
Chloroquine and Hydroxychloroquine: Efficacy in the Treatment of the COVID-19


 , , ,
, , ,  and
and 
Abstract
:1. Introduction
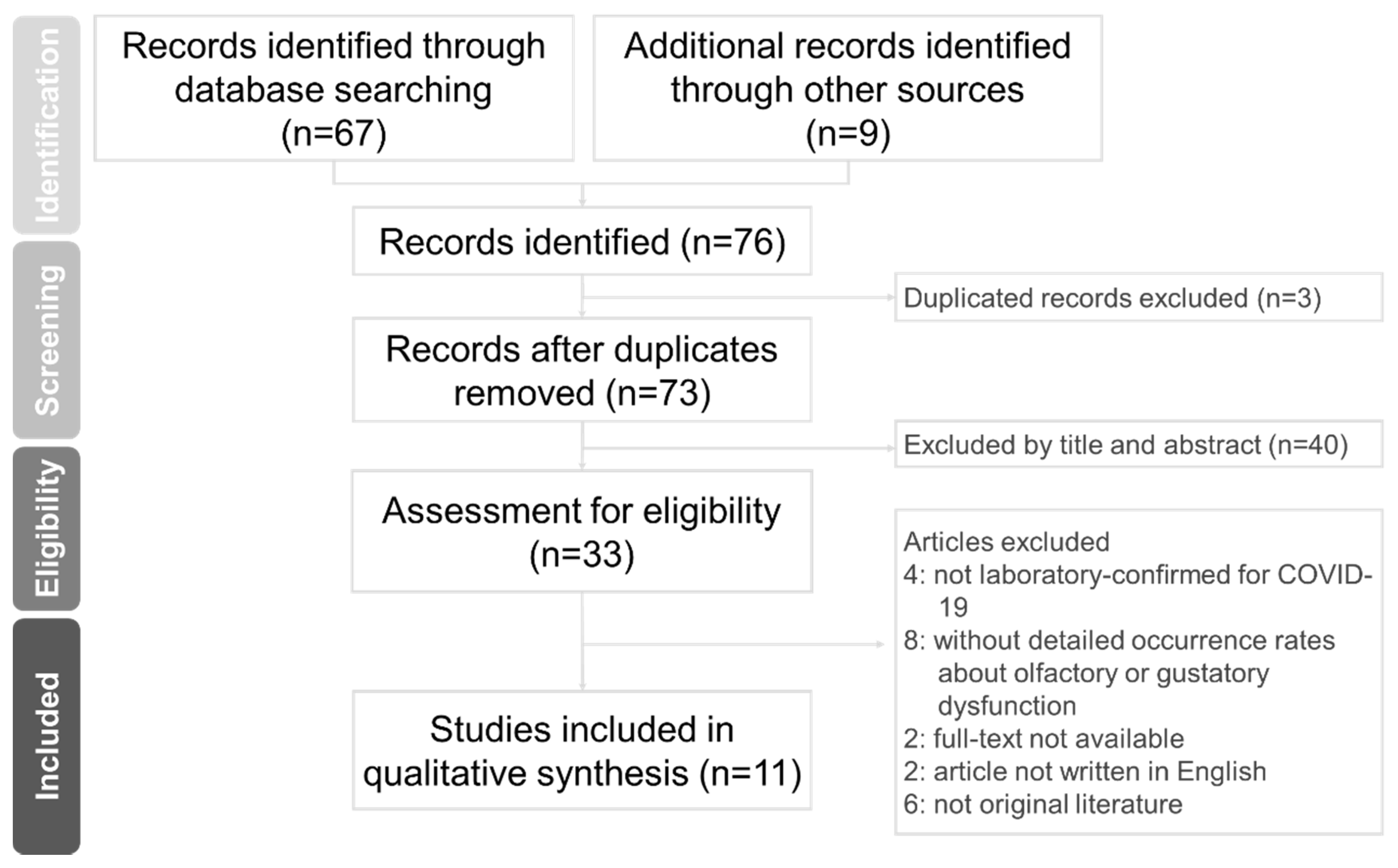
2. Method
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Disclosure Statement
Conflicts of Interest
References
- Ksiazek, T.G.; Erdman, D.; Goldsmith, C.S.; Zaki, S.R.; Peret, T.; Emery, S.; Tong, S.; Urbani, C.; Comer, J.A.; Lim, W.; et al. A Novel Coronavirus Associated with Severe Acute Respiratory Syndrome. N. Engl. J. Med. 2003, 348, 1953–1966. [Google Scholar] [CrossRef] [PubMed]
- Van der Hoek, L. Human coronaviruses: What do they cause? Antivir. Ther. 2007, 12, 651–658. [Google Scholar] [PubMed]
- Zhong, N.S.; Zheng, B.J.; Li, Y.M.; Poon, L.; Xie, Z.H.; Chan, K.H.; Li, P.H.; Tan, S.Y.; Chang, Q.; Xie, J.P.; et al. Epidemiology and cause of severe acute respiratory syndrome (SARS) in Guangdong, People’s Republic of China, in February, 2003. Lancet 2003, 362, 1353–1358. [Google Scholar] [CrossRef] [Green Version]
- Zaki, A.; Van Boheemen, S.; Bestebroer, T.; Osterhaus, A.; Fouchier, R. Isolation of a Novel Coronavirus from a Man with Pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Shi, N.; Shan, F.; Zhang, Z.; Shen, J.; Lu, H.; Ling, Y.; Jiang, Y.; Shi, Y. Emerging 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 11 February 2020).
- Petrosillo, N.; Viceconte, G.; Ergonul, O.; Ippolito, G.; Petersen, E. COVID-19, SARS and MERS: Are they closely related? Clin. Microbiol. Infect. 2020, 26, 729–734. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 4 February 2021).
- Lei, Z.-N.; Wu, Z.-X.; Dong, S.; Yang, D.-H.; Zhang, L.; Ke, Z.; Zou, C.; Chen, Z.-S. Chloroquine and hydroxychloroquine in the treatment of malaria and repurposing in treating COVID-19. Pharmacol. Ther. 2020, 216, 107672. [Google Scholar] [CrossRef]
- Liu, J.; Cao, R.; Xu, M.; Wang, X.; Zhang, H.; Hu, H.; Li, Y.; Hu, Z.; Zhong, W.; Wang, M. Hydroxychloroquine, a less toxic derivative of chloroquine, is effective in inhibiting SARS-CoV-2 infection In Vitro. Cell Discov. 2020, 6, 16. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) In Vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- Yao, X.; Ye, F.; Zhang, M.; Cui, C.; Huang, B.; Niu, P.; Liu, X.; Zhao, L.; Dong, E.; Song, C.; et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 71, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Oscanoa, T.J.; Romero-Ortuno, R.; Carvajal, A.; Savarino, A. A pharmacological perspective of chloroquine in SARS-CoV-2 infection: An old drug for the fight against a new coronavirus? Int. J. Antimicrob. Agents. 2020, 56, 106078. [Google Scholar] [CrossRef] [PubMed]
- Hickley, N.M.; Al-Maskari, A.; McKibbin, M. Chloroquine and hydroxychloroquine toxicity. Arch. Ophthalmol. 2011, 129, 1506–1507. [Google Scholar] [CrossRef] [PubMed]
