
Severe Pneumonia in Neonates Associated with Legionella pneumophila: Case Report and Review of the Literature


Abstract
:1. Introduction
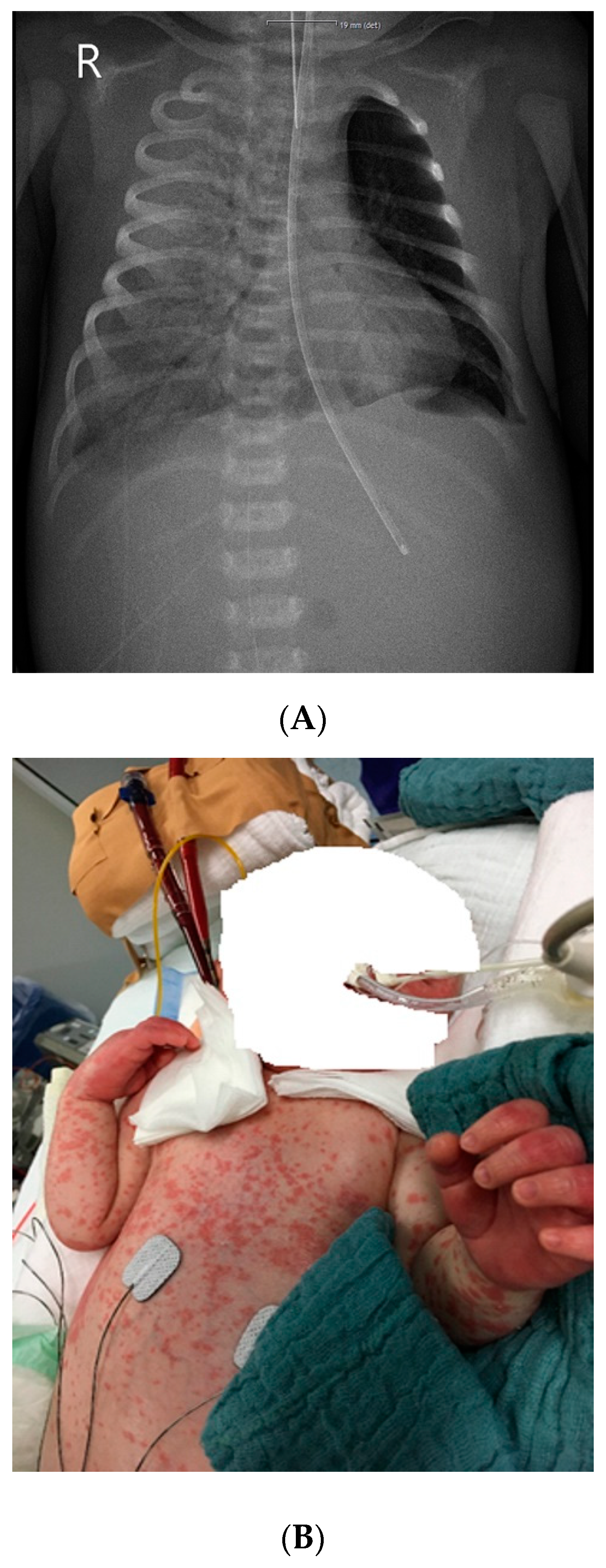
2. Case Report
3. Material and Methods
4. Results
4.1. Epidemiology and Environmental Isolation
4.2. Clinical Findings
4.3. Diagnostic Studies
4.4. Treatment and Outcome
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cunha, B.A.; Burillo, A.; Bouza, E. Legionnaires’ disease. Lancet 2016, 387, 376–385. [Google Scholar] [CrossRef]
- Franzin, L.; Scolfaro, C.; Cabodi, D.; Valera, M.; Tovo, P.A. Legionella pneumophila pneumonia in a newborn after water birth: A new mode of transmission. Clin. Infect. Dis. 2001, 33, e103–e104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shachor-Meyouhas, Y.; Kassis, I.; Bamberger, E.; Nativ, T.; Sprecher, H.; Levy, I.; Srugo, I. Fatal hospital-acquired legionella pneumonia in a neonate. Pediatr. Infect. Dis. J. 2010, 29, 280–281. [Google Scholar] [CrossRef] [PubMed]
- Yiallouros, P.K.; Papadouri, T.; Karaoli, C.; Papamichael, E.; Zeniou, M.; Pieridou-Bagatzouni, D.; Papageorgiou, G.T.; Pissarides, N.; Harrison, T.G.; Hadjidemetriou, A. First outbreak of nosocomial legionella infection in term neonates caused by a cold mist ultrasonic humidifier. Clin. Infect. Dis. 2013, 57, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Lück, P.C.; Dinger, E.; Helbig, J.H.; Thurm, V.; Keuchel, H.; Presch, C.; Ott, M. Analysis of Legionella pneumophila strains associated with nosocomial pneumonia in a neonatal intensive care unit. Eur. J. Clin. Microbiol. Infect. Dis. 1994, 13, 565–571. [Google Scholar] [CrossRef]
- Phin, N.; Cresswell, T.; Parry-Ford, F.; Cresswell, T.; Cresswell, T.; Phin, N.; Walker, J.; Aird, H.; Lloyd, K.; Fletcher, G.; et al. Case of legionnaires’ disease in a neonate following a home birth in a heated birthing pool, England, June 2014. Eurosurveillance 2014, 19, 20857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritschel, E.; Sanyal, K.; Threadgill, H.; Cervantes, D. Fatal legionellosis after water birth, Texas, USA, 2014. Emerg. Infect. Dis. 2015, 21, 130–132. [Google Scholar] [CrossRef]
- Moscatelli, A.; Buratti, S.; Castagnola, E.; Mesini, A.; Tuo, P. Severe neonatal Legionella Pneumonia: Full recovery after extracorporeal life support. Pediatrics 2015, 136, e1043–e1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrou, P.; Chiotaki, R.; Dalezios, Y.; Chalepakis, G. Overlapping and divergent localization of Frem1 and Fras1 and its functional implications during mouse embryonic development. Exp. Cell Res. 2007, 313, 910–920. [Google Scholar] [CrossRef]
- Fremgen, L. What We Learned about Waterbirth from a Case of Legionella. Midwifery Today Int. Midwife 2015, 115, 33–34. [Google Scholar]
- Collins, S.L.; Afshar, B.; Walker, J.T.; Aird, H.; Naik, F.; Parry-Ford, F.; Phin, N.; Harrison, T.G.; Chalker, V.J.; Sorrell, S.; et al. Heated birthing pools as a source of Legionnaires’ disease. Epidemiol. Infect. 2016, 144, 796–802. [Google Scholar] [CrossRef]
