Translation and Linguistic Validation of a Swedish Study-Specific Questionnaire for Use among Norwegian Parents Who Lost a Child to Cancer

Abstract
:1. Introduction
Childhood Cancer
2. The Swedish Study-Specific Questionnaire
2.1. Instrument Equivalence
2.2. Purpose
- whether the questions were understood as intended,
- whether the range of response alternatives was adequate, and
- whether there were any conceptual issues with the translation of the Swedish study-specific questionnaire.
3. Materials and Methods
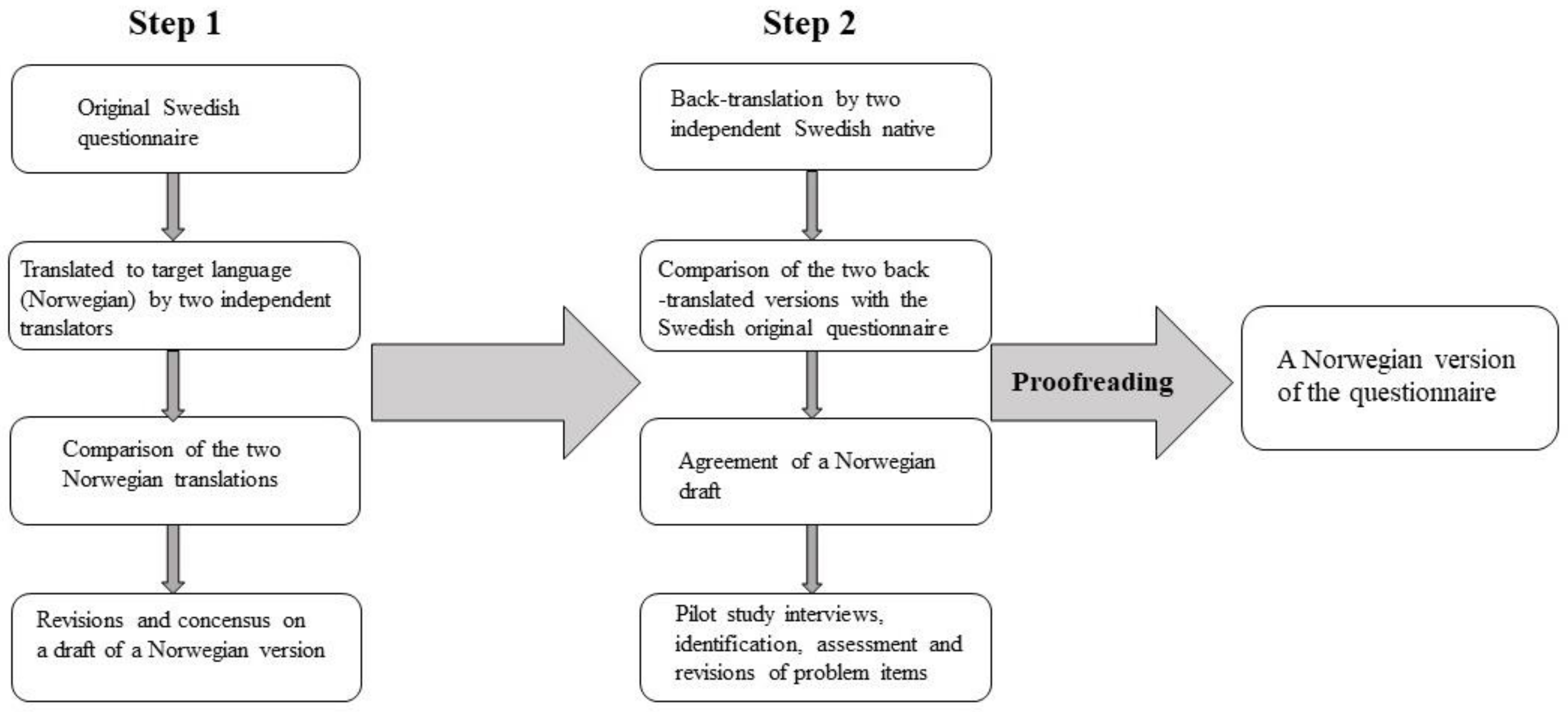
3.1. Translation and Linguistic Validation of the Study-Specific Questionnaire
3.2. Participants
3.3. Procedure
3.4. Data Analyses
- The research team independently analyzed the transcribed interviews, looking for parents’ comments about their understanding of questions, items, and response alternatives. The researchers also looked for words or phrases the informants found upsetting or negative in any way. At the end of each interview, the informants were asked if the questionnaire failed to address any important topics that were related to their experience of having a child with cancer who died of the disease.