- Gautret, P.; Lagier, J.C.; Parola, P.; Meddeb, L.; Sevestre, J.; Mailhe, M.; Doudier, B.; Aubry, C.; Amrane, S.; Seng, P.; et al. Clinical and microbiological effect of a combination of hydroxychloroquine and azithro-mycin in 80 COVID-19 patients with at least a six-day follow up: A pilot observational study. Travel Med. Infect. Dis. 2020, 34, 101663. [Google Scholar] [CrossRef]
- Gao, J.; Tian, Z.; Yang, X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associ-ated pneumonia in clinical studies. Biosci. Trends. 2020, 14, 72–73. [Google Scholar] [CrossRef] [Green Version]
- Tang, W.; Cao, Z.; Han, M.; Wang, Z.; Chen, J.; Sun, W.; Wu, Y.; Xiao, W.; Liu, S.; Chen, E.; et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: Open label, randomised controlled trial. BMJ 2020, 369, m1849. [Google Scholar] [CrossRef]
- Mahévas, M.; Tran, V.T.; Roumier, M.; Chabrol, A.; Paule, R.; Guillaud, C.; Gallien, S.; Lepeule, R.; Szwebel, T.A.; Lescure, X.; et al. No evidence of clinical efficacy of hydroxychloroquine in patients hospitalised for COVID-19 infection and requiring oxygen: Results of a study using routinely collected data to emulate a target trial. medRxiv 2020, 20060699. [Google Scholar] [CrossRef] [Green Version]
- Magagnoli, J.; Narendran, S.; Pereira, F.; Cummings, T.H.; Hardin, J.W.; Sutton, S.S.; Ambati, J. Outcomes of Hydroxychloroquine Usage in United States Veterans Hospitalized with COVID-19. medRxiv 2020, 1, 114–127. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Molina, J.; Delaugerre, C.; Le Goff, J.; Mela-Lima, B.; Ponscarme, D.; Goldwirt, L.; De Castro, N. No evidence of rapid antiviral clearance or clinical benefit with the combination of hydroxychloroquine and azithromycin in patients with severe COVID-19 infection. Méd. Mal. Infect. 2020, 50, 384. [Google Scholar] [CrossRef]
- Chen, Z.W.; Hu, J.J.; Zhang, Z.W.; Jiang, S.; Han, S.; Yan, D.; Zhuang, R.; Hu, B.; Zhang, Z. Efficacy of hydroxychloroquine in patients with COVID-19: Results of a randomized clinical trial. Preprint. medRxiv 2020, 20040758. [Google Scholar] [CrossRef] [Green Version]
- Borba, M.G.S.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.A.A.; Melo, G.C.; Brito, M.; Mourão, M.P.G.; Brito-Sousa, J.D.; Baía-da-Silva, D.; Guerra, M.V.F.; et al. Effect of High vs Low Doses of Chloroquine Diphosphate as Adjunctive Therapy for Patients Hospitalized With Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e208857. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 RISK and Treatments (CORIST) Collaboration. Use of hydroxychloroquine in hospitalised COVID-19 patients is associated with reduced mortality: Findings from the observational multicentre Italian CORIST study. Eur. J. Intern. Med. 2020, 82, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Catteau, L.; Dauby, N.; Montourcy, M.; Bottieau, E.; Hautekiet, J.; Goetghebeur, E.; Van Ierssel, S.; Duysburgh, E.; Van Oyen, H.; Wyndham-Thomas, C.; et al. Low-dose hydroxychloroquine therapy and mortality in hospitalised patients with COVID-19: A nationwide observational study of 8075 participants. Int. J. Antimicrob. Agents 2020, 56, 106144. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Mösbauer, K.; Hofmann-Winkler, H.; Kaul, A.; Kleine-Weber, H.; Krüger, N.; Gassen, N.C.; Müller, M.A.; Drosten, C.; Pöhlmann, S. Chloroquine does not inhibit infection of human lung cells with SARS-CoV-2. Nat. Cell Biol. 2020, 585, 1–5. [Google Scholar] [CrossRef]
- Yam, J.C.S.; Kwok, A.K.H. Ocular toxicity of hydroxychloroquine. Hong Kong Med. J. 2006, 12, 294–304. [Google Scholar]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Stokes, E.K.; Zambrano, L.D.; Anderson, K.N.; Marder, E.P.; Raz, K.M.; Felix, S.E.B.; Tie, Y.; Fullerton, K.E. Coronavirus Disease 2019 Case Surveillance—United States, 22 January–30 May 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 759–765. [Google Scholar] [CrossRef]
- Hamed, I.; Shaban, N.; Nassar, M.; Cayir, D.; Love, S.; Curran, M.D.; Webb, S.; Yang, H.; Watson, K.; Rostron, A.; et al. Paired Nasopharyngeal and Deep Lung Testing for Severe Acute Respiratory Syndrome Coronavirus-2 Reveals a Viral Gradient in Critically Ill Patients: A Multicenter Study. Chest 2021, S0012-3692(20)34909-6. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference | Institution/Country Study Conducted | Design | No. of Participants | Intervention | Results |
|---|---|---|---|---|---|
| Gao, J. et al. (2020) [16] | 10 hospitals in China in the cities of Wuhan, Jingzhou, Guangzhou, Beijing, Shanghai, Chungging, and Ningbo | Observational study | N = 100 Control group: unlisted Experimental group: unlisted | Unknown | Compared to the control group, CQ improves lung imaging findings, inhibits the exacerbation of pneumonia, and promotes a virus-negative conversion |
| Magagnoli, J. et al. (2020) [19] | Veterans Health Administration medical centers across the USA | Observational study | N = 807 Control group: no HCQ (n = 395) Experimental group: HCQ alone (n = 198) HCQ + AZ (n = 214) | HCQ alone: 400 mg/daily for 5 days HCQ + AZ: 422.2 mg/daily for 5 days. | Most of participants have chronic disease, such as diabetes and cancer. Compared to the control group, mortality risk is no significantly different in the HCQ group or in the HCQ + AZ group. The HCQ + AZ group has an increased risk of cardiac arrest. |
