
The Prevalence of Onchocerciasis-Associated Epilepsy in Mundri West and East Counties, South Sudan: A Door-to-Door Survey

 , ,
, , 
Abstract
:1. Introduction
2. Methodology
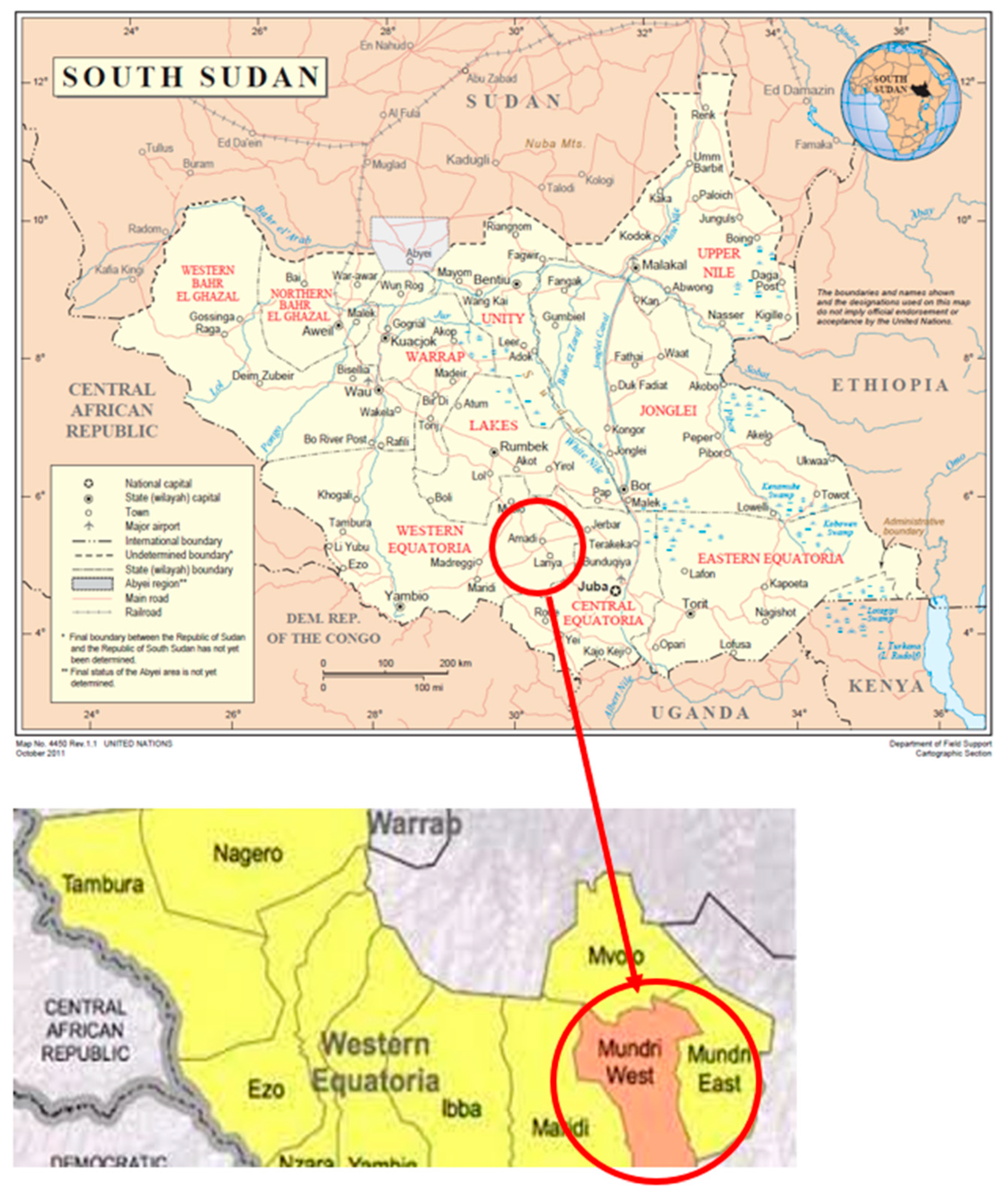
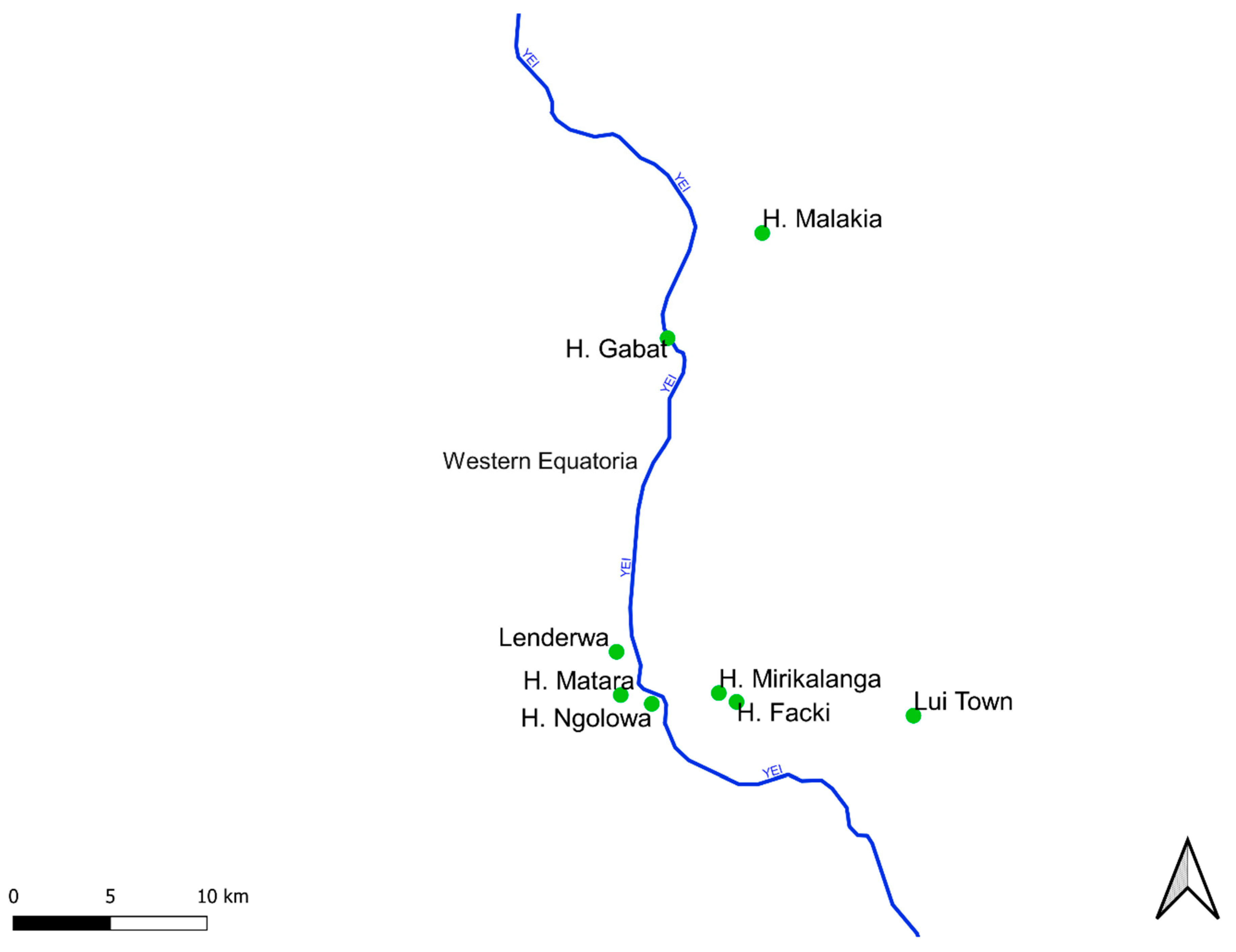
2.1. Study Setting
2.2. Study Design
2.3. Definitions
2.4. Data Collection, Management
2.5. Onchocerciasis Antibody Testing of Children
2.6. Data Analysis
3. Results
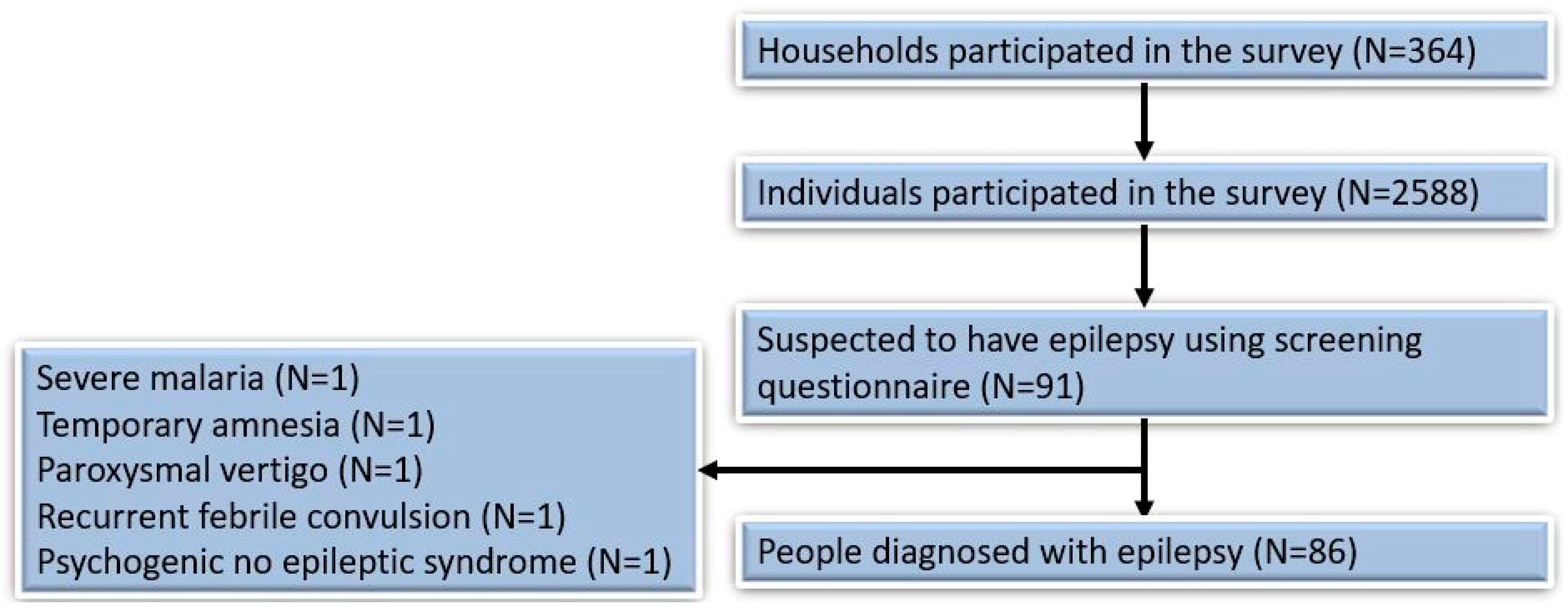
3.1. Households Participating in the Survey
3.2. Prevalence of Epilepsy and Potential Onchocerciasis-Associated Co-Morbidities
3.3. Characteristics of Persons with Epilepsy
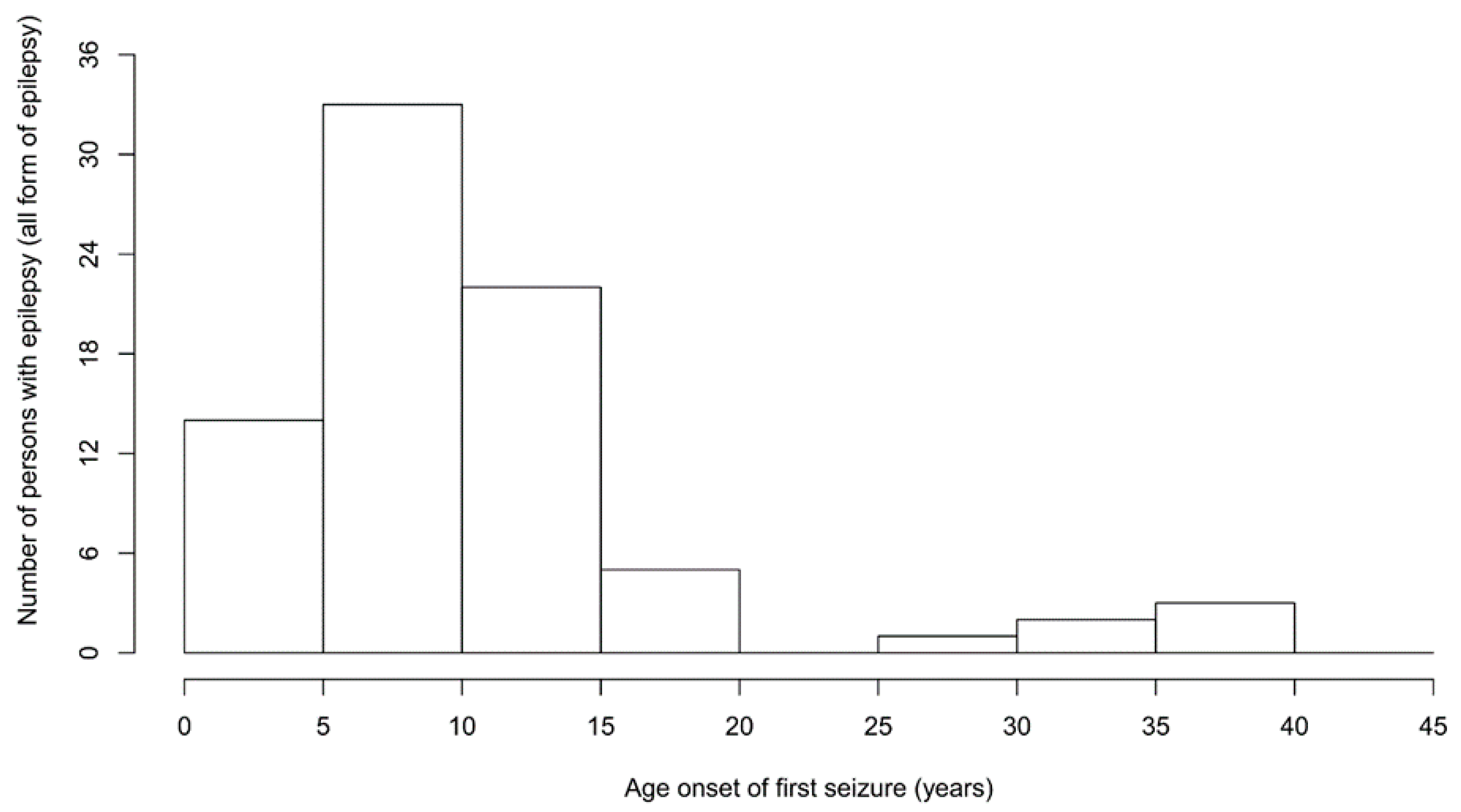
3.4. Incidence of Epilepsy
3.5. Onchocerciasis-Related Morbidity in the Family
3.6. Mortality of Persons with Suspected Epilepsy
3.7. Risk Factors for Epilepsy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Colebunders, R.; Siewe Fodjo, J.N.; Hopkins, A.; Hotterbeekx, A.; Lakwo, T.L.; Kalinga, A.; Logora, M.Y.; Basanez, M.G. From river blindness to river epilepsy: Implications for onchocerciasis elimination programmes. PLoS Negl. Trop. Dis. 2019, 13, e0007407. [Google Scholar] [CrossRef] [Green Version]
- Hotterbeekx, A.; Lammens, M.; Idro, R.; Akun, P.R.; Lukande, R.; Akena, G.; Nath, A.; Taylor, J.; Olwa, F.; Kumar-Singh, S.; et al. Neuroinflammation and Not Tauopathy Is a Predominant Pathological Signature of Nodding Syndrome. J. Neuropathol. Exp. Neurol. 2019, 78, 1049–1058. [Google Scholar] [CrossRef]