- After a discussion of the problematic issues, a Norwegian draft was made. The Norwegian draft was then compared to the Swedish version of the questionnaire. The research group evaluated the issues and made necessary adjustments to the questions, response alternatives, and/or items to achieve the best possible fit for a Norwegian population of bereaved parents.
- These two steps were repeated three times, after the first, fourth, and sixth interviews. After the sixth interview, a final version of the translated Norwegian study-specific questionnaire were made.
3.5. Ethics
4. Results
4.1. Issues with Medical Terminology
4.2. Conceptual Issues
4.3. Issues with Response Alternatives
4.4. Need for Extra Questions
5. Discussion
5.1. Questions Added
5.2. Vulnerable Population
6. Implications for Practice
7. Strengths and Limitations
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Akard, Terrah Foster, Mary Jo Gilmer, Katy Miller, Amii Corbisiero Steele, Kelly Hancock, Maru Barrera, Bruce Compas, Betty Davies, Mary S. Dietrich, Diane L. Fairclough, and et al. 2014. Factors affecting recruitment and participation of bereaved parents and siblings in grief research. Progress in Palliative Care 22: 75–79. [Google Scholar] [CrossRef] [PubMed]
- Alderman, Amy K., and Barbara Salem. 2010. Survey research. Plastic and Reconstructive Surgery 126: 1381–89. [Google Scholar] [CrossRef] [PubMed]
- Barrera, Maru, Norma Mammone D’Agostino, Gerald Schneiderman, Susan Tallett, Lynlee Spencer, and Vesna Jovcevska. 2007. Patterns of Parental Bereavement Following the Loss of a Child and Related Factors. Omega (Westport) 55: 145–67. [Google Scholar] [CrossRef] [PubMed]
- Barrera, Maru, Kathleen O’Connor, Norma Mammone D’Agostino, Lynlee Spencer, David Nicholas, Vesna Jovcevska, Susan Tallett, and Gerald Schneiderman. 2009. Early parental adjustment and bereavement after childhood cancer death. Death Studies 33: 497–520. [Google Scholar] [CrossRef] [PubMed]
- Beaton, Dorcas E., Claire Bombardier, Francis Guillemin, and Marcos B. Ferraz. 2000. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 25: 3186–91. [Google Scholar] [CrossRef] [PubMed]
- Bice, Thomas E., and Esko Kalimo. 1971. Comparisons of health-related attitudes: A cross-national, factor analytic study. Social Science and Medicine 5: 283–318. [Google Scholar] [CrossRef]
- Björk, Maria, Annelie J. Sundler, Inger Hallström, and Kina Hammarlund. 2016. Like being covered in a wet and dark blanket—Parents’ lived experiences of losing a child to cancer. European Journal of Oncology Nursing 25: 40–45. [Google Scholar] [CrossRef] [PubMed]
- Bogensperger, Julia, and Brigitte Lueger-Schuster. 2014. Losing a child: Finding meaning in bereavement. European Journal of Psychotraumatology 5: 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bricout, Vèronique-Aurèlie. 2017. Translation and linguistic validation of an English version of the Questionnaire of Fatigue for Sport Children “QFSC”. Physiology & Behavior 171: 55–60. [Google Scholar]
- Buyukcan-Tetik, Asuman, Catrin Finkenauer, Henk Schut, Margaret Stroebe, and Wolfgang Stroebe. 2017. The impact of bereaved parents` perceived grief similarity on relationship satisfaction. Journal of Family Psychology 31: 409–19. [Google Scholar] [CrossRef] [PubMed]
- Charlton, Rodger. 2000. Research: Is an “ideal” questionnaire possible? International Journal of Clinical Practice 54: 356–59. [Google Scholar] [PubMed]
- Da Silva, Guilherme F., Maria Tereza A. Morano, Maria Penha U. Sales, Natalia B. Olegário, Antonio George M. Cavalcante, and Eanes D. B. Pereira. 2014. Comparison of face-to-face interview and telephone interview administration of COPD assessment test: A randomized study. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation 23: 1193–97. [Google Scholar] [CrossRef] [PubMed]
- Dahlen, Aina Helen, Eva Widing, Bernward Zeller, Stein Aaserud, Solveig Hansen, Hilde Koch Lie, Finn Wesenberg, Liv Marit Dørum, and Lena Holmström. 2015. Årsrapport 2015 [Annual report 2015]. Available online: https://www.kreftregisteret.no/globalassets/publikasjoner-og-rapporter/arsrapporter/publisert-2016/arsrapport-2015-barnekreft.pdf (accessed on 16 November 2017).
