
Bronchoscopy and Lung Fine-Needle Aspiration for Antemortem Evaluation of Pulmonary Involvement in Dogs with Naturally Occurring Canine Leishmaniosis

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Study Population
2.2. Clinicopathological Examination
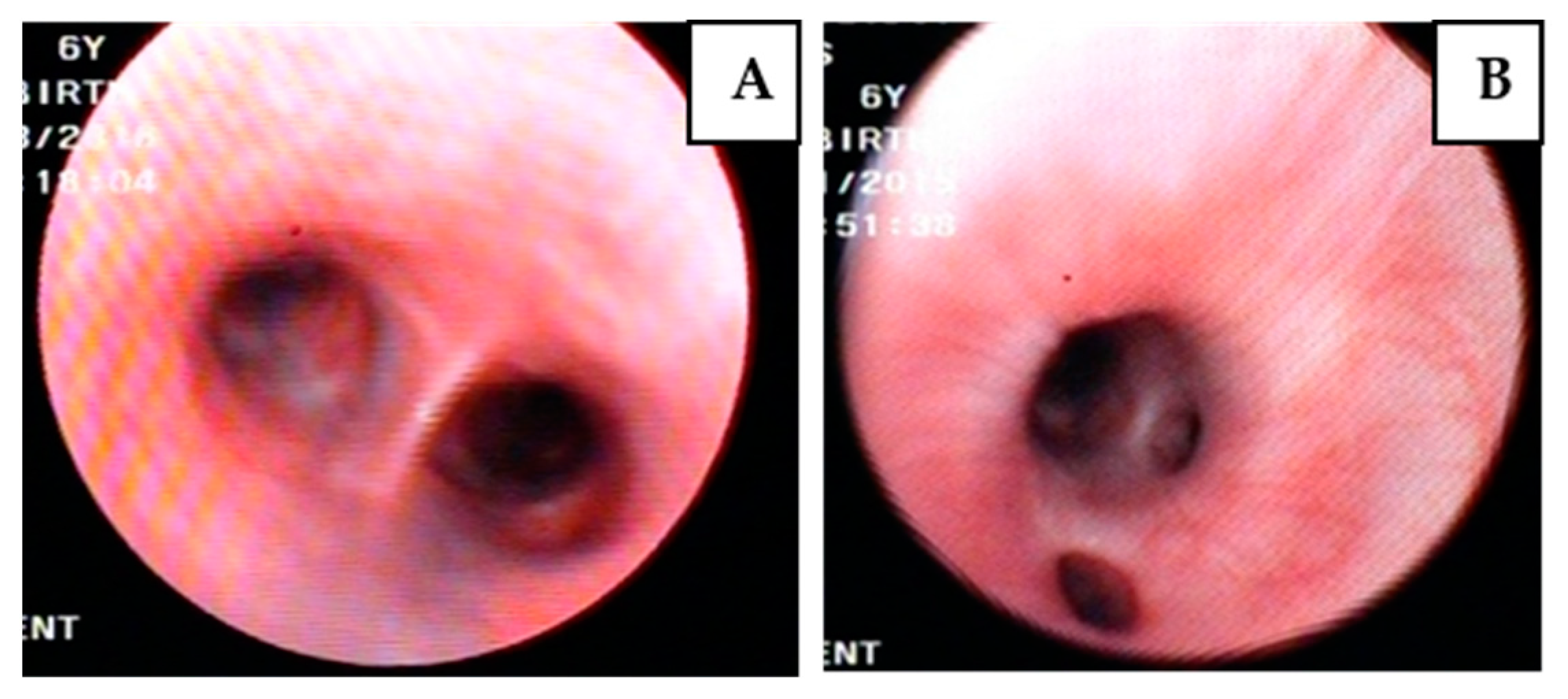
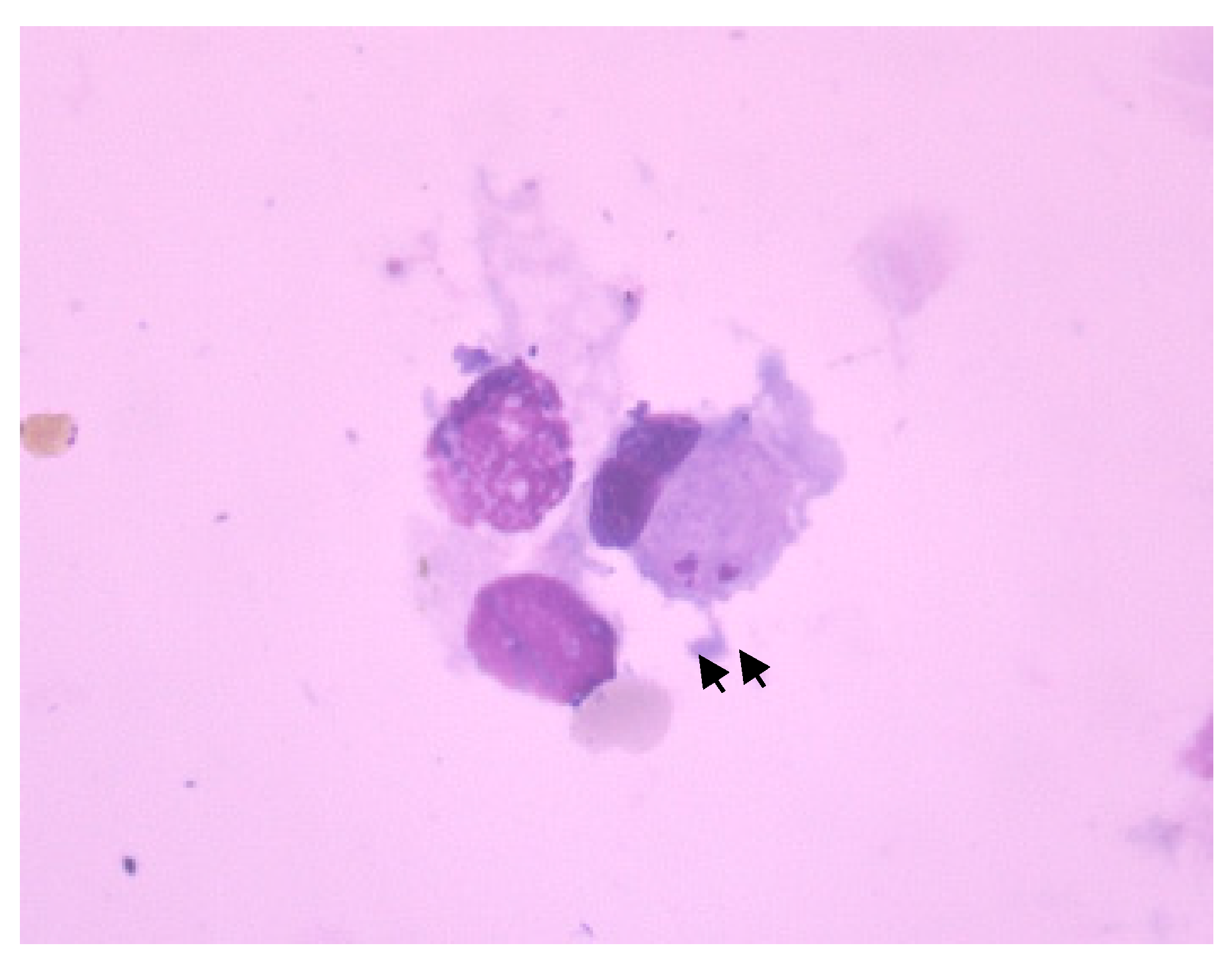
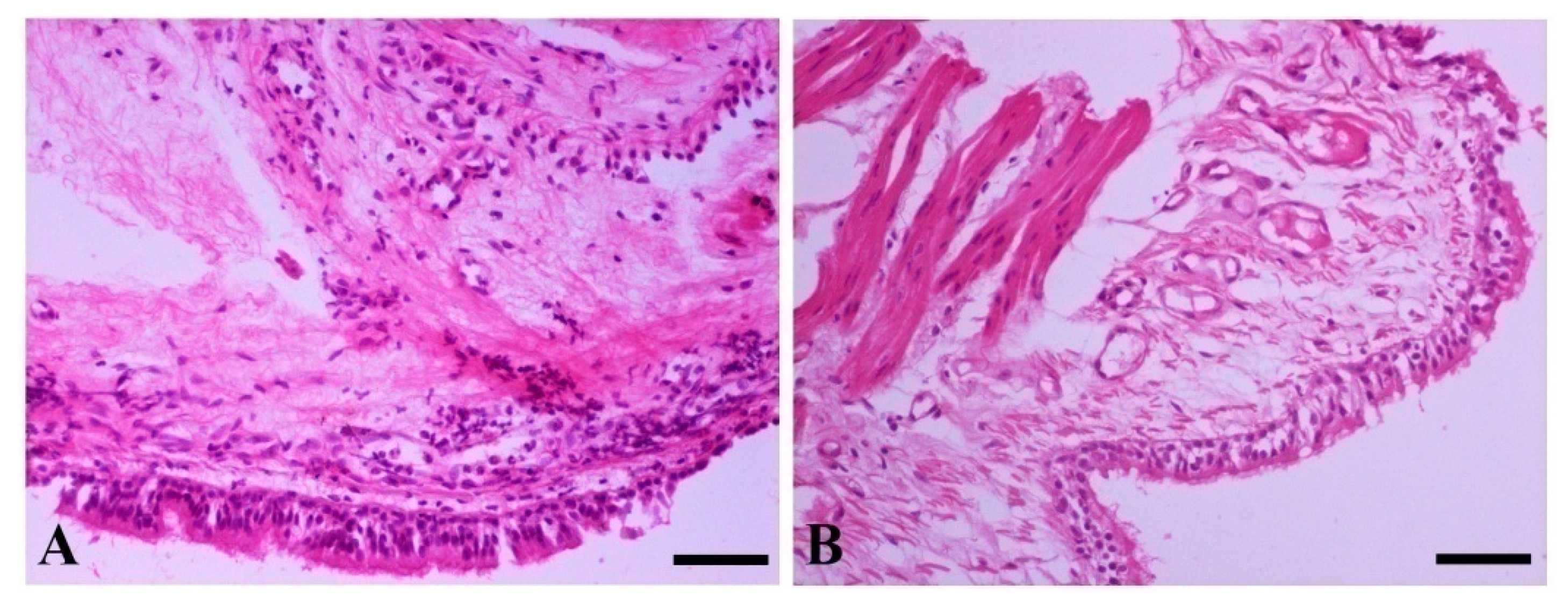
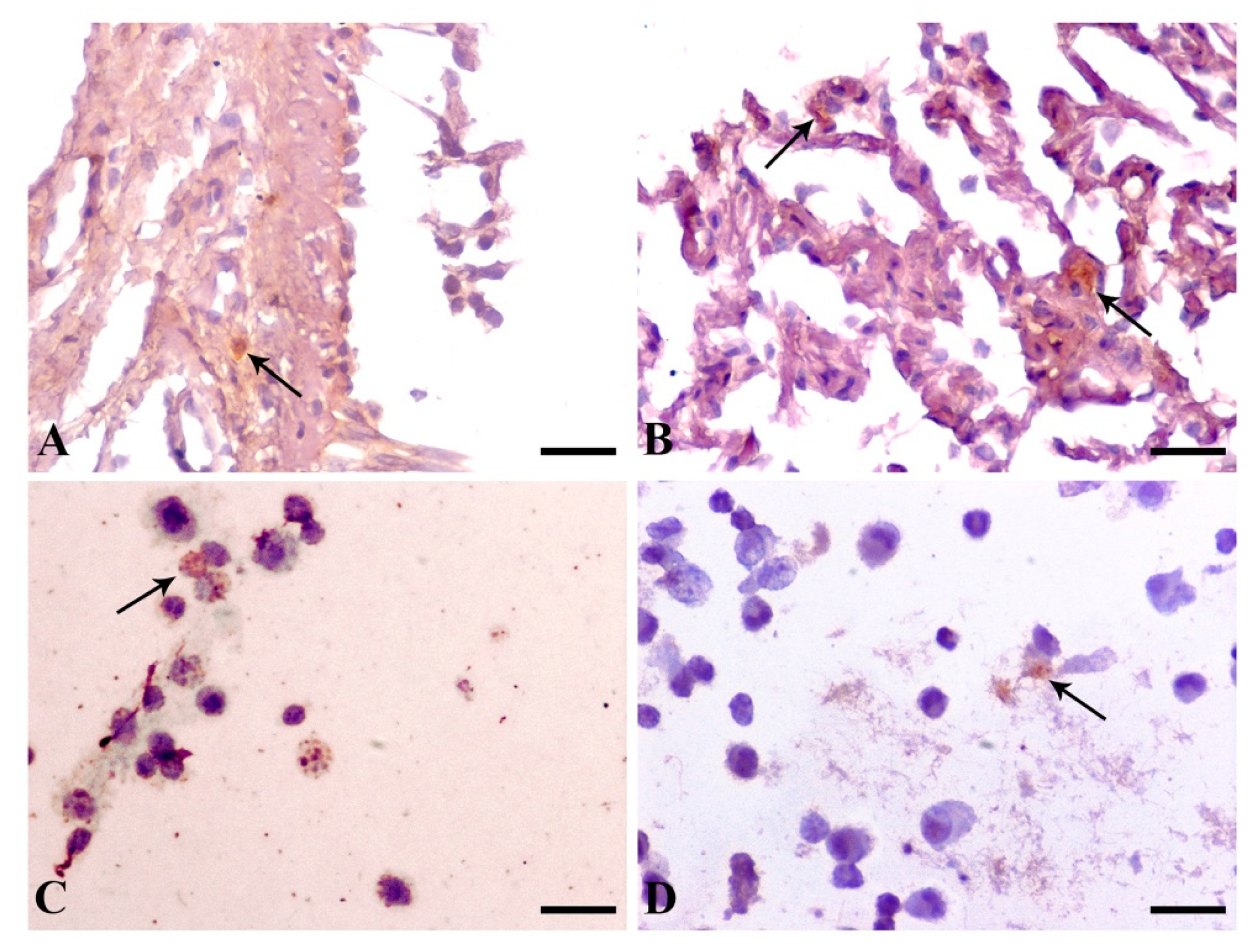
2.3. Bronchoscopy, Lung FNA, Immunodiagnostics
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Clinicopathological Examination
4.3. Bronchoscopy, Lung FNA, Immunodiagnostics
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baneth, G. Leishmaniasis. In Infectious Diseases of the Dog and Cat, 3rd ed.; Greene, C.E., Ed.; Saunders Elsevier: St. Louis, MO, USA, 2006; pp. 685–695. [Google Scholar]
- Saridomichelakis, M.N. Advances in the pathogenesis of canine leishmaniosis: Epidemiologic and diagnostic implications. Vet. Dermatol. 2009, 20, 471–489. [Google Scholar] [CrossRef]
- Segaraa, S. Nutritional Modulation of the Immune Response Mediated by Nucleotides in Canine Leishmaniosis. Microorganisms 2021, 9, 2601. [Google Scholar] [CrossRef] [PubMed]
- Koutinas, A.F.; Polizopoulou, Z.S.; Saridomichelakis, M.N.; Argyriadis, D.; Fytianou, A.; Plevraki, K.G. Clinical considerations on canine visceral leishmaniasis in Greece: A retrospective study of 158 cases (1989–1996). J. Am. Anim. Hosp. Assoc. 1999, 35, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Baneth, G.; Koutinas, A.F.; Solano-Galego, L.; Bourdeau, P.; Ferrer, L. Canine leishmaniosis—New concepts and insights on an expanding zoonosis: Part one. Trends Parasitol. 2008, 24, 324–330. [Google Scholar] [CrossRef]
- Ciaramella, P.; Oliva, G.; Luna, R.D.; Gradoni, L.; Ambrosio, R.; Cortese, L.; Scalone, A.; Persechino, A. A retrospective clinical study of canine leishmaniosis in 150 dogs naturally infected by Leishmania infantum. Vet. Rec. 1997, 141, 539–543. [Google Scholar] [CrossRef]
