
The Effectiveness of Healthy Community Approaches on Positive Health Outcomes in Canada and the United States


Abstract
:
1. Introduction

{kind=link}
{kind=link}
| Healthy Community Approaches | Target Population | Description |
|---|---|---|
| Healthy Cities | Whole populations | World Health Organization (WHO) initiative established in 1986 that seeks to protect health and support sustainable development. The basic features are community participation and empowerment, intersectoral collaboration, equity and action to address the social determinants of health [5]. |
| Child Friendly Cities | Children | Launched in 1996, this global movement supported by United Nations Children’s Fund (UNICEF) promotes children’s rights to the highest quality of life. The nine elements include children’s participation in issues that involve them, child friendly legal framework, children’s rights strategy, child rights unit, child impact assessment, budget to support children’s activities, children’s national report, advocacy for children’s rights and children’s ombudsman or commissioner [6]. |
| Smart Growth Planning | Whole populations | An approach, first launched in 1995, to land use planning and development that supports health, economic growth and prioritizes conservation. The ten fundamental principles include: mixed land use, promoting compact building design, providing a range of housing options, fostering attractive communities with a strong sense of place, preservation of open spaces, development of existing communities, variety of transportation choices, encouraging fair and cost effective development and supporting community collaboration in development [7]. |
| Safe Routes to School | Children in school settings | The US national program that uses multiple modalities including education, engineering improvements, enforcement and encouragement to increase student active travel [8]. Although activities occurred as early as 1997 in the US, the National Program Safe Routes to School Program was established by federal legislation in 2005. |
| Safe Communities | Whole populations | A global initiative supported by WHO that engages communities to promote safety and injury prevention. Multiple global networks have been established and provide accreditation to committed communities who satisfy the designated criteria [9]. The concept was introduced as a policy initiative in Sweden in 1989. |
| Active Living Communities | Whole populations in selected communities | A movement that is dedicated to increasing opportunities for population physical activity. Some projects may include other components such as Safe Routes to School or Smart Growth [10]. Active Living by Design (ALbD) was at the forefront of the movement and was launched in 2002. |
| Livable Communities | Whole populations | Livable communities embody multiple factors that contribute to good quality of life such as recreational and educational opportunities, attractive built and natural environment, social stability and economic prosperity [11]. Programs have been implemented by various partners for more than 25 years. |
| Social Cities | Whole Populations | A social city fosters social connectedness of its residents and improves the social architecture to strengthen these relationships [12]. The concept has been growing in popularity since 2009. |
| Age-Friendly Cities | Elderly population | Global Initiative that promotes active aging of older residents and increases opportunities for their social participation and security. The movement builds on the 2002 Policy Framework for Active Aging and considers key domains of the social and physical environment that need to be optimized to enhance the quality of life of older persons. These include the outdoor spaces and buildings, transportation, housing, social participation, respect and social inclusion, civic participation and employment, communication and information, community support and health [13]. |
| Dementia Friendly Cities | Persons living with dementia and their care givers | This initiative is supported by the Alzheimer’s Society and seeks to improve inclusion and quality of life of people living with dementia [14]. It has been gaining momentum especially in the United Kingdom since 2012. |
2. Methods
2.1. Data Sources and Search Strategy
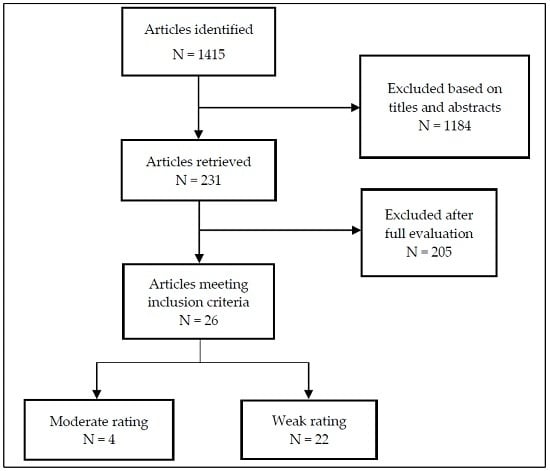
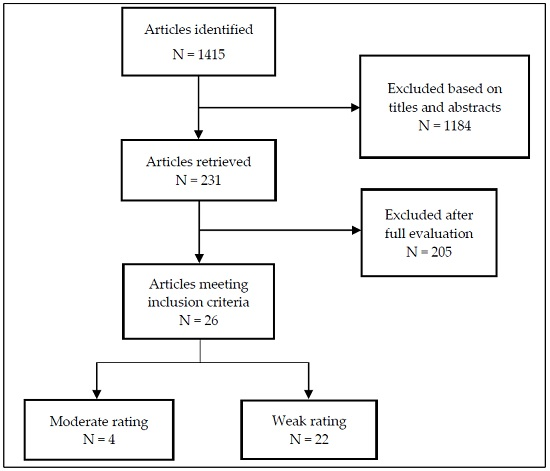
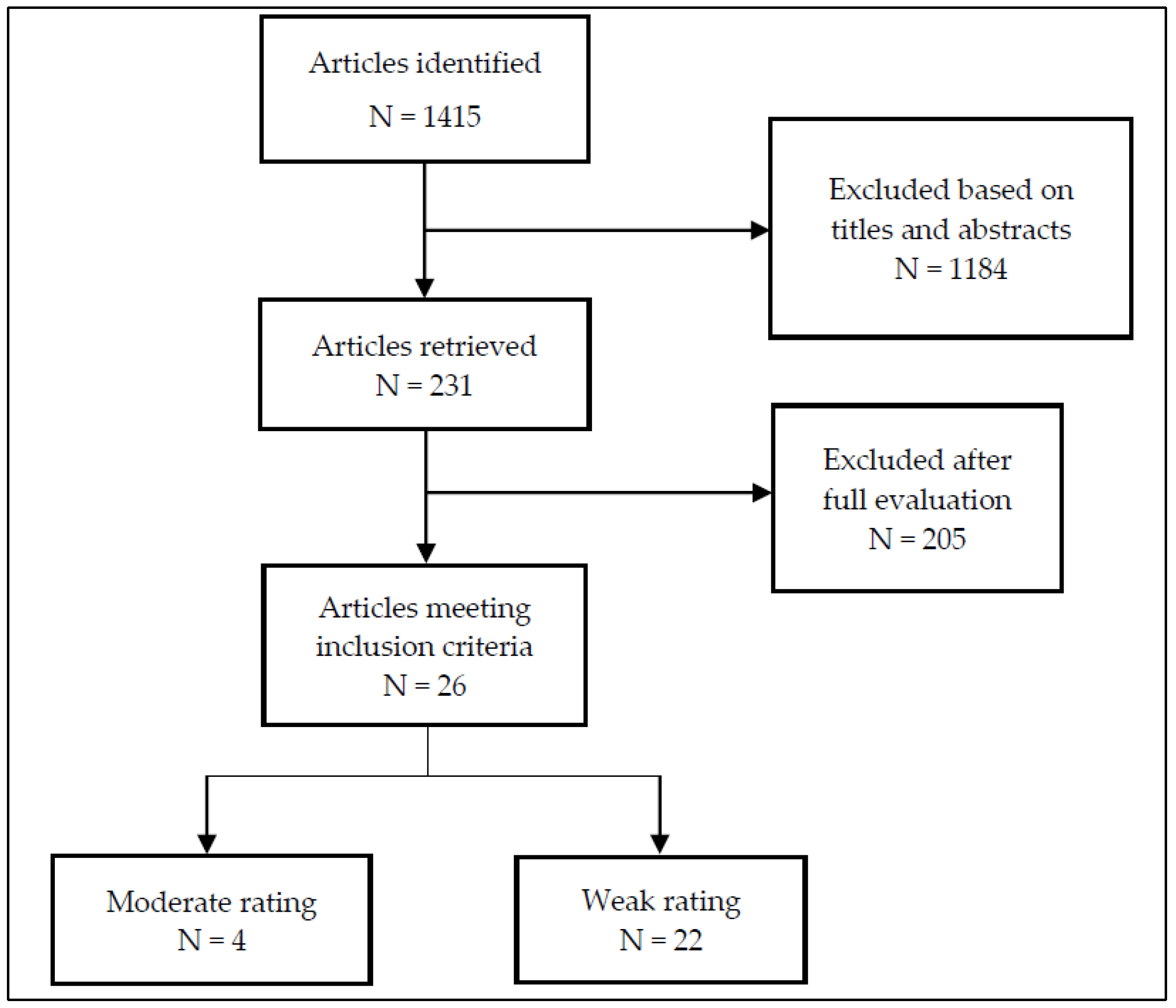
2.2. Selection and Review Process
3. Results and Discussion

3.1. Safe Routes to School
| Author/Date | Selection bias | Study design | Confounders | Blinding | Data collection methods | Withdrawals/drop outs | Global rating | ||
|---|---|---|---|---|---|---|---|---|---|
| Safe Routes to School | |||||||||
| Mendoza et al., 2009 [21] | Moderate | Moderate | Weak | N/A | Strong | Moderate | Moderate | ||