- Ferrer Marcelles, A.; García Hernández, F.; Elcuaz Romano, R.; Tokashiki Tokumura, N.; Fernández, F. Pneumonia caused by Legionella in a newborn infant. An. Esp. Pediatr. 1989, 30, 213–214. [Google Scholar]
- Aubert, G.; Bornstein, N.; Rayet, I.; Pozzetto, B.; Lenormand, P.H. Nosocomial infection with legionella pneumophila serogroup 1 and 8 in a neonate. Scand. J. Infect. Dis. 1990, 22, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Greene, K.A.; Rhine, W.D.; Starnes, V.A.; Ariagno, R.L. Fatal postoperative Legionella pneumonia in a newborn. J Perinatol. 1990, 10, 183–184. [Google Scholar]
- Holmberg Jr, R.E.; Pavia, A.T.; Montgomery, D.; Clark, J.M.; Eggert, L.D. Nosocomial Legionella pneumonia in the neonate. Pediatrics 1993, 92, 450–453. [Google Scholar]
- Unit for Surveillance and Control of Communicable Diseases. Legionnaires disease in a neonatal unit of a private hospital, Cyprus, December 2008: Preliminary outbreak report. Eurosurveillance 2009, 14, 19090. [Google Scholar] [CrossRef] [Green Version]
- Nagai, T.; Sobajima, H.; Iwasa, M.; Tsuzuki, T.; Kura, F.; Amemura-Maekawa, J.; Watanabe, H. Neonatal sudden death due to Legionella pneumonia associated with water birth in a domestic spa bath. J. Clin. Microbiol. 2003, 41, 2227–2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granseth, G.; Bhattarai, R.; Sylvester, T.; Prasai, S.; Livar, E. Notes from the Field: Two Cases of Legionnaires’ Disease in Newborns After Water Births—Arizona, 2016. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 590–591. [Google Scholar] [CrossRef] [Green Version]
- Barton, M.; McKelvie, B.; Campigotto, A.; Mullowney, T. Legionellosis following water birth in a hot tub in a Canadian neonate. CMAJ 2017, 189, E1311–E1313. [Google Scholar] [CrossRef] [Green Version]
- Dorfman, M.V.; Clark, J.D.; Brogan, T.V. ECLS for Legionella: All Ages Welcome in the ELSO Registry. ASAIO J. 2020, 66, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Womack, S.J.; Liang, K.C.; Ilagan, N.B.; Weyhing, B.T.; Planas, A. Legionella pneumophila in a preterm infant. A case report. J. Perinatol. 1992, 12, 303–305. [Google Scholar]
- Ferrer, A.; Elcuaz, R.I.; Giménez-Pérez, M.; Iglesias, J.; Fernández-Pérez, F. Childhood legionellosis. Enferm. Infecc. Microbiol. Clin. 1990, 8, 278–281. [Google Scholar]
- Leruste, A.; Rambaud, J.; Picard, C.; Jarraud, S.; Ferroni, A.; Lawrence, C.; Renolleau, S. Successful pediatric ECMO in a rare case of septic shock due to a community-acquired Legionella infection. Med. Mal. Infect. 2017, 47, 68–70. [Google Scholar] [CrossRef]
- Horie, H.; Kawakami, H.; Minoshima, K.; Kamohara, T.; Nakamura, T.; Kuroki, H.; Nakamura, A. Neonatal Legionnaires’ disease. Histopathological findings in an autopsied neonate. Acta Pathol. Jpn. 1992, 42, 427–431. [Google Scholar] [PubMed]
