
IL-16 and BCA-1 Serum Levels Are Associated with Disease Severity of C. difficile Infection




Abstract
:1. Introduction
2. Results
Characterization of the Immune Response in CDI Patients
3. Discussion
4. Materials and Methods
4.1. Study Population and Sample Collection
4.2. Measurement of Cytokine Concentrations–IL16, IL-21, IL-23, IL-33, BCA-1, TRAIL
4.3. Disease Severity Scoring and Demographic Data Collection
4.4. Toxin Detection
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khan, A.M.; Rahman, A.K.; Hossain, M.S.; Faruque, A.S.; Huq, S.; Chisti, M.J.; Salam, M.A. Nosocomial infections among patients admitted to an urban diarrhoeal-diseases treatment facility in Bangladesh: A preliminary survey. Ann. Trop. Med. Parasitol. 2008, 102, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Khurana, S.; Kahl, A.; Yu, K.; DuPont, A.W. Recent advances in the treatment of Clostridioides difficile infection: The ever-changing guidelines. Fac. Rev. 2020, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Dharbhamulla, N.; Abdelhady, A.; Domadia, M.; Patel, S.; Gaughan, J.; Roy, S. Risk Factors Associated with Recurrent Clostridium difficile Infection. J. Clin. Med. Res. 2019, 11, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, Y.P.; Lee, J.C.; Tsai, B.Y.; Wu, J.L.; Liu, H.C.; Liu, H.C.; Lin, H.J.; Tsai, P.J.; Ko, W.C. Risk factors of Clostridium difficile-associated diarrhea in hospitalized adults: Vary by hospitalized duration. J. Microbiol. Immunol. Infect. 2021, 54, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Hsiao, H.L.; Chia, C.Y.; Cheng, C.W.; Tsai, T.C.; Deng, S.T.; Chen, C.L.; Chiu, C.H. Risk factors and outcomes of Clostridium difficile infection in hospitalized patients. Biomed. J. 2019, 42, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Paudel, S.; Zacharioudakis, I.M.; Zervou, F.N.; Ziakas, P.D.; Mylonakis, E. Prevalence of Clostridium difficile infection among solid organ transplant recipients: A meta-analysis of published studies. PLoS ONE 2015, 10, e0124483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phatharacharukul, P.; Thongprayoon, C.; Cheungpasitporn, W.; Edmonds, P.J.; Mahaparn, P.; Bruminhent, J. The Risks of Incident and Recurrent Clostridium difficile-Associated Diarrhea in Chronic Kidney Disease and End-Stage Kidney Disease Patients: A Systematic Review and Meta-Analysis. Dig. Dis. Sci. 2015, 60, 2913–2922. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Phatharacharukul, P.; Edmonds, P.J.; Kaewpoowat, Q.; Mahaparn, P.; Bruminhent, J.; Erickson, S.B. Chronic kidney disease and end-stage renal disease are risk factors for poor outcomes of Clostridium difficile infection: A systematic review and meta-analysis. Int. J. Clin. Pr. 2015, 69, 998–1006. [Google Scholar] [CrossRef] [Green Version]