| Mendoza et al., 2011 [22] | Weak | Moderate | Weak | Moderate | Strong | Weak | Weak | ||
| Boarnet et al., 2005 [23] | Weak | Weak | Weak | Moderate | Weak | Moderate | Weak | ||
| Cooper et al., 2010 [24] | Weak | Moderate | Weak | Moderate | Strong | Weak | Weak | ||
| Buliung et al., 2011 [25] | Weak | Weak | Weak | Moderate | Weak | Weak | Weak | ||
| Mammen et al., 2014 [26] | Weak | Moderate | Moderate | N/A | Strong | Weak | Weak | ||
| Henderson et al.2013 [27] | Weak | Moderate | Weak | Moderate | Weak | Weak | Weak | ||
| McDonald et al., 2013 [28] | Weak | Moderate | Moderate | Moderate | Strong | Weak | Weak | ||
| McDonald et al., 2014 [29] | Weak | Weak | Strong | Moderate | Strong | Moderate | Weak | ||
| McDonald et al., 2013 [28] | Weak | Moderate | Moderate | Moderate | Strong | Weak | Weak | ||
| Moudon et al., 2012 [30] | Weak | Weak | Moderate | N/A | Weak | Strong | Weak | ||
| Staunton et al., 2003 [31] | Weak | Weak | Weak | N/A | Moderate | Weak | Weak | ||
| Buckley et al., 2013 [32] | Weak | Moderate | Weak | Moderate | Weak | Weak | Weak | ||
| Johnson et al., 2006 [33] | Weak | Moderate | Weak | Weak | Moderate | Weak | Weak | ||
| Sayers et al., 2012 [34] | Weak | Weak | Strong | Weak | Moderate | Weak | Weak | ||
| Di Maggio et al., 2013 [35] | Moderate | Moderate | Weak | Moderate | Moderate | Moderate | Moderate | ||
| Blomberg et al.,2008 [36] | Moderate | Weak | Weak | Moderate | Weak | Moderate | Weak | ||
| Orenstein et al., 2007 [37] | Moderate | Weak | Weak | N/A | Weak | Moderate | Weak | ||
| Ragland et al., 2014 [38] | Weak | Weak | Weak | Moderate | Strong | Weak | Weak | ||
| Mendoza et al., 2012 [39] | Weak | Strong | Moderate | Moderate | Strong | Weak | Weak | ||
| Active living communities | |||||||||
| Chomitz et al., 2012 [40] | Moderate | Moderate | Strong | Weak | Strong | Moderate | Moderate | ||
| TenBrink et al., 2009 [41] | Weak | Weak | Weak | Weak | Weak | Weak | Weak | ||
| Sayers et al., 2012 [42] | Weak | Weak | Weak | Weak | Moderate | Moderate | Weak | ||
| Safe communities | |||||||||
| Istre et al., 2011 [43] | Weak | Moderate | Weak | Weak | Weak | Moderate | Weak | ||
| Smart growth planning | |||||||||
| Dunton et al., 2011 [44] | Weak | Moderate | Weak | Moderate | Moderate | Strong | Weak | ||
| Age-friendly cities | |||||||||
| Lehning et al., 2012 [45] | Strong | Weak | Strong | Weak | Strong | Moderate | Weak | ||
| Menec and Nowicki, 2014 [46] | Weak | Weak | Strong | Weak | Moderate | Moderate | Weak | ||
| Study | Outcomes |
|---|---|
| Safe Routes to School | |
Mendoza et al., 2009 [21]
| The proportion of children who walked to intervention (20% ± 2%) and control schools (15% ± 2%) was similar at baseline. At 12 month follow up, a higher proportion of children walked to intervention schools (25% ± 2%) compared to control schools (7% ± 1%, p = 0.001). |
Mendoza et al., 2011 [22]
| Weekly percent active commuting increased in the intervention group, while a decrease was observed in the control group (p < 0.0001). Acculturation and parent outcome expectations were associated with a change in percent active commuting. In multivariable models predicting minutes of moderate to vigorous physical activity, children in the intervention group increased their minutes while a decline was observed in the participants in the control group (p = 0.029). |
Boarnet et al., 2005 [23]
| Among children who passed the project on the way to school, a greater proportion (15.4%) walked or bicycled more after the construction projects when compared to children who did not (4.3%) encounter the projects on the way to school (p < 0.01). |
Cooper et al., 2010 [24]
| Parental surveys reported modest increases in children walking to (29%) and from (26%) school over baseline. However student tallies showed marked variation with smaller increases (1 to 5%) in schools with paid coordinators and only one of the other six schools showed a clear increase (7% to 14%) in walking. In general, schools with paid coordinators had 50% more students walking in the morning and 45% in the afternoon than schools with volunteers. |
Buliung et al., 2011 [25]
| Small increases occurred in rates of active transportation from 43.5% (baseline) to 45.9% (follow up). Higher rates (43.5%) of active travel occurred at afternoons compared to mornings (37.3%). Among household respondents, 13.3% indicated that the intervention “resulted in less driving”. |
Mammen et al., 2014 [26]
| There was no increase over baseline in rates of active travel either in morning or afternoon after one year. Marked variation occurred in AST at the school level. The season of data collection predicted a decrease in AST in the morning (p < 0.05). |
Henderson et al., 2013 [27]