- Del Duca, Giovani Firpo, Markus Vinicius Nahas, Diego Augusto Santos Silva, Pedro Curi Hallal, Deborah Carvalho Malta, and Marco Aurèlio Peres. 2013. Physical activity indicators in adults from a state capital in the South of Brazil: A comparison between telephone and face-to-face surveys. Cardernos de Saude Publica 29: 2119–29. [Google Scholar] [CrossRef]
- Dyregrov, Kari. 2004. Bereaved parents’ experience of research participation. Social Science and Medicine 58: 391–400. [Google Scholar] [CrossRef]
- Eremenco, Sonya L., David Cella, and Benjamin J. Arnold. 2005. A Comprehensive Method for the Translation and Cross-Cultural Validation of Health Status Questionnaires. Evaluation & the Health Professions 28: 212–32. [Google Scholar]
- Gatta, Gemma, Laura Botta, Silvia Rossi, Tiiu Aareleid, Magdalena Bielska-Lasota, Jacqueline Clavel, Nadya Dimitrova, Zsuzsanna Jakab, Peter Kaatsch, Brigitte Lacour, and et al. 2014. Childhood cancer survival in Europe 1999–2007: Results of EUROCARE-5-a population-based study. The Lancet Oncology 15: 35–47. [Google Scholar] [CrossRef]
- Goodenough, Belinda, Donna Drew, Susan Higgins, and Susan Trethewie. 2004. Bereavement outcomes for parents who lose a child to cancer: Are place of death and sex of parent associated with differences in psychological functioning? Psycho-Oncology 13: 779–91. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services Food and Drug Administration. 2009. Guidance for Industry: Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims; Silver Spring: Silver spring Publishing.
- Hogan, Nancy S., and Lee A. Schmidt. 2002. Testing the grief to personal growth model using structural equation modeling. Death Studies 26: 615–34. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, Allyson L., Melanie C. Green, and Jon A. Krosnick. 2003. Telephone versus Face-to-Face Interviewing of National Probability Samples with Long Questionnaires. Public Opinion Quarterly 67: 79–125. [Google Scholar] [CrossRef]
- Hunt, Hayley, Unnur Valdimarsdottir, Lorelei Mucci, Ulrika Kreicbergs, and Gunnar Steineck. 2006. When death appears best for the child with severe malignancy: A nationwide parental follow-up. Palliative Medicine 20: 567–77. [Google Scholar] [CrossRef] [PubMed]
- Jalmsell, Li. 2015. Towards Good Palliation for Children with Cancer. Recognizing the Family and the Value of Communication. Uppsala, Sweden: Uppsala Universitet. [Google Scholar]
- Kamm, Sherrie, and Brian Vandenberg. 2001. Grief communication, grief reactions and marital satisfaction in bereaved parents. Death Studies 25: 569–82. [Google Scholar] [CrossRef] [PubMed]
- Kreicbergs, Ulrika. 2004. To Lose a Child to Cancer. A Nationwide Study of Parental Experiences. Stockholm: Karolinska Institutet. [Google Scholar]
- Kreicbergs, Ulrika, Unnur Valdimarsdóttir, Erik Onelöv, Jan-Inge Henter, and Gunnar Steineck. 2004. Anxiety and depression in parents 4–9 years after the loss of a child owing to a malignancy: A population-based follow-up. Psychological Medicine 34: 1431–41. [Google Scholar] [CrossRef] [PubMed]