- Solano-Gallego, L.; Miro, G.; Koutinas, A.F.; Cardoso, L.; Pennisi, M.G.; Ferrer, L.; Bourdeau, P.; Oliva, G.; Baneth, G.; The LeishVet Group. LeishVet guidelines for the practical management of canine leishmaniosis. Parasit. Vectors 2011, 4, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamama-Moraitou, K.K.; Rallis, T.S.; Koytinas, A.F.; Tontis, D.; Plevraki, K.; Kritsepi, M. Asymptomatic colitis in naturally infected dogs with Leishmania infantum: A prospective study. Am. J. Trop. Med. Hyg. 2007, 76, 53–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agut, A.; Corzo, N.; Murciano, J.; Laredo, F.G.; Soler, M. Clinical and readiographic study of bone and joint lesions in 26 dogs with leishmaniosis. Vet. Rec. 2003, 153, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, L.; de Lara, F.C.; Martin, E.; Hervás, J.; Molleda, J.M.; Gómez-Villsmsndos, J.C.; López, R. Acute haemorrhagic pancreatitis associated with canine leishmaniasis. Vet. Rec. 1997, 141, 519–521. [Google Scholar] [CrossRef] [PubMed]
- Márquez, M.; Pedregosa, J.R.; López, J.; Marco-Salazar, P.; Fondevila, D.; Pumarola, M. Leishmania amastigotes in the central nervous system of a naturally infected dog. J. Vet. Diagn. Investig. 2013, 25, 142–146. [Google Scholar]
- Gonçalves, R.; Tafuri, W.L.; Melo, M.N.; Raso, P.; Tafuri, W.L. Chronic interstitial pneumonitis in dogs naturally infected with Leishmania (Leishmania) chagasi: A histopathological and morphometric study. Rev. Inst. Med. Trop. Sao Paulo 2003, 45, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Duarte, M.I.; Laurenti, M.D.; Brandão Nunes, V.L.; Rego Junior, A.F.; Oshiro, E.T.; Corbett, C.E. Interstitial pneumonitis in canine visceral leishmaniasis. Rev. Inst. Med. Trop. Sao Paulo 1986, 28, 431–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toplu, N.; Aydogan, A. An immunohistochemical study in cases with usual and unusual clinicopathological findings of canine visceral leishmaniosis. Parasitol. Res. 2011, 109, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Alves, G.G.G.; Pinho, F.A.; Silva, S.M.M.S.; Cruz, M.S.P.; Costa, F.A.L. Cardiac and pulmonary alterations in symptomatic and asymptomatic dogs infected naturally with Leishmania (Leishmania) chagasi. Braz. J. Med. Biol. Res. 2010, 43, 310–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, D.C.; Buckner, R.G.; Glenn, B.L.; MacVean, D.W. Endemic canine leishmaniosis. Vet. Pathol. 1980, 17, 94–96. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.C.; Castro, R.S.; Figueiredo, M.M.; Michalick, M.S.; Tafuri, W.L.; Tafuri, W.L. Canine visceral leishmaniasis as a systemic fibrotic disease. Int. J. Exp. Pathol. 2013, 94, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, R.; Silva, S.O.; de Almeida, G.G.; de Souza, C.C.; Tafuri, W.L.; Norma Melo, M. Detection of Leishmania infantum DNA in the non-parasitized lung of dogs with visceral leishmaniasis. BMC Vet. Res. 2018, 14, 403. [Google Scholar] [CrossRef]
- Tafuri, W.L.; de Oliveira, M.R.; Melo, M.N.; Tafuri, W.L. Canine visceral leishmaniosis: A remarkable histopathological picture of one case reported from Brazil. Vet. Parasitol. 2001, 96, 203–212. [Google Scholar] [CrossRef]
- Andrade, Z.A. Interstitial pneumonitis in kala-azar. Hospital (Rio J) 1959, 55, 371–381. [Google Scholar]
- Duarte, M.I.; da Matta, V.L.; Corbett, C.E.; Laurenti, M.D.; Chebabo, R.; Goto, H. Interstitial pneumonitis in human visceral leishmaniasis. Trans. R. Soc. Trop. Med. Hyg. 1989, 83, 73–76. [Google Scholar] [CrossRef]
- Raso, P.; Siqueira, J.T. Contribution to the knowledge of the pathological anatomy of visceral leishmaniasis, with special reference to the pulmonary and cardiac lesions. Hospital (Rio J) 1964, 65, 1291–1309. [Google Scholar]
- Maltezou, H.C.; Siafas, C.; Mavrikou, M.; Spyridis, P.; Stavrinadis, C.; Karpathios, T.; Kafetzis, D.A. Visceral leishmaniasis during childhood in southern Greece. Clin. Infect. Dis. 2000, 31, 1139–1143. [Google Scholar] [CrossRef] [PubMed]
- Sarker, C.B.; Chowdhury, K.S.; Siddiqui, N.I.; Jamal, M.F.; Rahman, S.; Momen, A.; Dhar, D.K.; Alam, K.S. Clinical profile of Kala-azar in adults: As seen in Mymensingh Medical College Hospital, Mymensingh, Bangladesh. Mymensingh Med. J. 2003, 12, 41–44. [Google Scholar]
- Kotsifas, K.; Metaxas, E.; Koutsouvelis, I.; Skoutelis, A.; Kara, P.; Tatsis, G. Visceral leishmaniasis with endobronchial involvement in an immunocompetent adult. Case Rep. Med. 2011, 2011, 561985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasgupta, S.; Saha, M.; Chakraborty, J. Visceral leishmaniasis with pleural effusion in an immunocompetent patient. Lung India 2014, 31, 56–58. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, E.; Marty, P.; Pesce, A. Leishmania in bronchoalveolar lavage. Ann. Intern. Med. 1991, 114, 1064–1065. [Google Scholar] [CrossRef]