| Zhaowei, C et al. (2020) [22] | Hospital of Wuhan University, Wuhan, China | RCT | N = 62 Control group: No HCQ + SOC (n = 31) Experimental group: HCQ + SOC (n = 31) | HCQ, 200 mg, twice daily for 5 days | Severe COVID-19 patients are not enrolled in this study. Compared to the control group, the HCQ group (80.6%, 25/31) have pneumonia improvement and a shorter recovery time for clinical symptoms such as fever and cough. 2 patients in the HCQ group have mild adverse reactions such as rashes and headaches. |
| Mahevas, M. et al. (2020) [18] | 4 French tertiary care centers, France | Observational study | N = 181 Control group: no HCQ (n = 97) Experimental group: HCQ (n = 84) | HCQ, 600 mg/daily for 5 days (starting within 48 h after hospital admission) | The ratios of ICU admission, morality and ARDS development are not significantly different between the no HCQ group and the HCQ group. 8 patients in the HCQ group have electrocardiogram modifications and then HCQ discontinuation. |
| Gautret, P. et al. (2020) [15] | University Hospital Institute Méditerranée Infection in Marseille, France. | Observation study | N = 80 Control group: Not recruited Experimental group: HCQ + AZ (n = 80, 6 patients from a pervious study) | HCQ, 200 mg thrice daily for 10 days AZ, 500mg/daily for D1 and 250mg/daily for the D2 to D5 | 81.3% (65/80) of patients have a favorable outcome and are rapidly discharged from the hospital (mean of the discharged day: 4.1 days). |
| Gautret, P. et al. (2020) [20] | 4 centers in Southern France in cities of Marseille, Nice, Avignon and Briançon | Open-label, non-RCT | N = 32 Control group: no HCQ (n = 16) Experimental group: HCQ (n = 20) All group are further classified into three subgroups: asymptomatic, URTI and LRTI. | HCQ, 200 mg, thrice daily for 10 days 6 patients in HCQ group with combination of AZ (500 mg on D1 followed by 250 mg/daily for the D2 to D5) for prevention of bacterial infection | 6 days after treatment, the ratio of viral clearance in the HCQ + AZ group, HCQ alone group, and a control group is 100%, 57.1%, and 12.5%, respectively. |
| Tang, W. et al. (2020) [17] | Ruijin Hospital in Shanghai, China | Open label, RCT, Multicenter | N = 150 Control group: no HCQ + SOC (n = 80) Experimental group: HCQ + SOC (n = 70) | HCQ, 1200 mg/daily on D1 to D3 followed by 800 mg/daily for 2 to 3 weeks SOC, treatment includes another antiviral drug such as arbidol, virazole, lopinavir-ritonavir, oseltamivir, entecavir | 98.6% (148/150) of patients have mild or moderate COVID-19 cases. Comparted to the control group, the rate of negative virus conversion is not significantly different in the HCQ + SOC group. The rate of adverse reaction is higher in the HCQ group than that in the control group (30% v.s. 9%). |
