An Ultra-Sensitive Technique: Using Pv-mtCOX1 qPCR to Detect Early Recurrences of Plasmodium vivax in Patients in the Brazilian Amazon

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Pv-mtCOX1 qPCR, Pv 18S rRNA qPCR and Thick Blood Smear Agreement Results
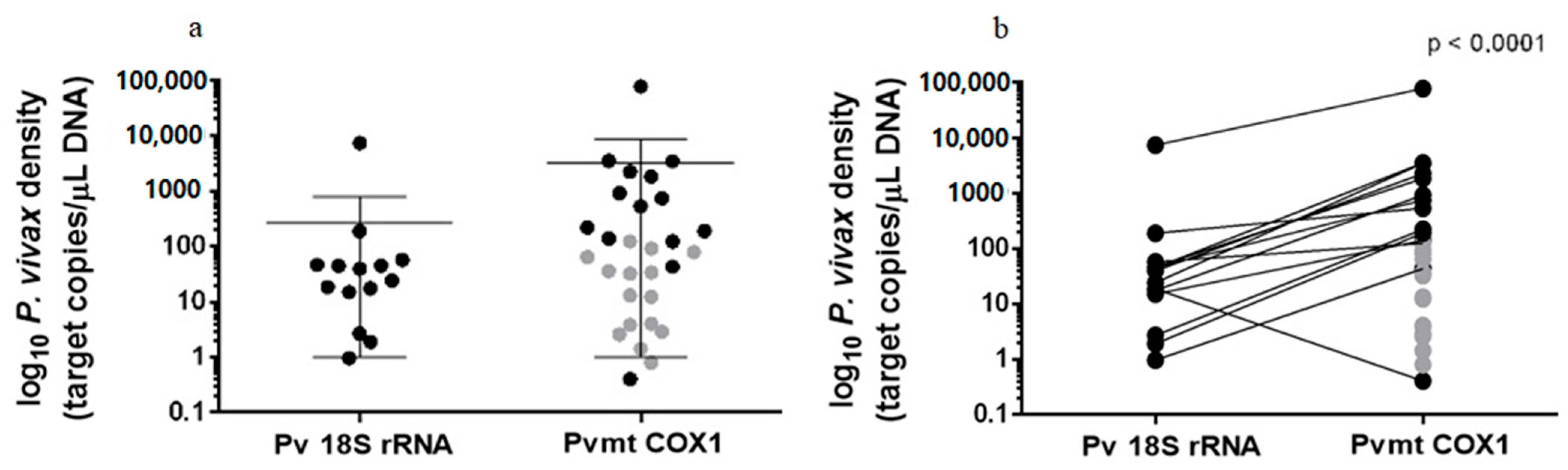
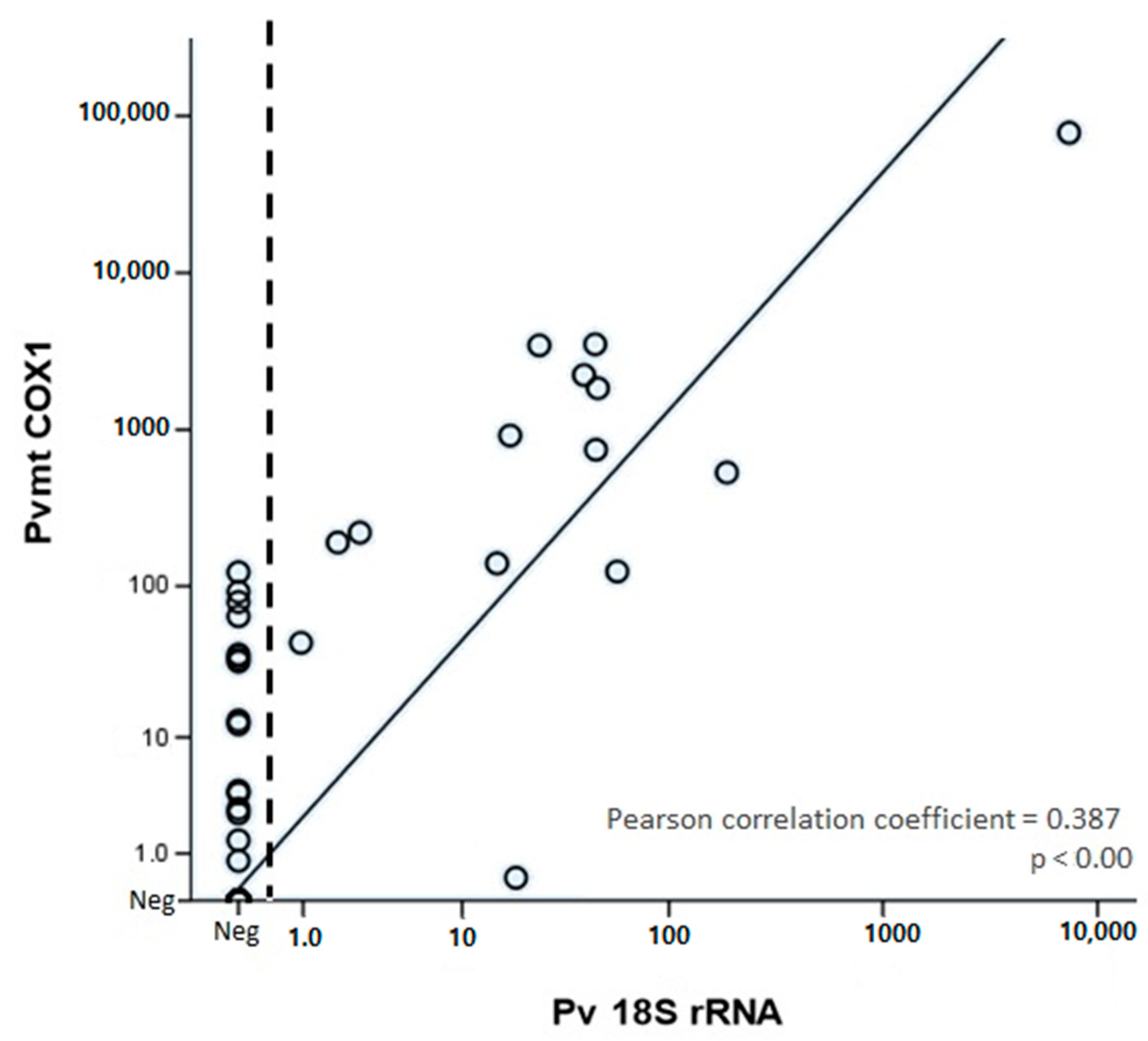
2.2. Parasitological Quantifications
2.3. Risk Factors
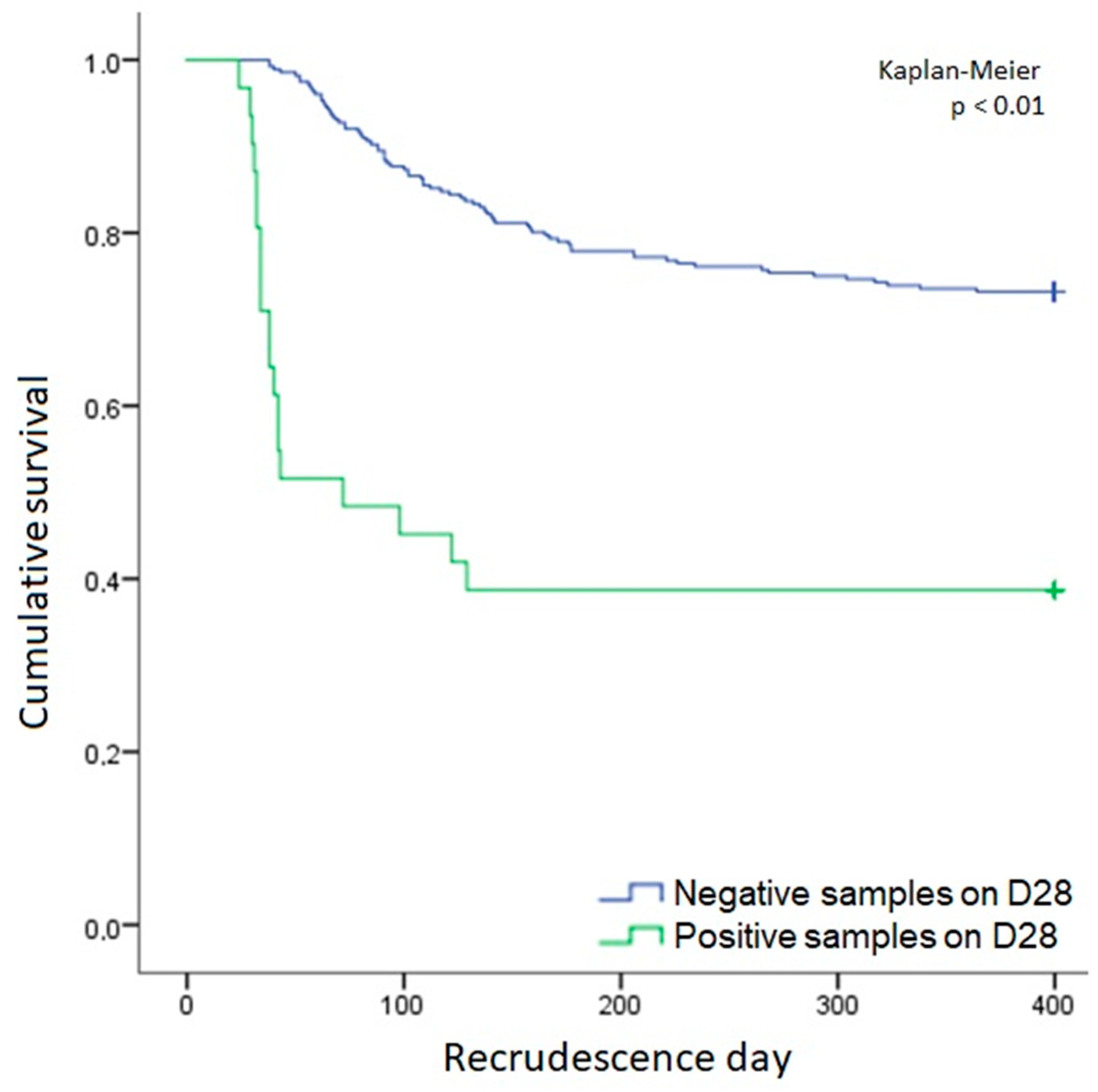
2.4. Symptomatic Recurrences
3. Discussion
4. Material and Methods
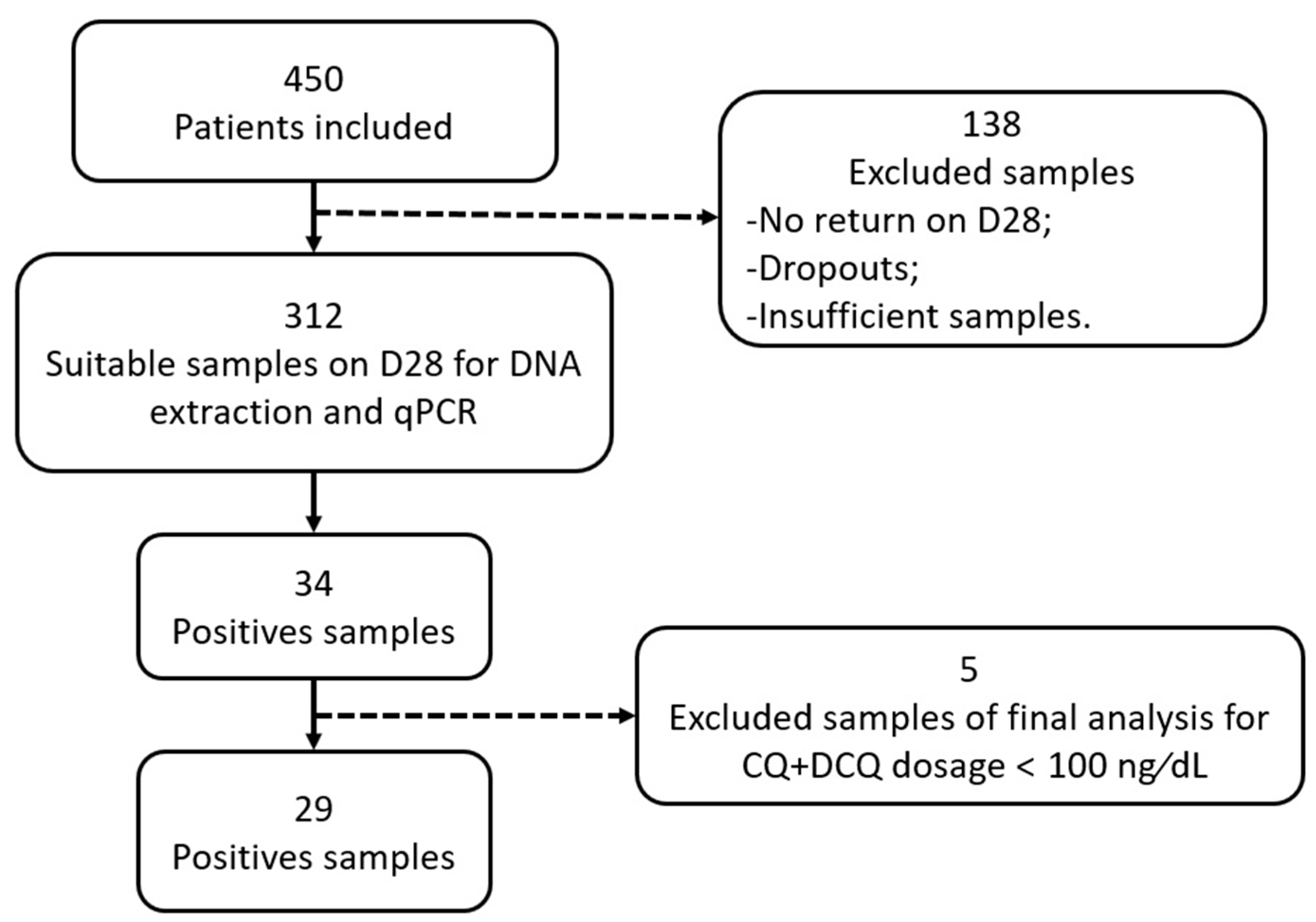
4.1. Ethics Statement, Study Site and Selection of Patients
4.2. P. vivax Malaria Diagnosis by Thick Smears
4.3. Detection of Plasmodium spp. By qPCR
4.4. CQ and DCQ Level
4.5. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Malaria Report 2019. Available online: https://www.who.int/publications-detail-redirect/9789241565721 (accessed on 18 September 2020).