- Ahrens, F.; Hell, W.; Hollandt, H.; Lewald, H.; Paust, H. Legionellose bei einem Neugeborenen. Monatsschr. Kinderheilkd. 1993, 141, 711–713. [Google Scholar]
- Levy, I.; Rubin, L.G. Legionella Pneumonia in Neonates: A Literature Review. J Perinatol. 1998, 18, 287–290. [Google Scholar]
- Skogberg, K.; Nuorti, J.P.; Saxen, H.; Kusnetsov, J.; Mentula, S.; Fellman, V.; Mäki-Petäys, N.; Jousimies-Somer, H. A newborn with domestically acquired legionnaires disease confirmed by molecular typing. Clin. Infect. Dis. 2002, 35, 82–85. [Google Scholar] [CrossRef]
- Franzin, L.; Cabodi, D.; Scolfaro, C.; Gioannini, P. Microbiological investigation of a nosocomial case of Legionella pneumophila pneumonia associated with water birth and review of neonatal cases. Infez. Med. 2004, 12, 69–75. [Google Scholar] [PubMed]
- Greenberg, D.; Chiou, C.C.; Famigilleti, R.; Lee, T.C.; Yu, V.L. Problem pathogens: Paediatric legionellosis-implications for improved diagnosis. Lancet Infect. Dis. 2006, 6, 529–535. [Google Scholar] [CrossRef]
- Yu, V.L.; Lee, T.C. Neonatal legionellosis: The tip of the iceberg for pediatric hospital-acquired pneumonia? Pediatr. Infect. Dis. J. 2010, 29, 282–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teare, L.; Millership, S. Legionella pneumophila serogroup 1 in a birthing pool. J. Hosp. Infect. 2012, 82, 58–60. [Google Scholar] [CrossRef] [PubMed]
- Allen, T.P.; Fried, J.S.; Wiegmann, T.B.; Hodges, G.R.; Dixon, A.Y.; Lee, S.H.; MacDougall, M.L. Legionnaires’ disease associated with rash and renal failure. Arch. Intern. Med. 1985, 145, 729–730. [Google Scholar] [CrossRef]
- Helms, C.M.; Donaldson, M.F.; Johnson, W.; Corry, R.J. Pretibial Rash in Legionella pneumophila Pneumonia. JAMA 1981, 245, 1758–1759. [Google Scholar] [CrossRef] [PubMed]
- Ziemer, M.; Ebert, K.; Schreiber, G.; Voigt, R.; Sayer, H.G.; Marx, G. Exanthema in Legionnaires’ disease mimicking a severe cutaneous drug reaction. Clin. Exp. Dermatol. 2009, 34, e72-4. [Google Scholar] [CrossRef]
- Padrnos, L.J.; Blair, J.E.; Kusne, S.; Dicaudo, D.J.; Mikhael, J.R. Cutaneous legionellosis: Case report and review of the medical literature. Transpl. Infect. Dis. 2014, 16, 307–314. [Google Scholar] [CrossRef]
- Whiley, H.; Taylor, M. Legionella detection by culture and qPCR: Comparing apples and oranges. Crit. Rev. Microbiol. 2016, 42, 65–74. [Google Scholar] [CrossRef] [Green Version]
- Yaradou, D.F.; Hallier-Soulier, S.; Moreau, S.; Poty, F.; Hillion, Y.; Reyrolle, M.; André, J.; Festoc, G.; Delabre, K.; Vandenesch, F.; et al. Integrated real-time PCR for detection and monitoring of Legionella pneumophila in water systems. Appl. Environ. Microbiol. 2007, 73, 1452–1456. [Google Scholar] [CrossRef] [Green Version]
- Wild, K.T.; Rintoul, N.; Kattan, J.; Gray, B.; Engle, R.W.; Keene, S.; Best, D.; Davis, C.; Digeronimo, R.; Raman, L. Extracorporeal Life Support Organization (ELSO): Guidelines for Neonatal Respiratory Failure. ASAIO J. 2020, 66, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Bartram, J.; Chartier, Y.; Lee, J.; Pond, K.; Surman-Lee, S. Legionella and the Prevention of Legionellosis; World Health Organization Press: Geneva, Switzerland, 2007. [Google Scholar]