- Gumisiriza, N.; Mubiru, F.; Siewe Fodjo, J.N.; Mbonye Kayitale, M.; Hotterbeekx, A.; Idro, R.; Makumbi, I.; Lakwo, T.; Opar, B.; Kaducu, J.; et al. Prevalence and incidence of nodding syndrome and other forms of epilepsy in onchocerciasis-endemic areas in northern Uganda after the implementation of onchocerciasis control measures. Infect. Dis. Poverty 2020, 9, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gumisiriza, N.; Kaiser, C.; Asaba, G.; Onen, H.; Mubiru, F.; Kisembo, D.; Siewe Fodjo, J.N.; Colebunders, R. Changes in epilepsy burden after onchocerciasis elimination in a hyperendemic focus of western Uganda: A comparison of two population-based, cross-sectional studies. Lancet Infect. Dis. 2020, 20, 1315–1323. [Google Scholar] [CrossRef]
- Tumwine, J.K.; Vandemaele, K.; Chungong, S.; Richer, M.; Anker, M.; Ayana, Y.; Opoka, M.L.; Klaucke, D.N.; Quarello, A.; Spencer, P.S. Clinical and epidemiologic characteristics of nodding syndrome in Mundri County, southern Sudan. Afr. Health Sci. 2012, 12, 242–248. [Google Scholar] [CrossRef] [Green Version]