- Kreicbergs, Ulrika, Unnur Valdimarsdóttir, Gunnar Steineck, and Jan-Inge Henter. 2004. A population-based nationwide study of parents’ perceptions of a questionnaire on their child’s death due to cancer. Lancet 364: 787–89. [Google Scholar] [CrossRef]
- Kreicbergs, Ulrika, Unnur Valdimarsdóttir, Erik Onelöv, Olle Björk, Gunnar Steineck, and Jan-Inge Henter. 2005. Care-related distress: A nationwide study of parents who lost their child to cancer. Journal of Clinical Oncology 23: 9162–71. [Google Scholar] [CrossRef] [PubMed]
- Kreicbergs, Ulrika C., Patrizia Lannen, Erik Onelov, and Joanne Wolfe. 2007. Parental grief after losing a child to cancer: Impact of professional and social support on long-term outcomes. Journal of Clinical Oncology 25: 3307–12. [Google Scholar] [CrossRef] [PubMed]
- Kristiansen, Ivar Sønbø, and Kjeld Møller Pedersen. 2000. Helsevesenet i de nordiske land—Er likhetene større enn ulikhetene? Tidsskrift for Den Norske Legeforening 17: 2023–29. [Google Scholar]
- Lannen, Patrizia. 2008. The Experience of Parents Who Have Lost a Child to Cancer: Palliative and Bereavement Care. Bern: University of Bern. [Google Scholar]
- Lannen, Patrizia K., Joanne Wolfe, Holly G. Prigerson, Erik Onelov, and Ulrika C. Kreicbergs. 2008. Unresolved grief in a national sample of bereaved parents: Impaired mental and physical health 4 to 9 years later. Journal of Clinical Oncology 26: 5870–76. [Google Scholar] [CrossRef] [PubMed]
- Li, Jiong, Dorthe Hansen Precht, Preben Bo Mortensen, and Jørn Olsen. 2003. Mortality in parents after death of a child in Denmark: A nationwide follow-up study. Lancet 361: 363–67. [Google Scholar] [CrossRef]
- Li, Jiong, Thomas Munk Laursen, Dorthe Hansen Precht, Jørn Olsen, and Preben Bo Mortensen. 2005. Hospitalization for Mental Illness among Parents after the Death of a Child. New England Journal of Medicine 352: 1190–96. [Google Scholar] [CrossRef] [PubMed]
- Lichtental, Wendy G., Corinne R. Sweeney, Kailey E. Roberts, Geoffrey W. Corner, Leigh A. Donovan, Holly G. Prigerson, and Lori Wiener. 2015. Bereavement Follow-Up after the Death of a Child as a Standard of Care in Pediatric Oncology. Pediatric Blood Cancer 62: 834–69. [Google Scholar] [CrossRef] [PubMed]
- Lichtenthal, Wendy G., Geoffrey W. Corner, Corinne R. Sweeney, Lori Wiener, Kailey E. Roberts, Raymond E. Baser, Yuelin Li, William Breitbart, David W. Kissane, and Holly G. Prigerson. 2015. Mental health services for parents who lost a child to cancer: If we build them, Will they come? Journal of Clinical Oncology 33: 2246–53. [Google Scholar] [CrossRef] [PubMed]
- Logan, Emma L., Jennifer A. Thornton, Robert T. Kane, and Lauren J. Breen. 2017. Social support following bereavement: The role of beliefs, expectations, and support intentions. Death Studies 1187: 34. [Google Scholar] [CrossRef] [PubMed]
- Maneesriwongul, Wantana, and Jane K. Dixon. 2004. Instrument translation process: A methods review. Journal of Advanced Nursing 48: 175–86. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, Maria C., Naomi E. Clarke, Cheng Lin Ting, Rowena Conroy, Vicki A. Anderson, and John A. Heath. 2010. Prevalence and predictors of parental grief and depression after the death of a child from cancer. Journal of Palliative Medicine 13: 1321–26. [Google Scholar] [CrossRef] [PubMed]