| There was an increase in the rates of walking to school in the morning (p < 0.0001) during the intervention period however no significant change was observed for the afternoon commute. Parental perception about school support for active modes of transport and the health benefits (0.01 < p < 0.001) and enjoyment associated with active modes of transportation (p < 0.0001) also improved. |
McDonald et al., 2013 [28]
| Regression models were used to estimate the marginal effects associated with walking or biking to school among the study population. Schools with more types of interventions had larger proportions of students who walked or biked to school. Programs that delivered education and encouragement components in addition to two other SRTS interventions were associated with a 20 percentage point increase in walking and a small but non-significant increase in biking. Infrastructure improvement interventions had borderline significance which might have been related to late completion of these components in the program cycle. Provision of covered bike parking was associated with large increases in walking (19 percentage points) and biking (11 percentage points). The Boltage intervention produced small increases in walking (5 percentage points) and biking (4 percentage points). |
McDonald et al., 2014 [29]
| Fractional logit models were used to estimate the marginal effects of the presence and number of years of SRTS interventions on walking and bicycling. Rates of active travel increased with each year of participation in SRTS programs. After five years, there was an absolute increase of 13 percentage points in the proportion of children who walked or biked. In multivariable models after adjustment for school and environmental characteristics, walking and bicycling rose by 1.1 percentage points for each year of participation in SRTS programs. The presence of an engineering component was associated with 3.3 percentage point increase in walking and bicycling. This was unrelated to the length of time that the improvement was in place. Smaller increases (0.9 percentage points) were associated with education and encouragement interventions. |
Moudon et al., 2012 [30]
| There was a statistically significant increase in rates of active transport for all modes of transport in all states except for biking in Florida. Rates of walking increased more than cycling. Changes in rates of active transport were not correlated with any project, school or neighborhood characteristics. |
Staunton et al., 2003 [31]
| There were marked increases in walking (64%), biking (114%) and carpooling (39% decrease in children arriving by car) over the two year period. |
Buckley et al. 2013 [32]
| The number of children who walked to school increased by 25% (19%–26%). During the same period, there was a decrease in the proportion of children walking to school at comparison sites. Direct observations of children at school crossings showed small improvements in street crossing safety over baseline however key desirable behaviors were present in less than 50% of all observed crossings. |
Johnson et al., 2006 [33]
| The number of children who walked to school increased by 25% (19%–26%). During the same period, there was a decrease in the proportion of children walking to school at comparison sites. Direct observations of children at school crossings showed small improvements in street crossing safety over baseline however key desirable behaviors were present in less than 50% of all observed crossings. |
Sayers et al., 2012 [34]
| There was no difference between the groups in physical activity levels (p = 0.17). The percentage of time spent in moderate to vigorous physical activity (MVPA) during the study was 38 (20.9 ± 6.9) for WSB participants and 39 (23.4 ± 8) in comparison group. In multivariable models, age was negatively associated with percentage of time spent in moderate to vigorous physical activity (r = −0.79, p < 0.001). |
Di Maggio and Li 2013 [35]
| Annual pedestrian injuries declined over time however the most pronounced reduction (33% 95% CI 30–36) was observed among school aged children (5–19 years) compared to 14% (95% CI 12–16) among other age groups. Pedestrian injury rates among school aged children in census tracts with SRTS interventions decreased between the pre-intervention and post intervention periods as well as during school travel hours (8 to 4.4 injuries per 10,000 persons). These observations were not apparent in census tracts without SRTS interventions. |
Blomberg et al. 2008 [36]
| There was a general decline in pedestrian and bicycling collison sover time. Marked reductions occurred for children 4 to 12 yeats served by SRTS focus sites when compared to state wide collisons, although the differences were not statistically significant. |
Orenstein et al., 2007 [37]
