1. Introduction
The global interconnectedness of health in our modern world is unquestionable. There is evidence to support how the state of health of one nation may affect the health and well-being of others globally. Each country must be resolute/firm in addressing health concerns in its foreign policy as they are with their domestic policy. Traditionally, the main issue on the global agenda was addressing mainly communicable or infectious diseases (
Saker et al. 2004). Increasingly, health issues are dominant and pervasive in the evolving global diplomacy agenda. Within this milieu, there are competing interests of actors, states, and other relevant parties that must be taken into account and influence the determination of the global health agenda. Equally important, is not only to understand the impacts (both good and bad) of globalization on health but also to develop appropriate, collective, and effective global responses to these emerging issues. Even though global health is not afforded the same priority as politics and economics, certain global health threats/epidemics, such as the current COVID-19 pandemic, make the state actors/governments consider it as a top priority as it has crippled and stagnated the economy and global supply chain systems. As per the Institute of Medicine’s Expert Committee, “Global health is the goal of improving the health for all people in all nations by promoting wellness and eliminating avoidable diseases, disabilities, and deaths. It can be attained by combining clinical care at the level of the individual person with population-based measures to promote health and prevent disease. This ambitious endeavor calls for an understanding of health determinants, practices, and solutions, as well as basic and applied research concerning risk factors, disease, and disability.” (
Fineberg and Hunter 2013). The WHO’s Report from the International Meeting on Health in All Policies (HiAP) in Adelaide (
Kickbusch 2010) and the term HiAP was first used in Europe during the Finnish presidency of the European Union in 2006. The aim of HiAP is to collaborate “across sectors to achieve common goals. It is a strategy to include health considerations in policy making across different sectors that influence health, such as transportation, agriculture, land use, housing, public safety, and education. HiAP reaffirms public health’s essential role in addressing policy and structural factors affecting health, as articulated by the Ten Essential Public Health Services, and it has been promoted as an opportunity for the public health sector to engage a broader array of partners.” (
Kickbusch 2010). Since then, Global Health Diplomacy (GHD) has evolved in significant ways and is ill-defined through different schools of thought have defined using various terminologies. According to the World Health Organization (WHO), GHD enables multiple stakeholders to contribute to the greater health needs of humanity. It brings together the disciplines of public health, international affairs, management, law, and economics and focuses on negotiations that shape and manage the global policy environment for health. The relationship between health, foreign policy, and trade is at the cutting edge of global health diplomacy (
Kickbusch et al. 2007). As Kickbusch and colleagues highlighted, recently, there has been increased importance afforded to GHD primarily because health itself has become a topically discussed issue by various actors outside the WHO, G8, G20, BRICS, and the EU (
Kickbusch and Kökény 2013). While looking through an “economic vs. ethical lens” about global society and neo-colonialism, Rubbini pointed out that in the relations between developed and emerging countries as part of global health diplomacy, there is a risk that the former can adopt behaviors induced by the financial needs of overcoming their crisis and if the “ethical lens” is to prevail, it will be most likely be the hypothesis of a global society where there is a respect of human rights in order to drive growth and harmonization of relations between Governments (
Rubbini 2018).
Furthermore, foreign ministries are becoming more involved with the health domain and the rise of new public–private partnerships and alliances. This is no different within the Caribbean HiAP Community (CARICOM), where GHD is growing in importance. The CARICOM is an organization comprising twenty (20) countries: 15 member states and five associate members. It was established in 1973 on three main pillars: economic integration, functional cooperation, and foreign policy coordination. The Secretariat is the principal administrative organ that is based in Georgetown, Guyana. Considering the increasing security concerns and challenges facing the region, its leaders agreed to establish security as a fourth pillar (
Martinez et al. 2020). Within the revised treaty of the CARICOM, there are five organs, one of which is the Council on Human and Social Development, which supports the improvement of health. Another initiative is the Caribbean Cooperation in Health, a regional health strategy that has prioritized preventing communicable and NCDs, and strengthens health systems, environmental health, food and nutrition, mental health, family and children’s health, and human resources training (
Buss and Tobar 2018). The 21st century has brought new opportunities and challenges for the health of the populations in the Caribbean region, whose countries are linked by geography, history, and culture. Chronic and communicable diseases are devastating to individuals and communities, threatening quality of life and becoming an increasingly important factor in the Caribbean’s development. In the Western hemisphere, the epidemic of chronic disease has most affected the Caribbean region Shirley Augustine (
Augustine 2010). Other health initiatives by CARICOM include the Pan Caribbean Partnership Against HIV and AIDS (PANCAP) and the Caribbean Public Health Agency (CARPHA), a regional public health institute founded in 2010 (
Powers 2011).