- McCoyd, Judith L.M., and Toba Schwaber Kerson. 2006. Conducting Intensive Interviews Using Email. Qualitative Social Work: Research and Practice 5: 389–406. [Google Scholar] [CrossRef]
- Mealer, Meredith, and Jacqueline Jones. 2014. Methodological and ethical issues related to qualitative telephone interviews on sensitive topics. Nurse Researcher 21: 32–37. [Google Scholar] [CrossRef] [PubMed]
- Meert, Kathleen L. M., Sherylyn H. Briller, Stephanie Myers Schim, Celia Thurston, and Allison Kabel. 2009. Examining the needs of bereaved parents in the pediatric intensive care unit: A qualitative study. Death Studies 33: 712–40. [Google Scholar] [CrossRef] [PubMed]
- Monterosso, Leanne, and Linda J. Kristjanson. 2008. Supportive and palliative care needs of families of children who die from cancer: An Australian study. Palliative Medicine 22: 59–69. [Google Scholar] [CrossRef] [PubMed]
- Murphy, Shirley A., Janet Lohan, Tom Braun, Clark L. Johnson, Kevin C. Cain, Randal D. Beaton, and Robert Baugher. 1999. Parents’ health, health care utilization, and health behaviors following the violent deaths of their 12- to 28-year-old children: A prospective longitudinal analysis. Death Studies 23: 589–616. [Google Scholar] [PubMed]
- Najman, Jake M., John C. Vance, Fran Boyle, Gary Embleton, Bill Foster, and John Thearle. 1993. The impact of a child death on marital adjustment. SosialScience &Medicine 37: 1005–10. [Google Scholar]
- Olsen, Jørgen H., Torgil Möller, Harald Anderson, Frøydis Langmark, Risto Sankila, Laufey Tryggvadóttír, Jeanette Falck Winther, Catherine Rechnitzer, Gudmundur Jonmundsson, Jane Christensen, and et al. 2009. Lifelong cancer incidence in 47 697 patients treated for childhood cancer in the nordic countries. Journal of the National Cancer Institute 101: 806–13. [Google Scholar] [CrossRef] [PubMed]
- Omerov, Pernilla, Gunnar Steineck, Bo Runeson, Anna Christensson, Ulrika Kreicbergs, Rossana Pettersén, Birgitta Rubenson, Johanna Skoogh, Ingela Rådestad, and Ullakarin Nyberg. 2013. Preparatory studies to a population-based survey of suicide-bereaved parents in Sweden. Crisis 34: 200–10. [Google Scholar] [CrossRef] [PubMed]
- Quittner, Alexandra L., Sheri Sweeny, Marc Watrous, Paul Munzenberger, Karen Bearss, Amy Gibson Nitza, Lisa A. Fisher, and Bernadette Henry. 2000. Translation and linguistic validation of a disease-specific quality of life measure for cystic fibrosis. Journal of Pediatric Psychology 25: 403–14. [Google Scholar] [CrossRef] [PubMed]
- Rapport fra Helsetilsynet. 2016. Informasjonen var mangelfull og kom ofte for sent. Oppsummering av landsomfattende tilsyn i 2015 med samhandling om utskriving av pasienter fra spesialisthelsetjenesten til kommunen. Oslo: Helsetilsynet, Available online: https://www.helsetilsynet.no/publikasjoner/rapport-fra-helsetilsynet/2016/informasjonen-var-mangelfull-og-kom-ofte-for-sent-oppsummering-av-landsomfattande-tilsyn-i-2015/ (accessed on 25 November 2017).