- Rieckmann, K.H.; Davis, D.R.; Hutton, D.C. Plasmodium vivax resistance to chloroquine? Lancet 1989, 334, 1183–1184. [Google Scholar] [CrossRef]
- Price, R.N.; Douglas, N.M.; Anstey, N.M. New developments in Plasmodium vivax malaria: Severe disease and the rise of chloroquine resistance. Curr. Opin. Infect. Dis. 2009, 22, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Marques, M.M.; Costa, M.R.F.; Santana Filho, F.S.; Vieira, J.L.F.; Nascimento, M.T.S.; Brasil, L.W.; Nogueira, F.; Silveira, H.; Reyes-Lecca, R.C.; Monteiro, W.M.; et al. Plasmodium vivax Chloroquine Resistance and Anemia in the Western Brazilian Amazon. Antimicrob. Agents Chemother. 2014, 58, 342–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alecrim, M.D.; Alecrim, W.; Macêdo, V. Plasmodium vivax resistance to chloroquine (R2) and mefloquine (R3) in Brazilian Amazon region. Rev. Soc. Bras. Med. Trop. 1999, 32, 67–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Santana Filho, F.S.; de Lima Arcanjo, A.R.; Chehuan, Y.M.; Costa, M.R.; Martinez-Espinosa, F.E.; Vieira, J.L.; Barbosa, M.d.G.V.; Alecrim, W.D.; Alecrim, M.D. Chloroquine-Resistant Plasmodium vivax, Brazilian Amazon. Emerg. Infect. Dis. 2007, 13, 1125–1126. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, A.M.; Alencar, A.C.; Melo, G.C.; Magalhaes, B.L.; Machado, K.; Alencar Filho, A.C.; Kuehn, A.; Marques, M.M.; Manso, M.C.; Felger, I.; et al. Fixed-Dose Artesunate–Amodiaquine Combination vs Chloroquine for Treatment of Uncomplicated Blood Stage P. vivax Infection in the Brazilian Amazon: An Open-Label Randomized, Controlled Trial. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 64, 166–174. [Google Scholar] [CrossRef]
- Baird, J.K.; Leksana, B.; Masbar, S.; Fryauff, D.J.; Sutanihardja, M.A.; Suradi; Wignall, F.S.; Hoffman, S.L. Diagnosis of Resistance to Chloroquine by Plasmodium vivax: Timing of Recurrence and Whole Blood Chloroquine Levels. Am. J. Trop. Med. Hyg. 1997, 56, 621–626. [Google Scholar] [CrossRef]
- Hwang, J.; Alemayehu, B.H.; Reithinger, R.; Tekleyohannes, S.G.; Takele, T.; Birhanu, S.G.; Demeke, L.; Hoos, D.; Melaku, Z.; Kassa, M.; et al. In Vivo Efficacy of Artemether-Lumefantrine and Chloroquine against Plasmodium vivax: A Randomized Open Label Trial in Central Ethiopia. PLoS ONE 2013, 8. [Google Scholar] [CrossRef]
- WHO. Safe and Rational Clinical Use of Blood; World Health Organization: Geneva, Switzerland, 2018; Available online: http://www.who.int/bloodsafety/clinical_use/en/ (accessed on 6 November 2018).