As globalization has pushed health to the forefront of international diplomatic efforts, global health diplomacy has emerged as a means of neutralizing, managing, and correcting health threats. Viruses such as the recent novel Coronavirus 2019 (COVID-19), Ebola (
Chattu et al. 2020), Zika (
Sikka et al. 2016), and Chikungunya have demonstrated that health issues are not contained/confined to one country, can have detrimental consequences, and require an immediate response. On 11 March 2020, the WHO declared COVID-19 a pandemic, and as of 22 May 2020, there have been 4,995,996 confirmed cases from 216 countries and territories with 327,821 deaths (
WHO 2020). As per the CARPHA’s status report, dated 22 May 2020, there are 22,254 cases in 33 countries/territories (including 24 CARPHA Member States) in the Caribbean region, with 807 deaths and a high-risk alert for further importation of cases (
CARPHA 2020). In order to confront this reality, the Small Island Developing States (SIDS) are increasingly engaging with global players and forums to have their unique positions and voices heard in the complex global field of health diplomacy. The SIDS of the CARICOM region are vulnerable to many natural and man-made disasters and also not well equipped with essential infrastructure to handle emergency situations and mostly dependent on neighboring big nations for support. Hence this review was undertaken with an aim to understand and explore the emerging role of GHD in addressing these challenges and how the health domain, peace, and the well-being of citizens can be achieved through the practice of GHD in the CARICOM region.
Although globalization has pushed health as a forerunner in international affairs, it also promotes a global culture based on consumerism and trade. Consequently, international banking institutions are gaining power, with the weakening of the nation-state, and local health institutions are increasingly less responsive to the public health demands with advances in the global economic development process. The IADB’s Suriname Land Management Program (SLMP) is a good case in relation to the latter. It shows how economic development programs that change non-marketed land and mineral resources into marketable resources for the global economy, which affect health outcomes. The balance of payments requirements motivate the Suriname government to adopt adjustment policies that dispossess indigenous people of their land and livelihoods. It is an example of how the health and well-being of indigenous people are linked to inequalities generated by a neoliberal approach to economic development (
Peplow and Augustine 2017). Perhaps, more “people-centered” policies for economic-development that meets the “balance-of-payment” goals, as outlined in the UNDP 1997–2002, can be developed and adopted.
2. Materials and Methods
In this systematic review, we tried to collect the existing evidence on GHD in the Caribbean for infectious diseases, HIV/AIDS, vector-borne diseases, health security, non-communicable diseases, and natural disasters. To find relevant articles for this review, PubMed, Web of Science, Scopus, Embase databases, and Google Scholar search engines were used to find the articles published during the period 1950–2019. Keywords included MeSH and common terms related to the topic: “Global Health Diplomacy” OR “foreign policy” OR “foreign affairs” OR “international relations” OR “Health Diplomacy” OR “Medical Diplomacy” OR “Negotiations” OR “Multilateral Engagement” OR “Noncommunicable Diseases” OR “Infectious Diseases” OR “Disasters” OR “Storms” OR “Hurricanes” AND “Caribbean”. Articles published in any language other than English, articles that were not unavailable in full text, dissertations, and redundant studies were excluded. Two authors (V.K.C. and G.C.) independently assessed the study eligibility by reviewing the titles of all potential citations. Discrepancies were resolved by consensus between the reviewers. Full texts of all the relevant articles were assessed, and the data were extracted from each eligible study on the location of the study, the author’s name, and the presence and discussion of the keywords of interest. All the reference lists of identified articles of a Caribbean context were chosen.
