 | 50.0 | 67 | 37.9 | Germany | 27 | 19.1 | 1848 | 16.5 | Ukraine |
| Oceania | 0 | 0.0 | 0 | 0.0 | 2 | 1.4 | 3 | 0.03 | N. Zealand | |
| Total | 40 | 100 | 177 | 100 | 141 | 100 | 11,175 | 100 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pintassilgo, S.; Santos, M.J.D.S.; Trindade, I.; Neves, D.M. Home Birth in Portugal—A Comprehensive Analysis Based on Official Statistical Data. Soc. Sci. 2023, 12, 314. https://doi.org/10.3390/socsci12060314
Pintassilgo S, Santos MJDS, Trindade I, Neves DM. Home Birth in Portugal—A Comprehensive Analysis Based on Official Statistical Data. Social Sciences. 2023; 12(6):314. https://doi.org/10.3390/socsci12060314
Chicago/Turabian StylePintassilgo, Sónia, Mário J. D. S. Santos, Inês Trindade, and Dulce Morgado Neves. 2023. "Home Birth in Portugal—A Comprehensive Analysis Based on Official Statistical Data" Social Sciences 12, no. 6: 314. https://doi.org/10.3390/socsci12060314
APA StylePintassilgo, S., Santos, M. J. D. S., Trindade, I., & Neves, D. M. (2023). Home Birth in Portugal—A Comprehensive Analysis Based on Official Statistical Data. Social Sciences, 12(6), 314. https://doi.org/10.3390/socsci12060314