- Cunha, M.G.; Medina, T.S.; Oliveira, S.G.; Marinho, A.N.; Póvoa, M.M.; Ribeiro-dos-Santos, A.K.C. Development of a Polymerase Chain Reaction (PCR) method based on amplification of mitochondrial DNA to detect Plasmodium falciparum and Plasmodium vivax. Acta Trop. 2009, 111, 35–38. [Google Scholar] [CrossRef]
- Hofmann, N.E.; Gruenberg, M.; Nate, E.; Ura, A.; Rodriguez-Rodriguez, D.; Salib, M.; Mueller, I.; Smith, T.A.; Laman, M.; Robinson, L.J.; et al. Assessment of ultra-sensitive malaria diagnosis versus standard molecular diagnostics for malaria elimination: An in-depth molecular community cross-sectional study. Lancet Infect. Dis. 2018. [Google Scholar] [CrossRef]
- Gruenberg, M.; Moniz, C.A.; Hofmann, N.E.; Wampfler, R.; Koepfli, C.; Mueller, I.; Monteiro, W.M.; Lacerda, M.; de Melo, G.C.; Kuehn, A.; et al. Plasmodium vivax molecular diagnostics in community surveys: Pitfalls and solutions. Malar. J. 2018, 17. [Google Scholar] [CrossRef] [PubMed]
- Britton, S.; Cheng, Q.; Grigg, M.J.; Poole, C.B.; Pasay, C.; William, T.; Fornace, K.; Anstey, N.M.; Sutherland, C.J.; Drakeley, C.; et al. Sensitive Detection of Plasmodium vivax Using a High-Throughput, Colourimetric Loop Mediated Isothermal Amplification (HtLAMP) Platform: A Potential Novel Tool for Malaria Elimination. PLoS Negl. Trop. Dis. 2016, 10, e0004443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruenberg, M.; Moniz, C.A.; Hofmann, N.E.; Koepfli, C.; Robinson, L.J.; Nate, E.; Monteiro, W.M.; de Melo, G.C.; Kuehn, A.; Siqueira, A.M.; et al. Utility of ultra-sensitive qPCR to detect Plasmodium falciparum and Plasmodium vivax infections under different transmission intensities. Malar. J. 2020, 19, 319. [Google Scholar] [CrossRef] [PubMed]
- Preiser, P.R.; Wilson, R.J.; Moore, P.W.; McCready, S.; Hajibagheri, M.A.; Blight, K.J.; Strath, M.; Williamson, D.H. Recombination Associated with Replication of Malarial Mitochondrial DNA. EMBO J. 1996, 15, 684–693. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.; Joshi, S.N.; Mbambo, G.; Mu, A.Z.; Roemmich, S.M.; Shrestha, B.; Strauss, K.A.; Johnson, N.E.; Oo, K.Z.; Hlaing, T.M.; et al. An ultrasensitive reverse transcription polymerase chain reaction assay to detect asymptomatic low-density Plasmodium falciparum and Plasmodium vivax infections in small volume blood samples. Malar. J. 2015, 14, 520. [Google Scholar] [CrossRef] [Green Version]