- Robert, Rhonda, Donna S. Zhukovsky, Riza Mauricio, Katherine Gilmore, Shirley Morrison, and Guadalupe R. Palos. 2012. Bereaved Parents’ Perspectives on Pediatric Palliative Care. Journal of Social Work in End-Of-Life & Palliative Care 8: 316–38. [Google Scholar]
- Rubin, Simon Shimshon, and Ruth Malkinson. 2001. Parental response to child loss across the life cycle: Clinical and research perspectives. In Handbook of Bereavement Research: Consequences, Coping, and Care. Edited by Margaret S. Stroebe, Wolfgang Stroebe, Robert O. Hansson and Henk Schut. Washington, DC: American Psychological Association, pp. 219–40. [Google Scholar]
- Siegel, Rebecca L., Kimberly D. Miller, and Ahmedin Jemal. 2018. Cancer Statistics, 2018. CA. A Cancer Journal for Clinicians 68: 7–30. [Google Scholar] [CrossRef] [PubMed]
- Song, Jieun, Frank J. Floyd, Marsha Mailick Seltzer, Jan S. Greenberg, and Jinkuk Hong. 2010. Long-Term Effects of Child Death on Parents’ Health-Related Quality of Life: A Dyadic Analysis. Family Relations 59: 269–82. [Google Scholar] [CrossRef] [PubMed]
- Sperber, Ami D. 2004. Translation and validation of study instruments for cross-cultural research. Gastroenterology 126: S124–28. [Google Scholar] [CrossRef] [PubMed]
- Sperber, Ami D., Robert F. Devellis, and Brian Boehlecke. 1994. Cross-Cultural Translation: Methodology and Validation. Journal of Cross-Cultural Psychology 25: 501–24. [Google Scholar] [CrossRef]
- Stevens, Michael M., Bruce A. Lord, Marie-Thèrèse Proctor, Sue Nagy, and Elizabeth O’Riordan. 2010. Research with Vulnerable Families Caring for Children with Life-Limiting Conditions. Qualitative Health Research 20: 496–505. [Google Scholar] [CrossRef] [PubMed]
- Stroebe, Margaret, Henk Schut, and Wolfgang Stroebe. 2007. Health outcomes of bereavement. The Lancet 370: 1960–73. [Google Scholar] [CrossRef]
- Surkan, Pamela J. 2006. Predictors and Consequences of Loss of a Child: Nationalwide Epidemiological Studies from Sweden. Stockholm: Karolinska Instutuet. [Google Scholar]
- Surkan, Pamela J., Ulrika Kreicbergs, Unnur Valdimarsdóttir, Ullakarin Nyberg, Erik Onelöv, Paul W. Dickman, and Gunnar Steineck. 2006. Perceptions of Inadequate Health Care and Feelings of Guilt in Parents after the Death of a Child to a Malignancy: A Population-Based Long-Term Follow-Up. Journal of Palliative Medicine 9: 317–31. [Google Scholar] [CrossRef] [PubMed]
- Trier-Bieniek, Adrienne. 2012. Framing the telephone interview as a participant-centred tool for qualitative research: A methodological discussion. Qualitative Research 12: 630–44. [Google Scholar] [CrossRef]
- UyBico, Stacy J., Shani Pavel, and Cary P. Gross. 2007. Recruiting vulnerable populations into research: A systematic review of recruitment interventions. Journal of General Internal Medicine 22: 852–63. [Google Scholar] [CrossRef] [PubMed]
- Valdimarsdóttir, Unnur, Ulrika Kreicbergs, Arna Hauksdóttir, Hayley Hunt, Erik Onelöv, Jan-Inge Henter, and Gunnar Steineck. 2007. Parents’ intellectual and emotional awareness of their child’s impending death to cancer: A population-based long-term follow-up study. Lancet Oncology 8: 706–14. [Google Scholar] [CrossRef]
- Van der Geest, Ivana M. M., Anne-Sophie E. Darlington, Isabelle C. Streng, Erna M. C. Michiels, Rob Pieters, and Marry M. van den Heuvel-Eibrink. 2014. Parents’ Experiences of Pediatric Palliative Care and the Impact on Long-Term Parental Grief. Journal of Pain and Symptom Management 47: 1043–53. [Google Scholar] [CrossRef] [PubMed]
- Weidner, Norbert. J., Marcella Cameron, Rebecca C. Lee, Judy McBride, Emily J. Mathias, and Terry L. Byczkowski. 2011. End-of-life care for the dying child: What matters most to parents. Journal of Palliative Care 27: 279–86. [Google Scholar] [PubMed]
- Wender, Esther. 2012. Supporting the family after the death of a child. Pediatrics 130: 1164–69. [Google Scholar] [CrossRef] [PubMed]
- White Paper nr. 47. 2009. The Coordination Reform, Proper Treatment—At the Right Place and Right Time; Oslo: Norwegian Ministry of Health and Care Services. Available online: https://www.regjeringen.no/contentassets/d4f0e16ad32e4bbd8d8ab5c21445a5dc/no/pdfs/stm200820090047000dddpdfs.pdf (accessed on 16 December 2017).