- Colebunders, R.; Chater, J.Y.; Olore, P.C.; Puok, K.; Bhattacharyya, S.; Menon, S.; Abd-Elfarag, G.; Ojok, M.; Ensoy-Musoro, C.; Lako, R.; et al. High prevalence of onchocerciasis-associated epilepsy in villages in Maridi County, Republic of South Sudan: A community-based survey. Seizure 2018, 63, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colebunders, R.; Abd-Elfarag, G.; Carter, J.Y.; Olore, P.C.; Puok, K.; Menon, S.; Fodjo Siewe, J.N.; Bhattacharyya, S.; Ojok, M.; Lako, R.; et al. Clinical characteristics of onchocerciasis-associated epilepsy in villages in Maridi County, Republic of South Sudan. Seizure 2018, 62, 108–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raimon, S.; Dusabimana, A.; Abd-Elfarag, G.; Okaro, S.; Carter, J.Y.; Newton, C.R.; Logora, M.Y.; Colebunders, R. High Prevalence of Epilepsy in an Onchocerciasis-Endemic Area in Mvolo County, South Sudan: A Door-To-Door Survey. Pathogens 2021, 10, 599. [Google Scholar] [CrossRef]
- Lakwo, T.L.; Raimon, S.; Tionga, M.; Siewe Fodjo, J.N.; Alinda, P.; Sebit, W.J.; Carter, J.Y.; Colebunders, R. The Role of the Maridi Dam in Causing an Onchocerciasis-Associated Epilepsy Epidemic in Maridi, South Sudan: An Epidemiological, Sociological, and Entomological Study. Pathogens 2020, 9, 315. [Google Scholar] [CrossRef] [PubMed]