- Jokipii, L.; Salmela, K.; Saha, H.; Kyrönseppä, H.; Eklund, B.; Evans, D.; von Willebrand, E.; Jokipii, A.M. Leishmaniasis diagnosed fron bronchoalveolar lavage. Scand. J. Infect. Dis. 1992, 24, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Marshall, B.G.; Kropf, P.; Clark, C.; Flanagan, A.M.; Davidson, R.N.; Shaw, R.J.; Müller, I. Bronchopulmonary and mediastinal leishmaniasis: An unusual clinical presentation of Leishmania donovani infection. Clin. Infect. Dis. 2000, 30, 764–769. [Google Scholar] [CrossRef]
- Herrejón, A.; Cervera, A.; Maciá, M.; Ferrer, R.; Blanquer, R. Adenoma bronquioloalveolar asociado a bronquiolitis obliterante y leishmaniasis pulmonary en el sida. Arch. Bronconeumol. 2005, 41, 233–235. [Google Scholar] [CrossRef] [PubMed]
- Robivaro, B.; Funk, G.C.; Dekan, G.; Demetriou, D.; Ziesche, R.; Winkler, S.; Block, L.H. Unusual microbes in asthma exacerbation: Alcaligenes xylosoxidans and Leishmania. Eur. Respir. J. 2009, 33, 1216–1219. [Google Scholar] [CrossRef]
- Donatien, A.; Lestoquard, F. Le parasitisme du poulmon dans la leishmaniose generale du chien. Bull. Soc. Pathol. Exot. 1937, 30, 28–31. [Google Scholar]
- Tryphonas, L.; Zawidzka, Z.; Bernard, M.A.; Janzen, E.A. Visceral leishmaniasis in a dog: Clinical hematological and pathological observations. Can. J. Comp. Med. 1977, 41, 1–12. [Google Scholar]
- Duarte, M.I.; Corbett, C.E. Histopathological and ultrastructural aspects of interstitial pneumonitis of experimental visceral leishmaniasis. Trans. R. Soc. Trop. Med. Hyg. 1984, 78, 683–688. [Google Scholar] [CrossRef]
- Slappender, R.J. Canine leishmaniasis. A review based on 95 cases in the Netherlands. Vet. Q. 1988, 10, 1–16. [Google Scholar] [CrossRef]
- Keenan, C.M.; Hendricks, L.D.; Lightner, L.; Johnson, A.J. Visceral leishmaniosis in the German shepherd dog. II. Pathology. Vet. Pathol. 1984, 21, 80–86. [Google Scholar] [CrossRef]
- Paulino JR, D.; Toni, M.C.; Meirelles, A.E.W.B.; Canola, J.C.; Camacho, A.A. Radiographic findings or uremic pneumonitis in dogs with chronic renal failure. Ars Veterinaria 2013, 29, 013–017. [Google Scholar] [CrossRef] [Green Version]
- Lamb, C.R. The Canine and Feline Lung. In Textbook of Veterinary Diagnostic Radiology, 5th ed.; Thrall, D.E., Ed.; Saunders Elsevier: St. Louis, MO, USA, 2006; pp. 591–608. [Google Scholar]