| Borba, MGS.et al. (2020) [23] | Fundação de Medicina Tropical Dr. Heitor Vieira Dourado, Manaus, Amazonas, Brazil | Double-blinded, phase IIb clinical trial | N = 440 (finally enrolled 81 patients for the study) Control group: no CQ from other countries Experimental group: High dosage CQ (n = 41) Low dosage CQ (n = 40) | High dosage CQ, 600 mg twice daily for 10 days Low dosage CQ, 450 mg twice daily on D1 and the 450mg/daily for remaining 4 days. | A high dosage of CQ for 10 days presented toxicity red flags, particularly affecting QTc prolongation. This study was terminated early because of the high dosage CQ resulted in a high rate of fatality. |
| Molina, J. M. et al. (2020) [21] | Infectious Diseases Department, AP–HP-Saint-Louis Hospital, Paris, France | Polit clinical trial | N = 11 Control group: Not recruited Experimental group: HCQ + AZ | HCQ, 200 mg thrice daily for 10 days; AZ, 500 mg on D1 followed by 250 mg/daily for the D2 to D5 | One patient died and another one discontinued treatment due to QTc prolongation. 20% of patients (2/10) have full viral clearance conversion on D6 after treatment. |
| Castelnuovo, D. A. et al. (2020) [24] | Mediterranea Cardiocentro, Napoli, Italy | Observational study, Multicenter | N = 3451 Control group: no HCQ (n = 817) Experimental group: HCQ (n = 2634) | HCQ, 400 mg twice daily or once daily on D1 and 200 mg/ daily on D2 to D5 or to D10 | HCQ treatment results in a 30% lower risk of death in COVID-19 hospitalized patients. |
| Catteau, L. et al. (2020) [25] | Department of Epidemiology and public health, Sciensano, Brussels, Belgium | Observational study, Multicenter | N = 8075 Control group: no HCQ (n = 3533) Experimental group: HCQ (n = 4542) | HCQ, 2400 mg in total over 5 days | Compared to the control group, the rate of mortality is significantly lower in the HCQ group. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, T.-C.; Wang, Y.-H.; Chen, Y.-L.; Tsai, W.-C.; Lee, C.-H.; Chuang, K.-P.; Chen, Y.-M.A.; Yuan, C.-H.; Ho, S.-Y.; Yang, M.-H.; et al. Chloroquine and Hydroxychloroquine: Efficacy in the Treatment of the COVID-19. Pathogens 2021, 10, 217. https://doi.org/10.3390/pathogens10020217
Ho T-C, Wang Y-H, Chen Y-L, Tsai W-C, Lee C-H, Chuang K-P, Chen Y-MA, Yuan C-H, Ho S-Y, Yang M-H, et al. Chloroquine and Hydroxychloroquine: Efficacy in the Treatment of the COVID-19. Pathogens. 2021; 10(2):217. https://doi.org/10.3390/pathogens10020217
Chicago/Turabian StyleHo, Tzu-Chuan, Yung-Hsuan Wang, Yi-Ling Chen, Wan-Chi Tsai, Che-Hsin Lee, Kuo-Pin Chuang, Yi-Ming Arthur Chen, Cheng-Hui Yuan, Sheng-Yow Ho, Ming-Hui Yang, and et al. 2021. "Chloroquine and Hydroxychloroquine: Efficacy in the Treatment of the COVID-19" Pathogens 10, no. 2: 217. https://doi.org/10.3390/pathogens10020217
APA StyleHo, T.-C., Wang, Y.-H., Chen, Y.-L., Tsai, W.-C., Lee, C.-H., Chuang, K.-P., Chen, Y.-M. A., Yuan, C.-H., Ho, S.-Y., Yang, M.-H., & Tyan, Y.-C. (2021). Chloroquine and Hydroxychloroquine: Efficacy in the Treatment of the COVID-19. Pathogens, 10(2), 217. https://doi.org/10.3390/pathogens10020217