- WHO. n.d. Process of Translation and Adaptation of Instruments. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 5 January 2018).
- Wild, Diane, Alyson Grove, Mona Martin, Sonya Eremenco, Sandra McElroy, Aneesa Verjee-Lorenz, and Pennifer Erikson. 2005. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: Report of the ISPOR Task Force for Translation and Cultural Adaptation. Value in Health 8: 94–104. [Google Scholar] [CrossRef] [PubMed]
- Zhang, XiaoChi, Lars Kuchinke, Marcella L. Woud, Julia Velten, and Jürgen Margraf. 2017. Survey method matters: Online/offline questionnaires and face-to-face or telephone interviews differ. Computers in Human Behavior 71: 172–80. [Google Scholar] [CrossRef]


{kind=link}
| Main Sections *1 | Questions *2 | Content Summary |
|---|---|---|
| Questions about you and your life situation at the time your child got sick | 14 questions (15 items) | Family situation at the time the child was diagnosed with cancer (e.g., gender, age, marital status, total number of children) Child’s age at the time of the diagnosis Whether the parents lived together and with the child at the time of diagnosis |
| How you and your child received the message about the cancer illness | 15 questions (27 items) | How the child was informed about the diagnosis (e.g., if the child was with one or both parents, without either parents, or if they were never informed). There is also a follow-up item asking who informed the child. How the parents were informed about the diagnosis (see example above) Whether the cancer disease was curable Whether the parents were satisfied with the information they received from health care professionals |
| Your child’s last month of life | 12 questions (56 items) | Parents’ experiences with the health care provided (pain relief, treatment of depression/anxiety) Communication with the child Whether the parents received the support they needed |
| Insight into your child’s death and conversation about death | 29 questions (48 items) | If and when the parents understood that their child was going to die If the child understood that he/she was going to die Conversations about death with the child Conversations about death with family/friends/health care professionals |
| The time after your child died | Eight questions (22 items) | Follow-up and conversations with the health care personnel treating the child The time-span of these conversations A retrospective view of the health care their child received during their illness period |
| You and your current life situation | 26 questions (34 items) | Sociodemographic questions Whether the parents religious beliefs was affected by their child’s death Social support Adjustment to the loss Items about how they experienced to fill out the questionnaire |
| Issues with Medical Terms | Modifications |
|---|---|
| “Did your child’s illness relapse (recidivate) after the illness had disappeared?” | “Did your child’s cancer disease reoccur (relapse) after he/she had been declared healthy?” |
| “How long before your child died was curative treatment discontinued?” | “How long before your child died was curative treatment for your child’s cancer disease discontinued?” |
| “Was the illness the direct cause of your child’s death, or was death due to complications caused by treatment?” | “Was the cancer disease the direct cause of your child’s death, or was it due to complications caused by the treatment?” |
| Conceptual issues | Modifications |
| “Do you think doctors should be explicit when they realise that the disease cannot be cured?” | “Do you think doctors should be explicit with the parents when they realise that the disease cannot be cured?” |
| “Could you talk with your child about topics you considered important during your child’s illness period?” | “Could you talk with your child about topics you considered important “there and then” during your child’s illness period?” |
| “The health-care professionals reacted quickly if my child or I needed help”. | “The health-care professionals reacted quickly if my child needed help”. |
| Issues with response alternatives | Modifications |