| The authors compared the change in injuries involving school aged children (5 to 18 years) pre and post SRTS construction projects for intervention and control sites in California. There was a general decline in the number of injuries between 1998 and 2005 with a similar percentage reduction in the annual number of injuries for both SRTS (13%) and non SRTS sites (15%). However when the changes in mobility patterns were accounted for, it was estimated that safety benefits ranged from no net change to a decrease of 49% in collisions among students at SRTS sites. |
Ragland et al., 2014 [38]
| In pedestrians ages 8 to 18 years there was a 50% reduction in collisions in the treatment area (within 250 feet of the countermeasure buffer zones). Although effect not statistically significant. Among pedestrians of all ages, there was a statistically significant 75% reduction of collisions in the treated areas compared to control areas. In the mobility analysis, living within 250 feet of the SRTS project improvement was associated with an increased probability of walking to school. |
Mendoza et al., 2012 [39]
| Compared to children at control schools, children at intervention schools has five times higher odds of crossing at crosswalk or corner (95% CI 2.79–8.99, p < 0.01) however also had five fold lower odds of stopping at the curb 95% CI 0.15–0.31, p < 0.01). Parent perception of neighborhood safety and number of traffic lanes were not associated with pedestrian safety outcomes in mixed models (p > 0.05). |
| Active Living Communities | |
Chomitz et al., 2012 [40]
| Adults in the intervention city were more likely than those in the comparison city to report meeting recommended physical activity guidelines (OR = 1.10, 95% CI 1.04–1.17). No differences were found in meeting the recommended physical activity guidelines among of children in both cities in adjusted analyses [middle school OR 1.06 (95% CI 0.78–1.45); high school OR 1.24 95% CI 0.98–1.58). |
TenBrink et al., 2009 [41]
| The number of students who walked to school (5%–15% increase) and participation in sentinel events such as Walk to School Day and Smart Commute Day increased during the project. Participation in Smart Commute Day increased from 165 (2004) to 520 persons (2008). Walk to school day participants increased from 600 in 2003 to 1200 in 2008. |
Sayers et al., 2012 [42]
| Pedestrian and cyclists counts increased from 2007 to 2009 particularly in the latter part (July and October) of 2009. Repeated measures ANOVA showed a statistically significant effect of year (p = 0.01), season (p < 0.001) and interaction of year and season (p = 0.05). Survey data indicated increased awareness of ALbD programming through media and advertisements in 2008 compared to 2003 (63% of respondents, N = 813). |
| Safe Communities | |
Istre et al., 2011 [43]
| In multivariable analyses, child restraint use (OR = 1.6 95% CI 1.2–2.2), drivers who were wearing a seatbelt (OR = 2.2 95% CI 1.5–3.2) and children riding in the back seat (OR = 1.3 95% CI 1.0–1.6) increased significantly over baseline for target communities compared to communities that did not receive the intervention. |
| Smart Growth Planning | |
Dunton et al., 2012 [44]
| Children in smart growth communities engaged in a greater proportion of physical activity bouts a few blocks from home (p < 0.001) and travelled more by walking (p < 0.011) than children in control communities. Over time, social context of physical activity did not change for either group however children in smart growth communities were more likely to report decreased physical activity indoors and an increase in outdoor locations with no traffic (p = 0.036). There was a greater increase in six month daily moderate to vigorous physical activity among children in intervention communities however it was not statistically significant (p = 0.10). |
| Age-Friendly Cities | |
Lehning et al., 2012 [45]
| In adjusted multivariable analyses, significant predictors of better self-rated health included access to health care (p < 0.01), social support (p < 0.01) and community engagement (p < 0.01) while neighborhood problems were associated with poorer self-rated health (p < 0.01). Addition of age-friendly environment characteristics weakened the association between self-rated health and three health measures (two functional limitations and chronic conditions) although still significant p < 0.001). Education and income variables were no longer significant when age-friendly characteristics were included in the model. |
Menec and Nowicki, 2014 [46]
| Higher Age-Friendly ratings were associated with greater life satisfaction (p < 0.0001) and self-perceived health (<0.01). In multivariable analyses among seniors, the Age-Friendly Index as well as five of the seven domains was associated with life satisfaction. Community support and health services were not associated with any health outcomes. Self-perceived health was associated with fewer age-friendly domains including physical environment, housing, social environment and transportation options. These results differed for younger respondents as age friendliness was not associated with self-perceived health and life satisfaction was only associated with health services/community support and opportunities for participation (p < 0.05). |