- Abd-Elfarag, G.; Logora, M.Y.; Carter, J.Y.; Ojok, M.; Songok, J.; Menon, S.; Wit, F.; Lako, R.; Colebunders, R. The effect of bi-annual community-directed treatment with ivermectin on the incidence of epilepsy in onchocerciasis endemic villages in South Sudan: A study protocol. Infect. Dis. Poverty 2018, 7, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diagana, M.; Preux, P.M.; Tuillas, M.; Ould Hamady, A.; Druet-Cabanac, M. Depistage de l’epilepsie en zones tropicales: Validation d’un questionnaire en Mauritanie. Bull Soc. Pathol. Exot. 2006, 99, 103–107. [Google Scholar] [PubMed]
- Fisher, R.S.; Cross, J.H.; D’Souza, C.; French, J.A.; Haut, S.R.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshe, S.L.; et al. Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia 2017, 58, 531–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, R.S.; Acevedo, C.; Arzimanoglou, A.; Bogacz, A.; Cross, J.H.; Elger, C.E.; Engel, J., Jr.; Forsgren, L.; French, J.A.; Glynn, M.; et al. ILAE official report: A practical clinical definition of epilepsy. Epilepsia 2014, 55, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. International Scientific Meeting on Nodding Syndrome, Kampala, Uganda. 2012. Available online: https://www.who.int/neglected_diseases/diseases/Nodding_syndrom_Kampala_Report_2012.pdf (accessed on 16 March 2022).