- Kutty, P.K.; Woods, C.W.; Sena, A.C.; Benoit, S.R.; Naggie, S.; Frederick, J.; Evans, S.; Engel, J.; McDonald, L.C. Risk factors for and estimated incidence of community-associated Clostridium difficile infection, North Carolina, USA. Emerg. Infect. Dis. 2010, 16, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, M.H.; Mooney, L.; Bendall, R.; Settle, C.D.; Fawley, W.N. A case-control study of community-associated Clostridium difficile infection. J. Antimicrob. Chemother. 2008, 62, 388–396. [Google Scholar] [CrossRef] [Green Version]
- Chitnis, A.S.; Holzbauer, S.M.; Belflower, R.M.; Winston, L.G.; Bamberg, W.M.; Lyons, C.; Farley, M.M.; Dumyati, G.K.; Wilson, L.E.; Beldavs, Z.G.; et al. Epidemiology of community-associated Clostridium difficile infection, 2009 through 2011. JAMA Intern. Med. 2013, 173, 1359–1367. [Google Scholar] [CrossRef] [Green Version]
- Guh, A.Y.; Adkins, S.H.; Li, Q.; Bulens, S.N.; Farley, M.M.; Smith, Z.; Holzbauer, S.M.; Whitten, T.; Phipps, E.C.; Hancock, E.B.; et al. Risk Factors for Community-Associated Clostridium difficile Infection in Adults: A Case-Control Study. Open Forum. Infect. Dis. 2017, 4, ofx171. [Google Scholar] [CrossRef] [Green Version]
- Jank, T.; Giesemann, T.; Aktories, K. Rho-glucosylating Clostridium difficile toxins A and B: New insights into structure and function. Glycobiology 2007, 17, 15R–22R. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nottrott, S.; Schoentaube, J.; Genth, H.; Just, I.; Gerhard, R. Clostridium difficile toxin A-induced apoptosis is p53-independent but depends on glucosylation of Rho GTPases. Apoptosis 2007, 12, 1443–1453. [Google Scholar] [CrossRef]
- Abt, M.C.; McKenney, P.T.; Pamer, E.G. Clostridium difficile colitis: Pathogenesis and host defence. Nat. Rev. Microbiol. 2016, 14, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Steiner, T.S.; Flores, C.A.; Pizarro, T.T.; Guerrant, R.L. Fecal lactoferrin, interleukin-1beta, and interleukin-8 are elevated in patients with severe Clostridium difficile colitis. Clin. Diagn. Lab. Immunol. 1997, 4, 719–722. [Google Scholar] [CrossRef] [Green Version]
- El Feghaly, R.E.; Stauber, J.L.; Deych, E.; Gonzalez, C.; Tarr, P.I.; Haslam, D.B. Markers of intestinal inflammation, not bacterial burden, correlate with clinical outcomes in Clostridium difficile infection. Clin. Infect. Dis. 2013, 56, 1713–1721. [Google Scholar] [CrossRef]
- Dinarello, C.A. Biologic basis for interleukin-1 in disease. Blood 1996, 87, 2095–2147. [Google Scholar] [CrossRef] [Green Version]
- Madan, R.; Petri, W.A., Jr. Immune responses to Clostridium difficile infection. Trends Mol. Med. 2012, 18, 658–666. [Google Scholar] [CrossRef] [Green Version]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, 987–994. [Google Scholar] [CrossRef]
- Cruikshank, W.; Center, D.M. Modulation of lymphocyte migration by human lymphokines. II. Purification of a lymphotactic factor (LCF). J. Immunol. 1982, 128, 2569–2574. [Google Scholar]