- Imwong, M.; Hanchana, S.; Malleret, B.; Rénia, L.; Day, N.P.J.; Dondorp, A.; Nosten, F.; Snounou, G.; White, N.J. High-Throughput Ultrasensitive Molecular Techniques for Quantifying Low-Density Malaria Parasitemias. J. Clin. Microbiol. 2014, 52, 3303–3309. [Google Scholar] [CrossRef] [Green Version]
- Mckenzie, F.E.; Wongsrichanalai, C.; Magill, A.J.; Forney, J.R.; Permpanich, B.; Lucas, C.; Erhart, L.M.; O’Meara, W.P.; Smith, D.L.; Sirichaisinthop, J.; et al. Gametocytemia in Plasmodium vivax and Plasmodium Falciparum Infections. J. Parasitol. 2006, 92, 1281–1285. [Google Scholar] [CrossRef]
- Martins-Campos, K.M.; Kuehn, A.; Almeida, A.; Duarte, A.P.M.; Sampaio, V.S.; Rodriguez, Í.C.; da Silva, S.G.M.; Ríos-Velásquez, C.M.; Lima, J.B.P.; Pimenta, P.F.P.; et al. Infection of Anopheles aquasalis from symptomatic and asymptomatic Plasmodium vivax infections in Manaus, western Brazilian Amazon. Parasit. Vectors 2018, 11. [Google Scholar] [CrossRef]
- Almeida, A.C.G.; Kuehn, A.; Castro, A.J.M.; Vitor-Silva, S.; Figueiredo, E.F.G.; Brasil, L.W.; Brito, M.A.M.; Sampaio, V.S.; Bassat, Q.; Felger, I.; et al. High proportions of asymptomatic and submicroscopic Plasmodium vivax infections in a peri-urban area of low transmission in the Brazilian Amazon. Parasit. Vectors 2018, 11. [Google Scholar] [CrossRef] [Green Version]
- Phommasone, K.; van Leth, F.; Imwong, M.; Henriques, G.; Pongvongsa, T.; Adhikari, B.; Peto, T.J.; Promnarate, C.; Dhorda, M.; Sirithiranont, P.; et al. The use of ultrasensitive quantitative-PCR to assess the impact of primaquine on asymptomatic relapse of Plasmodium vivax infections: A randomized, controlled trial in Lao PDR. Malar. J. 2020, 19, 4. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.T.; Patel, J.C.; Levitz, L.; Wojnarski, M.; Chaorattanakawee, S.; Gosi, P.; Buathong, N.; Chann, S.; Rekol, H.; Thay, K.; et al. Gametocyte Carriage, Antimalarial Use, and Drug Resistance in Cambodia, 2008–2014. Am. J. Trop. Med. Hyg. 2018, 99, 1145–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douglas, N.M.; Simpson, J.A.; Phyo, A.P.; Siswantoro, H.; Hasugian, A.R.; Kenangalem, E.; Poespoprodjo, J.R.; Singhasivanon, P.; Anstey, N.M.; White, N.J.; et al. Gametocyte Dynamics and the Role of Drugs in Reducing the Transmission Potential of Plasmodium vivax. J. Infect. Dis. 2013, 208, 801–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministério da Saúde, Secretaria de Vigilância em Saúde. Departamento de Imunização Guia Prático de Tratamento da Malária no Brasil; Ministério da Saúde, Secretaria de Vigilância em Saúde: Brasília, Brazil, 2020.