{kind=link}
{kind=link}
| Reference, Country | Type of Publication | No. of Cases | Age at Diagnosis (d) | Positive Diagnostics | Source of L. pneumophila | Serotype | Treatment with Macrolide Antibiotics | ECMO | Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Marcelles AF et al., 1989, [12] Spain–Europe | CR | 1 | 1 | Postmortem autopsy | 1 Humidifier of the respirator | 6 | No | No | Death |
| Aubert G et al., 1990, [13] France–Europe | CR | 1 | 10 | BAL culture | 1 Oxygen nebulizer, feeding bottle system | 1,8 | Unknown | No | Recovery |
| Greene KA et al., 1990, [14] North America | CR | * 1 | 12 | Postmortem autopsy | 1 Not detected | 1 | No | No | Death |
| Ferrer A et al., 1990, [22] Spain–Europe | CR (Review) | * 4 | 10–2555 | Pleural fluid, tracheal aspirate, BAL culture, postmortem biopsy | 1 Not detected | 6 | Yes | No | Recovery/ 3× death |
| Horie H et al., 1992, [24] Japan–Asia | CR | 1 | 5 | Postmortem autopsy | 1 Unknown | 1 | No | No | Death |
| Womack SJ et al., 1992, [21] North America | CR | * 1 | 16 | Postmortem Autopsy | Respirator | 1 | No | No | Death |
| Ahrens F et al., 1993, [25] Germany–Europe | CR | 1 | 5 | BAL culture | 1 Environmental cultures | 1 | Yes | No | Recovery |
| Holmberg Jr RE et al., 1993, [15] North America | CR | * 1 | 31 | Tracheal aspirate culture | 1 Nursery sink, nurse’s wet hand | 6 | Yes (+rifampicin) | No | Recovery |
| Lück PC et al., 1994, [5] Germany–Europe | CR | * 1 | 10 | Tracheal aspirate culture | 1 Humidifier of the respirator | 1 | No | No | Death |
| Levy I and Rubin LG, 1998, [26] North America | Review | * 9 | 4–31 | Pleural fluid, tracheal aspirate, BAL culture, DFA assay, postmortem biopsy | 1 Humidifier, nebulizer, incubator | 1,6 | Yes (+rifampicin) | No | Recovery/ death |
| Franzin et al., 2001, [2] Italy–Europe | CR | 1 | 7 | Urinary antigen test, DFA assay | 1 Pool water (water birth) | 1 | Yes | No | Recovery |
| Skogberg K et al., 2002, [27] Finland–Europe | CR | 1 | 7 | Urinary antigen test; BAL culture, DFA assay | 2 Apartment building | 6 | Yes (+rifampicin) | No | Recovery |
| Nagai T et al., 2003, [17] Japan–Asia | CR | 1 | 4 | Postmortem autopsy (PCR) | 2 Bath tub (water birth) | 1,6 | None | No | Death |
| Franzin L et al., 2004, [28] Italy–Europe | (CR) Review | * 11 | 7 | Urinary antigen test, DFA assay | 1 Pool water (water birth) | 1 | Yes | No | Recovery |
| Greenberg D et al., 2006, [29] North America | Review | * 76 | >5 | Culture methodology, DFA assay | 1 Environmental cultures | 1 | Yes | No | Recovery/ death |
| Eurosurveillance, 2009, [16] Europe | Outbreak | 11 | 6–12 | Urinary antigen test, BAL | 1 Humidifier | 1,3 | Yes (+rifampicin) | No | Recovery/ death |