3. Results
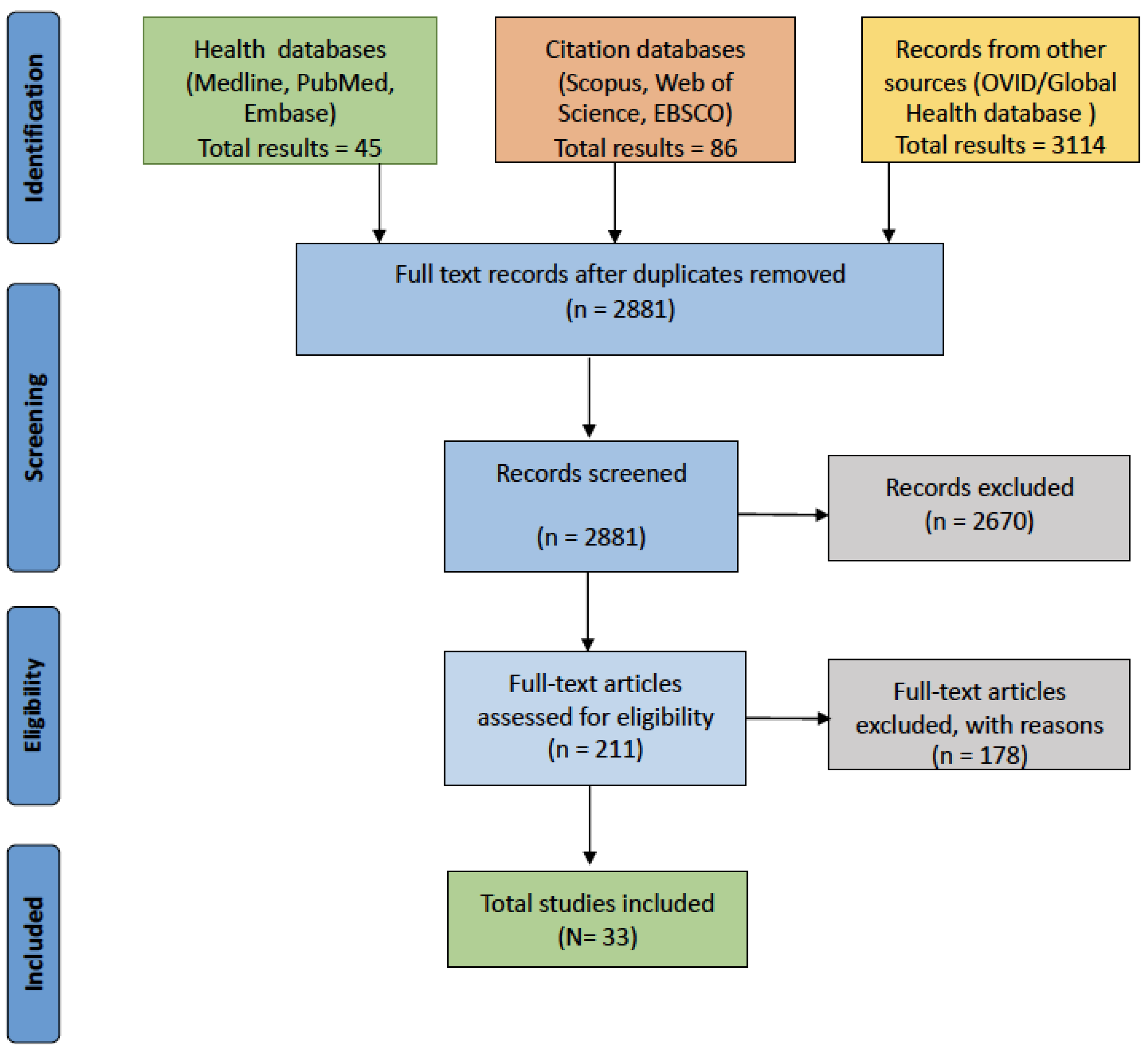
Overall, 3245 articles were extracted from all the databases. Initially, the title and abstract of the articles were screened based on the inclusion criteria, leaving 211 articles for full-text review. Around 178 articles were excluded due to lack of focus to the Caribbean region, unavailability in full-text form, or redundancy. Finally, 33 articles were selected for the final review. The screening process and search results are provided in the PRISMA flow diagram (
Liberati et al. 2009;
Figure 1).
This review attempted to highlight the key points that are essential for this multidisciplinary field in order to make successful negotiations. Nonetheless, high expectations are anticipated for global health initiatives by achieving development and diplomatic goals, which are documented in this review. All the important disasters, infectious diseases, including the recent COVID-19 pandemic, NCDs epidemics, and essential frameworks, are shown in the tables and figures in the next section. We also described the context, practice, and components of global health diplomacy, as applied in the Caribbean region.
3.1. Challenges and Outcomes of Global Health Diplomacy in the CARICOM Region
Caribbean nations have launched responses to unfavorable health trends regionally. Moreover, many countries in this region are heavily dependent on tourism for their survival. In this regard, small island states such as St Lucia, Barbados, Grenada, and Jamaica are particularly vulnerable to health threats. The Prime Minister of St. Lucia, Kenny Anthony, told the Miami Herald that “we are an exceedingly small country with very limited resources and inexperienced in dealing with a global health crisis” (
Chattu 2017). Hence, there is an urgent need to strengthen and have effective, coordinated measures for addressing health threats within the CARICOM region.
The concept of nations joining together in the diplomatic fora to tackle public health problems is a core principle of GHD (
Koplan et al. 2009). In this regard, the need for an appropriate and effective practice of GHD was evident with the global response to the Ebola outbreak in 2014. This crisis showed demands for more concerted policy responses, as well as diplomatic coordination at the global level during such a health emergency crisis. Partly in response to this, but also in recognition of the need to address ongoing global health disparities and realize the Sustainable Development Goals, CARICOM countries have focused greater attention and scrutiny on health policy. As such, regional health diplomacy is geared towards the dual goals of improving health and strengthening relations among CARICOM nations.
In the area of health, there have been some significant developments towards health promotion: the establishment of 5 regional health institutions, investments in tertiary-level institutions, and the Caribbean Cooperation in Health, which is the guide for the regional health agenda for the CARICOM states (
Theodore-Gandi and Barclay 2008). In 2007, Heads of State of Caribbean nations convened the Summit on Non-Communicable Diseases to address, for the first time, the combined epidemics (i.e., cardiovascular illness, diabetes, cancer) in the region (
PAHO 2011). The Caribbean regional “Port of Spain declaration” is one of the good examples of successful health diplomacy, which has led to the formulation of the WHO’s Global Action Plan for the Prevention and Control of NCDs (
Chattu and Knight 2019). Country-specific achievements underscore the important strides made toward improving health outcomes. Moreover, the emphasis by governments within the region on sanitation, nutrition, and primary health care has shown improvement in the health status of people in the Caribbean (
CARICOM 2006).
3.1.1. Natural Disasters in the CARICOM Region
The 2010 earthquake in Haiti is an extreme example that took lives of over 230,000 people, displaced 1.5 million, and was followed by the largest cholera epidemic ever reported in a single country (
Domercant et al. 2015). The other natural disasters that happened during the past decade (
OCHA 2019) are summarized in
Table 1 below.