- Foger, K.; Gora-Stahlberg, G.; Sejvar, J.; Ovuga, E.; Jilek-Aall, L.; Schmutzhard, E.; Kaiser, C.; Winkler, A.S. Nakalanga Syndrome: Clinical Characteristics, Potential Causes, and Its Relationship with Recently Described Nodding Syndrome. PLOS Negl. Trop Dis. 2017, 11, e0005201. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Collier, J.M.; Quah, D.M.; Purvis, T.; Bernhardt, J. The modified Rankin Scale in acute stroke has good inter-rater-reliability but questionable validity. Cerebrovasc. Dis. 2010, 29, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Siewe Fodjo, J.N.; Tatah, G.; Tabah, E.N.; Ngarka, L.; Nfor, L.N.; Chokote, S.E.; Mengnjo, M.K.; Dema, F.; Sitouok, A.T.; Nkoro, G.; et al. Epidemiology of onchocerciasis-associated epilepsy in the Mbam and Sanaga river valleys of Cameroon: Impact of more than 13 years of ivermectin. Infect. Dis. Poverty 2018, 7, 114. [Google Scholar] [CrossRef] [PubMed]
- Siewe, J.N.F.; Ukaga, C.N.; Nwazor, E.O.; Nwoke, M.O.; Nwokeji, M.C.; Onuoha, B.C.; Nwanjor, S.O.; Okeke, J.; Osahor, K.; Chimechefulam, L.; et al. Low prevalence of epilepsy and onchocerciasis after more than 20 years of ivermectin treatment in the Imo River Basin in Nigeria. Infect Dis. Poverty 2019, 8, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logora, M.Y.; National Neglected Tropical Disease Control, Ministry of Health, Juba, South Sudan. Personal communication, 2022.
- Jada, R.S.; Amref Health Africa, Juba, South Sudan. Personal communication, 2022.