- Proverbio, D.; Spada, E.; Bagnagatti de Giorgi, G.; Perego, R.; Valena, E. Relationship between Leishmania IFAT titer and clinicopathological manifestations (clinical score) in dogs. BioMed Res Int. 2014, 2014, 412808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saridomichelakis, M.N.; Mylonakis, M.E.; Leontides, L.S.; Koutinas, A.F.; Billinis, C.; Kontos, V.I. Evaluation of lymph node and bone marrow cytology in the diagnosis of canine leishmaniasis (Leishania infantum) in symptomatic and asymptomatic dogs. Am. J. Trop. Med. Hyg. 2005, 73, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Drent, M.; Wagenaar, S.; van Velzen-Blad, H.; Mulder, P.G.; Hoogsteden, H.C.; van den Bosch, J.M. Relationship between plasma cell levels and profile of bronchoalveolar lavage fluid in patients with subacute extrinsic allergic bronchiolitis. Thorax 1993, 48, 835–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalil, A.; Moja, P.; Lambert, C.; Perol, M.; Cotte, L.; Livrozet, J.M.; Boibieux, A.; Vergnon, J.M.; Lucht, F.; Tran, R.; et al. Decreased production of local immunoglobulin A to Pneumocystis carinii in bronchoalveolar lavage fluid from human immunodefieciency virus-positive patients. Infect. Immun. 2000, 68, 1054–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baumann, U.; Göcke, K.; Gewecke, B.; Freihorst, J.; Specht, B.U. Assessment of pulmonary antibodies with induced sputum and bronchoalveolar lavage induced by nasal vaccination against Pseudomonas aeruginosa: A clinical phase I/II study. Respir. Res. 2007, 8, 57–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bispo, A.J.B.; Almeida, M.L.D.; Almeida, R.P.; Bispo Neto, J.; de Oliveira Brito, A.V.; França, C.M. Pulmonary involvement in human visceral leishmaniosis: Clinical and tomographic evaluation. PLoS ONE 2020, 15, e0228176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Rios, F.; González-Lois, C.; Sotelo, T. Pathologic Quiz Case: A patient with acquired immunodeficiency syndrome and endobronchial lesions. Arch. Pathol. Lab. Med. 2001, 125, 1511–1512. [Google Scholar] [CrossRef] [PubMed]