3.1.2. Waterborne Diseases
In relation to health, natural disasters such as tropical storms and hurricanes provide the ideal context for the spreading of infectious diseases (
WHO 2006). Heavy rainfall, floods, and stagnant water produce the setting for the development of diseases related to water pollution. For example, Hurricane Matthew triggered the outbreak of cholera in Haiti in October 2016, as the spread of the disease was from contaminated water sources and person-to-person transmission. Additionally, in cases where is there is the internal displacement of people who are required to remain in temporary shelters where sanitary conditions are lacking, this intensifies the likelihood of contracting infectious diseases.
3.1.3. Vector Transmitted Diseases
Vector-borne diseases are human diseases caused by parasites, viruses, and bacteria that are spread by vectors (
WHO 2006). These diseases disproportionately affect the poorest populations. In recent years, outbreaks of dengue, Chikungunya, yellow fever, and Zika have caused great anxiety among populations, claimed lives, and put pressure on health systems in several countries (
Sikka et al. 2016). Furthermore, the occurrence of some vector transmitted diseases can be directly linked to tropical storms. For example, diseases such as dengue can spread during hurricane season, as stagnated water and water storage containers are ideal for the reproduction of infected mosquitoes (vectors). Dengue remains a vital concern in the Caribbean and, as seen in Haiti and the Dominican Republic, require monitoring by PAHO as an upsurge of cases was observed weeks after Hurricane Matthew.
3.1.4. Medicine Supply
Another important area is the area of medicine supply. Hurricanes can adversely impact on medicine supply in terms of its accessibility and the safety of vaccines and prescription drugs for patients with non-communicable diseases. During hurricanes, there is the likelihood of power cuts and energy shutdowns, and some of these drugs require refrigeration. This is a major problem during natural disasters, and the security of the medicines cannot be fully guaranteed.
3.2. Growing Epidemic of Non-Communicable Diseases (NCDs) in the CARICOM
CARICOM countries vary in size, geography, and resources. In this region, NCDs are seen as the highest health-related problems and the main cause of death. Aging of the population, successes in primary health care in the treatment of infectious and other diseases, and economic development have led to an NCD-epidemiological transition within the Caribbean region (
Razzaghi et al. 2019). During the period of 1999–2014, the 3 major NCDs, namely, cardiovascular diseases (CVDs), diabetes mellitus (DM), and cancers accounted for 39–67% of all deaths in the 20 Caribbean countries.
3.2.1. Cardiovascular Diseases and Hypertension
Cardiovascular disease (stroke, coronary artery disease, and diabetes) is the major cause of death in the region. Elevated blood pressure is the primary cause of cardiovascular disease. The regional Port of Spain Summit declaration of 2007, initiated by the regional heads of the state, is the only policy dedicated to NCDs using a multipronged and multi-sectoral approach. Through successful global health diplomacy and negotiations, this Caribbean declaration was elevated to a global level and resulted in the development of the declaration on the prevention and control of non-communicable diseases by the UN in September 2011 (
Chattu and Sakhamuri 2018). The CVDs were ranked as the leading cause of death during this decade, as shown below in
Table 2.
3.2.2. Diabetes
Diabetes is a major cause of death and concern in the region and has been increasing over the last decade (
Rivera-Andrade and Luna 2014). The Anglophone Caribbean is experiencing significant increases in obesity and diabetes levels. Although atypical diabetes is prevalent in this region, type 2 DM is the major public health burden, with prevalence rates that are higher than those reported in many developed countries. (
Boyne 2009). This burden is compounded by staggering projected incidence rates for obesity and, thus, diabetes. Thus, primary prevention measures (lifestyle interventions), active diabetes screening, and surveillance will be needed for the 21st century. Since the origins of diabetes may also begin from early life, more research is required to describe these mechanisms, as well as to introduce appropriate public health measures. These intervention strategies should probably be directed toward women of child-bearing age, as well as children. This would result in the perception that intervention for diabetes (and other chronic, non-communicable diseases) needs to occur throughout the life span. However, the precise nature of such interventions is indeterminate presently.
3.2.3. Cancer
Almost 1.1 million new cancer cases were estimated in Latin America and the Caribbean, with a total number of deaths estimated at around 600,000 (
Bray and Piñeros 2016). Overall, prostate, colorectal, and breast cancer are now the leading causes of cancer in the Caribbean, with higher rates of prostate cancer (PCa) incidence and mortality among black populations in this region. Changes in lifestyle factors, such as decreased fertility and birth rates, changes in tobacco smoking habits, and changes in diet, most likely explain the changing cancer profile in the Caribbean. Differences in diagnostic and treatment practices, access to healthcare and public health policy, could further explain the overall variations observed in the Caribbean (
Joachim et al. 2019).