- Colebunders, R.; Njamnshi, A.K.; Menon, S.; Newton, C.R.; Hotterbeekx, A.; Preux, P.M.; Hopkins, A.; Vaillant, M.; Siewe Fodjo, J.N. Onchocerca volvulus and epilepsy: A comprehensive review using the Bradford Hill criteria for causation. PLoS Negl. Trop Dis. 2021, 15, e0008965. [Google Scholar] [CrossRef] [PubMed]
- Wagner, R.G.; Bottomley, C.; Ngugi, A.K.; Ibinda, F.; Gomez-Olive, F.X.; Kahn, K.; Tollman, S.; Newton, C.R.; Group, S.W.; Wagner, R.; et al. Incidence, Remission and Mortality of Convulsive Epilepsy in Rural Northeast South Africa. PLoS ONE 2015, 10, e0129097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngugi, A.K.; Bottomley, C.; Kleinschmidt, I.; Wagner, R.G.; Kakooza-Mwesige, A.; Ae-Ngibise, K.; Owusu-Agyei, S.; Masanja, H.; Kamuyu, G.; Odhiambo, R.; et al. Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: Cross-sectional and case-control studies. Lancet Neurol. 2013, 12, 253–263. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Village | Participants in Survey, n | Epilepsy Confirmed Cases, n (%) | Probable Nodding Syndrome, n (%) | Itching, n (%) | Blindness, n (%) | Ivermectin Use, n (%) | Approximate Distance to Yei River in km |
|---|---|---|---|---|---|---|---|
| Mundri West | |||||||
| Amadi Payam | |||||||
| Hai Gabat | 328 | 14 (4.3) | 4 (1.2) | 231 (70.4) | 18 (5.5) | 155 (47.3) | <2 km |
| Hai Malakia | 256 | 3 (1.2) | 0 (0.0) | 174 (67.9) | 10 (3.9) | 140 (54.7) | >2 km |
| Mundri Centre Payam | |||||||
| Hai Facki | 332 | 12 (3.6) | 3 (0.9) | 155 (46.7) | 14 (4.2) | 213 (64.2) | >2 km |
| Hai Ngulawa | 286 | 10 (3.5) | 4 (1.4) | 88 (30.8) | 7 (2.4) | 136 (47.5) | <2 km |
| Hai Lenderwa | 151 | 10 (6.6) | 4 (2.6) | 46 (30.5) | 4 (2.6) | 85 (56.3) | <2 km |
| Hai Mirikalanga | 372 | 8 (2.2) | 2 (0.5) | 133 (35.7) | 10 (2.7) | 202 (54.3) | >2 km |
| Mundri East | |||||||
| Lui town | 862 | 28 (3.2) | 6 (0.7) | 214 (2.5) | 7 (0.8) | 295 (34.2) | >2 km |
| Overall East and West Mundri | 2588 | 85 (3.3) | 23 (0.9) | 1041 (40.2) | 70 (2.7) | 1226 (47.4) | |
| Participants’ Characteristics | |
|---|---|
| Female sex, n (%) | 43 (50.0) |
| Age (years), median (IQR) | 25.0 (20.0–29.0) |
| Born in the study village, n (%) | 48 (57.1) |
| Period (years) of residing in the survey area, median (IQR) | 20.0 (10.0–25.0) |
| Epilepsy features | |
| Age of onset of the first seizure in all PWE, median (IQR) * | 10.0 (8.0–15.0) |
| Age of onset of the first nodding seizure, median (IQR) | 8.0 (5.0–12.0) |
| Onset of the first seizure last year, n (%) | 2 (2.4) |
| Onset of the first seizure in last 5 years, n (%) | 4 (5.0) |
| Experienced absence(s) or sudden loss of contact with surroundings, for a short duration of time, n (%) | 1 (1.2) |
| Experienced sudden, uncontrollable twitching or shaking of arms, legs, or head, for a period of a few minutes, with amnesia ^ n (%) | 76 (90.5) |
| History of head nodding, n (%) | 23 (27.4) |
| Loss of bladder control, n (%) | 58 (69.1) |
| Foaming at the mouth, n (%) | 77 (91.7) |
| Biting of the tongue, n (%) | 68 (80.9) |
| Most frequent seizure types | |
| Generalised convulsive seizures only, n (%) | 61 (72.6) |
| Only nodding seizures, n (%) | 7 (8.3) |
| Nodding and convulsive seizures, n (%) | 16 (19.1) |
| Frequency of seizures | |
| Daily seizure, n (%) | 1 (1.2) |
| Weekly seizure, n (%) | 13 (15.5) |
| Monthly seizure, n (%) | 55 (63.1) |
| Yearly seizure, n (%) | 86 (100) |
| Experienced seizure in the last 12 months, n (%) | 72 (83.7) |