3.2. Active Living Communities
3.3. Age-Friendly Cities
3.4. Safe Communities
3.5. Smart Growth Planning
3.6. Other Healthy Community Approaches
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ASRTS | Active and Safe Routes to School; |
| ALbD | Active Living by Design; |
| CDC | Centers for Disease Control; |
| EPPHP | Effective Public Health Practice Project; |
| NTL | National Transportation Library; |
| SAFETEA-LU | Safe Accountable Flexible Efficient Transportation Equity Act: A Legacy for Users; |
| STP | School Travel Planning; |
| SRTS | Safe Routes to School; |
| UNICEF | United Nations Children Fund; |
| WHO | World Health Organization; |
| WSB | Walking School Bus. |
Appendix: Search Strategy for Safe Routes to School
Medline OVID SP (2000 – 2014)
| SCOPUS (Limits to English, 2000 – 2014)
|
References and Notes
- Commission on Social Determinants of Health (CSDH). Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. Final Report of the Commission on Social Determinants of Health. Geneva: World Health Organization, 2008, Available online: http://www.who.int/social_determinants/thecommission/finalreport/en/ (accessed on 10 October 2014).
- Timothy Evans, Margaret Whitehead, Finn Diderichsen, Abbas Bhuiya, and Meg Wirth. Challenging Inequities in Health Care: From Ethics to Action. New York: Oxford University Press, 2001, pp. 309–22. [Google Scholar]
- Trevor Hancock. “Act Locally: Community-Based Population Health Promotion.” Available online: http://www.parl.gc.ca/Content/SEN/Committee/402/popu/rep/appendixBjun09-e.pdf (accessed on 7 August 2015).
- National Research Council and Institute of Medicine. U.S. Health in International Perspective: Shorter Lives, Poorer Health. Panel on Understanding Cross-National Health Differences among High-Income Countries. Edited by Steven H. Woolf and Aron Laudan. Washington: The National Academies Press, 2013. [Google Scholar]
- Tyler Norris, and Mary Pittman. “The healthy communities movement and the coalition for healthier cities and communities.” Public Health Reports 115 (2000): 118. [Google Scholar] [CrossRef] [PubMed]
- UNICEF Innocenti Research Centre. “Building Child Friendly Cities: A framework for action.” Available online: http://childfriendlycities.org/wp_content/uploads/2013/04/pdf/BuildingCFC_AFrameworkforaction_en.pdf (accessed on 9 September 2015).
- Smart Growth Online. “What is smart growth? ” Available online: http://www.smartgrowth.org/what-is-smart-growth/ (accessed on 9 September 2015).
- “National Center for Safe Routes to School.” Available online: http://saferoutesinfo.org/about-us/history-srts (accessed on 9 September 2015).
- “WHO Collaborating Centre on Community Safety Promotion.” Available online: http://isccc.global/how-to-become-an-international-safe-community (accessed on 25 December 2015).
- “Active Living Research.” Available online: http://activelivingresearch.org/active-living-topics (accessed on 9 September 2015).
- Elizabeth E. Fischer. “Building livable communities for the 21st century.” Public Roads 63 (2000): 30–34. [Google Scholar]
- Cardus. “About the Social Cities Research Program.” Available online: http://www.cardus.ca/research/socialcities/ (accessed on 9 September 2015).
- World Health Organization. “Global Age Friendly Cities: A Guide.” Available online: http://apps.who.int/iris/bitstream/10665/43755/1/9/8921 (accessed on 9 September 2015).
- Alzheimer’s Society. “Dementia Friendly Communities.” Available online: http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=1843 (accessed on 10 September 2015).
- Noreen C. McDonald, Pamela H. Barth, and Ruth L. Steiner. “Assessing the Distribution of Safe Routes to School Program Funds, 2005–2012.” American Journal of Preventive Medicine 45 (2013): 401–6. [Google Scholar] [CrossRef] [PubMed]
- Angie L. Cradock, Billy Fields, Jessica L. Barrett, and Steven Melly. “Program practices and demographic factors associated with federal funding for the Safe Routes to School program in the United States.” Health & Place 18 (2012): 16–23. [Google Scholar] [CrossRef] [PubMed]
- Philip Bors, Mark Dessauer, Rich Bell, Risa Wilkerson, Joanne Lee, and Sarah L. Strunk. “The Active Living by Design national program: Community initiatives and lessons learned.” American Journal of Preventive Medicine 37 (2009): S313–21. [Google Scholar] [CrossRef] [PubMed]
- Lynn Weigand. “A review of literature: The effectiveness of Safe Routes to School and other programs to promote active transportation to school.” Available online: https://www.pdx.edu/ibpi/sites/www.pdx.edu.ibpi/files/Safe%20Routes%20White%20Paper.pdf (accessed on 25 August 2015).