| Shachor-Meyouhas Y et al., 2010, [3] Israel–Asia | CR | * 1 | 11 | Postmortem Autopsy (culture) | 1 Sink of the ward | 1 | Yes | No | Death |
| Yu VL and Lee TC, 2010, [30] North America | Review | 4–11 | Urinary antigen test, culture | 1 Environmental cultures | 1,6 | Yes | No | Unknown | |
| Teare L, Millership S, 2012, [31] UK–Europe | Review | Pool water (water birth) | 1 | Not detected | No | Unknown | |||
| Yiallouros PK et al., 2013, [4] Cyprus–Europe | Outbreak | 9 | 6–12 | Urinary antigen test, tracheal aspirate culture | 1 Humidifier | 1,3 | Yes (+rifampicin) | No | Recovery/ 3x death |
| Phin N et al., 2014, [6] UK–Europe | CR | 1 | 3 | BAL culture | 2 Birthing pool (water birth) | 1 | ECMO | Yes | Unknown |
| Fritschel E et al., 2015, [7] North America | CR | 1 | 6 | Urinary antigen test, tracheal aspirate PCR | 2 Collapsible tub (water birth) | 1 | No | Yes | Death |
| Moscatelli A et al., 2015, [8] Italy–Europe | CR | * 1 | 12 | BAL PCR | 1 Environmental cultures | Unknown | Yes (+rifampicin) | Yes | Recovery |
| Fremgen L, 2015, [10] North America | CR | 1 | 2 Pool water (water birth) | Not detected | Not detected | No | Unknown | ||
| Collins SL et al., 2016, [11] UK–Europe | CR | 1 | 3 | BAL culture/ PCR | 2 Birthing pool (water birth) | 1 | Not detected | No | Unknown |
| Granseth G et al., 2016, [18] North America | CR | * 2 | 1,3 | Urinary antigen test, tracheal aspirate, BAL culture | 2 Tub (water birth) | 1,6 | Yes | No | Recovery |
| Barton M et al., 2017, [19] UK–Europe | CR | 1 | 8 | Urinary antigen test, tracheal aspirate culture | 2 Hot tub (water birth) | 6 | Yes (+rifampicin) | No | Recovery |
| Leruste A et al., 2017, [23] France-Europe | CR | * 1 | 27 | Tracheal aspirate, BAL culture/PCR | 2 Not detected | 3 | Yes | Yes | Recovery |
| Dorfman MV et al., 2020, [20] North America | Review | 1 | 6 | Urinary antigen test, tracheal aspirate culture | 2 Water birth | Unknown | Yes | Yes | Recovery |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez Ortiz, A.; Hahn, C.; Schaible, T.; Rafat, N.; Lange, B. Severe Pneumonia in Neonates Associated with Legionella pneumophila: Case Report and Review of the Literature. Pathogens 2021, 10, 1031. https://doi.org/10.3390/pathogens10081031
Perez Ortiz A, Hahn C, Schaible T, Rafat N, Lange B. Severe Pneumonia in Neonates Associated with Legionella pneumophila: Case Report and Review of the Literature. Pathogens. 2021; 10(8):1031. https://doi.org/10.3390/pathogens10081031
Chicago/Turabian StylePerez Ortiz, Alba, Camilla Hahn, Thomas Schaible, Neysan Rafat, and Bettina Lange. 2021. "Severe Pneumonia in Neonates Associated with Legionella pneumophila: Case Report and Review of the Literature" Pathogens 10, no. 8: 1031. https://doi.org/10.3390/pathogens10081031
APA StylePerez Ortiz, A., Hahn, C., Schaible, T., Rafat, N., & Lange, B. (2021). Severe Pneumonia in Neonates Associated with Legionella pneumophila: Case Report and Review of the Literature. Pathogens, 10(8), 1031. https://doi.org/10.3390/pathogens10081031