| Seizures/head nodding triggers | |
| Spontaneous (no obvious trigger), n (%) | 67 (79.8) |
| Sight of food, n (%) | 8 (9.5) |
| Cold weather, n (%) | 9 (10.7) |
| Severe diseases preceding the onset of seizures | |
| Measles, n (%) | 1 (1.2) |
| Malaria, n (%) | 1 (1.2) |
| Physical examination/symptoms & | |
| Reduced vision or blind in at least one eye, n (%) | 3 (3.6) |
| Thoracic/spinal abnormalities, n (%) | 2 (2.4) |
| Cervical lymph nodes, n (%) | 10 (11.9) |
| Nakalanga manifestations, n (%) | 2 (2.5%) |
| Itching, n (%) | 20 (23.8) |
| Burn lesions, n (%) | 14 (16.7) |
| Papular/nodular pruritic skin, n (%) | 12 (14.3) |
| Neurological examination & | |
| Severe cognitive impairment, n (%) | 6 (7.1) |
| Paresis, n (%) | 3 (3.6) |
| Behavioural problem, n (%) | 1 (1.2) |
| Level of autonomy assessed with a modified Rankin scale | |
| No significant disability despite symptoms (able to carry out all usual duties and activities) | 67 (79.8) |
| Slight disability (unable to carry out all previous activities, but able to look after own affairs without assistance) | 8 (9.5) |
| Moderate disability (requiring some help, but able to walk without assistance) | 5 (5.9) |
| Moderately severe disability (unable to walk without assistance and unable to attend to own bodily needs without assistance) | 4 (4.8) |
| Epilepsy classification | |
| Epilepsy without head nodding, n (%) | 63 (73.2) |
| Head nodding only, n (%) | 7 (8.1) |
| Head nodding with other seizure types, n (%) | 16 (18.6) |
| Meeting OAE criteria +, n (%) | 65 (81.3) |
| Family members with epilepsy | |
| Family history of seizures, n (%) | 45 (53.6) |
| Siblings (brother/sister) P, n (%) | 37 (82.2) |
| Father/Mother P, n (%) | 7 (15.7) |
| Grandparent P, n (%) | 1 (2.2) |
| History of anti-seizure medication | |
| Never used an anti-seizure medication, n (%) | 4 (4.6) |
| Currently taking an anti-seizure medication, n (%) | 82 (95.4) |
| Type of anti-seizure medication T | |
| Phenobarbital, n (%) | 24 (29.4) |
| Phenytoin, n (%) | 1 (1.2) |
| Carbamazepine, n (%) | 55 (67.1) |
| Sodium valproate, n (%) | 1 (1.2) |
| Ivermectin intake | |
| Ever received ivermectin, n (%) # | 58/74 (78.4) |
| Ivermectin intake in 2021, n (%) $ | 33/79 (41.7) |
| Ivermectin intake in 2021 not known, n (%) | 7 (8.9) |
| Epilepsy without Nodding Syndrome (n = 63) | Nodding Syndrome (n = 23) | p-Value | |
|---|---|---|---|
| Female, n (%) | 31 (50.8) | 13 (56.5) | 0.825 |
| Age (years), median (IQR) | 25.0 (20.0–32.0) | 24.0 (20.0–28.0) | 0.012 |
| Age of onset of first seizures (years) | 10.0 (8.0–15.0) | 8.0 (5.0–12.0) | 0.007 |
| Triggers of seizures | |||
| Sight of food, n (%) | 0 (0.0) | 8 (34.8) | NA |
| Cold weather, n (%) | 1 (1.6) | 7 (30.4) | <0.001 |
| Spontaneous (no obvious trigger), n (%) | 60 (95.2) | 8 (34.8) | <0.001 |
| Itching, n (%) | 13 (20.6) | 7 (30.4) | 0.556 |
| Burn lesion (s), n (%) | 5 (7.9) | 5 (21.7) | 0.183 |
| Papular/nodular pruritic skin, n (%) | 8 (12.7) | 4 (17.3) | 0.881 |
| Moderate and severe disabilities, n (%) | 5 (7.9) | 4 (17.4) | 0.384 |
| Characteristics | aOR | 95% CI | p-Value | |
|---|---|---|---|---|
| Age (years) | 1.450 | 1.286 | 1.636 | <0.0001 |
| Age*Age | 0.994 | 0.992 | 0.996 | <0.0001 |
| Male vs. female sex | 1.143 | 0.712 | 1.836 | 0.580 |
| Family income from activities related to the river vs. from other activities & | 1.178 | 0.520 | 2.670 | 0.694 |