- Anneliese Spinks, Cathy Turner, Jim Nixon, and Roderick J. McClure. “The WHO Safe Communities model for the prevention of injury in whole populations.” Cochrane Database of Systematic Reviews 3 (2009): CD004445. [Google Scholar] [PubMed]
- Effective Public Health Practice Project. “Quality Assessment Tool for Quantitative Studies.” Available online: http:///www.ephpp.ca/Tools.html (accessed on 7 August 2015).
- Jason A. Mendoza, David D. Levinger, and Brian D. Johnston. “Pilot evaluation of a walking school bus program in a low-income, urban community.” BMC Public Health 9 (2009): 122. [Google Scholar] [CrossRef] [PubMed]
- Jason A. Mendoza, Kathy Watson, Tom Baranowski, Theresa A. Nicklas, Doris K. Uscanga, and Marcus J. Hanfling. “The walking school bus and children’s physical activity: A pilot cluster randomized controlled trial.” Pediatrics 128 (2011): e537–44. [Google Scholar] [CrossRef] [PubMed]
- Marlon G. Boarnet, Craig L. Anderson, Kristen Day, Tracy McMillan, and Mariela Alfonzo. “Evaluation of the California Safe Routes to School legislation: Urban form changes and children’s active transportation to school.” American Journal of Preventive Medicine 28 (2005): 134–40. [Google Scholar] [CrossRef] [PubMed]
- Jill F. Cooper, and Tracy E. McMillan. “Safe Routes to School Local School Project: A health evaluation at 10 low income schools.” Available online: http://saferoutespartnership.org/sites/default/files/pdf/Health_Evaluation_Feb_2010.pdf (accessed on 8 August 2015).
- Ron Buliung, Guy Faulkner, Theresa Beesley, and Jacky Kennedy. “School travel planning: Mobilizing school and community resources to encourage active school transportation.” Journal of School Health 81 (2011): 704–12. [Google Scholar] [CrossRef] [PubMed]
- George Mammen, Michelle R. Stone, Guy Faulkner, Subha Ramanathan, Ron Buliung, Catherine O’Brien, and Jacky Kennedy. “Active school travel: An evaluation of the Canadian school travel planning intervention.” Preventive Medicine 60 (2014): 55–59. [Google Scholar] [CrossRef] [PubMed]
- Susan Henderson, Robin Tanner, Norma Klanderman, Abby Mattera, Lindsey Martin Webb, and John Steward. “Safe Routes to School: A public health practice success story—Atlanta, 2008–2010.” Journal of Physical Activity and Health 10 (2013): 141–42. [Google Scholar] [PubMed]
- Noreen C. McDonald, Yizhao Yang, Steve M. Abbott, and Allison N. Bullock. “Impact of the Safe Routes to School program on walking and biking: Eugene, Oregon study.” Transport Policy 29 (2013): 243–48. [Google Scholar] [CrossRef]
- Noreen C. McDonald, Ruth L. Steiner, Chanam Lee, Tori Rhoulac Smith, Xuemei Zhu, and Yizhao Yang. “Impact of the safe routes to school program on walking and bicycling.” Journal of the American Planning Association 80 (2014): 153–67. [Google Scholar] [CrossRef]
- Anne Vernez Moudon, and Orion Stewart. “Moving forward: Safe Routes to School progress in five states. ” Available online: http://www.wsdot.wa.gov/research/reports/fullreports/743.3.pdf (accessed on 8 August 2015).
- Catherine E. Staunton, Deb Hubsmith, and Wendi Kallins. “Promoting safe walking and biking to school: The Marin County success story.” American Journal of Public Health 93 (2003): 1431–34. [Google Scholar] [CrossRef] [PubMed]
- Aaron Buckley, Michael B. Lowry, Helen Brown, and Benjamin Barton. “Evaluating safe routes to school events that designate days for walking and bicycling.” Transport Policy 30 (2013): 294–300. [Google Scholar] [CrossRef]
- Brian D. Johnston, Jason Mendoza, Sarah Rafton, Denise Gonzalez-Walker, and David Levinger. “Promoting physical activity and reducing child pedestrian risk: Early evaluation of a walking school bus program in central Seattle.” Journal of Trauma and Acute Care Surgery 60 (2006): 1388–89. [Google Scholar] [CrossRef]
- Stephen P. Sayers, Joseph W. LeMaster, Ian M. Thomas, Gregory F. Petroski, and Bin Ge. “A Walking School Bus program: Impact on physical activity in elementary school children in Columbia, Missouri.” American Journal of Preventive Medicine 43 (2012): S384–89. [Google Scholar] [CrossRef] [PubMed]
- Charles DiMaggio, and Guohua Li. “Effectiveness of a safe routes to school program in preventing school-aged pedestrian injury.” Pediatrics 131 (2013): 290–96. [Google Scholar] [CrossRef] [PubMed]
- Richard D. Blomberg, Arlene M. Cleven, F. Dennis Thomas III, and Raymond C. Peck. Evaluation of the Safety Benefits of Legacy Safe Routes to School Programs; Washington: National Highway Traffic Safety Administration, 2008. Available online: http://www.nhtsa.gov/DOT/NHTSA/Communication%20.../tt368.pdf (accessed on 8 August 2015).