- Dehgani, M.; Monabati, A.; Sanei, M.; Davarpanah, M.A. Visceral Leishmaniasis with massive pulmonary involvement: A case report. Int. J. Infect. 2019, 6, e87993. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | Leish Stage |
|---|---|
| 1 | 3 (severe) |
| 5 | 3 (severe) |
| 11 | 1 (mild) |
| 12 | 3 (severe) |
| 15 | 1 (mild) |
| 19 | 3 (severe) |
| 21 | 2 (moderate) |
| 22 | 3 (severe) |
| 23 | 3 (severe) |
| 24 | 4 (very severe) |
| 25 | 3 (severe) |
| 26 | 3 (severe) |
| 27 | 2 (moderate) |
| 30 | 2 (moderate) |
| 32 | 1 (mild) |
| 35 | 3 (severe) |
| 36 | 3 (severe) |
| 37 | 2 (moderate) |
| 39 | 2 (moderate) |
| 40 | 2 (moderate) |
| 41 | 2 (moderate) |
| 42 | 2 (moderate) |
| 43 | 2 (moderate) |
| 44 | 2 (moderate) |
| 45 | 3 (severe) |
| 46 | 3 (severe) |
| 49 | 2 (moderate) |
| 51 | 2 (moderate) |
| 52 | 3 (severe) |
| 53 | 2 (moderate) |
| 54 | 2 (moderate) |
| Case Number | Lymph Node FNA Cytology | Bone Marrow Cytology | BALF Cytology | Lung FNA Cytology | Serum IFAT Titer | BALF IFAT | Bronchial Mucosa Histopathology | Bronchial Mucosa Immunohistochemistry | BALF Immunocytochemistry | Lung FNA Immunocytochemistry |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Positive | Positive | Negative | Negative | 1/1600 | Positive | Negative | Positive | Positive | Positive |
| 5 | Positive | Positive | Negative | Negative | 1/400 | Positive | Negative | Positive | Positive | Positive |
| 11 | Positive | Negative | Negative | Negative | 1/100 | Positive | Negative | Positive | Positive | Positive |
| 12 | Positive | Positive | Negative | Negative | 1/1600 | Positive | Negative | Negative | Positive | Positive |
| 15 | Positive | Positive | Negative | Negative | 1/3200 | Positive | Negative | Positive | Positive | Positive |
| 19 | Positive | Positive | Negative | Negative | 1/1600 | Positive | Negative | Positive | Positive | Positive |
| 21 | Positive | Positive | Negative | Negative | 1/3200 | Positive | Negative | Negative | Positive | Positive |
| 22 | Positive | Positive | Negative | Negative | 1/1600 | Positive | Negative | Positive | Positive | Positive |
| 23 | Positive | Positive | Negative | Negative | 1/800 | Positive | Negative | Positive | Positive | Positive |
| 24 | Positive | Positive | Negative | Negative | 1/1600 | Negative | Negative | Positive | Positive | Positive |