- WHO. World Malaria Report 2017; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Dua, V.K.; Kar, P.K.; Gupta, N.C.; Sharma, V.P. Determination of chloroquine and desethylchloroquine in plasma and blood cells of Plasmodium vivax malaria cases using liquid chromatography. J. Pharm. Biomed. Anal. 1999, 21, 199–205. [Google Scholar] [CrossRef]
- Patchen, L.C.; Mount, D.L.; Schwartz, I.K.; Churchill, F.C. Analysis of filter-paper-absorbed, finger-stick blood samples for chloroquine and its major metabolite using high-performance liquid chromatography with fluorescence detection. J. Chromatogr. 1983, 278, 81–89. [Google Scholar] [CrossRef]
- Price, R.N.; von Seidlein, L.; Valecha, N.; Nosten, F.; Baird, J.K.; White, N.J. Global extent of chloroquine-resistant Plasmodium vivax: A systematic review and meta-analysis. Lancet Infect. Dis. 2014, 14, 982–991. [Google Scholar] [CrossRef] [Green Version]
- WHO. Methods for Surveillance of Antimalarial Drug Efficacy; World Health Organization: Geneva, Switzerland, 2009; Available online: https://www.who.int/docs/default-source/documents/publications/gmp/methods-for-surveillance-of-antimalarial-drug-efficacy.pdf?sfvrsn=29076702_2 (accessed on 18 September 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Sample size | 307 |
| Mean age, years (SD) | 39.4 (14.3) |
| No. of males (%) | 215 (70) |
| Parasite geometric mean D0 per mm3 (SD) | 3781.6 (4109.2) |
| No. with presence of gametocytes D0 under microscopy (%) | 259 (84.4) |
| Mean hemoglobin in D0, g/dL (SD) a | 13.4 (1.7) |
| Mean hemoglobin in D28, g/dL (SD) a | 13.6 (1.1) |
| No. with anemia (%) a,b | 57 (27.5) |
| Factor | Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| Odds Ratio | 95% Confidence Interval | p-Value | Adjusted Odds Ratio | 95% Confidence Interval | p-Value | |||
| Lower | Upper | Lower | Upper | |||||
| Male gender | 0.72 | 0.30 | 1.76 | 0.471 | 0.91 | 0.29 | 2.84 | 0.872 |
| Presence of gametocytes under microscopy | 3.98 | 1.51 | 9.54 | 0.001 | 3.64 | 1.10 | 12.08 | 0.035 |
| Asexual parasites > 5000/mm3 | 2.14 | 0.72 | 6.37 | 0.161 | 1.03 | 0.26 | 4.03 | 0.968 |
| Anemia D0 a,b | 1.65 | 0.42 | 5.76 | 0.497 | 1.51 | 0.40 | 5.73 | 0.541 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbosa, L.R.A.; da Silva, E.L.; de Almeida, A.C.G.; Salazar, Y.E.A.R.; Siqueira, A.M.; Alecrim, M.d.G.C.; Vieira, J.L.F.; Bassat, Q.; de Lacerda, M.V.G.; Monteiro, W.M.; et al. An Ultra-Sensitive Technique: Using Pv-mtCOX1 qPCR to Detect Early Recurrences of Plasmodium vivax in Patients in the Brazilian Amazon. Pathogens 2021, 10, 19. https://doi.org/10.3390/pathogens10010019
Barbosa LRA, da Silva EL, de Almeida ACG, Salazar YEAR, Siqueira AM, Alecrim MdGC, Vieira JLF, Bassat Q, de Lacerda MVG, Monteiro WM, et al. An Ultra-Sensitive Technique: Using Pv-mtCOX1 qPCR to Detect Early Recurrences of Plasmodium vivax in Patients in the Brazilian Amazon. Pathogens. 2021; 10(1):19. https://doi.org/10.3390/pathogens10010019
Chicago/Turabian StyleBarbosa, Laila R. A., Emanuelle L. da Silva, Anne C. G. de Almeida, Yanka E. A. R. Salazar, André M. Siqueira, Maria das Graças Costa Alecrim, José Luiz Fernandes Vieira, Quique Bassat, Marcus V. G. de Lacerda, Wuelton M. Monteiro, and et al. 2021. "An Ultra-Sensitive Technique: Using Pv-mtCOX1 qPCR to Detect Early Recurrences of Plasmodium vivax in Patients in the Brazilian Amazon" Pathogens 10, no. 1: 19. https://doi.org/10.3390/pathogens10010019
APA StyleBarbosa, L. R. A., da Silva, E. L., de Almeida, A. C. G., Salazar, Y. E. A. R., Siqueira, A. M., Alecrim, M. d. G. C., Vieira, J. L. F., Bassat, Q., de Lacerda, M. V. G., Monteiro, W. M., & Melo, G. C. (2021). An Ultra-Sensitive Technique: Using Pv-mtCOX1 qPCR to Detect Early Recurrences of Plasmodium vivax in Patients in the Brazilian Amazon. Pathogens, 10(1), 19. https://doi.org/10.3390/pathogens10010019