3.3. Vulnerability to Current COVID-19 Pandemic and Other Infectious Disease Epidemics
With the rise of communicable diseases like COVID-19, Ebola, and Zika, it has been seen how these diseases threaten the well-being of citizens globally and affect the peace and development initiatives of many countries. Consequently, the well-being and protection of all human lives become critical and require a number of interconnecting and engaging bodies and partnerships in furtherance of GHD. As of 22 May 2020, COVID-19 has affected all the states and territories in the Caribbean (
Johns Hopkins University 2020) and has caused a great economic loss to the Caribbean region with over 20,742 infections and over 790 deaths (
Table 3). As a result of this crisis, many countries have closed their borders, stopped all the flights (incoming and outgoing) and cruise ships, and announced lockdowns in order to contain the epidemic. However, this has affected the CARICOM to a great extent as the region depends mostly on imports, income from tourism, and also creates a burden on their fragile health systems with frequent disasters and epidemics.
3.4. Addressing Any Epidemic/Health Security Threat through GHD
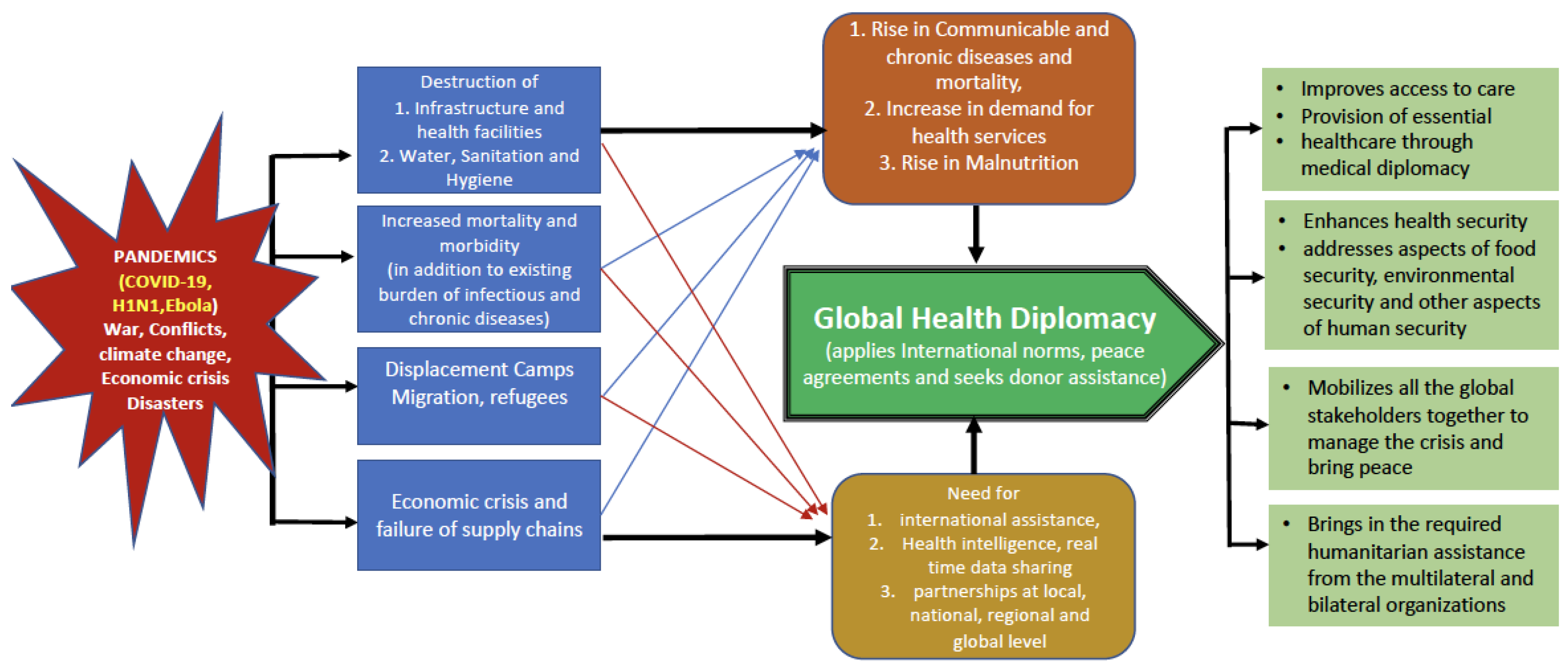
Health has become an issue of national security/global concern and GHD aids in the development of new bilateral or multilateral agreements to safeguard the health and well-being of people in a globalizing world. The health and well-being of citizens essentially emphasize the growing interlinkages between global health, diplomacy, and foreign policy. Given the history and prone for regular disasters and threats in the region, a hypothetical scenario depicted below (
Figure 2) explains how a typical emergency situation in any CARICOM nation can create complications and how these challenges can be addressed by multi-sectoral coordination and applying global governance frameworks through successful GHD based on the international norms and agreements. The CARICOM members can be successful in dealing effectively through their regional unity, existing partnerships with Latin America and North America, regional bodies such as Organization of American States and other bilateral and multilateral organizations working in the region by taking advantage of the existing norms, agreements and negotiate with donor agencies to get the necessary support in order to revive from the crisis situation. Hence, GHD holds great promise to address the needs of global health security through its binding or non-binding instruments enforced by global governance institutions. As such, CARICOM States must become equipped with the tools for effective health diplomacy.