| 25 | Positive | Positive | Negative | Negative | 1/3200 | Positive | Negative | Positive | Positive | Negative |
| 26 | Positive | Positive | Negative | Negative | 1/3200 | Positive | Negative | Positive | Positive | Positive |
| 27 | Positive | Positive | Negative | Negative | 1/3200 | Negative | Negative | Positive | Positive | Negative |
| 30 | Positive | Positive | Negative | Negative | 1/1600 | Negative | Negative | Positive | Positive | Positive |
| 32 | Positive | Negative | Negative | Negative | 1/1600 | Negative | Negative | Positive | Positive | Positive |
| 35 | Positive | Positive | Positive | Negative | >1/3200 | Positive | Negative | Positive | Positive | Positive |
| 36 | Positive | Positive | Negative | Negative | 1/3200 | Negative | Negative | Negative | Negative | Positive |
| 37 | Positive | Positive | Negative | Negative | 1/800 | Negative | Negative | Positive | Positive | Positive |
| 39 | Positive | Positive | Negative | Negative | 1/1600 | Negative | Negative | Positive | Positive | Positive |
| 40 | Positive | Positive | Negative | Negative | 1/800 | Negative | Negative | Positive | Positive | Positive |
| 41 | Positive | Positive | Negative | Negative | >1/3200 | Negative | Negative | Negative | Positive | Positive |
| 42 | Positive | Positive | Negative | Negative | >1/3200 | Positive | Negative | Positive | Positive | Negative |
| 43 | Positive | Positive | Negative | Negative | 1/3200 | Negative | Negative | Positive | Positive | Positive |
| 44 | Positive | Positive | Negative | Negative | 1/800 | Negative | Negative | Positive | Positive | Positive |
| 45 | Positive | Positive | Negative | Negative | 1/3200 | Negative | Negative | Positive | Positive | Positive |
| 46 | Positive | Positive | Negative | Negative | 1/1600 | Negative | Negative | Positive | Positive | Positive |
| 49 | Positive | Positive | Negative | Negative | 1/3200 | Positive | Negative | Positive | Positive | Negative |
| 51 | Positive | Positive | Negative | Negative | 1/3200 | Negative | Negative | Positive | Positive | Positive |
| 52 | Positive | Positive | Negative | Negative | 1/1600 | Positive | Negative | Positive | Positive | Positive |
| 53 | Positive | Positive | Negative | Negative | 1/800 | Negative | Negative | Positive | Positive | Positive |