| Village < 2 km from the Yei River vs. >2 km from the Yei River | 1.692 | 0.918 | 3.117 | 0.092 |
| Ivermectin taken during last round vs. no ivermectin taken | 0.638 | 0.376 | 1.083 | 0.096 |
| Skin itching vs. no itching in the family | 1.014 | 0.543 | 1.893 | 0.965 |
| Blindness/blurred vision vs. no blindness in the family | 1.940 | 0.956 | 3.940 | 0.067 |
| 1.685 (0.767) | ||||
| Variables | aOR | 95% CI | p-Value | |
|---|---|---|---|---|
| Age (years) | 1.635 | 1.353 | 1.975 | <0.0001 |
| Age*Age | 0.991 | 0.988 | 0.995 | <0.0001 |
| Male vs. female sex | 0.990 | 0.546 | 1.797 | 0.975 |
| Family income from activities related to the river vs. from other activities & | 1.184 | 0.459 | 3.054 | 0.727 |
| Village < 2 km from the Yei River vs. >2 km from the Yei River | 2.241 | 1.034 | 4.861 | 0.041 |
| 2.419 (1.338) | ||||
| Age Group (years) | Ivermectin Use in the Total Study Population, n (%) # | Ivermectin Use Among PWE, n (%) * | p-Value & |
|---|---|---|---|
| <5 years | 0/240 (0.0) | 0 (0.0) | NA |
| 5–10 years | 235/492 (48.0) | 0 (0.0) | NA |
| 10–15 years | 183/369 (49.6) | 1/4 (25.0) | 0.691 |
| 15–20 years | 235/426 (55.2) | 10/23 (43.5) | 0.998 |
| 20–25 years | 138/245 (56.3) | 9/24 (37.5) | 0.534 |
| 25–30 years | 115/211 (54.5) | 8/20 (40.0) | 0.295 |
| 30–35 years | 56/99 (56.6) | 3/6 (50.0) | 0.775 |
| 35–40 years | 72/149 (48.3) | 1/2 (50.0) | 0.999 |
| 40–45 years | 29/69 (42.0) | 0/2 (0.0) | NA |
| >45 years | 142/276 (51.4) | 1/4 (25.0) | 0.584 |
| Overall | 1212/2583 (46.9) | 33/79 (41.8) | 0.706 |
| Study Site | Ov16 IgG4 Seroprevalence | Ivermectin Coverage * | ||||||
|---|---|---|---|---|---|---|---|---|
| 3 years | 4 years | 5 years | 6 years | 7 years | 8 years | 9 years | ||
| Amadi | 3/8 (37.5%) | 0/4 (0.0%) | 3/18 (16.7%) | 2/7 (28.5%) | 1/11 (9.1%) | 4/14 (28.6%) | 6/12 (50.0%) | 22/62 (35.5%) |
| Mundri Centre | 1/24 (4.2%) | 0/17 (0.0%) | 1/26 (3.8%) | 1/18 (5.5%) | 0/26 (0.0%) | 1/23 (4.3%) | 0/16 (0.0%) | 21/109 (19.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jada, S.R.; Dusabimana, A.; Abd-Elfarag, G.; Okaro, S.; Brusselaers, N.; Carter, J.Y.; Logora, M.Y.; Rovarini, J.M.; Newton, C.R.; Colebunders, R. The Prevalence of Onchocerciasis-Associated Epilepsy in Mundri West and East Counties, South Sudan: A Door-to-Door Survey. Pathogens 2022, 11, 396. https://doi.org/10.3390/pathogens11040396
Jada SR, Dusabimana A, Abd-Elfarag G, Okaro S, Brusselaers N, Carter JY, Logora MY, Rovarini JM, Newton CR, Colebunders R. The Prevalence of Onchocerciasis-Associated Epilepsy in Mundri West and East Counties, South Sudan: A Door-to-Door Survey. Pathogens. 2022; 11(4):396. https://doi.org/10.3390/pathogens11040396
Chicago/Turabian StyleJada, Stephen Raimon, Alfred Dusabimana, Gasim Abd-Elfarag, Samuel Okaro, Nele Brusselaers, Jane Y. Carter, Makoy Yibi Logora, Jacopo Mattia Rovarini, Charles R. Newton, and Robert Colebunders. 2022. "The Prevalence of Onchocerciasis-Associated Epilepsy in Mundri West and East Counties, South Sudan: A Door-to-Door Survey" Pathogens 11, no. 4: 396. https://doi.org/10.3390/pathogens11040396
APA StyleJada, S. R., Dusabimana, A., Abd-Elfarag, G., Okaro, S., Brusselaers, N., Carter, J. Y., Logora, M. Y., Rovarini, J. M., Newton, C. R., & Colebunders, R. (2022). The Prevalence of Onchocerciasis-Associated Epilepsy in Mundri West and East Counties, South Sudan: A Door-to-Door Survey. Pathogens, 11(4), 396. https://doi.org/10.3390/pathogens11040396