- Marla R. Orenstein, Nicolas Gutierrez, Thomas M. Rice, Jill F. Cooper, and David R. Ragland. Safe Routes to School Safety and Mobility Analysis; Berkley: UC Berkley Traffic Safety Center, 2007. Available online: http://www.dot.ca.gov/hq/LocalPrograms/saferoutes/documents/SR2S+Final_Report_to_the_Legislature.pdf (accessed on 9 August 2015).
- David R. Ragland, Swati Pande, John Bigham, and Jill F. Cooper. “Ten years later: Examining the long term impact of the California Safe Routes to School Program.” In Paper presented at the Transportation Research Board 93rd Annual Meeting, Washington, DC, USA, 12–16 January 2014; Available online: http://doc.trb.org/prp/14-4226.pdf (accessed on 25 December 2015).
- Jason A. Mendoza, Kathy Watson, Tzu-An Chen, Tom Baranowski, Theresa A. Nicklas, Doris K. Uscanga, and Marcus J. Hanfling. “Impact of a pilot walking school bus intervention on children’s pedestrian safety behaviors: A pilot study.” Health & Place 18 (2012): 24–30. [Google Scholar] [CrossRef] [PubMed]
- Virginia R. Chomitz, Julia C. McDonald, Denise B. Aske, Lisa N. Arsenault, Nicole A. Rioles, Lisa B. Brukilacchio, Karen A. Hacker, and Howard J. Cabral. “Evaluation results from an active living intervention in Somerville, Massachusetts.” American Journal of Preventive Medicine 43 (2012): S367–78. [Google Scholar] [CrossRef] [PubMed]
- David S. TenBrink, Randall McMunn, and Sarah Panken. “Project U-Turn: Increasing active transportation in Jackson, Michigan.” American Journal of Preventive Medicine 37 (2009): S329–35. [Google Scholar] [CrossRef] [PubMed]
- Stephen P. Sayers, Joseph W. LeMaster, Ian M. Thomas, Gregory F. Petroski, and Bin Ge. “Bike, Walk, and Wheel: A way of life in Columbia, Missouri, revisited.” American Journal of Preventive Medicine 43 (2012): S379–83. [Google Scholar] [CrossRef] [PubMed]
- Gregory R. Istre, Martha Stowe, Mary A. McCoy, Billy J. Moore, Dan Culica, Katie N. Womack, and Ron J. Anderson. “A controlled evaluation of the WHO Safe Communities model approach to injury prevention: Increasing child restraint use in motor vehicles.” Injury Prevention 17 (2011): 3–8. [Google Scholar] [CrossRef] [PubMed]
- Genevieve F. Dunton, Stephen S. Intille, Jennifer Wolch, and Mary Ann Pentz. “Investigating the impact of a smart growth community on the contexts of children’s physical activity using Ecological Momentary Assessment.” Health & Place 18 (2012): 76–84. [Google Scholar] [CrossRef] [PubMed]
- Amanda J. Lehning, Richard J. Smith, and Ruth E. Dunkle. “Age-Friendly Environments and Self-Rated Health: An Exploration of Detroit Elders.” Research on Aging 36 (2012): 72–94. [Google Scholar] [CrossRef] [PubMed]
- Verena H. Menec, and Scott Nowicki. “Examining the relationship between communities’ ’age-friendliness’ and life satisfaction and self-perceived health in rural Manitoba, Canada.” Rural and Remote Health 14 (2014): 1–14. Available online: http://www.rrh.org.au/articles/subviewnew.asp?ArticleID=2594 (accessed on 25 December 2015). [Google Scholar]
- Kim L. Bercovitz, and Harvey A Skinner. “Active Living—Just a passing fad? ” Canadain Journal of Public Health 87 (1996): 275–79. [Google Scholar]
- Elaine Gallagher, and Angie Mallhi. “Age-Friendly British Columbia. Lessons learned from October 1, 2007–September 30, 2010. ” Available online: http://www2.gov.bc.ca/assets/gov/people/seniors/about-seniorsbc/afbc/afbc_evaluation_report.pdf (accessed on 25 December 2015).
- Neil Steffler, and Lisa Kaldeway. “City of Kawartha Lakes Age-Friendly Project Assessment: Report to the Community, 2011.” Available online: http://www.hkpr.on.ca/Portals/0/PDF%20Files%20-%20CDIP/AFReport-web.pdf (accessed on 10 October 2014).
- Verena H. Menec, Sheila Novek, Dawn Veselyuk, and Jennifer McArthur. “Lessons learned from a Canadian province-wide age-friendly initiative: The Age-Friendly Manitoba Initiative.” Journal of Aging & Social Policy 26 (2014): 33–51. [Google Scholar] [CrossRef] [PubMed]
- Mary Wiley. “Niagara Age-Friendly Community Initiative Year 1 2010–2011. Evaluation Report.” Available online: https://notl.civicweb.net/document/3543/Niagara%20Age-Friendly%20Summary%20Report.pdf?handle=0A6A4D09624A46BF808D78BEB6BFA16F (accessed on 25 December 2015).