4. Discussion
We examined the basic foundations of various approaches to global health diplomacy, along with their implications for the policies shaping the international public health and foreign policy environments. Increasing demands on global health diplomacy need a delicate mixture of technical expertise, legal knowledge, and diplomatic skills that have not been fully or thoroughly developed between the foreign service and global health professionals. A review by Birn and colleagues uncovered notable articulation of a set of values and strategies that characterize social justice oriented south–south cooperation compared to other types of health aid. The analysis was found to bear relevance for the conceptualization, policy development, and practice of equitable health cooperation, demonstrating that anti-hegemonic health solidarity is possible even amid considerable political constraints (
Birn et al. 2019). A recent review by Smith to identify factors affecting civil society influence in the pre-implementation stages of the policy process found that the power of civil society actors was enhanced when they joined strong epistemic networks and broader coalitions of stakeholders, were resourced, and framed issues in ways that resonated with national policies and political priorities (
Smith 2019). Williams and Rushton argue that the key contemporary discourses influencing Global Health Governance are biomedicine, human rights, economism, and security, but that other (currently recessive) discourses also have an influence. Though these discourses are promoted by different global health actors, who have gained salience in particular issue areas, the contemporary Global Health Governance is shaped by the interplay of these discourses—a process in which both power and ideas play a role (
Williams and Rushton 2009).
Today’s agenda in this globalized world includes a different range of issues, such as climate change, the growing burden of non-communicable diseases (NCDs), urban health, equity aspects in public health, food insecurity, the growing burden of refugee and forced migration, and strengthening comprehensive health systems to deliver the universal health coverage (UHC) and other United Nations Sustainable Development Goals (SDGs) is necessary.
CARICOM took the initiative for the establishment of PAHO Office of Caribbean Program Coordination (OCPC) in October 2005, which supports the Caribbean region in achieving the objectives of its health agenda, contributes to global and regional public health action and building Caribbean infrastructure and capacity with a focus on sustainability. Despite these achievements, many bottlenecks do exist for accessing care and affecting the well-being of the Caribbean people. As such, some recommendations can be proffered to improve the general health of the CARICOM region.
4.1. Establish a Critical Cadre of Leaders in GHD
The PAHO–OCPC considers the leadership element as a major priority of its agenda for the Caribbean region. Health leadership in the Caribbean in the face of a rapidly changing global environment is no longer confined to the traditional model of leadership solely undertaken by the medical profession. As Kickbusch pointed out earlier, there is a need for this cadre of global health diplomats who have a critical understanding of health and also the practice of diplomacy since such serious health issues have implications at the global level in this globalized world. (
Kickbusch et al. 2014). A study in Thailand concluded that for building capacity in GHD, it is essential to educate both health and non-health actors on global health issues and to use a combination of formal and informal mechanisms to participate in GHD. Additionally, in developing sustainable capacity in GHD, it requires long term commitment and strong leadership from both the health and non-health sectors (
Thaiprayoon and Smith 2015).
4.2. PAHO/WHO Alliances
It is critical that PAHO/WHO strengthens ties with all stakeholders and partners working on the development agenda within the region, ensuring the participation of every member. The acknowledgment and understanding of the historical roles of the cultural, economic, and political aspects unique to the CARICOM region are critical, especially as strategies are developed to protect and promote regional health and development.
4.3. Regional Partnerships for Peace and Health Development
Communication and community engagement: Strengthening the information, education, and communication (IEC) campaigns with a focused message to educate all the citizens. There is a great need for involving and working with civil society organizations and the private sector as well. For example, the Healthy Caribbean Coalition (HCC) was informally established following a multi-sectoral regional meeting in 2008 as a direct response to the POS Declaration’s call for a whole of society approach to the challenge of NCDs. HCC currently comprises over 100 health and non-health civil society organizations across the region and remains the only Caribbean NCD alliance. It works in NCD prevention and control with close regional and international leadership to leverage the power of civil society by strengthening and supporting its membership in the implementation of programs. In 2013, with support from the American Cancer Society, the HCC started to work with regional cancer societies to build capacity to effectively advocate for cervical cancer prevention. This has resulted in a collaboration with 23 cancer societies across CARICOM and the conduct of situational analyses in the region. Also, in partnership with PAHO, the HCC developed advocacy campaigns and formed the Caribbean Cancer Alliance (CCA), which further led a joint regional awareness campaign, namely, the Caribbean Civil Society Cervical Cancer Advocacy Initiative, which is a result of community and stakeholder engagement (
HCC 2020).