| 54 | Positive | Positive | Negative | Negative | 1/200 | Negative | Negative | Positive | Positive | Positive |
| Bronchoscopic Lesions | n (%) |
|---|---|
| Edema | 15 (48.4) |
| Hyperemia | 7 (22.6) |
| Mucosal granularity | 7 (22.6) |
| Secretions | 2 (6.5) |
| Groups | n (%) |
|---|---|
| Mild | 17 (89.5) |
| Moderate | 2 (10.5) |
| Severe | 0 |
| Histopathological Findings | n (%) |
|---|---|
| Macrophage infiltration | 17 (54.8) |
| Edema | 12 (38.7) |
| Neutrophilic infiltration | 9 (29) |
| Fibroblasts | 7 (22.6) |
| Lymphocytic infiltration | 6 (19.3) |
| Bronchial gland hyperplasia | 6 (19.3) |
| Thickening of vessel walls | 5 (16.1) |
| Thickening of the bronchial smooth muscles | 3 (9.7) |
| Severity of Histopathological Lesions | n (%) |
|---|---|
| Mild | 19 (79.2) |
| Moderate | 5 (20.8) |
| Severe | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kavarnos, I.; Pardali, D.; Brellou, G.D.; Papadopoulos, E.; Kritsepi-Konstantinou, M.; Adamama-Moraitou, K.K. Bronchoscopy and Lung Fine-Needle Aspiration for Antemortem Evaluation of Pulmonary Involvement in Dogs with Naturally Occurring Canine Leishmaniosis. Pathogens 2022, 11, 365. https://doi.org/10.3390/pathogens11030365
Kavarnos I, Pardali D, Brellou GD, Papadopoulos E, Kritsepi-Konstantinou M, Adamama-Moraitou KK. Bronchoscopy and Lung Fine-Needle Aspiration for Antemortem Evaluation of Pulmonary Involvement in Dogs with Naturally Occurring Canine Leishmaniosis. Pathogens. 2022; 11(3):365. https://doi.org/10.3390/pathogens11030365
Chicago/Turabian StyleKavarnos, Ioannis, Dimitra Pardali, Georgia D. Brellou, Elias Papadopoulos, Maria Kritsepi-Konstantinou, and Katerina K. Adamama-Moraitou. 2022. "Bronchoscopy and Lung Fine-Needle Aspiration for Antemortem Evaluation of Pulmonary Involvement in Dogs with Naturally Occurring Canine Leishmaniosis" Pathogens 11, no. 3: 365. https://doi.org/10.3390/pathogens11030365
APA StyleKavarnos, I., Pardali, D., Brellou, G. D., Papadopoulos, E., Kritsepi-Konstantinou, M., & Adamama-Moraitou, K. K. (2022). Bronchoscopy and Lung Fine-Needle Aspiration for Antemortem Evaluation of Pulmonary Involvement in Dogs with Naturally Occurring Canine Leishmaniosis. Pathogens, 11(3), 365. https://doi.org/10.3390/pathogens11030365