- WHO Centre for Health Development. “2nd WHO Consultation on Developing Indicators for Age-Friendly Cities.” 8 September 2013. Available online: http://www.seniorscouncil.net/uploads/files/AFC_Mtg-2_Report_SEP2013_Quebec.pdf (accessed on 14 August 2015).
- “Parachute.” Available online: http://www.parachutecanada.org/safecommunities (accessed on 6 September 2015).
- Nilsen Per. “What makes community based injury injury prevention work? In search of evidence of effectiveness.” Injury Prevention 10 (2004): 268–274. [Google Scholar] [CrossRef] [PubMed]
- Brian D. Johnston. “Injury prevention in safe communities.” Injury Prevention 17 (2011): 1–2. [Google Scholar] [CrossRef] [PubMed]
- Casey P. Durand, Mohammad Andalib, Genevieve F. Dunton, Jennifer Wolch, and Mary Ann Pentz. “A systematic review of built environment factors related to physical activity and obesity risk: Implications for smart growth urban planning.” Obesity Reviews 12 (2011): e173–82. [Google Scholar] [CrossRef] [PubMed]
- Nazeem Muhajarine. “Canadian Evidence on Built Environment and Health.” Canadian Journal of Public Health 103 (2012): S3–72. [Google Scholar] [PubMed]
- Lynne Mitchell, Elizabeth Burton, and Shibu Raman. “Dementia-friendly cities: Intelligible neighbourhoods for life.” Journal of Urban Design 9 (2004): 89–101. [Google Scholar] [CrossRef]
- Lynne Mitchell. “Breaking New Ground. The Quest for Dementia-Friendly Communities.” 2012. Available online: www.housinglin.org.uk (accessed on 14 September 2015).
- Jason Su. “Built for Dementia: Urban Design analysis for Dementia-Friendly Communities.” Master Thesis, San Jose State University, San Jose, CA, USA, 1 April 2013. Available online: http://scholarworks.sjsu.edu/cgi/viewcontent.cgi?article=1317&context=etd_projects (accessed on 25 December 2015). [Google Scholar]
- Matthias Ruth, and Rachel S. Franklin. “Livability for all? Conceptual limits and practical limitations.” Applied Geography 49 (2014): 18–23. [Google Scholar] [CrossRef] [PubMed]
- “Partnership for Sustainable Communities. ” Available online: https://www.sustainablecommunities.gov/mission/livability-principles (accessed on 6 September 2015).
- Atlanta Regional Commission. “Livable Centers Initiative (LCI) Implementation Report.” 2013. Available online: http://www.atlantaregional.com/land-use/livable-centers-initiative (accessed on 10 August 2015).
- “Partners for Livable Communities.” Available online: http://livable.org (accessed on 6 September 2015).
- Silvie Schulze, and Francesca Moneti. “The Child Friendly Cities Initiative.” Municipal Engineer 160 (2007): 77–81. [Google Scholar] [CrossRef]
- World Health Organization. “Healthy Settings.” 2014. Available online: http://www.who.int/healthy_settings/types/cities/en (accessed on 6 September 2015).
- Malin Arvidson, Fergus Lyon, Stephen McKay, and Domenico Moro. “The ambitions and challenges of SROI. Third Sector Research Centre.” 2010. Available online: https://eprints.mdx.ac.uk/7104/1/The_ambitions_and_challenges_of_SROI.pdf (accessed on 6 September 2015).
- Ray Pawson, and Nick Tilley. Realistic Evaluation. London: Sage, 1997. [Google Scholar]
- Sarah Earl, Fred Carden, and Terry Smutylo. Outcome Mapping. Building Learning and Reflection into Development Programs. Ottawa: International Development Research Centre, 2001, Available online: http://www.outcomemapping.ca/download.php?file=/resource/files/OM_English_final.pdf (accessed on 25 December 2015).
- Evelyne De Leeuw, and Thomas Skovgaard. “Utility-driven evidence for healthy cities: Problems with evidence generation and application.” Social Science & Medicine 61 (2005): 1331–41. [Google Scholar] [CrossRef] [PubMed]
- Evelyne De Leeuw. “Evaluating WHO Healthy Cities in Europe: Issues and perspectives.” Journal of Urban Health 90 (2013): 14–22. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williams-Roberts, H.; Jeffery, B.; Johnson, S.; Muhajarine, N. The Effectiveness of Healthy Community Approaches on Positive Health Outcomes in Canada and the United States. Soc. Sci. 2016, 5, 3. https://doi.org/10.3390/socsci5010003
Williams-Roberts H, Jeffery B, Johnson S, Muhajarine N. The Effectiveness of Healthy Community Approaches on Positive Health Outcomes in Canada and the United States. Social Sciences. 2016; 5(1):3. https://doi.org/10.3390/socsci5010003
Chicago/Turabian StyleWilliams-Roberts, Hazel, Bonnie Jeffery, Shanthi Johnson, and Nazeem Muhajarine. 2016. "The Effectiveness of Healthy Community Approaches on Positive Health Outcomes in Canada and the United States" Social Sciences 5, no. 1: 3. https://doi.org/10.3390/socsci5010003
APA StyleWilliams-Roberts, H., Jeffery, B., Johnson, S., & Muhajarine, N. (2016). The Effectiveness of Healthy Community Approaches on Positive Health Outcomes in Canada and the United States. Social Sciences, 5(1), 3. https://doi.org/10.3390/socsci5010003