4.4. Promotion of Peace in the Region
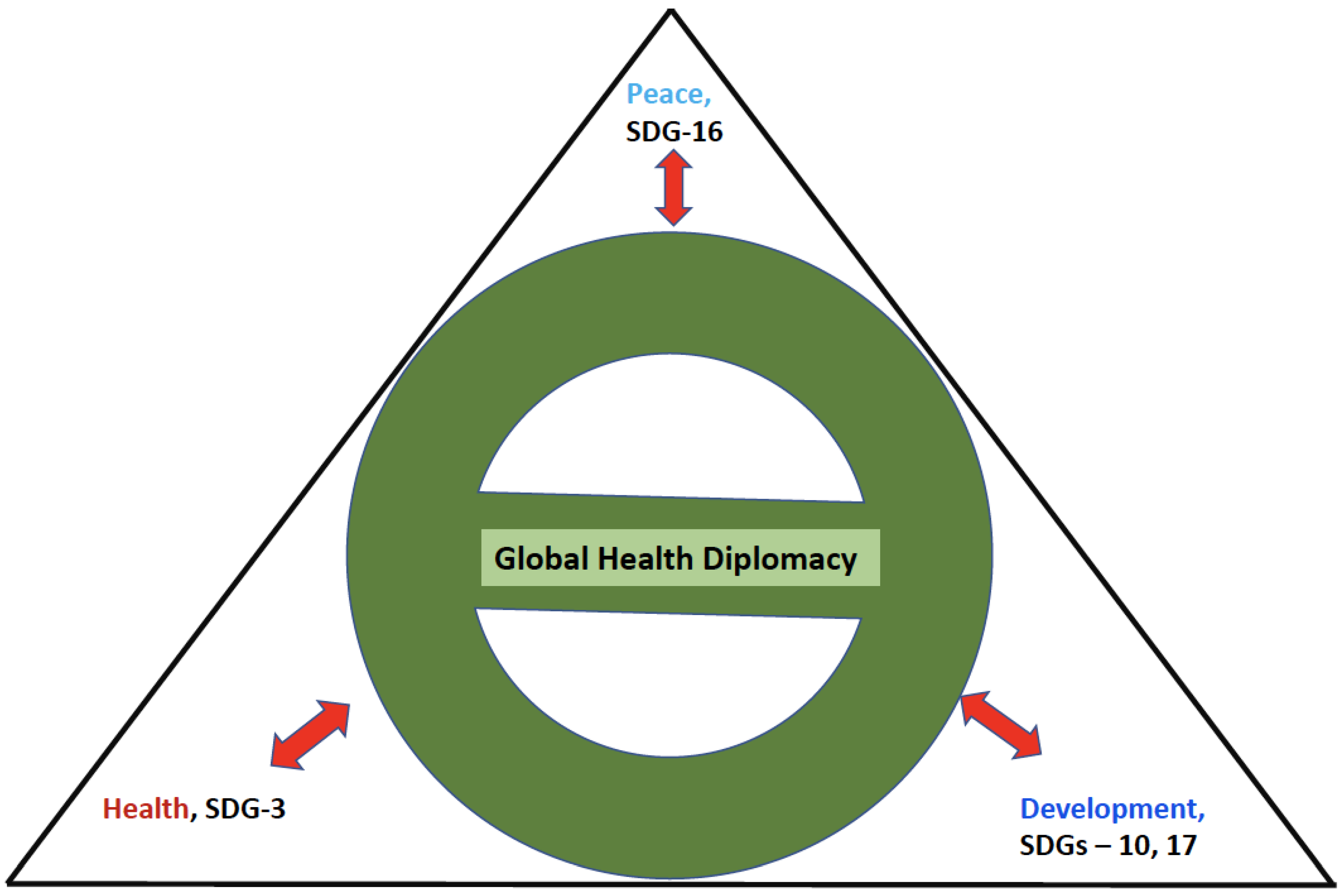
The CARICOM region has been facing a number of challenges on various fronts to tackle their economies, political instabilities, fragile systems, problems of refugees and migrants, and the devastating impacts of climate change. The declaration by UN Human Rights Council (
OHCHR 1948) emphasized “peace, development, health, security and human rights are interlinked and mutually reinforcing”, which is highlighted in the UN Sustainable Development Goals (SDGs) as the interrelated dimensions of “peace, health, and social development”. For example, SDG-3 emphasizes health and well- being, SDGs -10 and -17 focuses on development, and SDG-16 on peace, justice, and strong institutions. The interconnectedness between peace, health, and development is depicted below, where global health diplomacy acts as a dynamic wheel engaging with these dimensions (
Figure 3). The three domains provide a continuum for addressing the challenges posed by natural disasters, economic crises, and conflicts as these crisis situations offer an opportunity for professionals in international relations, development sector to become engaged with the health sector while simultaneously allowing global health experts to interact within the domain of diplomacy.
4.5. Strengthening Leadership, Governance, and Systems
Limited research resources, policy, and governance: Regional institutes such as CARPHA should play a more proactive and pivotal role in the creation of regional response teams in all the island nations collaborating with the departments of public health at The University of the West Indies located in different campuses in the region (Trinidad and Tobago, Jamaica, and Barbados) (
Chattu 2017).
The recent establishment of the Caribbean Center for Biosecurity at the University of the West Indies campus in Barbados is a great addition to improving health security in the region. It is aimed at reducing or eliminating biological threats that could adversely affect the Caribbean’s way of life and destabilize regional economies (
UWI 2018).
Lack of skilled health care personnel: Strengthening of surveillance and epidemic response team by having more qualified staff and improving training, equipment, laboratories, and containment. Strengthening and coordinating the preventive and control measures at ports of entry at all borders (illegal entry points too) so that the island community can be protected.
4.6. Collaboration with Global Health Institutions
The global health institutions need to play a lead role and assist the regional and individual states by reviewing the standard operating procedures, guidelines, and reinforce the effectiveness of the measures that are being implemented. The role of global health diplomacy and its practice should be encouraged to reach a consensus among the stakeholders to overcome the regional health security threats.