- Cruikshank, W.W.; Kornfeld, H.; Center, D.M. Interleukin-16. J. Leukoc. Biol. 2000, 67, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Parada, N.A.; Center, D.M.; Kornfeld, H.; Rodriguez, W.L.; Cook, J.; Vallen, M.; Cruikshank, W.W. Synergistic activation of CD4+ T cells by IL-16 and IL-2. J. Immunol. 1998, 160, 2115–2120. [Google Scholar] [PubMed]
- Seegert, D.; Rosenstiel, P.; Pfahler, H.; Pfefferkorn, P.; Nikolaus, S.; Schreiber, S. Increased expression of IL-16 in inflammatory bowel disease. Gut 2001, 48, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.; Chen, K.; Sun, Y.; Carter, M.; Garey, K.W.; Savidge, T.C.; Devaraj, S.; Tessier, M.E.; von Rosenvinge, E.C.; Kelly, C.P.; et al. Cytokines Are Markers of the Clostridium difficile-Induced Inflammatory Response and Predict Disease Severity. Clin. Vaccine Immunol. 2017, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legler, D.F.; Loetscher, M.; Roos, R.S.; Clark-Lewis, I.; Baggiolini, M.; Moser, B. B cell-attracting chemokine 1, a human CXC chemokine expressed in lymphoid tissues, selectively attracts B lymphocytes via BLR1/CXCR5. J. Exp. Med. 1998, 187, 655–660. [Google Scholar] [CrossRef]
- Ansel, K.M.; Harris, R.B.; Cyster, J.G. CXCL13 is required for B1 cell homing, natural antibody production, and body cavity immunity. Immunity 2002, 16, 67–76. [Google Scholar] [CrossRef] [Green Version]
- George, S.; Lucero, Y.; Torres, J.P.; Lagomarcino, A.J.; O’Ryan, M. Gastric Damage and Cancer-Associated Biomarkers in Helicobacter pylori-Infected Children. Front. Microbiol. 2020, 11, 90. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.; Lin, C.; Li, H.; Xu, Z.; Wang, J.; Li, R.; Liu, H.; Zhang, H.; He, H.; Xu, J. CXCL13 expression is prognostic and predictive for postoperative adjuvant chemotherapy benefit in patients with gastric cancer. Cancer Immunol. Immunother. 2018, 67, 261–269. [Google Scholar] [CrossRef]
- Fan, L.; Zhu, Q.; Liu, L.; Zhu, C.; Huang, H.; Lu, S.; Liu, P. CXCL13 is androgen-responsive and involved in androgen induced prostate cancer cell migration and invasion. Oncotarget 2017, 8, 53244–53261. [Google Scholar] [CrossRef] [Green Version]
- Rampuria, P.; Lang, G.A.; Devera, T.S.; Gilmore, C.; Ballard, J.D.; Lang, M.L. Coordination between T helper cells, iNKT cells, and their follicular helper subsets in the humoral immune response against Clostridium difficile toxin B. J. Leukoc. Biol. 2017, 101, 567–576. [Google Scholar] [CrossRef]
- McDermott, A.J.; Falkowski, N.R.; McDonald, R.A.; Pandit, C.R.; Young, V.B.; Huffnagle, G.B. Interleukin-23 (IL-23), independent of IL-17 and IL-22, drives neutrophil recruitment and innate inflammation during Clostridium difficile colitis in mice. Immunology 2016, 147, 114–124. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.H.; Gerding, D.N.; Johnson, S.; Kelly, C.P.; Loo, V.G.; McDonald, L.C.; Pepin, J.; Wilcox, M.H.; Society for Healthcare Epidemiology of America; Infectious Diseases Society of America. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA). Infect. Control. Hosp. Epidemiol. 2010, 31, 431–455. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | n (%) |