| Question: “Did your child receive bone marrow transplant?” “No, my child did not receive a bone marrow transplant”. “Yes, he/she had bone marrow transplant with his/her own bone marrow”. “Yes, he/she had bone marrow transplant with a donor’s bone marrow”. “Yes, he/she had multiple bone marrow transplants, _______times”. | Question: “Did your child receive bone marrow transplant?” “No, my child did not receive a bone marrow transplant”. “Yes, he/she had bone marrow transplant with his/her own bone marrow”. “Yes, he/she had bone marrow transplant with a donor’s bone marrow”. “Please, comment”. Space for personal comments was added in the questionnaire. |
| Question: “Did you receive any social support to help you deal with your emotions and the situation in general during your child’s illness period?” “From health-care personnel”; “From family, relatives and friends”; “Other, who?” The response alternatives are: “No, not at all”; “Yes some”; “Yes, enough”; “Yes, a lot”. | Question: “Did you receive any social support to help you deal with your emotions and the situation in general during your child’s illness period?” “From health-care personnel”; “From family, relatives and friends”; “Other, who?” The response alternatives were revised to: “No, not at all”; “Yes some”; “Yes, enough”; “Yes, a lot”: and “Not relevant, I did not need social support”. |
| Question: “Do you think you have processed your grief?” “No, not at all”; “Yes, a little”; “Yes, fairly much”; and “Yes, completely”. | Question: “Do you think you have processed your grief?” “No, not at all”; “Yes, a little”; “Yes, fairly much”. |
| Question: “Have your personal or spiritual/religious beliefs been affected by the loss of your child?” The response alternatives are: “Not relevant, I do not have a spiritual/religious beliefs”, “Yes, some”; “Yes, to a certain degree”; “Yes, a lot”. | Question: “Have your personal or spiritual/religious beliefs been affected by the loss of your child?” The response alternatives are revised to: “No”; “Not relevant, I do not have a spiritual/religious beliefs”; “Yes, some”; “Yes, to a certain degree”; “Yes, a lot”. |
| Question added | |
| One recurring theme in the interviews was the lack of follow-up in the municipalities after the child died | Question: “Have your received any help/follow-up from your municipality to help you in your grief process after your child’s death? From whom?” Response alternatives: “GP”; “Psychiatric nurse in your municipality”; “Psychologist”; “Home nursing care”; “Bereavement group”; “Voluntary/humanitarian organization”; “Religious community”; “Other:______ ” Follow-up item: “Did you find the help from the municipality useful”: “Yes/No”. “”Please comment”: Space was added for personal comments. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vegsund, H.-K.; Rannestad, T.; Reinfjell, T.; Moksnes, U.K.; Wallin, A.E.; Eilertsen, M.-E.B. Translation and Linguistic Validation of a Swedish Study-Specific Questionnaire for Use among Norwegian Parents Who Lost a Child to Cancer. Soc. Sci. 2018, 7, 187. https://doi.org/10.3390/socsci7100187
Vegsund H-K, Rannestad T, Reinfjell T, Moksnes UK, Wallin AE, Eilertsen M-EB. Translation and Linguistic Validation of a Swedish Study-Specific Questionnaire for Use among Norwegian Parents Who Lost a Child to Cancer. Social Sciences. 2018; 7(10):187. https://doi.org/10.3390/socsci7100187
Chicago/Turabian StyleVegsund, Hilde-Kristin, Toril Rannestad, Trude Reinfjell, Unni Karin Moksnes, Alexandra Eilegård Wallin, and Mary-Elizabeth Bradley Eilertsen. 2018. "Translation and Linguistic Validation of a Swedish Study-Specific Questionnaire for Use among Norwegian Parents Who Lost a Child to Cancer" Social Sciences 7, no. 10: 187. https://doi.org/10.3390/socsci7100187
APA StyleVegsund, H. -K., Rannestad, T., Reinfjell, T., Moksnes, U. K., Wallin, A. E., & Eilertsen, M. -E. B. (2018). Translation and Linguistic Validation of a Swedish Study-Specific Questionnaire for Use among Norwegian Parents Who Lost a Child to Cancer. Social Sciences, 7(10), 187. https://doi.org/10.3390/socsci7100187