4.7. Promoting Digital Health and Providing Access to Quality Health Information
Digital health is fast emerging as one of the most defining trends of this decade and will have a profound influence on geopolitical and socioeconomic realities in the future (
Ranganathan 2020). Telemedicine offers an opportunity to improve health systems delivery, access, and efficiency. Telehealth and telemedicine in the Caribbean are at a relatively early stage, with a lack of cohesive telehealth strategies and policies which need to be strengthened in order to improve access to all its citizens, especially during this COVID-19 pandemic, with stringent public health measures in place. Essentially, it is important to emphasize that health information is an essential input for public health policy-making. Public health policy-making is highly reliant on the accessibility of sound data, which in return must be produced, investigated, and distributed through cohesive health information networks. A comprehensive health information system should function in a systemic manner, that is a structured process of collecting, sharing, examining, and using health-related data for critical decision-making and as a means of converting information into knowledge for action for the benefit of the region. Linked to the latter is the development of health technologies (HT) in the region. The lack of policies and standards to regulate the implementation and practice of HT, the underdevelopment of support technologies, and inequities in access to accessible HT. Therefore, for the region, telemedicine would be indispensable in creating futuristic and resilient health systems that can support the small island communities amidst pandemics, and by the technological innovations such as artificial intelligence and robotics, will have a long-term impact on future medicine to respond to future pandemics beyond the current pandemic.
4.8. Establishment of Regional Global Health Diplomacy Centre
The establishment of a regional Global Health Diplomacy Centre (GHDC) is key in conducting and improving research, training, and capacity building, focusing on global health governance and diplomacy for the Caribbean region. It would be a first of its kind for the region and echoes the broader trend in both the practice and analysis of global health, which focuses increasingly on the connection between health, foreign policy, trade, and development. This Centre would bring a better understanding of the regional global health in relation to the roles of government, private sector, and non-governmental organizations. Also, the Centre would enhance capability by engaging in research, knowledge acquisition and dissemination as well as by conducting wide-ranging training sessions and workshops in global health diplomacy for and with major stakeholders in the region.
Within the CARICOM region, the growing interdependence between countries has increased substantially in recent decades, with greater proximities in their social and health realities. As a result, these countries are increasingly sensitive to events in neighboring countries. In this context, health diplomacy serves as an appropriate instrument for collective action and for influencing the global determinants of health, as well as for the production of some key global public goods in health. The examples of regional partnerships, collaborations, and involvement of civil societies discussed in this article demonstrate the potential advantages of these integration processes for health. Hence in this context of CARICOM, the emerging challenges of health and health threats posed by infectious agents or man-made bio-attacks, there is a need for greater emphasis to “think locally and act regionally.”
As Buss and colleagues highlighted, the regional integration processes in health provide an opportunity to build a political health community with shared values and interests, joint efforts, coordination, and cooperation to manage the current health challenges and build a common agenda in order to guarantee the right to health for all the region’s inhabitants, e.g., the common efforts to achieve UN SDGs by 2030 (
Buss and Tobar 2018). Regionalism needs to reorient its mechanisms to promote the positive role of NGOs, individuals, and public–private partnerships for global health. Regionalism would also offer grounds for experimentation of global health diplomacy. As global health diplomacy is gaining in importance, negotiators should be well prepared. In this regard, some countries have added health attaché to their diplomatic staff and also diplomats to the staff of international health departments. Furthermore, the challenge is that increasingly rapid decisions and skillful negotiations are required in the face of outbreaks of disease, security threats, or other issues.
5. Conclusions
In an increasingly interdependent globalized world, it is critical for every country to live in a safe and healthy environment and ensure the well-being of its populations. Increasingly, there is the need for greater cooperation between global health experts and foreign policy practitioners to be well informed of their activities and by clearly drawing the link between these activities and the broader policy objectives of foreign policy. Global health proponents also have the space and opportunity to become more visible and to emphasize within diplomatic circles the health implications associated with climate change and human trafficking. Still, in light of the difficult financial and non-financial constraints faced by many donor countries and inherent tensions between foreign policy and global health objectives, the scope and influence of GHD going forward remain unpredictable. However, if global health and foreign policy practitioners collaborate for greater mutual understanding and coordination, the conditions can be created for all parties to benefit from the growing importance of GHD.
Recommendations
To have established centers dedicated to the promotion of GHD for the Caribbean. Centers can be established at (1) the Center for Biosecurity, the University of the West Indies, Cave Hill Campus Barbados, Trinidad and Tobago, St. Augustine Campus (2) the Diplomatic Academy of the Caribbean (DAOC), the University of the West Indies, St. Augustine campus, in collaboration with national/regional agencies to conduct workshops, training sessions, and regular webinars on GHD. To invest in developing a center for excellence with a multidisciplinary team foreseeing the emergencies/disasters/epidemics and ensure preparedness. Additionally, to represent at a global level and influence the global platforms for issues like climate change, pandemic preparedness, and anti-microbial resistance to combat the issues effectively.







{kind=link}
{kind=link}
{kind=link}