|---|---|
| Gender | |
| Male | 21 (38.9) |
| Female | 33 (61.1) |
| Disease severity | |
| Mild to moderate | 20 (37) |
| Severe | 34 (63) |
| Toxins Presence | |
| Toxin A | 6 (11.1) |
| Toxin B | 14 (25.9) |
| Toxins A + B | 34 (63) |
| In-hospital mortality | |
| Alive | 39 (72.2) |
| Died | 15 (27.8) |
| Infection acquisition | |
| Nosocomial | 37 (68.5) |
| Community | 17 (31.5) |
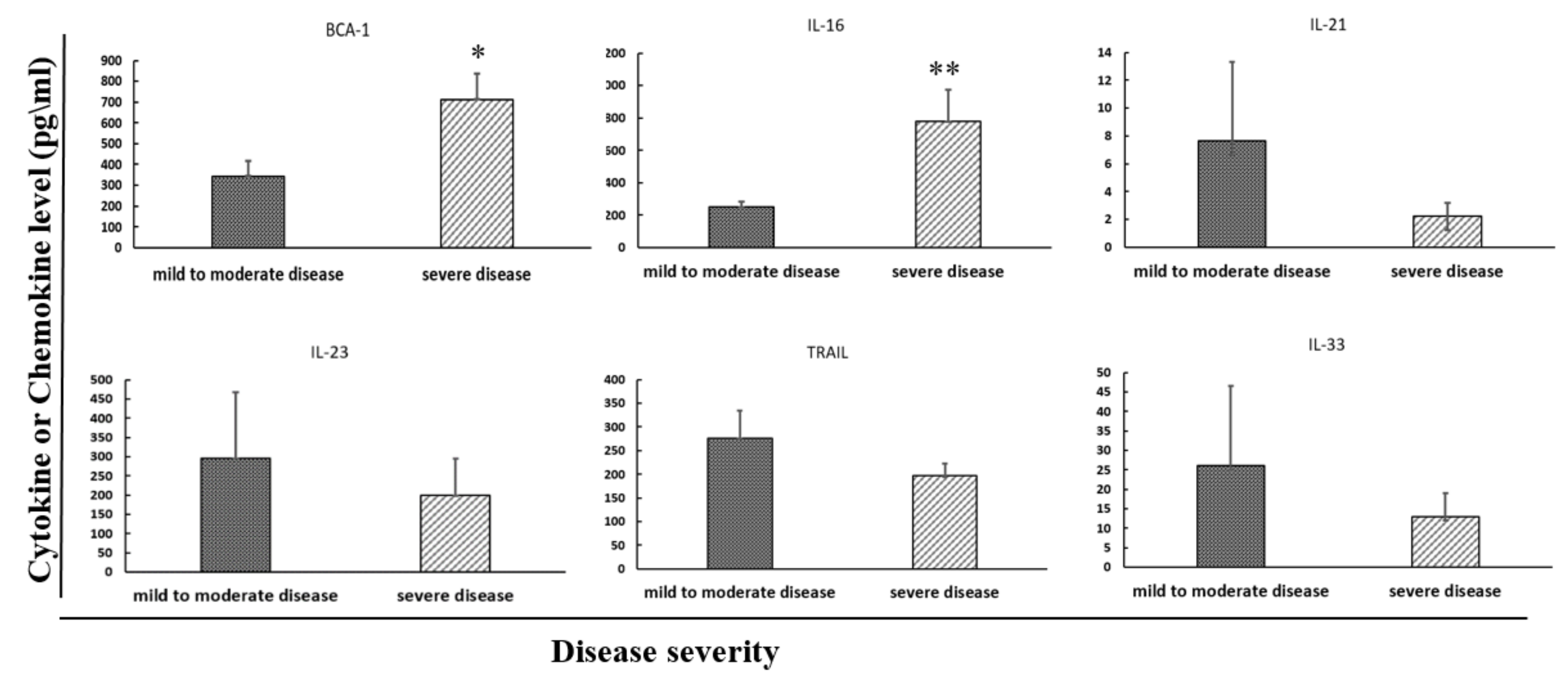
| Mild-Moderate (n = 20) Mean (Range) | Severe (n = 34) Mean (Range) | p-Value | |
|---|---|---|---|
| IL-16 | 250.3 (0–622.1) | 778 (0–6578.3) | 0.005 ** |
| IL-21 | 7.7 (0–110.9) | 2.2 (0–27.7) | 0.956 |
| IL-23 | 294.8 (0–3083.6) | 198.9 (0–2638.1) | 0.740 |
| IL-33 | 26 (0–408.8) | 12.9 (0–174.1) | 0.758 |
| BCA-1 | 344.7 (63.2–1000) | 712.8 (39.6–4266) | 0.012 ** |
| TRAIL | 276 (16.9–881.1) | 190.8 (0–584.3) | 0.333 |
| p-Value | ||||||
|---|---|---|---|---|---|---|
| Parameter | IL-16 | IL-21 | IL-23 | IL-33 | BCA-1 | TRAIL |
| Gender (Male/Female) | 0.531 | 0.182 | 0.360 | 0.751 | 0.487 | 0.401 |
| Toxins Presence (Toxin A/B/A + B) | 0.215 | 0.391 | 0.851 | 0.936 | 0.543 | 0.098 |
| In-Hospital Mortality (Alive/Dead) | 0.284 | 0.792 | 0.227 | 0.207 | 0.309 | 0.380 |
| Infection Acquisition (Nosocomial/Community) | 0.635 | 0.474 | 1 | 0.600 | 0.322 | 0.402 |
| Pearson Coefficient | ||||||
|---|---|---|---|---|---|---|
| Parameter | IL-16 | IL-21 | IL-23 | IL-33 | BCA-1 | TRAIL |
| Creathinine | −0.06 | −0.04 | −0.05 | 0.06 | 0.31 * | −0.35 * |
| Albumin | 0.06 | −0.07 | −0.21 | 0.02 | −0.11 | 0.46 *** |
| CRP | −0.15 | −0.05 | −0.07 | 0 | 0.06 | −0.28 * |
| WBC | 0.30 * | −0.09 | −0.05 | 0 | −0.06 | −0.10 |
| Neutrophils | 0.15 | 0.07 | 0.07 | 0.09 | −0.42 ** | −0.11 |
| Lymphocytes | −0.13 | −0.08 | −0.03 | −0.10 | 0.45 *** | 0.06 |
| Calprotectin | 0.01 | 0.02 | 0.12 | 0.16 | −0.04 | 0.13 |
| Procalcitonin | 0.03 | −0.05 | −0.05 | −0.02 | 0.02 | −0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gotshal, D.; Azrad, M.; Hamo, Z.; Nitzan, O.; Peretz, A. IL-16 and BCA-1 Serum Levels Are Associated with Disease Severity of C. difficile Infection. Pathogens 2021, 10, 631. https://doi.org/10.3390/pathogens10050631
Gotshal D, Azrad M, Hamo Z, Nitzan O, Peretz A. IL-16 and BCA-1 Serum Levels Are Associated with Disease Severity of C. difficile Infection. Pathogens. 2021; 10(5):631. https://doi.org/10.3390/pathogens10050631
Chicago/Turabian StyleGotshal, Dor, Maya Azrad, Zohar Hamo, Orna Nitzan, and Avi Peretz. 2021. "IL-16 and BCA-1 Serum Levels Are Associated with Disease Severity of C. difficile Infection" Pathogens 10, no. 5: 631. https://doi.org/10.3390/pathogens10050631
APA StyleGotshal, D., Azrad, M., Hamo, Z., Nitzan, O., & Peretz, A. (2021). IL-16 and BCA-1 Serum Levels Are Associated with Disease Severity of C. difficile Infection. Pathogens, 10(5), 631. https://doi.org/10.3390/pathogens10050631